
Abstract
Objective
This study aims to tackle the existing challenges associated with the prediction and optimization of pharmaceutical interventions for osteoarthritis (OA). The primary objective is to develop an innovative tool that provides objective and patient-specific information regarding the most affected tissue in OA, articular cartilage.
Design
We employed an organ-on-a-chip (OoC) approach to replicate the 3D structure of cartilage in an in vitro setup. The study focused on assessing the individual drug responses of common medications using this innovative platform. Additionally, we conducted a biomarker analysis to gain insights into the variability of drug responses across patients.
Results
Our findings reveal that OA articular cartilage demonstrates an individualized response to pharmaceutical interventions. Despite the diverse nature of patient responses, our study indicates that Triamcinolone, a standard-of-care medication, consistently exhibits a robust anti-inflammatory response across patient tests. However, as seen in clinical studies, Triamcinolone was concurrently associated with degeneration. The biomarker analysis further underscores the importance of considering individual drug responses in developing effective treatment plans.
Conclusion
In conclusion, this study introduces a valuable tool that not only mimics the 3D structure of cartilage but also provides crucial insights into the individualized responses of patients to various OA treatments. The application of an OoC approach may allow for a more accurate assessment of treatment efficacy. This objective biomarker analysis on patient-specific tissue offers clinicians a means to tailor treatment plans, thereby minimizing joint damage and advancing toward a more personalized approach in OA management.
Introduction
Osteoarthritis (OA) is a very common degenerative musculoskeletal disorder affecting more than 500 million people worldwide. 1 It has a multifactorial causation for the progression of the disease, which leads to demanding challenges within the field of degenerative joint illness. 2 The disease is often triggered by injuries to the cartilage tissue in the joint, which result in inflammation and degeneration of the affected cartilage tissue. Eventually, it leads to complete degeneration of the articular cartilage, alterations in subchondral bone morphology, and chronic synovial inflammation.2,3 As the global population ages and the prevalence of obesity rises, imposing sustained stress on joints, the burden of OA continues to increase, with low efficacy rates of current treatment modalities. 4 This necessitates innovative research approaches aimed at not only deepening our understanding of the underlying mechanisms of OA but also laying the groundwork for the development of effective therapeutic interventions. 5 In the pursuit of unraveling the intricate etiology of OA and devising interventions that can curtail its progression, conventional in vitro cell culture models prove to be limited in their capacity to replicate the dynamic and multifaceted environment of the joint. 6 Cartilage cells in particular have been shown to adopt an altered phenotype when cultured in a 2D in vitro environment. This limitation significantly impedes their utility in accurately studying the intricate processes that underlie the development of OA and evaluating the potential efficacy of emerging therapeutic strategies.6,7 The emerging technology of organ-on-a-chip (OoC) systems holds the promise to surmount these barriers and revolutionize the field of OA research. 8
The incorporation of OoC technology into the realm of OA research heralds a paradigm shift, particularly in the domain of testing and validating potential medications. 9 At the same time, it addresses the existing challenges that have hampered the progress of OA drug development. The current strategies employed for the development of OA medications are often mired in trial-and-error methodologies, frequently yielding suboptimal outcomes. 10 This challenge is further exacerbated by the absence of in vitro models that can faithfully recapitulate the intricacies of the joint microenvironment. Moreover, the multifaceted and heterogeneous nature of OA necessitates a comprehension of the intricate disease pathways, a prerequisite for the identification of viable therapeutic targets.11,12 OoC models provide an avenue for the incorporation of patient-specific cells, thereby unlocking the potential for personalized medicine approaches. This approach stands poised to usher in an era where treatment regimens can be tailored to the unique genetic and molecular makeup of individual patients, markedly reducing reliance on generic cell lines or animal models. 12
OoC technology’s compatibility with clinical materials represents a pivotal advancement. For instance, the utilization of cells sourced from arthroscopic tissue fragments aligns seamlessly with the capabilities of OoC platforms. Tissue samples procured during arthroscopy can be harnessed to cultivate patient-specific disease models within OoC systems. 13 This strategic amalgamation facilitates an in-depth exploration of the genetic and cellular transformations that manifest in distinct patients. 14 Consequently, the integration of clinical observations with experimental investigations is fortified, significantly augmenting the translational potency of OoC systems. The advent of OoC systems has the capacity to overcome some of the most pressing challenges that have hampered OA research. 15 From their potential to transform medication testing and validation, their compatibility with patient-derived cells, and their ability to replicate joint biomechanics, OoC platforms emerge as a beacon of hope in the quest for improved OA management.
