
Abstract
Objective
The purpose of the study was to determine average tensile forces resulting in suture failure while tying a knot during repair of complete radial meniscus tears and to compare the failure tensile force based on meniscus tissue location: the peripheral (red-red) versus inner (white-white).
Design
This study was designed as a cadaveric biomechanical study using 24 menisci harvested from fresh frozen cadaveric knees with midbody radial tears. Tears were repaired using 2-0 nonabsorbable suture in both the inner meniscus and the peripheral meniscus. A force gauge was used to measure the tension of a surgeon’s knot until failure of either the suture or the meniscus tissue. Statistical analysis was performed comparing suture failure tensile forces between inner and peripheral sutures using 2-sample t test.
Results
Suture repairs primarily failed due to meniscal tissue cut-out after suture tensioning (96%). There was no statistical difference in failure mode between medial and lateral meniscus for both the inner (100% cut-out) and the peripheral (92% cut-out; P = 0.703) sutures. The peripheral sutures failed as significantly higher loads (54 ± 26 N) than the inner sutures (36 ± 11 N, P = 0.006). The peripheral meniscus tissue tolerated significantly higher tension at failure (36 ± 7 N) than the inner meniscus (26 ± 7 N, P < 0.001).
Conclusion
When tying parallel sutures to repair a radial meniscus tear, suture tensile forces above 30 N may tear through meniscus tissue. Surgeons should not use suture tying forces above 30 N when repairing radial meniscus tears with parallel sutures. The peripheral meniscus can withstand higher knot-tying forces than the inner meniscus, so surgeons should consider tying the peripheral suture before the inner suture.
Introduction
Meniscus tears are one of the most common orthopedic injuries. 1 Common meniscal tear types include radial, horizontal, longitudinal, and root tears. 1 Radial meniscus tears can have a more damaging impact on knee biomechanics than other tears and have been found in 15% of patients with meniscal tears. 2 Radial tears are typically vertical cleavage tears that arise at the inner (white-white) zone and extend outward to the periphery of the meniscus (red-red) disrupting the circumferential collagen fibers, leading to loss of the hoop tension function resulting in a nonfunctional meniscus.1,3,4 These tears cause increased contact pressure and improper load transferring capability of the meniscal tissue due to decreased surface area and anatomic gapping of the meniscal cartilage.3,5,6 Repair of these tear types is recommended since untreated radial meniscus tears can lead to early osteoarthritis. 7 In the past, radial meniscus tears were treated with both conservative and surgical options, typically involving partial and total meniscectomies. 8 The inner (white-white zone) of the meniscus is generally avascular with limited regenerative capabilities; therefore, meniscectomies were historically used to treat tears in this region.1,9,10 Meniscectomies do not come without consequence as they can lead to early articular cartilage degeneration and knee osteoarthritis progression.
There has been a recent trend shifting toward repairing radial tears to promote meniscal tissue healing and to restore the load transferring ability of the meniscus. 3 The parallel suture technique was traditionally used to repair radial tears; however, various repair techniques have been utilized recently such as the cross stitch and rebar techniques. 11 Radial tears in the red-red zone or periphery of the meniscus have a better probability of healing due to greater vascular supply than tears located in inner portion or white-white zone.3,12,13 Because of this known anatomic characteristic, there has been an increased emphasis among surgeons to encourage peripheral meniscus healing by direct surgical repair, rather than menisectomy. 14
All-cause meniscus repair failure rates have been described as ranging from 5% to 25% at 5 years after meniscus repair.10,15-17 One study describes a failure rate of 20.8% (5/24) for radial meniscus tear repairs.5,15 Currently, the most common surgical techniques used to repair radial meniscus tears are the inside-out, all-inside, and transtibial repair techniques.18-20 The surgical technique utilized depends on the size, location, type of tear, and surgeon preference. 4 Recent studies have demonstrated that the all-inside technique with parallel sutures may demonstrate a less invasive technique that may also improve strength of the radial meniscus repair and decrease failure rates.1,15 There are many described mechanisms of meniscus repair failure using the all-inside repair technique, including tissue failure resulting in suture cut-out or suture failure.1,21,22
While there are many studies evaluating the failure of meniscus repair after it has been repaired, there is limited evaluation of tissue failure at the time of knot tying intraoperatively. This study’s purpose was to determine the average tensile forces that result in suture failure while tying a suture knot during the repair of complete radial meniscus tears. A secondary objective of this study was to compare the failure tensile force based on meniscus tissue location: peripheral (red-red zone) region versus the inner (white-white) region. The hypothesis was that the peripheral tissue would be able to sustain a higher tensile force than the inner tissue before repair failure.
