
Abstract
Purpose
This study aimed to identify potential impinging and shear stress-inducing factors in knees with medial meniscus posterior horn horizontal tears (MMPHHT) using magnetic resonance imaging (MRI) in middle-aged patients with meniscal degeneration.
Materials and Methods
We retrospectively analyzed and compared consecutive patients with MMPH signal changes or MMPHHT on MRI from January 2015 to January 2022. After 1:1 propensity score matching, 80 patients in each group were analyzed. Bony impinging factors, including the femoral condylar offset ratio, the ratio of posterior condylar offset (PCO) to tibial width, posterior medial tibial plateau concavity, and the medial tibial slope, were assessed. Soft tissue impinging factors, such as the MMPH coverage ratio, presence of medial femoral condyle focal cartilage defects or posterior tibial osteophytes, were also analyzed.
Results
Demographic data did not differ between MMPHHT and MMPH signal change groups. MMPHHT group showed increased medial tibial slope (5.33 ± 2.05° vs 4.21 ± 2.58°, P = .003), higher incidence of posterior medial tibial plateau concavity (P = .040), greater MMPH coverage ratio (0.43% ± 0.05% vs 0.41% ± 0.04%, P = .022), and more posterior tibial osteophytes (P = .012). Multivariate logistic regression identified higher medial tibial slope (OR = 1.288, P = .016), MMPH coverage ratio (OR = 1.369 × 104, P = .020), and posterior tibial osteophytes (OR = 4.525, P = .009) as independent factors associated with MMPHHT.
Conclusion
In conclusion, we have determined several anatomical contributing factors related to MMPHHT. Such factors may be useful in understanding the progression of meniscus degeneration in early OA knees. Furthermore, addressing correctable factors during surgery such as tibia slope correction or osteophytectomy may improve repair results of MMPHHT in the future.
Introduction
Medial meniscus posterior horn horizontal tears (MMPHHT) are the most common type of meniscal tear with an incidence ranging from 12% to 40% among all meniscus tears.1,2 They are likely to occur in individuals over 40 years old with underlying degenerative changes, often in the absence of a distinct traumatic event. Pain during flexion, locking, and altered tibiofemoral contact mechanics make MMPHHT a clinically important entity, particularly in the context of osteoarthritis (OA) continuum. Despite the high prevalence and clinical significance, the exact mechanisms and pathophysiology of MMPHHT remain largely unknown. This lack of knowledge hinders the development of optimal preventive, surgical, and rehabilitative strategies. 3
Medial meniscus posterior horn horizontal tears are largely degenerative and are presumably caused by a combination of cumulative axial loading and rotational forces that generate shearing forces on the meniscus. Suganuma et al. 4 proposed a potential tear inducing mechanism using dynamic magnetic resonance imaging (MRI), suggesting that MMPHHT results from posteromedial tibiofemoral incongruence (PMTFI), a form of “cam impingement” that occurs during full flexion. While PMTFI provides a dynamic explanation for the shear stress experienced by the MMPH during full flexion, static factors contributing to shear stress are relatively unknown.5,6
Some anatomical changes that induce shear force in the presence of a compressive load during weightbearing have been reported.7,8 Moon et al. 9 recently reported that MMPHHT are associated with increased posterior tibial slope, while Barber et al. 10 reported that complex MM tears are associated with biconcave medial tibial plateau. We hypothesized that MMPHHT are associated with surrounding anatomical changes that contribute to impingement of the MMPH, consequently generating shearing forces between the superior and inferior meniscus tear leaflets of MMPHHT. The aim of this study was to identify potential impinging and shear stress-inducing factors in knees with MMPHHT via MRI in middle aged patients between 40 and 65 years with meniscus degeneration.
Materials and Methods
Study Design
This study was designed as a single-center, case-control study. All data acquisition and analysis were conducted under the approval of our institutional review board (AJOUIRB-DB-2023-057) which waived the requirement for informed consent from the patients owing to the retrospective nature of the study.
From January 2015 to January 2022, consecutive radiological data of patients who underwent knee MRI for chronic knee pain in our outpatient clinic were retrospectively reviewed. Patients who had MMPH degenerative changes in knee MRI between the ages of 40 and 65 years were included. Patients with the following conditions were excluded: (1) Kellgren-Lawrence (K-L) grade ≥ 3 osteoarthritis, (2) Inflammatory arthritis, (3) Previous traumatic injury of the knee joint, (4) Surgical history of the affected knee, (5) Meniscal pathology other than MMPHHT, including MM posterior root tear or meniscus tears elsewhere than MMPH, and (6) Lotysch grade II MMPH changes (linear areas of hyperintensity not extending to articular surface).
Radiographic assessment
All MRI images were acquired on a 1.5T MR unit (Discovery MR750W; GE Healthcare, Waukesha, WI) using a transmit-receive quadrature knee coil (GE Healthcare). MRI scans included sagittal T1 FS(TR/TE = 710/9, slice thickness = 3 mm, field of view = 160 mm), sagittal T2 FS(TR/TE = 3824/75, slice thickness = 3 mm, field of view = 160 mm), sagittal PD FS(TR/TE = 1800/25, slice thickness = 3 mm, field of view = 160 mm), coronal T2 FS(TR/TE = 2331/70, slice thickness = 3 mm, field of view = 160 mm), and axial PD FS(TR/TE = 1800/25, slice thickness = 3 mm, field of view = 160 mm).