In this study, we present a novel in vitro model designed to offer patient-specific insights into medication responses with minimal patient intervention, merely involving a cartilage biopsy procured from medical waste from arthroplasties. Our research involved the utilization of chondrocytes sourced from 13 distinct patients, showcasing a promising avenue for enhanced and personalized treatment strategies for individuals afflicted by OA. To replicate the intricate physiological milieu of the joint environment, we engineered a microfluidic chip. 16 This cutting-edge chip allowed for the cultivation of cells in a 3-dimensional setting over multiple days, enabling the systematic assessment of their reactions to diverse medications, all aimed at achieving optimal treatment outcomes. In an effort to emulate the chronic inflammation that typifies OA, we artificially introduced interleukin (IL)-1b and tumor necrosis factor (TNF)-α. Following the treatment protocol, we meticulously gauged individualized treatment responses by employing a panel of 10 biomarkers. These biomarkers were leveraged to dissect alterations in gene expression patterns anticipated to directly correlate with treatment outcomes. Through this comprehensive analysis, we aimed to unearth a deeper understanding of how chondrocytes respond to distinct medications, thereby paving the way for more tailored and efficacious therapeutic regimens.
Materials and Methods
Isolation of Chondrocytes
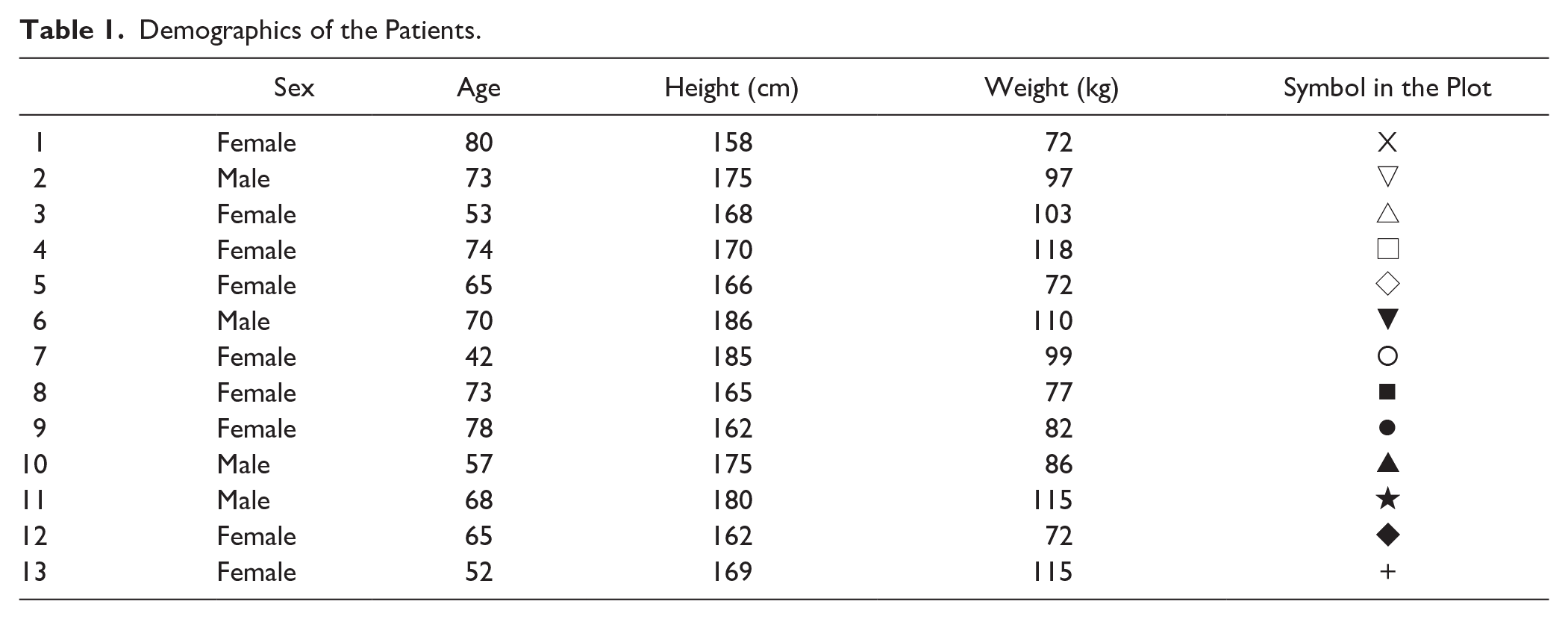
We obtained ethical approval and informed consent from all patients. The study was approved by the Ethics Committee of Lower Austria (EK 1100/2020) and conducted in accordance with the World Medical Association’s Declaration of Helsinki (1969, including any subsequent revisions). Patient samples were not pooled, but were tested individually; the demographics of the patient samples are shown in Table 1. The samples were surgical waste that resulted from knee replacement. Bauer et al. 17 detailed the process of isolating and cultivating chondrocytes.
Demographics of the Patients.