Methods
Specimen Preparation
This study was a cadaveric biomechanical study; therefore, it did not require Institutional Review Board approval. In total, 19 medial and 19 lateral menisci were dissected and extracted from 19 fresh frozen cadaveric knees and preserved for testing. These meniscus specimens were examined for quality and any meniscus with tissue damage was excluded from the study. Twenty-four fresh frozen menisci (9 lateral and 15 medial menisci) were selected for quality from 19 human knee specimens. The selected menisci were thawed for 24 hours prior to testing. Measurements of the meniscus were obtained using a caliper (Shars Tools, St. Charles, IL). The meniscus length, lateral thickness, inner width, and outer width were measured in millimeters for both the medial and the lateral meniscus specimens (
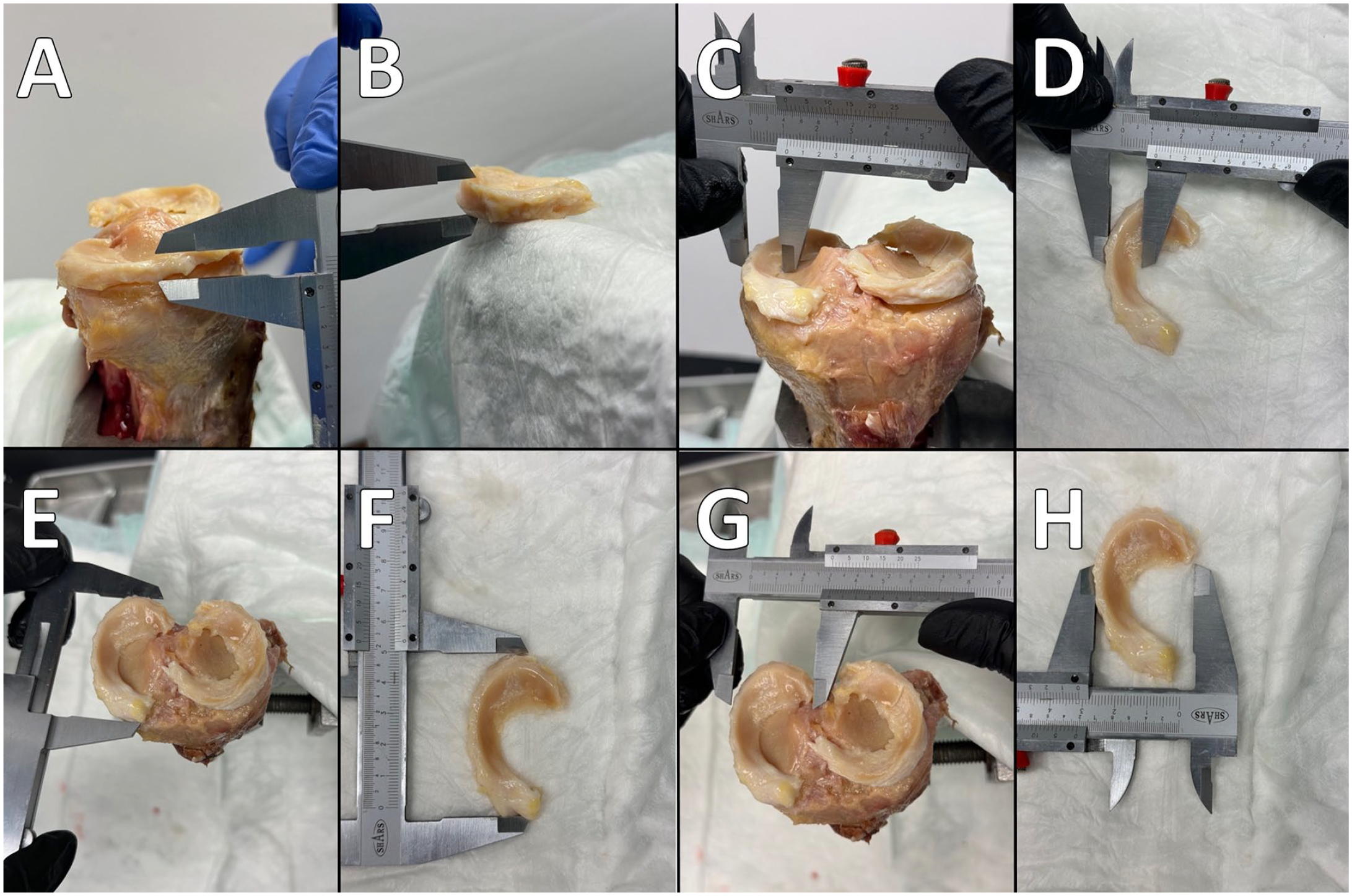
Demonstration of measuring the meniscal specimen. (
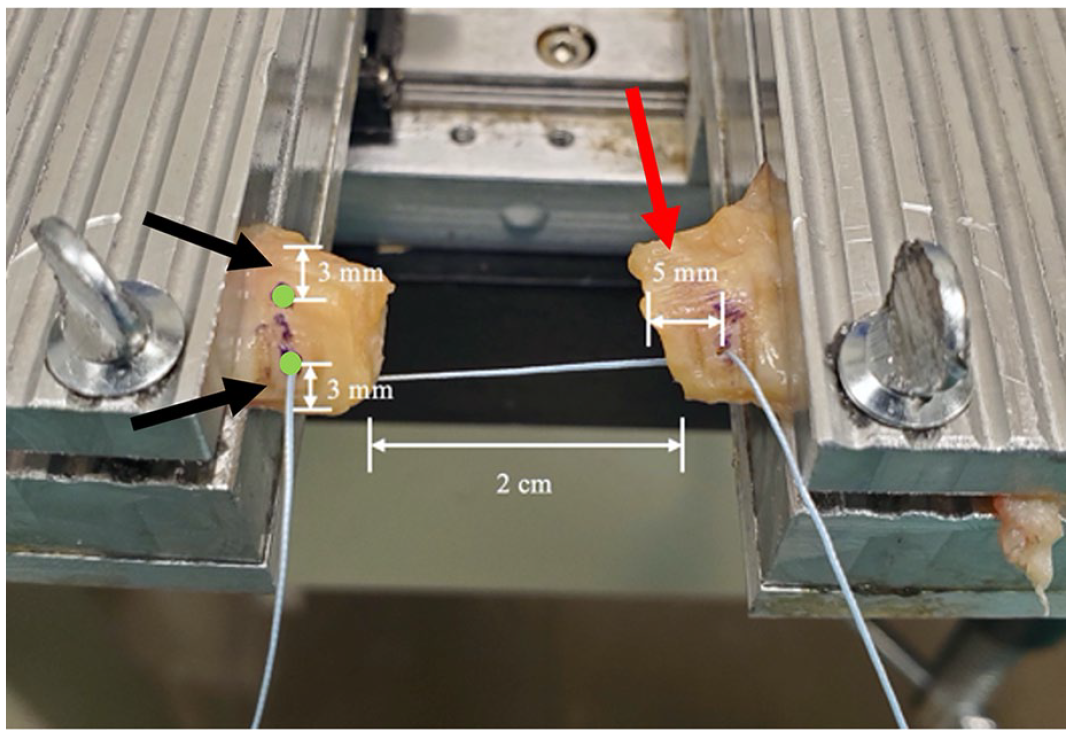
The sutures in both the inner (white-white) region and peripheral (red-red) region were positioned 5 mm from the radial cut edge of the specimen segment (red arrow). The peripheral suture was placed 3 mm from the peripheral edge of the meniscus specimen, and the inner suture was placed 3 mm from the meniscus free edge (black arrows). Suture positions are marked (green dots). A tear gap of 2 cm was created.