Magnetic resonance imaging grading of the medial meniscus was evaluated using the method described by Lotysch et al. 11 Medial meniscus signal change (Lotysch grade 1) was defined as increased focal intensity with no extension to the articular surface. Lotysch grade 2 changes, defined as horizontal linear signals not contacting the articular surface, were excluded from this study due to its potential representation of normal radial tie fibers of the meniscus rather than degenerative tears. 12 MMPHHT (Lotysch grade 3) was defined as a horizontal linear signal that contacts the articular surface.
Potential bony-impinging factors
Potential bony-impinging factors affecting MMPH include a relatively larger posterior medial femoral condyle (MFC), posterior medial tibial plateau concavity, and an increased tibial slope.9,10,13 Posterior condylar offset (PCO) was measured in the MRI scans by identifying the sagittal longitudinal axis of the femur on a central sagittal scan, translating it to the posterior femoral cortex, and then identifying the center of the MFC on an axial scan. From this sagittal section, the shortest distance of each tangent along the posterior cortex to the most posterior extent of medial condyle was defined as PCO.14,15 Femur diaphyseal width was measured 5 cm above the joint line on a central sagittal scan. Femoral condylar offset ratio was calculated by dividing the PCO by the diaphyseal width (
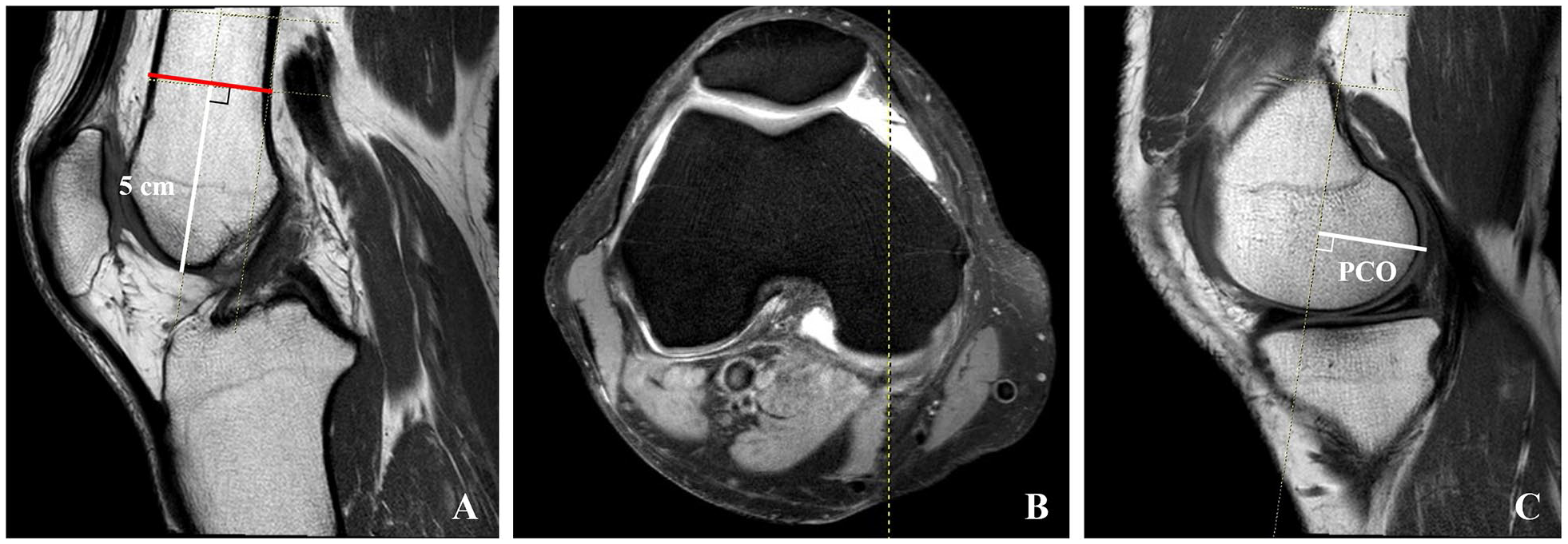
Method of measurement of femur diaphyseal width and posterior condylar offset (PCO).
Medial tibial slope was measured by the method of Hudek et al.
