
Abstract
Introduction
Lumbar puncture is a commonly used diagnostic and therapeutic procedure albeit with several minor notable complications routinely expressed to patients. 1 In rare instances, serious complications may arise, including intracranial hypotension and cerebral herniation. 2 Yet, a more insidious complication, pneumocephalus, may present with various cranial nerve deficits that may present in patients post-procedurally as gravely concerning for such aforementioned major complications.
Pneumocephalus or intracranial aerocele is the presence of air within the ventricular system, brain parenchyma, or epidural, subdural, and subarachnoid compartments which may be intra-axial or extra-axial. 3 This is frequently reported in patients undergoing invasive neurosurgical procedures (e.g., craniotomies)4,5 but also noted to be secondary to infections, 6 tumors of the skull, 7 and traumas which create a communication between the intracranial structures and air-containing cavities. 8 Spontaneous occurrence of this condition is a possibility without clear etiology. 9 However, pneumocephalus is uncommonly reported after procedures such as spinal or epidural anesthesia and is furthermore an even lesser complication following lumbar punctures. 10
A review by Nashio et al. on the presentation of post-procedural cranial nerve palsies in patient case reports published from 1930 to 2002 found diplopia as commonplace after lumbar punctures. 11 Specifically, an abducens nerve palsy was the predominantly affected cranial nerve in as high as 95% of the cases and that 80% of such cases presented with co-occurring multiple cranial nerve palsies. They postulated that the extraocular muscle abnormalities were due to sheer stress and downward traction on cranial nerves secondary to cerebrospinal fluid (CSF) leak after a dural puncture. Moreover, pneumocephalus was reported as a complication of spinal anesthesia in 47% of cases, followed by myelography in 18%, diagnostic lumbar puncture in 12%, epidural anesthesia/injection in 11%, continuous spinal anesthesia in 4%, and other dural procedures accounting for 9%. 11 Few case reports identified this complication after epidural injection with an accidental dural puncture and is described in the literature as extremely rare,12–14 and in one report, incidence was reported to be approximating 1–2 cases per year. 15
Currently, the incidence of pneumocephalus from lumbar punctures is not well described in the literature despite its risk from epidural injections reported as 1 in 67. 16 The incidence of a cranial nerve palsy that is attributed to pneumocephalus is furthermore extremely rare. Here, we present a patient undergoing active chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) in addition to intrathecal methotrexate for high-grade mature T-cell non-Hodgkin’s lymphoma complicated by an acute onset of horizontal diplopia post-intrathecal injection. Diplopia is not a known complication of the patient’s chemotherapy regimen, and further imaging studies demonstrated a new pneumocephalus abutting the abducens nerve in the prepontine cistern.
Here, we review the most up-to-date literature on this complication as it pertains to pneumocephalus causing extraocular visual motor dysfunction after spinal procedures, including the following: epidural anesthesia, intrathecal chemotherapy, steroid injections, lumbar punctures, and lumbar laminectomies. We analyze different presentations of pneumocephalus clinically, highlight their location on various imaging modalities, including computed tomography (CT) and magnetic resonance imaging (MRI), and discuss treatment options utilized among cases reported.
Case report
A 61 year-old female patient with an insignificant medical history presented to us for an enlarging neck lymph node that was biopsied to reveal a high-grade mature T-cell non-Hodgkin lymphoma. During the admission, the patient received the first cycle of CHOP chemotherapy and a first infusion intrathecal methotrexate infusion. Post-procedurally, the patient developed a new onset of painless right-sided horizontal diplopia. The intrathecal injection was performed in prone positioning using a fluoroscopic-guided 20-gauge spinal needle into the L2–L3 space. Next, approximately 10 mL of CSF fluid was collected followed by 12 mg of methotrexate intrathecal injection. CSF studies returned unremarkable for inflammatory, malignant, and infectious markers.