Repair Technique
For this study, an all-inside repair technique was used and nonabsorbable 2-0 sutures (Arthrex, Naples, FL) were deployed in the 2-parallel suture technique using a knee-specific suture passer (Arthrex, Naples, FL). Two 2-0 sutures were used per specimen. The sutures in both the inner (white-white) region and the peripheral (red-red) region were positioned 5 mm from the radial cut edge of the specimen segment. The peripheral suture was placed 3 mm from the peripheral edge of the meniscus specimen, and the inner suture was placed 3 mm from the meniscus free edge (
Testing
The peripheral and inner sutures were tested and tensioned independently. For each test, 2 needle drivers were used during testing and each needle driver was clamped to the free end of the suture (
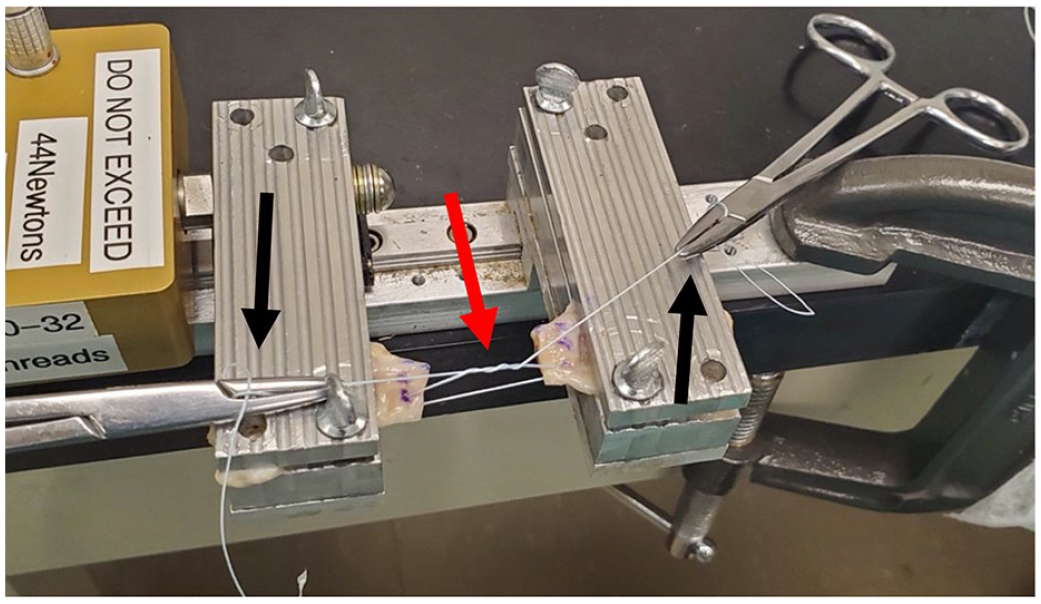
Testing configuration prior to suture tensioning. A loose surgeon’s knot was tied in a single suture (red arrow) and suture ends were gripped with needle drivers (black arrows).