16
An initial midline sagittal image outlining the tibial attachment of the Posterior cruciate ligament (PCL) was selected. A first circle was drawn tangent to the proximal, anterior, and posterior tibial borders, and then a second circle was drawn centered on the circumference of the first circle. The MRI-longitudinal axis was defined by a line that connected the centers of 2 circles. MTS was defined as the angle between the medial tibial plateau and a line perpendicular to the longitudinal axis of the tibia (
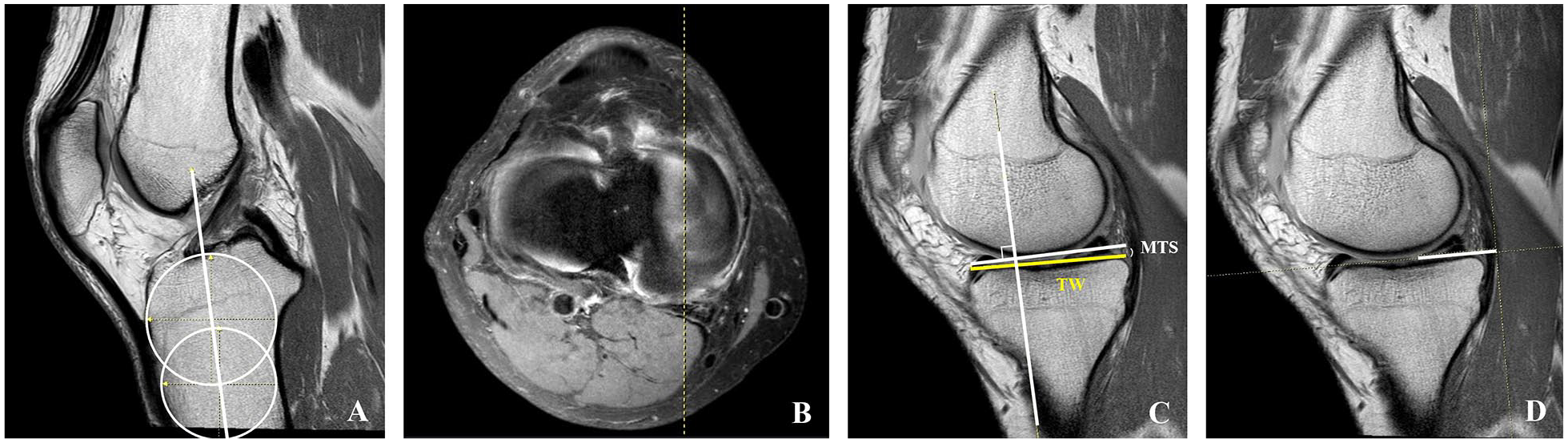
Method of measurement of medial tibial slope (MTS), tibial width (TW), and medial meniscus posterior horn (MMPH) coverage ratio.
A posterior medial tibial plateau concavity is defined as a concave anatomical feature of the tibial surface located inferior to the MMPH. The presence of posterior medial tibial plateau concavity was evaluated on sagittal MRI views along the cartilage margin (
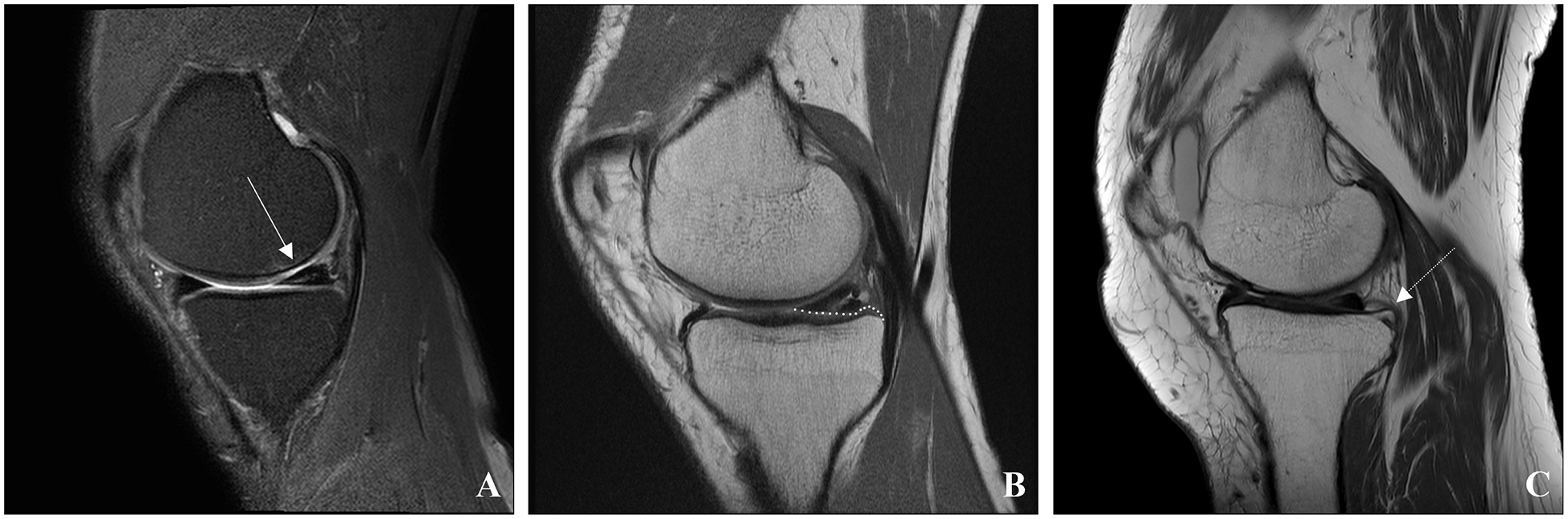
MRI image on a sagittal scan of medial femoral condyle (MFC) focal cartilage defect (
Potential soft tissue impinging factors
Potential soft tissue impinging factors including MFC focal cartilage defects, osteophytes on the posterior articular surface of the tibia, and increased tibial coverage of the MMPH were evaluated in the MRI scans (
Posterior tibial osteophytes may hinder posterior translation of MMPH during flexion. Posterior tibial osteophyte was defined as a posterior tibial osteophyte in contact with posterior aspect of the MMPH.