Upon physical examination, there was a notable partial right-sided abducens palsy without any other focal neurological deficits. Non-contrast computed tomography (CT) scan of the head demonstrated a pneumocephalus anterior to the pons and at the level of the clivus abutting the right abducens nerve (Figure 1). Follow-up magnetic resonance image (MRI) of the brain with and without contrast was unremarkable for other potential causes of this acute palsy presentation, including infections, ischemic stroke, or herniation from intracranial hypotension. The patient was monitored and managed expectantly without any acute interventions and upon follow-up in 24 hours there was complete resolution of her symptoms. Axial (a), coronal (b), and sagittal (c) non-contrast head CT highlighting a right-sided pneumocephalus in the prepontine cistern compressing the right abducens nerve (arrows in A, B, and C). Axial MRI sections including diffusion-weighted images (DWI) (d), fluid-attenuated inversion recovery (FLAIR) (e), and T2-weighted image (f) were unremarkable.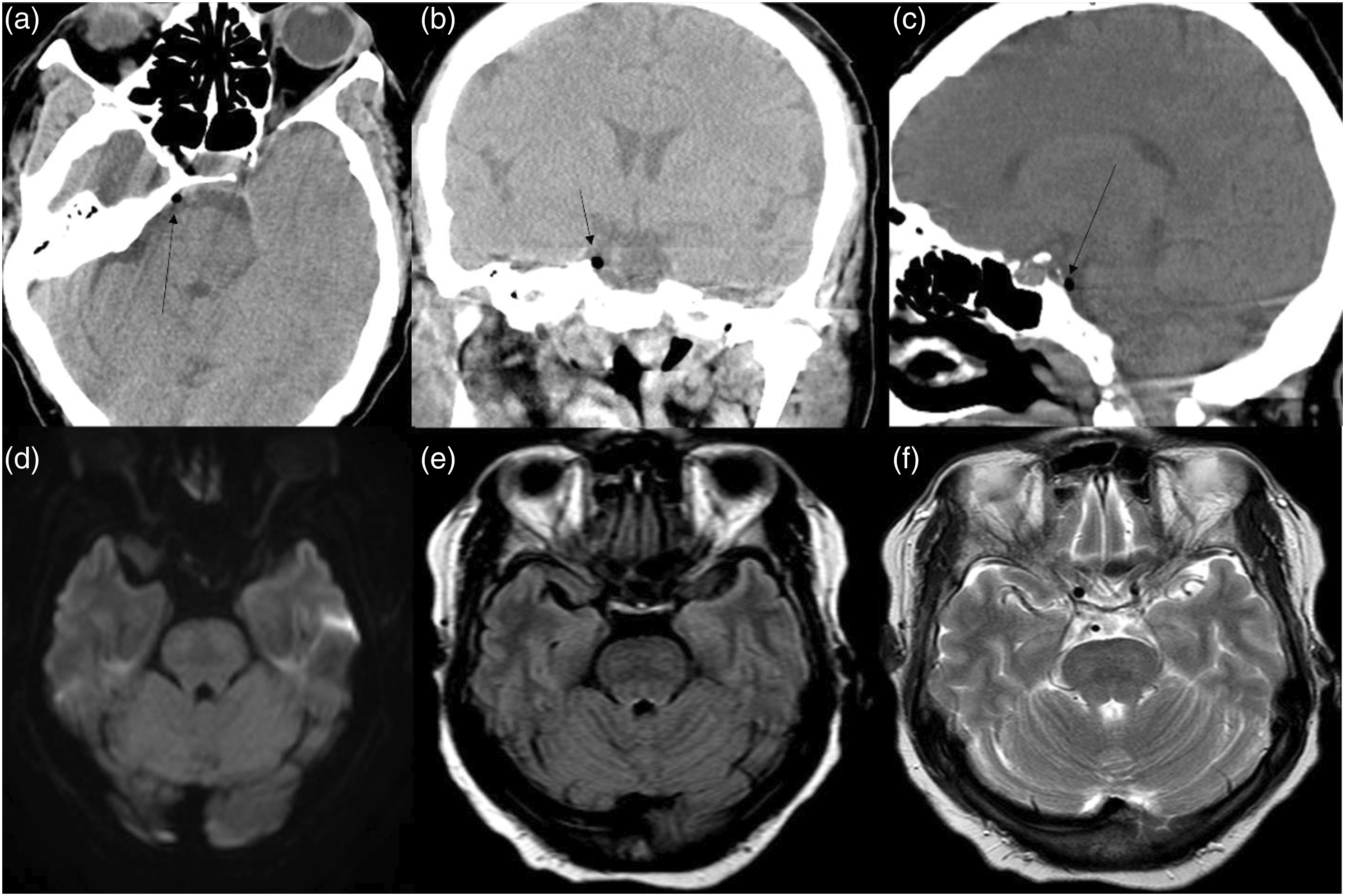
Methods
We performed a literature search using PubMed in April 2022. The terms “pneumocephalus” and “cranial nerve palsy” or “diplopia” were used either alone or in combination with “lumbar puncture,” “epidural injection,” or “spinal procedures.” We have included articles that discuss patients who underwent various spinal procedures, including intrathecal injections, epidural anesthesia, epidural steroid injections, lumbar punctures, and laminectomies with pneumocephalus as a complication causing cranial nerve palsy in conjunction with or without other features. Data presented here was derived from retrospective observational studies, review articles, case series, and individual reports.
Discussion