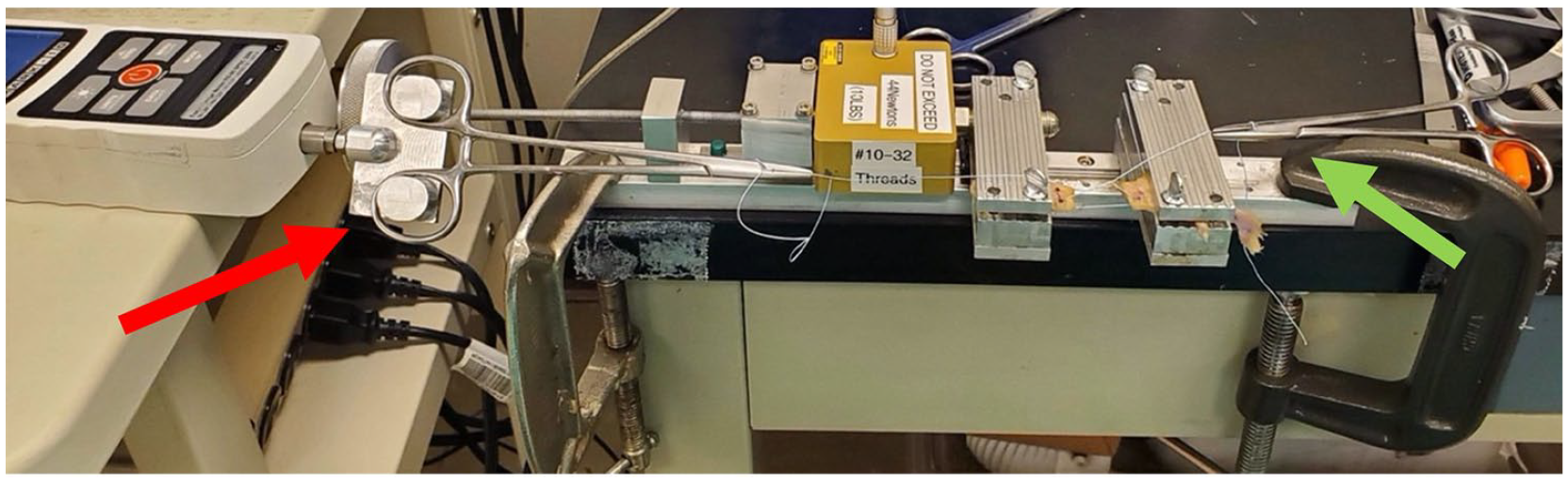
Testing configuration of suture tensioning. A force gauge (red arrow) is used to pull one of the needle drivers that is holding a suture end. The force gauge and the second needle driver (green arrow) are tensioned, parallel to the knot, by the tester until suture failure.
Statistics
Statistical analysis was performed with SPSS (Version 29.0, IBM, Armonk, NY). An a priori analysis was performed with 5 pairs (inner vs. outer). For a power of .8, it was determined that there needed to be at least 19 pairs. To make sure there was a sufficient sample size, it was determined that 24 pairs or 48 suture repairs were needed. A chi-squared test was used to compare force data between meniscal suture positions, inner versus peripheral group. The suture failure tensile forces comparing inner and peripheral sutures were compared using a 2-sample t test. In addition, lateral and medial meniscus specimen suture force data were compared using a 2-sample t test.
Results
There were 48 suture repairs that were tested (24 inner and 24 peripheral). The suture repairs primarily failed due to meniscal tissue cut-out after suture tensioning. All 24 sutures in the inner region (white-white zone) failed due to meniscal tissue cut-out, whereas tissue cut-out occurred in 22 out of 24 (92%) of the peripheral sutures located in the red-red zone. The suture ruptured at the needle driver-suture interface for the remaining 2 sutures in the peripheral group. There was no difference statistically in failure mode between medial and lateral meniscus specimens for both the inner and the peripheral sutures. The 2 suture ruptures occurred in the periphery of 1 medial meniscus specimen and 1 lateral meniscus specimen.
The average failure tensile force for the inner sutures was 36 ± 11 N and the peripheral group had an average failure tensile force of 54 ± 26 N (
Table 1
and
Mean Failure Tension in Newton (N) of Parallel Suture Repair of Radial Meniscus Tear Based on Location of the Suture.

Statistically significant results are bolded.