Increased MMPH tibial coverage may increase the relative area of potential impingement. The MMPH tibial coverage was measured as the length in parallel with the tibial slope from the semimembranosus to the anterior edge of MMPH at the sagittal section at the level where the medial meniscus is the longest in an axial cut. The MMPH tibial coverage ratio was defined as the MMPH coverage divided by the TW (
Medial femoral condyle focal cartilage defects may induce shear stress on the overlying superior surface of MMPH. MFC focal cartilage defects were considered if there were cartilage defects of more than 50% thickness of the MFC cartilage (International Cartilage Repair Society [ICRS] grade 3-4). All radiographic measurements were performed using the Picture Archiving and Communication Systems (PACS: Carestream Health, Rochester, New York, USA).
Statistical analysis
For continuous variables, independent t-tests were used to compare groups. For non-continuous variables, either the chi-square test or Fisher’s exact test was performed. Statistical analysis was performed using R, version 3.6.3. The level of significance was set at P < .05. To mitigate confounding effects of age, sex, and K–L grade, 1:1 propensity score matching was performed using a nearest-neighbor matching algorithm. Power analysis was performed using G*Power (version 3.1.9.7) with a confidence level of 95% (α = .05) and a power (1 − β) of 80%, resulting in a minimum requirement of 70 patients for each group based on a previous study. 9
Intraobserver and interobserver reliability
Intraobserver and interobserver reliability were assessed using intraclass correlation coefficients (ICC) for continuous variables, while categorical features were evaluated using linear weighted kappa statistics. Two observers conducted their assessments in a blinded fashion, with the first observer performing a second measurement after 4 weeks to assess intraobserver reliability. For categorical variables, the first measurement from the first observer was used for analysis, while for continuous variables, the average of the 2 observers’ measurements was used. For ICC and kappa, values below .2 were considered to indicate poor agreement, values between .21 and .40 as fair, .41 to .60 as moderate, .61 to .80 as good, and values above .80 as excellent. For radiographic measurements, intraobserver ICC and kappa values ranged from 0.860 to 0.976, and interobserver values ranged from .720 to .931, showing good to excellent consistency.
Results
A total of 95 patients with MMPH signal changes and 80 patients with MMPHHT were enrolled in the study. After performing 1:1 propensity score matching, each group consisted of 80 patients with comparable demographic characteristics, as summarized in Table 1 .
The Demographic Data.
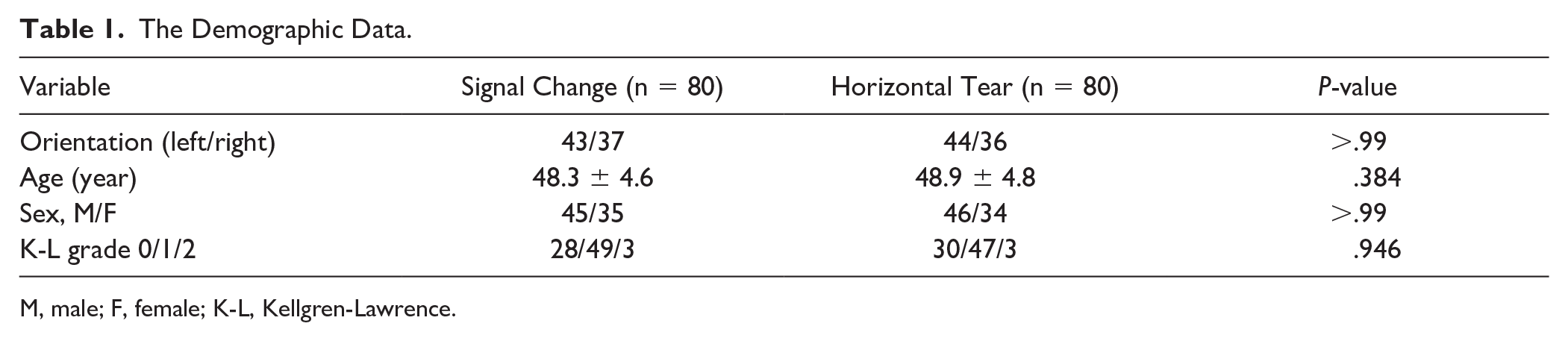
M, male; F, female; K-L, Kellgren-Lawrence.
As for bony impinging factors, the femoral condylar offset ratio and the ratio of PCO to TW did not show significant differences between the 2 groups (P = .661 and P = .256, respectively). MMPHHT group, however, exhibited a significantly higher MTS (P = .003) and higher incidence of posterior medial tibial plateau concavity (P = .040) compared with the MMPH signal change group ( Table 2 ).
Possible Bony Impinging Factors in 2 Groups.