Pathophysiology
It is theorized that pneumocephalus occurs after an accidental introduction of air into the subarachnoid space as a complication that arises from spinal procedures. The commonly used technique called “Loss-of-Resistance” to air was shown to be associated with a higher risk for pneumocephalus and post-procedural headaches. This is likely attributed to accidental dura puncture and hence air migration.17–19 Two other mechanisms were described as possibly contributory: the ball-valve theory, wherein a dura defect acts as a one-way valve trapping air inside the cranial cavity, 20 and the inverted bottle theory, whereby negative intracranial pressure ensued from retrieved CSF is replaced by air. 21 While a cranial nerve palsy, often abducens palsy, after lumbar puncture is hypothesized to be due to intracranial hypotension with downward traction of the nerve due to its anatomic course, pneumocephalus may in fact be the etiology and investigated. 11
Symptomatology
This table shows the cases presented throughout the literature and compares different patients’ clinical presentations including their symptoms as well as their physical examination with the cranial nerve being involved. It also reports the images used and their findings.
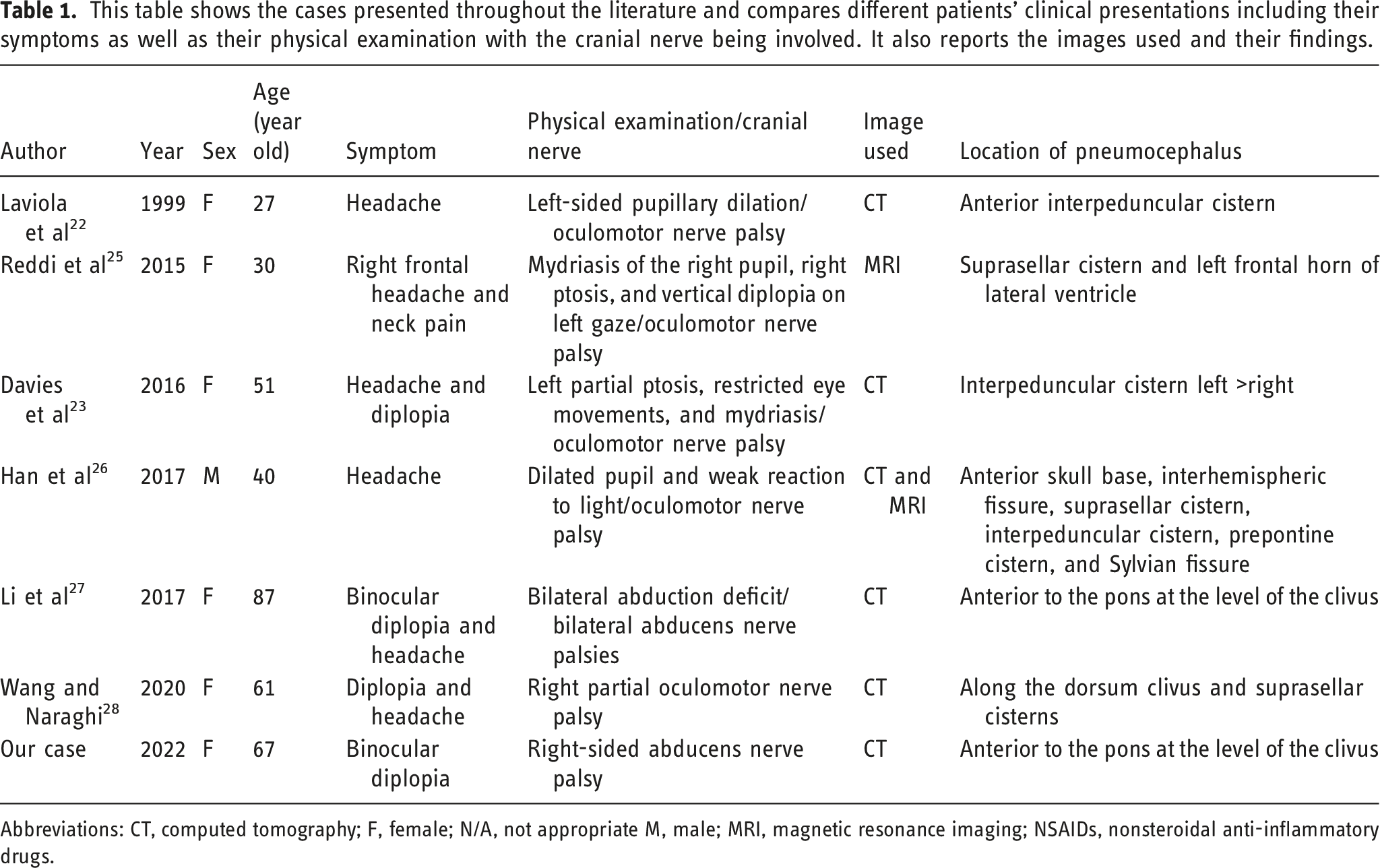
Abbreviations: CT, computed tomography; F, female; N/A, not appropriate M, male; MRI, magnetic resonance imaging; NSAIDs, nonsteroidal anti-inflammatory drugs.
Simple pneumocephalus must be differentiated from tension pneumocephalus, in which the latter represents a large amount of air accumulating intracranially producing pressure with midline shift which can lead to a fulminant presentation of neurosurgical emergency. 