
Abstract
During COVID-19, conspiracy theories were intensely discussed in the media. Generally, both believing in conspiracy theories (i.e., explanations for events based on powerholders’ secret arrangements) and being confronted with a conspiracy theory have been found to predict cognition and behavior with negative societal effects, such as low institutional trust. Accordingly, believing in conspiracy theories around COVID-19 should reduce institutional trust, support of governmental regulations and their adoption, and social engagement (e.g., helping members of risk groups). We tested these predictions in a national random sample survey, an experiment, and a longitudinal study (N total = 1,213; all studies were preregistered). Indeed, believing in and being confronted with a COVID-19 conspiracy theory decreased institutional trust, support of governmental regulations, adoption of physical distancing, and—to some extent—social engagement. Findings underscore the severe societal effects of conspiracy theories in the context of COVID-19.
As COVID-19 was spreading around the world, so did conspiracy theories—that is, explanations for events based on powerholders’ secret, malevolent arrangements (Goertzel, 1994)—about the virus according to media reports (Gogarty & Hagle, 2020; Schulman & Siman-Tov, 2020). Some of these theories center on the origin of the virus, while others focus on the local or national reaction to the pandemic (Gogarty & Hagle, 2020). Believing in conspiracy theories is known to undermine prosocial behavior and trust in authorities (Imhoff et al., 2018; Jolley & Douglas, 2014b). Both are key to the successful fight against COVID-19. Indeed, the fight against this pandemic will, according to most experts (e.g., Chu et al., 2020), only be successful when most people adopt hygiene measures and physical distancing—thereby following governmental recommendations. Accordingly, the support of conspiracy theories is likely to endanger the success of efforts to fight the pandemic.
An investigation of the consequences of belief in a conspiracy theory related to COVID-19 on attitudes and behavior during the pandemic thus is of highest societal relevance and the main objective of the current research. Across one survey study with a national random sample, one experiment, and one longitudinal study, we examine the influence of the belief in and the confrontation with a conspiracy theory about the governmental reaction to COVID-19, the political COVID-19 conspiracy (PCC). More specifically, the PCC suggests that the powerful in one’s society are exploiting the pandemic to their advantage. Overall, our studies not only contribute to the understanding of conspiracy theories during the fight against COVID-19 but also to the understanding of effects of conspiracy theories in general, for instance, by advancing research on conspiracy theories through testing their consequences in an experiment and a longitudinal study—including analyses for a reversed direction of relations.
Effects of Conspiracy Theories
Conspiracy theories are built on the notion that a powerful group is acting in secret, thus building on (and potentially also creating) suspicion toward the powerful such as the government. Therefore, it is not surprising that a general conspiracy mentality (CM)—that is, the mental preparedness to belief in conspiracy theories (Imhoff & Bruder, 2014)—is negatively related with trust in experts and authorities (Imhoff & Lamberty, 2018; Imhoff et al., 2018). Being confronted with conspiracy theories, in addition, reduces the willingness to engage in joint societal efforts: For instance, being confronted with an anti-vaccine conspiracy theory decreased vaccination intentions (Jolley & Douglas, 2014a), and being confronted with a conspiracy theory about global warming reduced pro-environmental behavior (Van der Linden, 2015). Taken together, this suggests that in the context of COVID-19, believing in or being confronted with a PCC should undermine trust in the government and other authorities as well as prosocial attitudes and behaviors.
What attitudes and behaviors are likely to be affected by the belief in a conspiracy theory and are relevant in the context of COVID-19? First, trusting is closely related to agreement with the trustee’s arguments (e.g., Légal et al., 2012). Hence, a stronger belief in PCC should also lead to less support of governmental regulations in the context of COVID-19. Second, these regulations strongly require (among others) two types of behavior, namely, the adoption of hygiene measures and physical distancing. Whereas hygiene measures are a well-established means of health prevention, physical distancing has been a so far unfamiliar measure for societies at large. Consequently, those measures are applied out of different motivations: Hygiene measures are in line with intuitive responses to a health threat, whereas physical distancing requires trust in health officials. Accordingly, a stronger belief in PCC should lead to less physical distancing but not necessarily affect the adoption of hygiene measures. Indeed, first studies provide evidence that the belief in PCC is negatively related to behavior relevant for the containment of the COVID-19 pandemic in general (Imhoff & Lamberty, 2020; Teovanovic et al., 2020) and specifically to physical distancing (Biddlestone et al., 2020; Bierwiaczonek et al., in press). Finally, there was a wave of prosocial behavior related to the pandemic such as helping vulnerable people at high risk to deal with the situation (BBC, 2020; Vergin, 2020). Given that conspiracy beliefs have been shown to undermine prosocial behavior in other domains, the belief in PCC might also predict lower social engagement related to the pandemic.
In sum, we predicted that the belief in PCC leads to (i) lower institutional trust, (ii) lower support of governmental regulations, (iii) lower adoption of physical distancing (but not lower adoption of hygiene measures), and (iv) lower social engagement.
Overview of Current Research
So far, most research tested the relation between the belief in conspiracy theories and other variables, such as trust, using cross-sectional or correlational studies (e.g., Goertzel, 1994; Imhoff & Lamberty, 2018). More recently, experimental studies started to provide evidence for the effects of the confrontation with conspiracy theories with the aim to establish causality (e.g., Einstein & Glick, 2015; Jolly & Douglas, 2014a; Van der Linden, 2015). Longitudinal research that provides evidence for the effects of beliefs across time is very rare. The only exception we are aware of is a very recent article by Bierwiaczonek et al. (in press), demonstrating that the belief in COVID-19 conspiracy theories predicts lower physical distancing. Extending this work, we sought to test (i) whether this effect generalizes to trust in and support for governmental regulations, as well as social engagement, and (ii) whether the confrontation with a PCC results in the same effects.
Tackling these gaps and in order to provide a comprehensive test of our predictions, we conducted a cross-sectional correlational study using a random sample (Study 1), an experiment confronting participants with a PCC (Study 2), and a two-wave longitudinal study testing the predicted effects of belief in a PCC across time (and also the reversed order; Study 3).