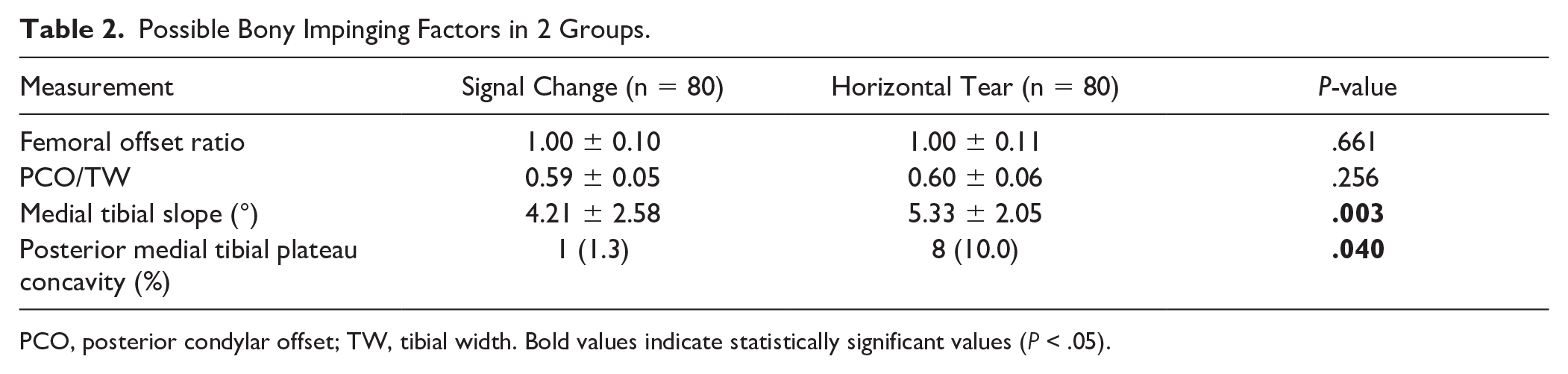
PCO, posterior condylar offset; TW, tibial width. Bold values indicate statistically significant values (P < .05).
As for soft tissue impinging factors, the incidence of MFC focal cartilage defects showed no significant difference between the MMPH signal change and MMPHHT groups (P = .232). MMPHHT group, however, exhibited a higher MMPH coverage ratio (P = .022) and higher incidence of posterior tibial osteophytes (P = .012) compared with the MMPH signal change group ( Table 3 ).
Possible Soft Tissue Impinging Factors in 2 Groups.

MMPH, medial meniscus posterior horn; MFC, medial femoral condyle.
Univariable logistic regression analysis identified significant factors associated with MMPHHT, that included higher MTS (OR = 1.234, P = .004), higher MMPH coverage ratio (OR = 4.797 × 10³, P = .025), presence of posterior tibial osteophytes (OR = 4.048, P = .009), and presence of posterior medial tibial plateau concavity (OR = 8.778, P = .043). Multivariable logistic regression analysis further confirmed that higher MTS (OR = 1.288, P = .016), higher MMPH coverage ratio (OR = 1.369 × 104, P = .020), and the presence of posterior tibial osteophytes (OR = 4.525, P = .009) were significant independent contributing factors of MMPHHT ( Table 4 ).
Univariable and Multivariable Logistic Regression Analysis of Contributing Factors for Medial Meniscus Posterior Horn Horizontal Tears.
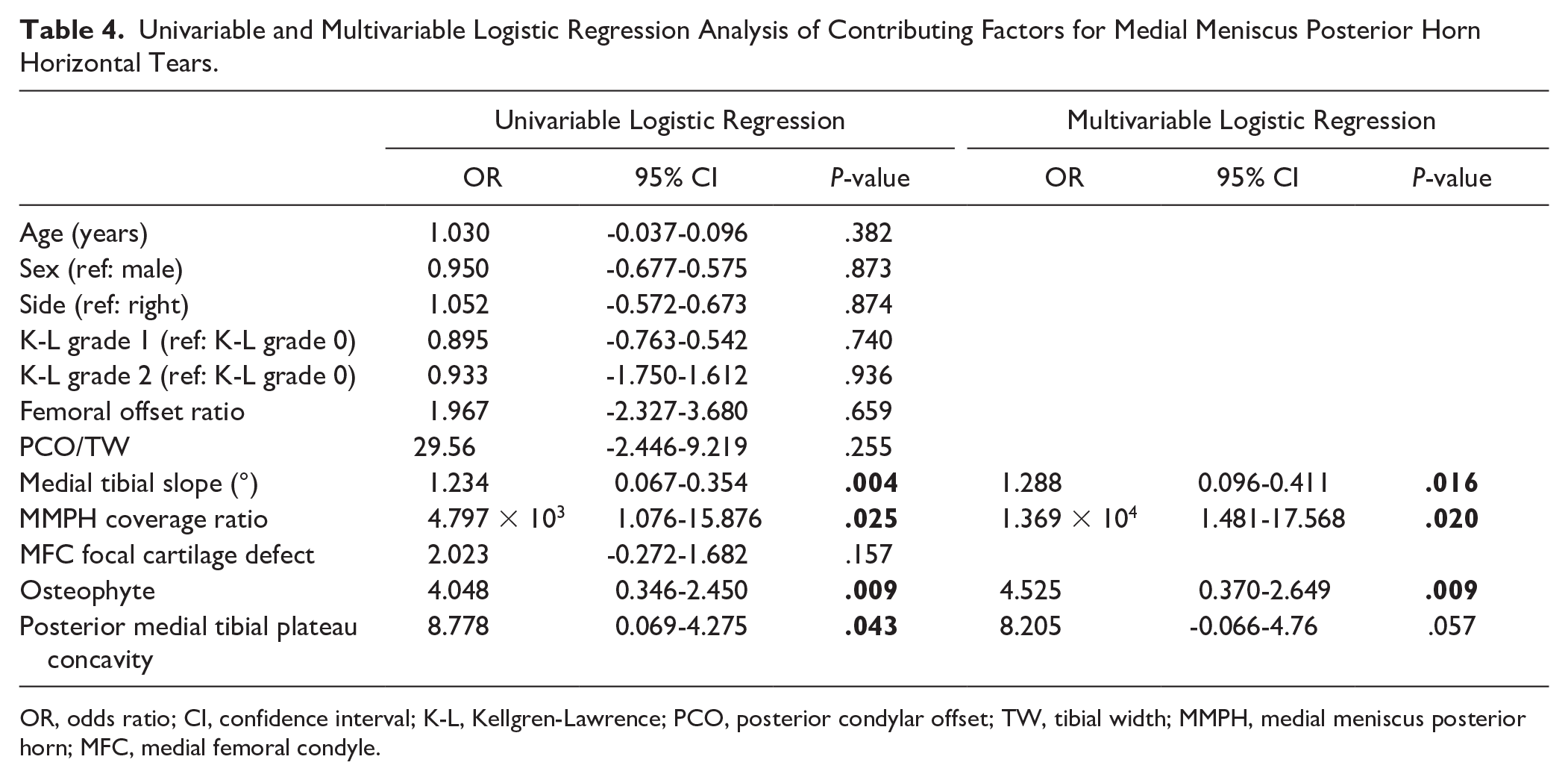
OR, odds ratio; CI, confidence interval; K-L, Kellgren-Lawrence; PCO, posterior condylar offset; TW, tibial width; MMPH, medial meniscus posterior horn; MFC, medial femoral condyle.
Among the 80 MMPHHT patients, 14 received arthroscopic partial meniscectomy. A total of 8 out of 14 operated meniscus showed paradoxical movement of the superior leaflet during arthroscopy, that is, anterior translation during knee flexion and posterior translation during knee extension (

Medial meniscus posterior horn horizontal tear (MMPHHT) showing paradoxical movement of the superior leaflet during arthroscopy.