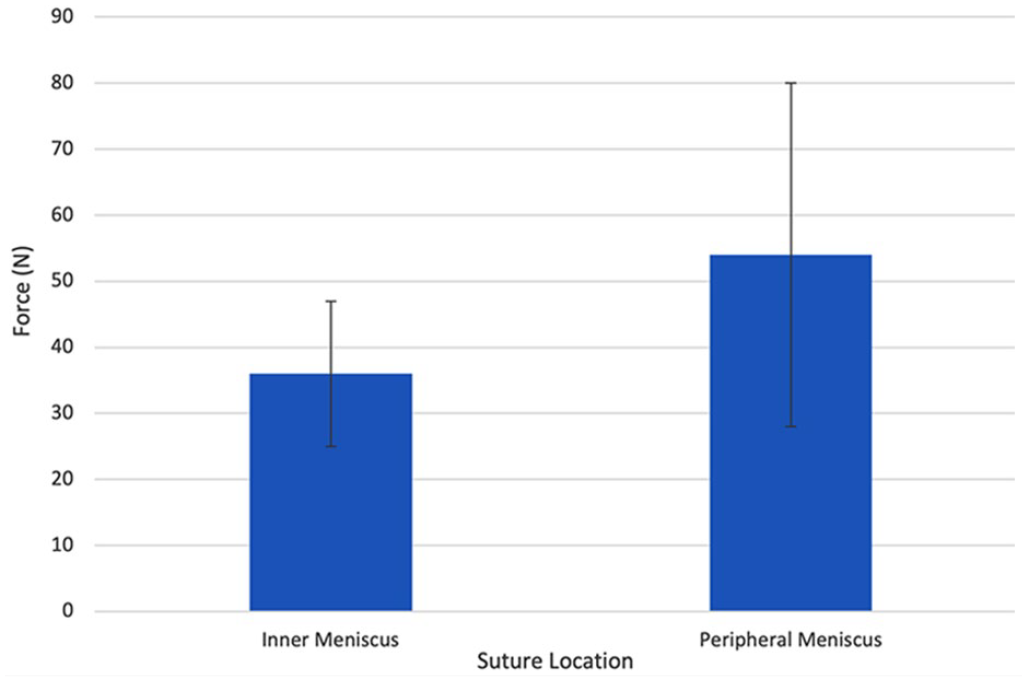
Mean failure tension in Newton (N) of parallel suture when repairing radial meniscus tear based on suture location. Sutures in the peripheral meniscus failed at a mean of 54 N while mean failure occurred at 36 N in the inner tissue (P = 0.006).
The peak tensile force acting on the meniscal fibers at the parallel suture repair failure was recorded for both the inner and the peripheral sutures. The meniscus experienced an average peak tensile force of 36 ± 7 N when the peripheral sutures failed by tissue cut-out or suture rupture, whereas the average peak force on the inner meniscus was 26 ± 7 N at meniscus tissue cut-out ( Table 1 ). The mean meniscal tension across all 48 samples was 30.9 N. The peripheral meniscus tolerated higher tension at failure than the inner meniscus (P < 0.001). Post hoc analysis based on the average suture tensile failure load of the inner versus outer meniscus demonstrated a power of 1.0.
Medial and Lateral Meniscus Comparisons
The peak tensile suture load for the lateral versus medial meniscus was not statistically significant for both the inner (P = 0.58) and the peripheral sutures (P = 0.53). In addition, the peak forces experienced by the meniscal tissue at suture failure for medial versus lateral meniscus specimens were not statistically different when comparing both the inner (P = 0.40) and the peripheral sutures (P = 0.16).