Study 1: Survey Study
Method
Participants and Procedure
This preregistered study (https://aspredicted.org/ks4ch.pdf) was part of the weekly COVID-19 Snapshot MOnitoring in Denmark (COSMO Denmark; see http://dx.doi.org/10.23668/psycharchives.2795). Therefore, the sample size was not tailored to the current research question. Instead, a random sample of 5,000 people of the Danish adult population (for details, see Online Supplemental Material) was invited on March 30, 2020, via citizens’ official digital mail (e-Boks, see https://e-boks.com/danmark/en/) to complete an online survey set up via formr (Arslan et al., 2020) about COVID-19, which was completed by 775 respondents (15.5%). As preregistered, 344 participants were excluded from the analyses, because they worked in the health sector, are chronically ill, or had been infected by the virus, leaving a sample size of N = 425 (48.9% = male, 50.8% = female; M Age = 52.53, range = 20–84 years). According to a sensitivity power analysis, this sample size is sufficient to detect an effect of r = .173 with 95% power and of r = .135 with 80% power, respectively. Responses to all items were voluntary and participants were only included in the analyses when they responded to all items of a scale, which is why Ns vary slightly across analyses. A complete list of measures, further methodological details, and deviations from the preregistrations for all three studies are included in the Online Supplemental Material. All data and scripts are openly available under http://dx.doi.org/10.23668/psycharchives.4587 (data) and http://dx.doi.org/10.23668/psycharchives.4660 (scripts).
Measures
For internal consistency and descriptive statistics of each scale, see Table 1.
Internal Consistency, Mean, and Standard Deviation (SD) for All Scales in Study 1.
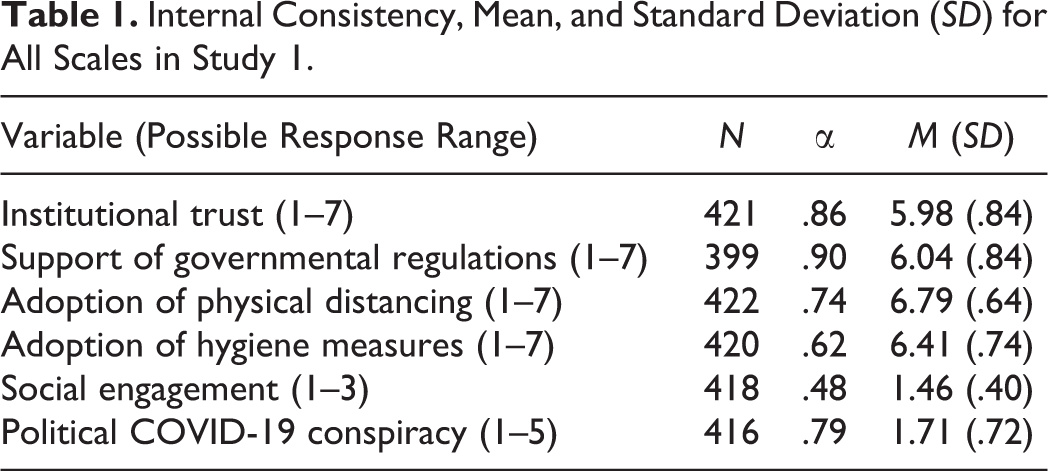
Institutional trust was assessed with five items measuring trust toward the police, state authorities, politicians, experts, and hospitals/doctors, respectively, on a 7-point scale from 1 = very low confidence to 7 = very high confidence.
Support of governmental regulations: Participants rated their perception of the appropriateness of 18 policies implemented by the Danish government to fight COVID-19 (e.g., “It makes sense that schools and day-care institutions are closed”) on a scale from 1 = disagree to 7 = agree.
Adoption of physical distancing was assessed by letting participants evaluate two behaviors aimed at keeping distance to other people on a 7-point scale from 1 = never to 7 = often (e.g., “I try to limit the amount of physical contact I have with others [e.g. handshakes, kisses on the cheek, hugs]).”
Adoption of hygiene measures was assessed regarding three behaviors communicated by health officials aimed at avoiding infection (e.g., “I make sure to cough or sneeze in my sleeve rather than in my hands”) on a 7-point scale from 1 = never to 7 = often.
Social engagement was assessed with five items (e.g., “Helping elderly, sick, or quarantined people with shopping or related tasks”) on a 3-point scale (1 = I’ve already done this, 2 = I plan to do this, and 3 = I do not plan to do this). The internal consistency of this scale and the adoption of hygiene measures were not satisfying, which could also not be improved by excluding items. Thus, results need to be interpreted with caution.
PCC items were inspired by news articles (e.g., Karni, 2020; NDR Kultur, 2020) and tweets (Kirk, 2020; Mitchell, 2020). Participants rated five items (e.g., “Powerful people are using COVID-19 in order to crash the economy”) on a 5-point scale from 1 = disagree to 5 = agree.
Results
We tested the hypothesized relation between PCC and all outcome measures in multiple regressions controlling for participants’ gender, children (yes/no), and education (see Table 2). Due to a high number of missing values (N = 164) and hereby deviating from our preregistration, we did not include age in these analyses. As hypothesized, people who believed to a stronger extent in the PCC reported lower institutional trust, lower support of governmental regulations, less adoption of physical distancing, and less social engagement. As further predicted, PCC was unrelated to the adoption of hygiene measures. Results including age as additional predictor showed the same effects, except for an nonsignificant prediction of social engagement (see Online Supplemental Material, Table S2).
Multiple Regressions for All Outcomes on Political COVID-19 Conspiracy (PCC), Gender, Children, and Education.

Discussion
This survey study provided first evidence for our hypothesis that the belief in PCC is related to lower institutional trust, support of governmental regulations, adoption of physical distancing, and social engagement. No relation was found between belief in PCC and adoption of hygiene measures. Given that the internal consistency of the social engagement scale was relatively low and that the effect of PCC on this outcome did not hold when only participants providing their age were included, this particular finding needs to be treated with caution. The low internal consistency might have resulted from the fact that we assessed prosocial behavior across very different domains, where adopting one behavior might exclude adopting another one (e.g., for time reasons). We altered this measure in Study 2 accordingly. Due to its cross-sectional design, the current study did not allow to draw any conclusions about causality. Therefore, we experimentally manipulated the confrontation with a PCC in Study 2.