26 This condition is reported to cause cerebral herniation, coma, and death, often occurring after traumatic skull fractures, severe brain atrophy, or intracranial tumor resections.29,30 In contrast, as seen in our case, simple pneumocephalus can be benign with minimal symptoms and signs on examination which typically resolve independently (Table 1).27,28
Most case reports to-date that highlight oculomotor nerve palsy had a pneumocephalus in the interpeduncular cistern where the nerve travels. 31 Laviola et al. demonstrated a case of a pregnant patient who underwent an epidural anesthesia for labor and had developed a dilated and non-reactive pupil on the left, correlating with a pneumocephalus directly abutting the oculomotor nerve. 22 Davies et al. also reported an oculomotor nerve palsy due to pneumocephalus manifesting as headache and diplopia after posterior hemilaminectomy at L2–L3 for the treatment of an intradural myxopapillary ependymoma. 23
Diagnosis
In our patient, the abducens nerve was clearly involved as the location of the pneumocephalus on CT imaging correlates with both clinical presentation and known anatomical nerve course. The nerve has four divisions, including its source nucleus, the cisternal portion, cavernous sinus portion, and orbital portion. Approximately 40% of the nerve axons traverse through the medial longitudinal fasciculus and cross over to the contralateral medial rectus nuclei. 32 The axons exit the nuclei and travel rostral and anterior in the pontomedullary groove toward the clivus via Dorello’s canal where it will enter the dura inferior to the clinoid process to emerge into the cavernous sinus. 33 It is within this cisternal portion of the nerve trajectory that it is susceptible to increasing tension from increased intracranial pressures or, as in this case, impingement by a pneumocephalus that can be visualized with imaging.