Following partial meniscectomy for the MMPHHT, paradoxical movement is observed: during knee flexion, the superior leaflet translates anteriorly while the inferior leaflet translates posteriorly. Conversely, during knee extension, the superior leaflet translates posteriorly, and the inferior leaflet translates anteriorly.
Discussion
The aim of this study was to determine possible impinging and shear stress inducing factors in knees with MMPHHT via MRI in middle aged patients with meniscus degeneration. We have found that bony impinging factors such as increased MTS and posterior medial tibial plateau concavity, together with soft tissue impinging factors such as higher MMPH coverage ratio, and posterior tibial osteophytes are associated with MMPHHT. Based on our results, we can speculate that these factors contribute to horizontal tear progression in degenerated MMPH.
Reasoning behind anatomical impingement factor selection and potential effects to tear progression are as follows. Two main forces have been identified to cause MMPHHT, compression and shear tension.
17
We therefore examined anatomical factors that could increase local compressive forces, as well as shearing stress on MMPH. Higher PCO may induce a cam impingement like effect of MMPH during flexion, as proposed by Suganuma et al.
4
Increased MTS is also known to cause increased compressive forces on MMPH during weightbearing.
18
During knee flexion, the MMPH normally translates posteriorly to avoid impingement. A higher MMPH coverage ratio places a larger tissue area under compressive loads even during knee flexion.
19
Posterior medial tibial plateau concavity may reduce MMPH mobility and disrupt congruency, potentially leading to trapping of the MMPH during flexion and subsequent MMPHHT formation. Posterior tibial osteophytes situated near the postero-inferior border of the MMPH, can also directly hinder normal posterior translation during knee flexion in a similar fashion. Focal cartilage defects overlying MMPH are associated with meniscus tears, potentially affecting meniscus movement due to shearing forces during knee range of motion.