Study 2: Experimental Study
Method
Participants and Procedure
We aimed to recruit 200 participants to be able to detect an effect of d = .40 (roughly the mean effect size across the four outcome measures in Study 1) at 80% power with α = .05. Participants were invited via a German university’s student mailing list on May 29, 2020, for participation in a short study about COVID-19. Of the 261 who completed the questionnaire, 19 participants were excluded, based on preregistered criteria (https://aspredicted.org/hg5a7.pdf), leaving N = 242 participants for the final sample (69.8% = female, 28.1% = male; M Age = 23.98, range = 18–61 years). Participation was not compensated. Due to unexpectedly quick responses, the sample size was slightly larger than planned.
After providing consent, participants in the PCC condition read about a fictitious conspiracy theory in the format of a news report. In this report, it was suggested that a big German company was using COVID-19 as a cover to ally with the government in order to implement digital medical data storage (see Online Supplemental Material). Participants considered the text as medium plausible (M = 3.29, standard deviation [SD] = 1.67, 7-point response scale from 1 = not at all to 7 = totally plausible). No text was given in the control condition. Afterward, the measures described below were administered. Participants in the experimental condition were then very thoroughly debriefed, after which the belief that the company was involved in a conspiracy theory was lower in the experimental versus control group, t(234.24) 1 = −2.17, p = .031, d = .28.
Measures
Items were similar to those in Study 1 but adapted to the German language and context. Descriptive statistics and internal consistency for all scales are reported in Table 3.
Internal Consistency, Mean, and Standard Deviation (SD) for All Scales in Study 2.
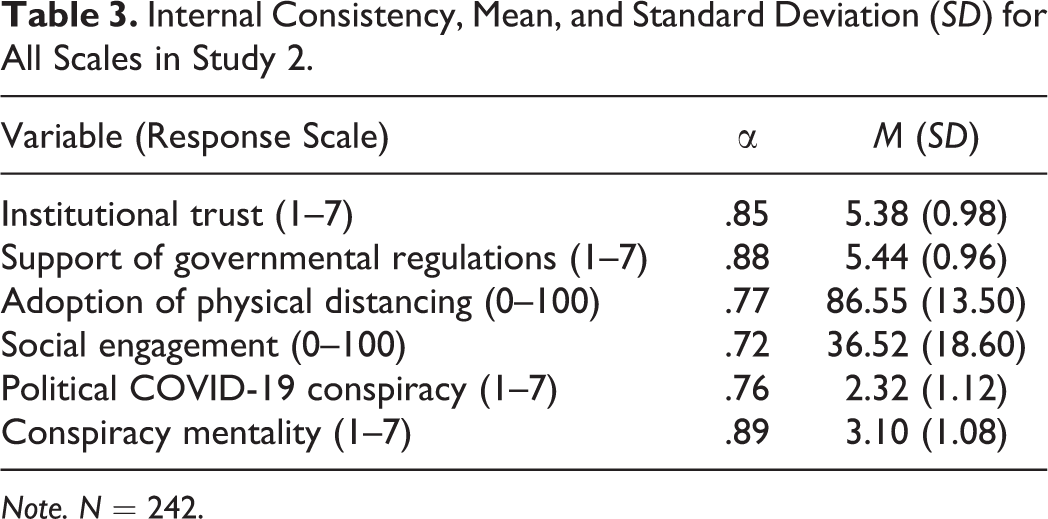
Note. N = 242.
Institutional trust was assessed with four items about trust in the federal and state ministries as well as federal institutions with a 7-point scale from 1 = really low trust to 7 = really high trust.
Support of governmental regulations: Participants indicated their support for 11 regulations implemented in Germany to fight the virus in case of another rapid spread (e.g., school closure; 1 = totally unacceptable to 7 = totally acceptable).
Adoption of physical distancing consisted of six items, two items used in Study 1 plus four additional items for better reliability (e.g., “Do not meet in big groups”), which were answered regarding another rapid spread using a slider from I would not do it (0%) to I would do it (100%).
Social engagement in case of another rapid spread was measured with seven items (e.g., “Offering to talk with people at risk”), four of them also included in Study 1, with a slider from 0% = I would not do it to 100% = I would do it. The substantial changes to this scale resulted in a higher internal consistency.
PCC was assessed with the same five items as in Study 1.
CM was assessed using the 12-item scale by Imhoff and Bruder (2014; e.g., “Those at the top do whatever they want”) from 1 = disagree to 7 = agree in order to explore whether the manipulation specifically affects the belief in PCC or also CM more generally.
Results
Manipulation Check
As intended, participants confronted with the conspiracy theory (M = 2.57, SD = 1.29) scored higher on the PCC scale than participants in the control group (M = 2.14, SD = 0.94), t(177.68) = 2.82, p = .005, 95% CIΔM [0.128, 0.721], d = 0.38. Regarding conspiracy mentality, the PCC group (M = 3.21, SD = 1.14) did not differ from the control group (M = 3.02, SD = 1.03), t(240) = 1.41, p = .159, 95% CIΔM [−0.078, 0.474], d = 0.17, suggesting that the confrontation affected the belief in PCC but not CM more generally.
Hypothesis Tests
We tested our hypothesis that being confronted with PCC leads to lower institutional trust, support of governmental regulations, adoption of physical distancing, and social engagement using independent sample t tests (Welch’s tests in cases where the variance differed between conditions, see Table 4). As hypothesized, participants in the PCC (vs. control) condition reported lower institutional trust, less support of governmental regulations, and less adoption of physical distancing. Contradicting our prediction, social engagement did not differ between conditions.
Means, Standard Deviations (SDs), and Test Statistic Comparing Experimental and Control Group in Study 2.