CT scans are highly sensitive and specific for detecting air. As little as 0.5 cc of air can be detected on a standard CT. This is due to the low attenuation coefficient of air making it easily discernible from surrounding tissue as it carries a standard of −1000 Hounsfield units. As highlighted in Table 1, most cases in the literature begin diagnostic evaluation with a CT scan that is sufficiently diagnostic. 3 Nevertheless, it is critical to distinguish simple from tension pneumocephalus, as the latter is a neurosurgical emergency. 26 In fact, one study suggests approximately 65 cc of air is sufficient to cause tension pneumocephalus, however, other reports dispute this figure with one study demonstrating no significant difference in volume of air between tension and non-tension pneumocephalus.34,35 Therefore, further imaging and monitoring may be necessary in such unclear circumstances. “Peaking sign” refers to air compression of the frontal lobes and creating a “peak” in the midline. It has been proposed by Pop et al. that this finding is due to pressure from air forcing blood from the bridging vein into the superior sagittal sinus. 36 This sign is more commonly seen in non-tension pneumocephalus. 35 The “Mount Fuji” sign refers to a similar compression of the frontal lobes by air but is differentiated by the separation of the frontal lobe. It was postulated by Ishitwata et al. that this occurs when the pressure of air exceeds that of the CSF between the frontal lobes. 35 In the same report, a “Mount Fuji” sign was seen in 80% of the cases of tension pneumocephalus. These radiographic signs, combined with the clinical picture, are essential to determine the need for emergent intervention.
Although CT imaging is an adequate, fast, and cost-effective modality for diagnosing pneumocephalus, clinicians should consider obtaining an MRI to rule out other potential etiologies of the clinical presentation. 37 As in our case, patients with a trivial amount of air and coexisting comorbidities often require further imaging to rule out other etiologies.