20
In all, we propose a potential mechanisms in which such factors impinge and create a shear stress, resulting in the distinctive MMPHHT tear pattern (
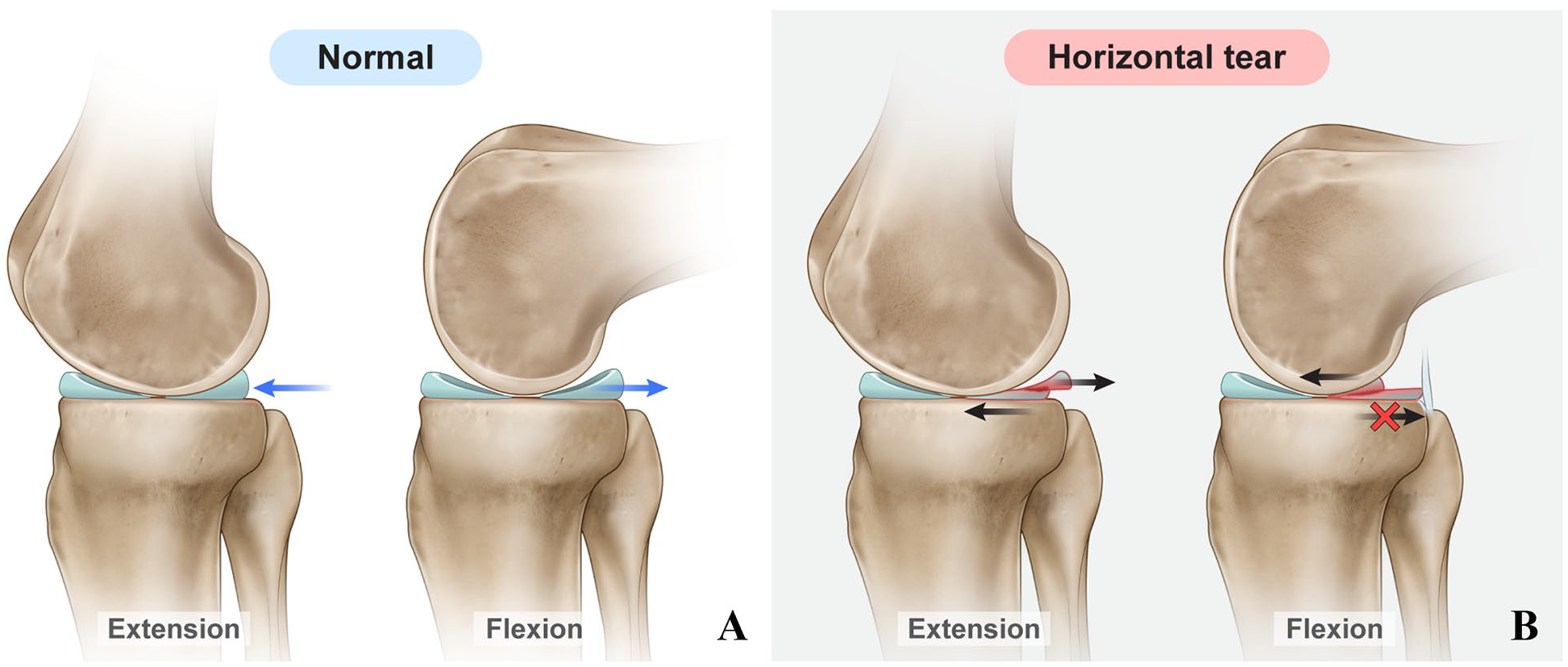
Schematic illustration of medial meniscus posterior horn (MMPH) movement in normal and horizontal tear conditions.
Previous studies have discussed several anatomical factors associated with MMPHHTs. As for increased MTS, Moon et al. 9 found that increase slope is associated with an increased incidence of MMPH tears. In addition, Giffin et al. 7 found that an increased MTS leads to greater anterior displacement of the tibia, resulting in a higher likelihood of MMPH tears. In contrast, Khan et al. 6 reported that MMPH tears were associated with a shallower MTS. Our data shows an association between increased MTS and MMPHHT, similar to studies done by Moon et al. and Griffin et al. As for tibial osteophytes, several studies have reported that medial tibial osteophytes are associated with medial meniscus tears or medial meniscus extrusion.21,22 Such relationship was also evident in our data, possibly due to the restriction of MMPH posterior translation during flexion. Posterior tibial osteophytes only reach superiorly half of the cross-sectional height of the MMPH, matching the horizontal tear site in sagittal images of MRI, further supporting the potential shear stress caused by the posterior osteophytes obstructing posterior meniscus translation.
Posterior medial tibial plateau concavity is an anatomical feature similar to the biconcave medial tibial plateau, but is confined to the tibia plateau below the MMPH. Barber et al. 10 demonstrated the association between biconcave medial tibial plateau with complex MM tears through arthroscopy and MRI. Posterior medial tibial plateau concavity may reduce MMPH mobility and disrupt joint congruency. In the present study, posterior medial tibial plateau concavity was identified as a contributing factor to MMPHHT albeit not a significant factor in the multivariate analysis.
Therefore, its impact appears to be less influential compared with MTS, MMPH coverage ratio, and posterior tibial osteophytes. During knee flexion, increased contact between the femoral posterior condyle and the meniscus leads to greater hoop stress within the meniscus. It is presumed that a larger radius of the posterior condyle results in increased compressive forces on the meniscus. According to Wang et al., 13 a larger radius of the medial femoral posterior condyle is associated with MMPH root tears. Conversely, Khan et al. 6 reported that a smaller posterior condyle radius is related to MMPH tears. In the present study, no significant differences were observed between the groups in femoral condylar offset ratio or PCO. As for MFC cartilage defects, Ji et al. 23 demonstrated a significant increase in compressive stresses in the femoral cartilage, meniscus, and tibial cartilage with an 8-mm defect in the MFC at 0°, 30°, 60°, and 90° of knee flexion through a finite element study. While this study reported the impact of MFC focal cartilage defects on the meniscus, the causal relationship between cartilage defects and MMPHHTs is still unclear. In this study, no significant difference in MFC focal cartilage defects was observed between the 2 groups, suggesting that the influence of this factor may be less substantial compared with others.