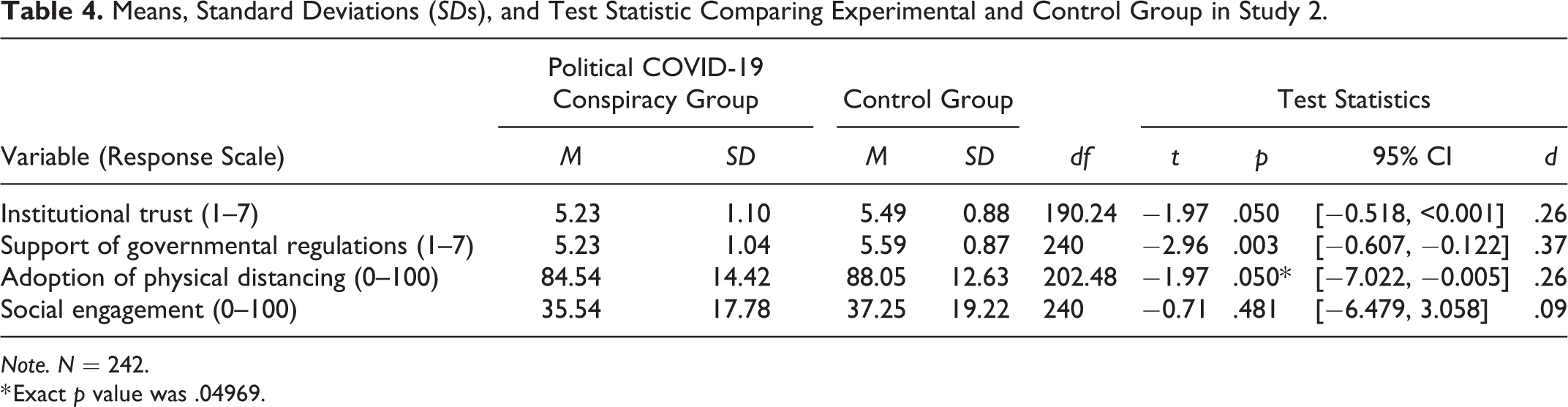
Note. N = 242.
* Exact p value was .04969.
Discussion
Results from this experiment largely replicate the results of the correlational Study 1. Individuals were affected by the confrontation with a PCC in the expected direction: less institutional trust, less support of governmental regulations, and less adoption of physical distancing, although the effects for adoption of physical distancing and institutional trust were on the margin of the conventional levels of significance (one p slightly smaller and one slightly larger than .05). It seems noteworthy that these consequences resulted from simply reading a short text about the mentioned conspiracy theory, though.
As a limitation, participants in the control condition did not read any text, which is an additional difference between conditions beside the confrontation with the conspiracy in the experimental condition and might thus have affected the results. However, additional analyses reported in the Online Supplemental Material (Table S11) showed that PCC carried large parts of the effect of the experimental manipulation. Therefore, we are confident that the results can be interpreted as an outcome of confrontation with the PCC.
Study 3 aimed to come as close as possible to the test of causal effects of the belief in (rather than the confrontation with) a PCC. To this end, we implemented a longitudinal design. In addition, we aimed to replicate the findings from Study 1 in a cross-sectional analysis.
Study 3: Longitudinal Study
Method
Participants and Procedure
Participants were invited during the first shutdown in Germany on March 24, 2020, via the student mailing list of a Germany university to fill in an online questionnaire in exchange for the chance of winning one of the twenty-five €10 gift cards. At Timepoint 1 (t1), we aimed to recruit 350 participants to be able to detect correlations of r = .15 at 80% power with α = .05. Due to unexpectedly quick responses, data collection was only stopped after 552 university students completed the study of which 546 (69.6% = female, 30% = male; M Age = 24.11, range = 18–61 years) fulfilled the preregistered inclusion criteria (for t1: https://aspredicted.org/w5hf5.pdf; for t2: https://aspredicted.org/m6pg3.pdf).
After providing informed consent, participants completed measures of institutional trust, support of governmental regulations, adoption of physical distancing, adoption of hygiene measures, social engagement, CM, and belief in PCC (for additional measures unrelated to the current hypotheses, see Online Supplemental Material). At the end of the questionnaire, participants could voluntarily provide their email address and consent to be invited for a second wave, which 194 participants did. Between May 15 and 28—when shops had reopened, but a lot of restrictions were still in place in Germany—150 participants took part in the second survey (t2), with 134 participants (15.7% = male, 83.6% = female; M Age = 24.18, range = 18–61 years) fulfilling the preregistered inclusion criteria. With the given sample size, the longitudinal analysis can detect an effect of f 2 = .059 (≈r = .24) with 80% power and α = .05 according to a sensitivity power analysis using G*Power (Faul et al., 2007). No substantial differences between this subgroup and the whole sample regarding the variables included in the analyses below occurred (for details, see Online Supplemental Material).
Measures
Table 5 provides information about descriptive statistics and internal consistency of the scales.
Internal Consistency, Mean, and Standard Deviation (SD) for All Scales at t1 (N = 546) and t2 (N = 134) in Study 3.
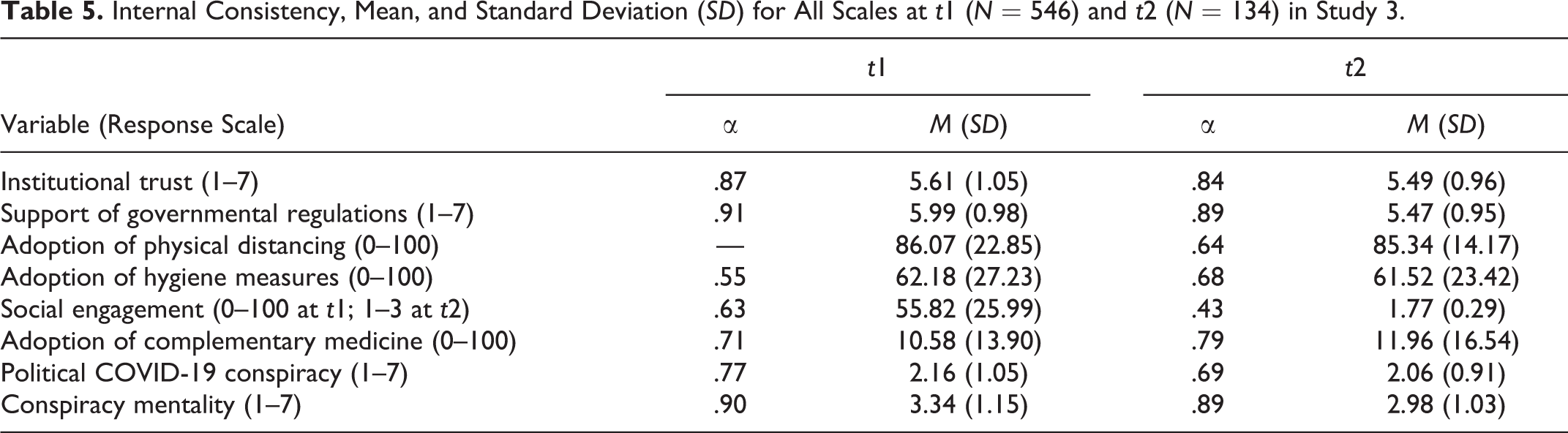
Institutional trust and support of governmental regulations were assessed with the same scales as in Study 2.