Subgroup Analysis
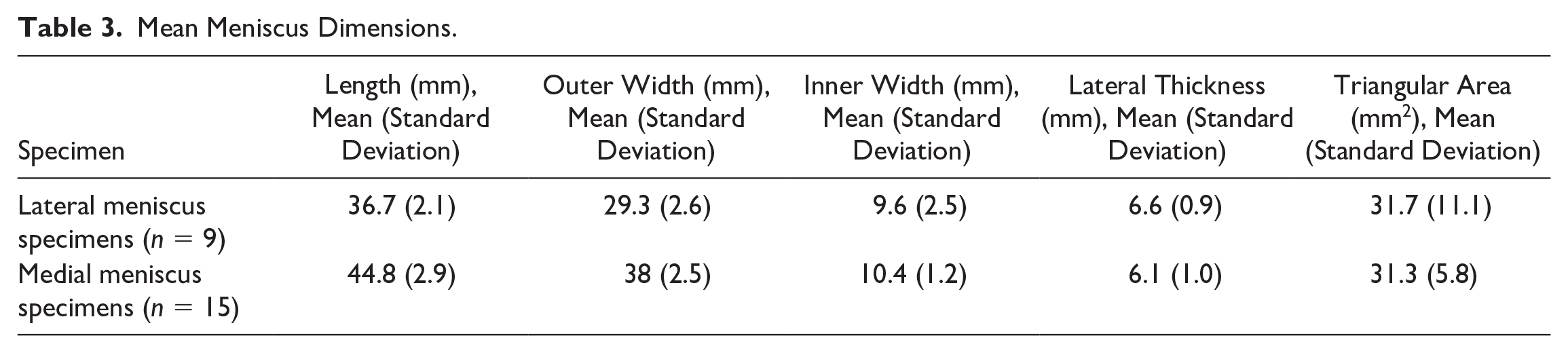
For the lateral meniscus, there was a significantly higher suture tension load to failure for the peripheral versus inner sutures (P = 0.040; Table 2 ). For the medial meniscus, there was not a significant difference between the suture failure load for the peripheral versus inner sutures (P = 0.140). Regarding intra-meniscal tissue tension, peripheral tissue withstood significantly higher load to failure forces in both lateral and medial menisci (P = 0.01 and P ≤ 0.01, respectively; Table 2 ). The meniscus dimensions are reported in Table 3 .
Subgroup Analysis of Medial and Lateral Meniscus: Mean Peak Failure Tension in Newton (N) Peripheral versus Inner Tissue for Parallel Suture Repair of Radial Meniscus Repair.

Statistically significant results are bolded.
Mean Meniscus Dimensions.
Discussion
Radial meniscus repairs can be challenging due to their biomechanical properties and biologic healing potential.
The key finding of this investigation is that the average failure tension load while tightening a parallel suture in a radial meniscal tear in peripheral (red-red) tissue is 54 ± 26 N and 36 ± 11 N for inner (white-white) tissue. Sutures through peripheral tissue demonstrated a failure load that was significantly higher than the inner tissue. The peripheral meniscus was also able to withstand significantly higher tension within the tissue itself compared to the inner meniscus with failure loads of 36 ± 7 N versus 26 ± 7 N. The primary mode of failure was meniscal tissue cut-out (96%) with only 2 cases (4%) resulting in failure of the suture material at the suture-needle driver interface. Failure loads were not significantly different between lateral and medial menisci. The present study is, to our knowledge, the first to report on human meniscal tissue failure at the time of knot tying, simulating the intraoperative setting of a radial tear repaired with parallel suture technique.
Numerous studies have described suture cut-out as a mode of failure following meniscal repair.21,22,27-29 A previous study of human cadaveric menisci using 2-0 nonabsorbable suture in parallel technique to repair a radial tear demonstrated a mean failure load of 85.5 N. 11 This study tested load to failure with 2 sutures in place, while our study examined forces placed on only 1 suture at a time to simulate a real-world knot-tying scenario. The reported failure load with 2 sutures (85.5 N) was more than double that seen with a single suture in the present study (overall mean of 30.9 N). The results from the 2-suture testing differ significantly from our results in an unpaired t test (P = 0.0001). Hang et al. 30 studied failure loads in porcine menisci using 2 sutures placed in parallel. This group describes an average failure load of 148.5 N for this repair, with the only observed mode of failure being tissue cut-out. Matthews and colleagues 28 tested failure loads in porcine menisci using a single suture. This group found tissue cut-out to occur at an average of 124.6 N when using a nonabsorbable 2-0 suture (Arthrex, Naples, FL), the same suture material used in our study. When compared using an unpaired t test, neither the study by Hang et al. nor the study by Matthews et al. reported results similar to our findings (P = 0.0001 and P = 0.0001, respectively). It is difficult to compare these previous studies to our study, because the previous studies focus on pulling the meniscus under tension after the repair has been completed. Our study was specifically evaluating the force applied to the suture as it is being tied. One thing is clear, that is the force required for a suture to cut through meniscus tissue while tying is much less than the force required for meniscus to cut through after the suture has been tied.