Overall, among the various factors hypothesized to contribute to increased compressive and shearing forces on the MMPH, those related to the tibia rather than the femur emerged as significant contributing factors toward MMPHHTs. One possible explanation for the significant association between tibial factors and MMPHHT lies in the distinct anatomical roles of the tibia compared with the femur. Anatomically, the medial meniscus is firmly anchored to the tibia through its anterior and posterior roots, as well as the meniscotibial ligaments. 24 This robust structural attachment allows mechanical forces transmitted through the tibia to be directly imposed on the meniscus. In contrast, the femur primarily interacts with the meniscus through articulation without a fixed attachment, resulting in a more dynamic and less forceful relationship. Therefore, tibial factors are likely to have a greater impact on meniscal tears than femoral factors.
Clinical significance of this study concerns treatment of MMPHHT. Several studies attempted to repair MMPHHT via various suture techniques, yet the clinical results have been mixed. According to Shanmugaraj et al., although clinical outcomes between meniscectomy and MMPHHT repair are reported to be similar, the complication rate for MMPHHT repair was higher at 12.9%. The most common complication was healing failure, necessitating a secondary meniscectomy. 25 However, Pearsall et al. 26 reported that MMPHHT repair offers superior biomechanical advantages, including increased contact area and reduced peak contact pressure. In addition, it may be more favorable in preventing OA progression. 27 Nevertheless, MRI evaluations have shown that the healing of MMPHHT repairs is poorer compared with that of vertical meniscal tear repairs. Our results may offer several correctable factors during repair, such as increased tibial slope, or posterior osteophytes. Correction of tibial slope by selective high tibial osteotomy or osteophytectomy may reduce impingement and shear stress on MMPH, potentially improving clinical results and decreasing retear rates after repair. 28 We are currently examining the clinical results of MMPHHT repairs after such corrections. Furthermore, our results contribute to the understanding of degeneration progression of meniscus in OA knees. Little is known regarding the natural history and contributing factors of degeneration progression of meniscus, from intrameniscus high signal intensity to MMPHHT. Our results offers some important anatomical changes in the posterior medial knee regarding MMPHHT which is valuable in understanding changes in early OA.
This study has several limitations. First limitation concerns the analyzed groups, where we compared MMPHHT (Lotych grade III) with MMPHs with intrameniscal high signal intensity (Lotych grade I) rather than normal MMPHs. “Normal anatomy” knees are difficult to define and vary significantly according to age, sex, and ethnicity, especially within the MRI data available in the clinical setting. We concentrated on analyzing factors that contribute to MMPHHT in OA knees, factors that may have contributed the intrameniscal high signal intensities to progress toward horizontal cleavage tears. The inclusion of “normal anatomy” knees may overstate factors that contribute to early OA changes rather than the tear itself. Lotych grade II menisci were also excluded from analysis, as the liner signal may represent radial tie fibers of the meniscus rather than actual tears. 12 Second, the static MRI factors analyzed in our study have not been validated in a dynamic model. A few studies have used dynamic MRI in the evaluation of MMPH tears and have reported favorable outcomes when meniscus repair is combined with decompression in cases of cam impingement.4,29 While we have provided arthroscopic images of impingement and paradoxic movement of leaflets in select patients undergoing partial meniscectomy, further studies using dynamic MRI, cadaveric or animal models are required to visualize and quantify impingement and shear stress of each factor on MMPHHT. In that sense, a cause-effect relationship cannot be established among the MRI factors and MMPHHT.
Conclusion
In conclusion, we have determined several anatomical contributing factors related to MMPHHT. Such factors may be useful in understanding the progression of meniscus degeneration in early OA knees. Furthermore, addressing correctable factors during surgery such as tibia slope correction or osteophytectomy may improve repair results of MMPHHT.
Footnotes
Acknowledgment and Funding
This research was supported by National Research Foundation (NRF) funded by the Korean Government (MSIT) (2023R1A2C1007200 (D.Y.P.)). This work was supported by the Korean Fund for Regenerative Medicine (KFRM) grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Health & Welfare) (grant no. 22C0601L1 (D.Y.P.))
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions Statement
S.L., J.Y.C., and D.Y.P. conceived and designed the study. S.L. and D.Y.P. took the lead in writing the manuscript. S.L., J.Y.P., and H.W.Y. collected the clinical data. S.L., J.Y.C., J.Y.P., S.N., and D.Y.P. contributed to the statistical analysis. S.L., J.Y.C., H.W.Y., S.N., and D.Y.P. contributed to the interpretation of the results. All authors agree with the content in the submitted manuscript. Critical revision and final approval were done by all authors.
Ethics Statement
This study was designed as a single-center, case-control study. All data acquisition and analysis were conducted under the approval of our institutional review board (AJOUIRB-DB-2023-057) which waived the requirement for informed consent from the patients owing to the retrospective nature of the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.