Adoption of physical distancing was assessed using one item at t1 (“Do not meet other people”). For t2, the same six items were used as reported in Study 2. Adoption of physical distancing, hygiene measures, and complementary medicine all used the same slider from 0 = I have not adapted to 100 = I have 100% adapted this behavior.
Adoption of hygiene measures was captured by three behaviors at t1 and five at t2 communicated by the Centers for Disease Control and Prevention (2020) and its German equivalent, the Robert Koch Institute (2020; e.g., “In case you have to sneeze: Cover your mouth and nose with a tissue”), which resembled the hygiene items used in Study 1 but considers differences between recommendations in Denmark and Germany.
Adoption of complementary medicine: For exploratory purposes, we also asked about behavior changes that are implemented to avoid a COVID-19 infection with eight behaviors that have no scientifically proven impact in fighting the virus (adapted from Betsch et al., 2020; e.g., “Drinking ginger tea”). Similar questions are part of the prepping behavior measure by Imhoff and Lamberty (2020), which contained items about the reliance on alternative remedies.
Social engagement was measured with four items at t1 (e.g., “Could you imagine to socially engage during the pandemic by running errands for members of the risk population?”) with a slider from 0 = not willing to engage to 100 = willing to engage. At t2, the same seven items as in Study 2 (including the four items from t1) were used, and this time measured on a 3-point scale (would not do it, would do it, and already have done it) to also include self-reported behavior in the indicator.
CM and PCC were assessed using the same scales as in Study 2.
Results
Cross-Sectional Analysis
As in Study 1, we computed bivariate correlations between PCC and the outcome measures at t1 (see Table 6). People who believed stronger in the PCC trusted institutions less, supported governmental regulations less, and reported less physical distancing as well as social engagement. Adoption of hygiene measures was unrelated to the belief in PCC. These results are consistent with the results of Studies 1 and 2. They should, however, be considered as exploratory, due to deviations from our preregistration regarding scale composition (for details, see Online Supplemental Material, especially Table S13).
Bivariate Correlations Between the Political COVID-19 Conspiracy (PCC) Scale as Well as Conspiracy Mentality (CM) Scale and Outcomes Assessed at t1 (N = 546) in Study 3.
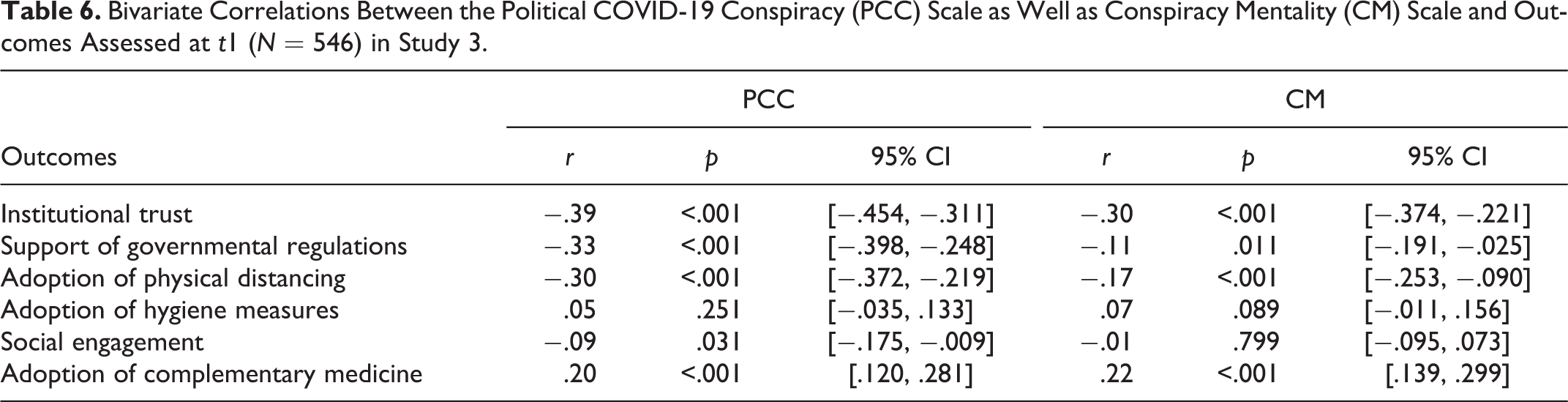
Additional exploratory analyses indicate that the belief in PCC was positively related to the adoption of complementary medicine. Moreover, the correlations between CM and the outcome measures match those for belief in PCC, except that CM does not correlate with social engagement.