With an average suture tension failure load of 36 N in the inner and 54 N in the peripheral meniscus using parallel technique, we recommend that surgeons do not exceed 30 N (6.74 pound-force) of force when tying meniscal sutures. A spring tensioner is a rather simple device that can be used to measure tensile forces. Similar tensioners are already used in orthopedics (graft tensioners, cerclage wire tensioners) and may be easily repurposed for this task. If high tensile forces are needed to reduce a meniscal tear, starting with the peripheral tissue would potentially give a better chance of a successful reduction without cut-out. These recommendations are most applicable to complete radial tears that require significant tension to reduce, hence the gap used in our testing set up. Further tests should be completed on fully reduced tears to determine how this may alter cut-out mechanics.
It is worth noting that alternative suture patterns, as well as repair augmentations, have been shown to impact the failure loads of completed repairs.27,31 It would follow that augments and different repair techniques may alter the failure loads during the knot-tying process, and this is an area for future research. In addition, tying mechanics will vary even with the same repair technique when knots are tied from different angles or through arthroscopic portals. Our testing setup, tensioning a surgeon’s knot parallel to the sutures placed in the tissue, likely imparted a near maximum amount of force through the tissue. If a knot is tensioned with the free suture ends not oriented in line with the repair, the forces through the tissue may be altered and would likely be lower due to added friction within the knot. Tying through portals will also alter the tension imparted to the tissue due to friction.
Intraoperative failure of both devices and patient’s tissue is a complication that all orthopedic surgeons will inevitably face. However, limited data are available on the incidence of intraoperative complications relating to the process of knot tying. Iatrogenic injury caused by suture cut-out can quickly turn a straightforward meniscal tear into a complex injury requiring more time and resources to repair. A more complex tear increases morbidity for patients and is likely to prolong downtime for athletes with these injuries.32,33 The information in the present study helps to characterize how knot-tying-related iatrogenic injuries happen and can be used to minimize complications and both intra-operative and post-operative failure rates.
Limitations
Several limitations exist in this study. One limitation is that factors affecting healing of radial meniscus tear repairs were not addressed in this study since no living tissue was tested. In addition, this study was performed with arthroscopic instruments in an open setting allowing precise placement of sutures in each repair for consistency. Suture placement will inevitably be less precise in a true arthroscopic setting. The present study simulates tightening a suture to reduce a meniscal tear with a significant gap, but failure forces may be altered by additional support within the tissues from compression between the halves. The gap was created to simulate a real-world scenario where there is a gap in the tissue. Further research could repeat the biomechanical testing in this study and place the 2 meniscus halves adjacent to one another. Finally, we did not examine different types of repairs. Additional studies could also investigate different suture patterns, suture materials, suture passing devices, and types of meniscal tears.
Conclusion
When tying parallel sutures to repair a radial meniscus tear, suture tensile forces above 30 N may tear through meniscus tissue. Surgeons should not use suture tying forces above 30 N when repairing radial meniscus tears with parallel sutures. The peripheral meniscus can withstand higher knot-tying forces than the inner meniscus, so surgeons should consider tying the peripheral suture before the inner suture.
Footnotes
Acknowledgments and Funding
The authors would like to acknowledge Baraa Shihadeh for preparation of manuscript. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This project was approved by our Institutional Review Board (STUDY00001626).