Treatment and timeline of symptoms
This table highlights details of the procedure that was done in each of the reported cases, symptom onset, timeline of symptoms, and physical exam findings as well as the treatment modality that was used.
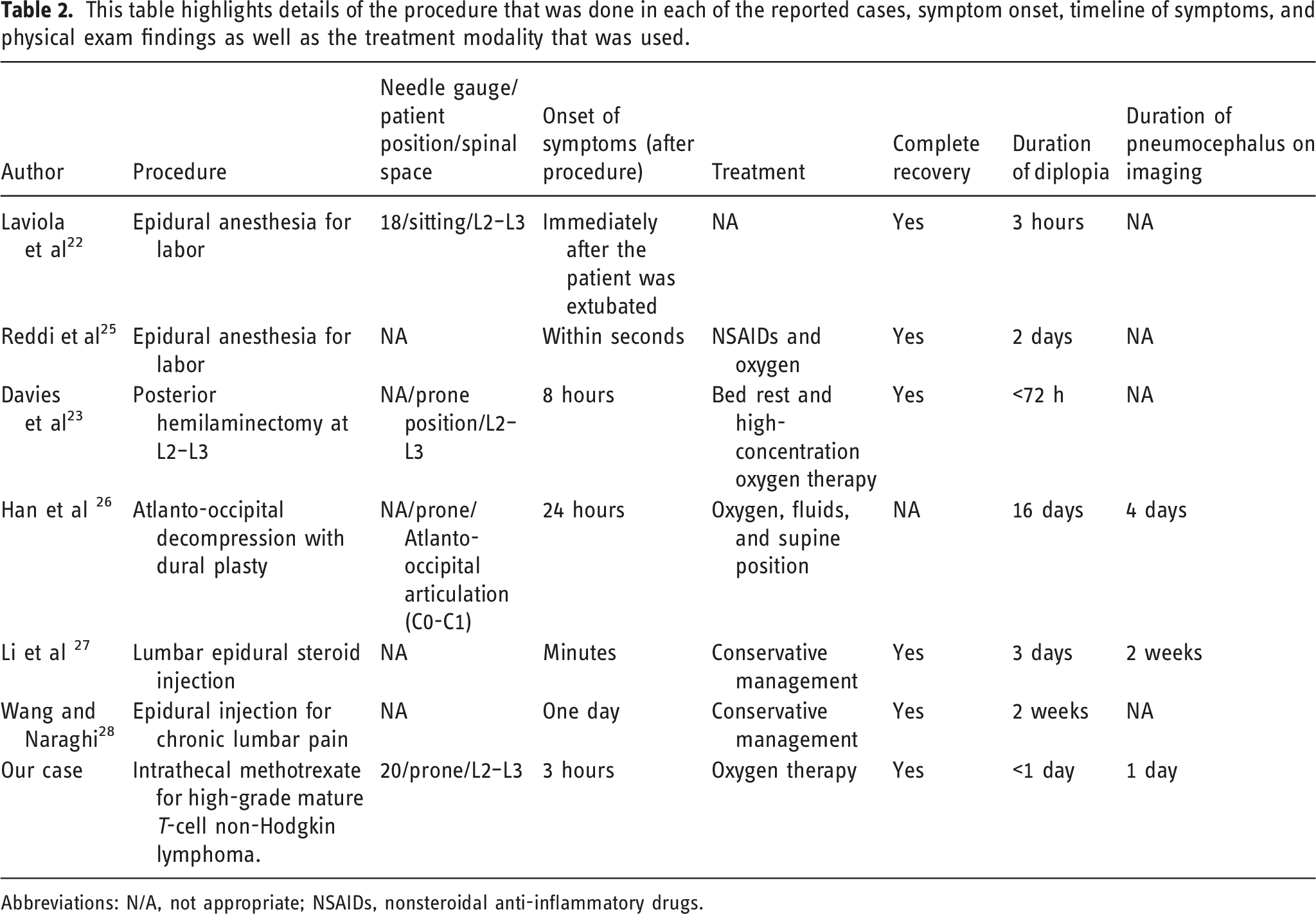
Abbreviations: N/A, not appropriate; NSAIDs, nonsteroidal anti-inflammatory drugs.
Conclusion
Pneumocephalus causing a cranial nerve palsy, such as abducens nerve, is a rare condition with only a few cases reported in the literature to date. This air entry into various structures of the central nervous system is most often secondary to various surgical and minimally invasive techniques, such as intrathecal injections. Its complications may be as trivial as headaches, to more complex presentations such a cranial nerve palsy, to exceedingly dangerous complications such as a tension pneumocephalus. Though the presentations vary, clinicians must maintain a high index of clinical suspicion and consider imaging studies for evaluation. A non-contrast CT scan of the head can be an effective and rapid diagnostic tool with treatment utilizing high oxygen airflow supplementation and conservative management of constitutional symptoms. Patients with more complex presentations concerning for tension pneumocephalus or those without resolution of symptoms in a timely fashion (i.e., hours to days) may require further imaging with MRI to assess for more insidious etiologies of cranial nerve palsies.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No institutional approval required for case reports.
Informed consent
The patient agreed on publishing this material.
Data availability
All data are available from the corresponding author upon reasonable request.