Longitudinal Analysis
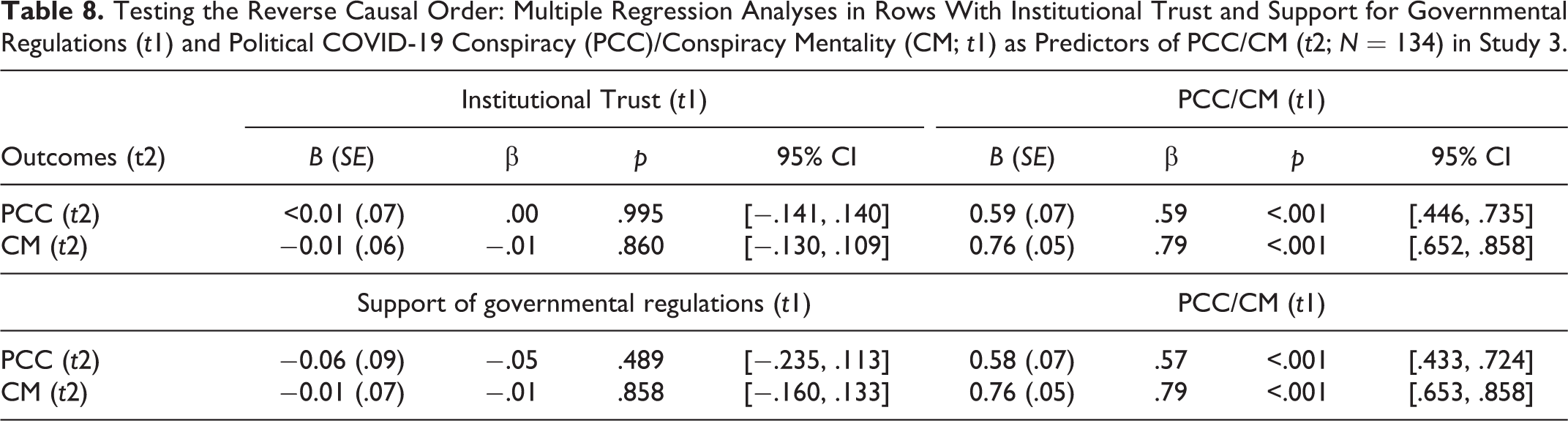
Next, we tested our hypotheses using the cross-lagged prediction of each outcome measure at t2 by PCC at t1, controlling for the respective outcome at t1 using separate linear regressions (see Table 7). As hypothesized, PCC predicted lower institutional trust and (marginally) also lower support of governmental regulations. Different to our hypotheses, PCC at t1 did not predict the adoption of physical distancing and social engagement at t2. Additional exploratory tests for the reverse direction of the relation (i.e., regressing PCC-t2 on PCC-t1 and institutional trust-t1 or support of governmental regulations-t1) did not provide evidence for the prediction of PCC from institutional trust or support of governmental regulations (see Table 8). Thus, the belief in PCC seems to affect institutional trust and support of governmental regulations rather than the other way around.
Multiple Regression Analyses in Rows With Political COVID-19 Conspiracy (PCC; t1) and Criterion (t1) as Predictors of Criterion (t2; N = 134) in Study 3.
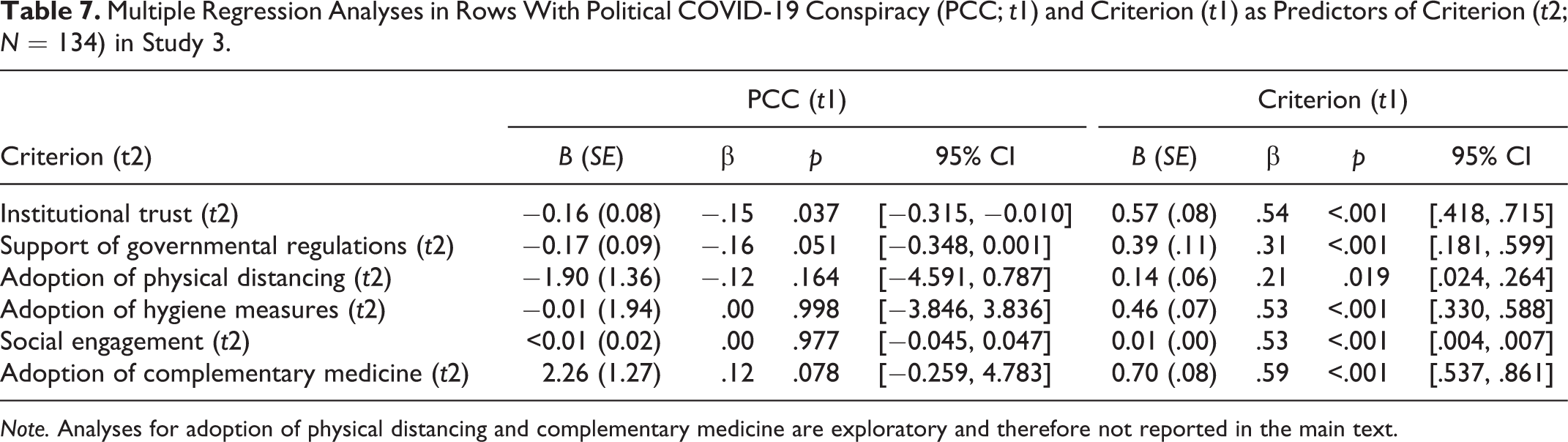
Note. Analyses for adoption of physical distancing and complementary medicine are exploratory and therefore not reported in the main text.
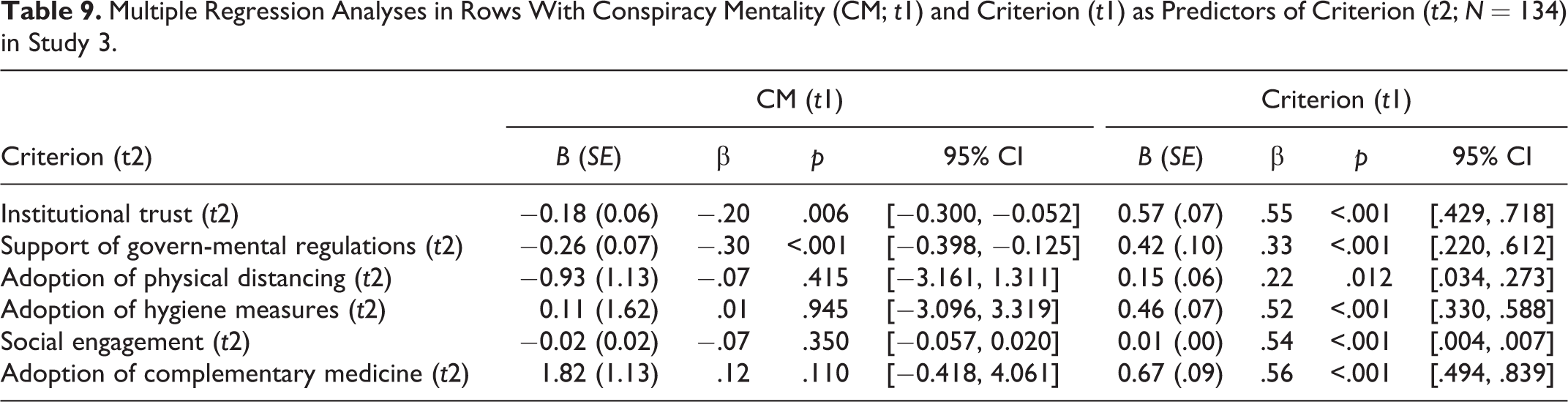
When entering CM at t1 as predictor for exploratory purposes, it likewise predicted institutional trust and support of governmental regulations, but no evidence for the reverse direction of the relation occurred (see Tables 8 and 9), suggesting that both concepts have similar longitudinal effects.
Testing the Reverse Causal Order: Multiple Regression Analyses in Rows With Institutional Trust and Support for Governmental Regulations (t1) and Political COVID-19 Conspiracy (PCC)/Conspiracy Mentality (CM; t1) as Predictors of PCC/CM (t2; N = 134) in Study 3.
Multiple Regression Analyses in Rows With Conspiracy Mentality (CM; t1) and Criterion (t1) as Predictors of Criterion (t2; N = 134) in Study 3.
Discussion
The current results replicated the findings from Study 1 and added that PCC positively predicted higher adoption of complementary medicine as well as that all outcome measures except social engagement showed the same correlation pattern with CM. Moreover, PCC and CM predicted trust and support for governmental regulations, as well as marginally the adoption of complementary medicine, but not adoption of physical distancing and social engagement across time. No evidence for reverse cross-lagged effects was found. The lack of predicted significant effects for some of the outcomes in the longitudinal analyses might be due to a lower sample size at t2 or due to the low internal consistency of the Social Engagement Scale. The lack of a relation between PCC/CM and the adoption of physical distancing and social engagement over time might result from situational changes (the shutdown had been lifted between both measurement points). Alternatively, these behaviors might be rather stable (similar to habits) and, thus, barely any changes across time occur, which would be required to find an effect in the reported analysis.
In addition to the results reported here, we explored the effect of another conspiracy theory, namely, that the virus was intentionally created by humans in China (see Online Supplemental Material, Table S12). Given that belief in one conspiracy theory is highly correlated with the belief in other—sometimes even contradictory—conspiracy theories (Bruder et al., 2013; Swami et al., 2010; Wood et al., 2012), one might assume that the China-related conspiracy theory should assert the same effects as PCC, but correlations were substantially lower. This suggests that conspiracy theories might assert mainly an effect in the domain they are about, but this needs to be tested in future research.
General Discussion
The current research examined the relation between the belief in PCC and societally important attitudes as well as (self-reported) behaviors in the context of COVID-19. We tested the hypotheses that the belief in PCC asserts a negative influence on institutional trust, support for governmental regulations, adoption of physical distancing, and social engagement, but not on the adoption of hygiene measures in a survey study with a random sample, an experimental study, and a longitudinal study—all preregistered—conducted in two different European countries. Given that effects in some studies did not reach conventional levels of significance, we summarize the results in Figure 1. Based on effect sizes and p values, the effects in Study 2 and the longitudinal analysis of Study 3 are weaker, which is further not surprising, given that the influence of third variables and reversed directions of relations are not accounted for in Study 1. Across studies, PCC predicted less institutional trust, less support for governmental regulations, and (to a somewhat lesser extent given the results of the longitudinal analysis in Study 3) also less adoption of physical distancing. The borderline effects (i.e., p > .03) in these cases can, given the overall pattern, most likely be attributed to the random variance of effect sizes rather than to the nonexistence of the respective effect. Moreover, PCC clearly did not predict the adoption of hygiene measures. For social engagement, no clear evidence for a relation to PCC was found. In sum, our hypotheses regarding institutional trust, support for governmental regulations, adoption of physical distancing, and (with a null effect) for hygiene measures were supported.
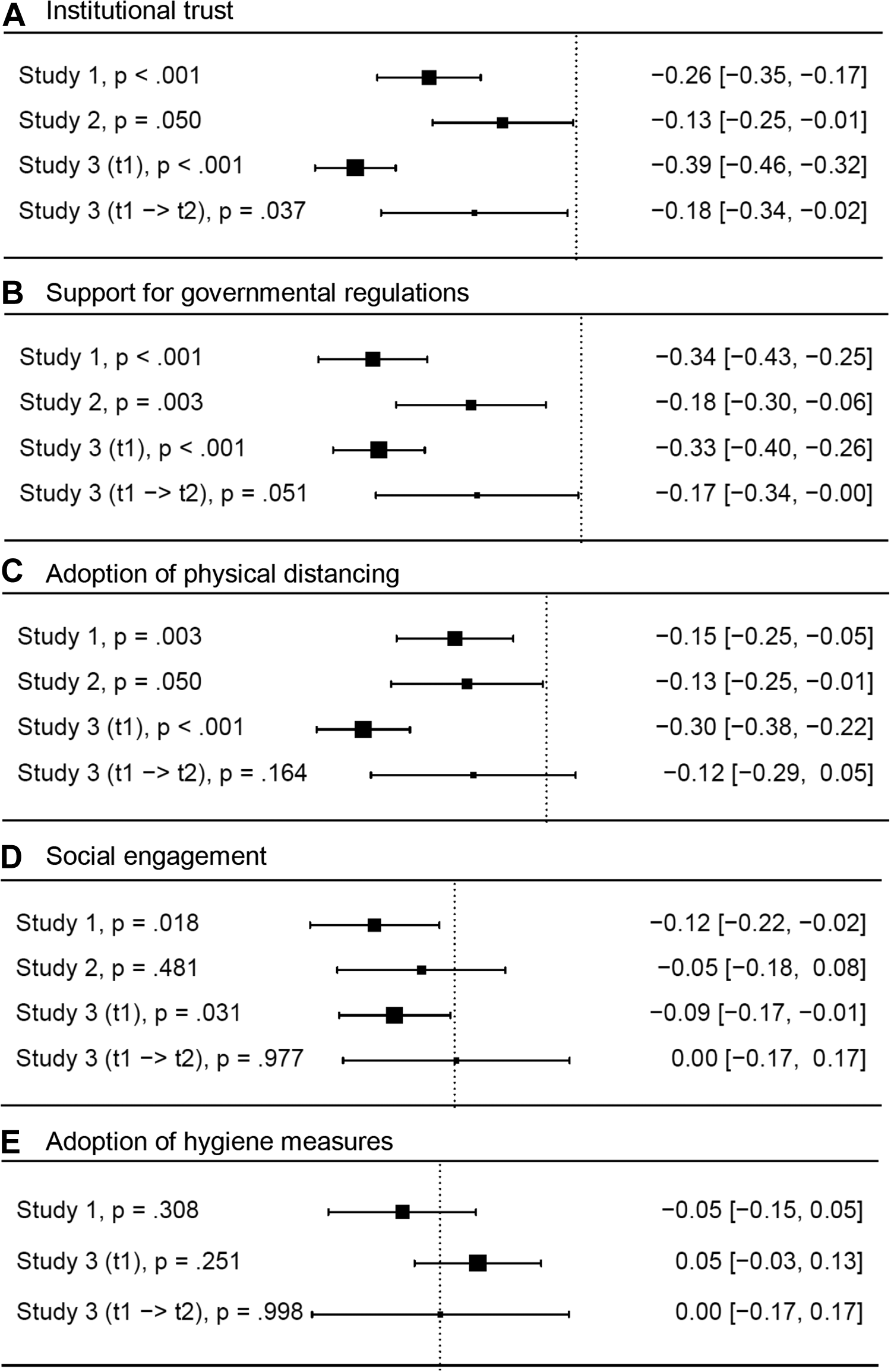
Relation between political COVID-19 conspiracy and outcomes variables across all studies. Effect sizes transformed to r with 95% confidence interval. (A) Institutional trust. (B) Support for governmental regulations. (C) Adoption of physical distancing. (D) Social engagement. (E) Adoption of hygiene measures.
A number of additional findings are worth noting. First, CM also predicted institutional trust and support for governmental regulations, but none of the other measures. This indicates that considering the belief in specific conspiracy theories is worthwhile, given that PCC predicted different outcomes than the more general concept of conspiracy mentality. Second, as low institutional trust might also be the cause of lower support of governmental regulations and the adoption of behavior implied by these regulations, we preregistered and tested whether institutional trust mediates those effects of PCC. Considering all results, we found no convincing support for this mediation because no evidence was found in those analyses testing effects of PCC (for details, see Online Supplemental Material, Table S14). Further research should explore additional possible concepts underlying the effects of PCC.
The results extend existing research on the negative effects of conspiracy theories on societally relevant behavior by showing that such effects also occur in the context of COVID-19. Going beyond earlier research, our results suggest that PCC (a) asserts a causal effect (e.g., compared to Imhoff & Lamberty, 2020) and (b) predicts trust and support for governmental regulations (but not individual health behaviors), and not only adoption of physical distancing (compared to Bierwiaczonek et al., in press). Thinking about the implications, the finding that being only confronted with a conspiracy theory can undermine institutional trust, support of governmental regulations, and adoption of physical distancing suggests that media coverage sharing conspiracy theories might counteract the fight against the virus. Given the importance of successfully fighting new COVID-19 infections, gaining the summarized insides for this specific context is a relevant contribution in itself.
The current set of studies also advances the research about conspiracies in general. The most important contribution in this respect is the demonstration that the confrontation with and the belief in conspiracy theories are related and show the same pattern of effects. We combined—to our knowledge, for the first time—experimental and longitudinal research on PCC in a certain context and found equivalent results, even though believing in a conspiracy is very different from reading about it for the first time. This raises the question whether being convinced of a conspiracy is crucial or whether the mere knowledge about it has similar effects, which should be addressed by future research.
Second, Study 3 is among the few longitudinal studies testing the effect of conspirational thoughts across time. The findings of this study advance our knowledge about the effects of conspiracy theories, in particular because we find effects of PCC and CM across time, but not for the reversed temporal relation. Given that this is only one study, further research replicating this pattern regarding societal and other outcomes is needed.
Clearly, the current research also has some limitations. First, one methodological limitation is that the sample size of the longitudinal data set was not ideally suited for (re)testing the small to medium effects we found for some of the outcome measures in Studies 1 and 2. The overview of effect sizes suggests that a highly powered longitudinal study might also have found effects on the adoption of physical distancing and potentially also on social engagement. Second, our findings concern a political conspiracy theory surrounding COVID-19, thus around the topic of a health and global crisis. It is an open question whether the findings might generalize to other pandemics and health-related issues and (especially) to conspiracy theories surrounding other issues. Also, the COVID-19 conspiracy and our measurements were political in nature; thus, there might have been an influence of, for example, ideology and other political attitudes that were not considered herein.
To conclude, the current research advances our knowledge about conspiracy theories, by demonstrating that the confrontation with and the belief in conspiracy theories are associated with less institutional trust and lower support for and adoption of regulations put forward by these institutions. This advances research on conspiracy beliefs by showing parallel effects for confrontation with and believing in conspiracies. In the context of the COVID-19 pandemic, the current findings imply that the spread of a political COVID-19 conspiracy undermines the attitudes and behaviors related to a successful mitigation of the spread of COVID-19.
Supplemental Material
Supplemental Material, sj-pdf-1-spp-10.1177_19485506211000217 - Conspiracy Theories and Their Societal Effects During the COVID-19 Pandemic
Supplemental Material, sj-pdf-1-spp-10.1177_19485506211000217 for Conspiracy Theories and Their Societal Effects During the COVID-19 Pandemic by Lotte Pummerer, Robert Böhm, Lau Lilleholt, Kevin Winter, Ingo Zettler and Kai Sassenberg in Social Psychological and Personality Science
Footnotes
Acknowledgment
The authors thank Carl Leonhard Walzer for his contributions to Study 2.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: Parts of the reported research have been supported by a grant by the Deutsche Forschungsgemeinschaft to the last author (DFG: SA800/17-1).
Supplemental Material
The supplemental material is available in the online version of the article.
Note
Author Biographies
Handling Editor: Igor Grossmann.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.