Cells were grown to 80% confluency in 2 × 75 cm2 flasks (in Passage 2), which is sufficient to load an OoC (Pregenerate, Vienna, Austria). To track the cells, they were stained with CellTracker® Green CMFDA (Thermo Fisher Scientific, Waltham, MA, USA) half an hour before loading onto the chip. Then cells were detached using accutase (Corning, Corning, NY, USA), counted, and viability measured with the Countess II FL (Thermo Fisher Scientific). Afterward, the cells were washed and adjusted to a cell concentration of 1 × 107/ml. Notably, 3 parts of cells were mixed with 2 parts of 100 mg/ml fibrinogen (Sigma-Aldrich). 2 U/ml thrombin (Sigma-Aldrich) in 40 mM CaCl2 (Thermo Fisher Scientific) was added to the cell/fibrinogen mixture and 12 µl was immediately transferred to a chamber (see
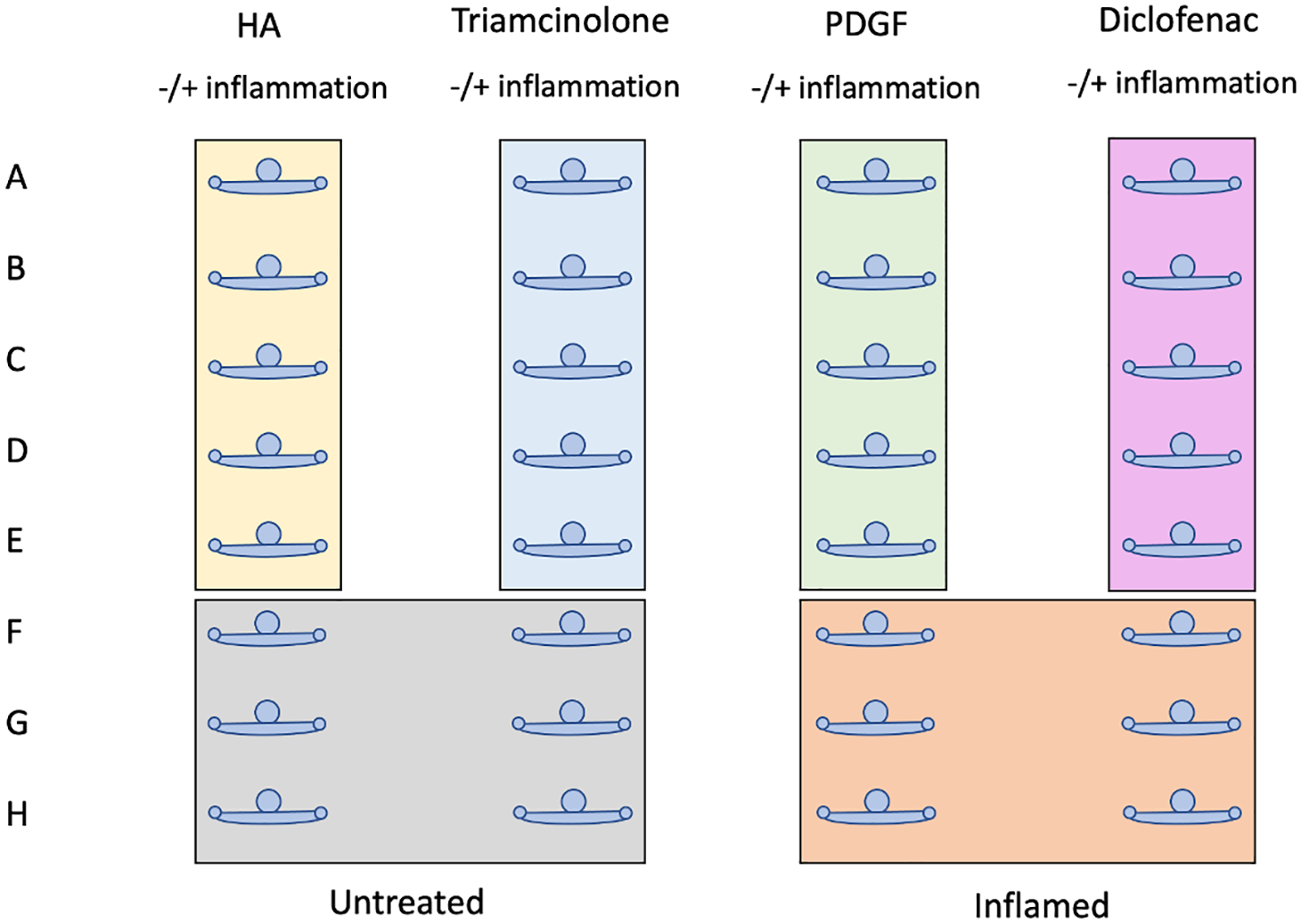
Schematic presentation of the chip. The medications are illustrated in different colors: yellow box: hyaluronic acid, blue box: triamcinolone, green box: PDGF, and pink box: diclofenac. Controls are shown in gray—untreated (complete media only) and in orange—inflamed. There are 5 chambers for each of the 4 medications. For the controls, non-inflamed and inflamed 6 chambers were used.
Following treatments based on the literature were used: 400 μg/ml hyaluronic acid (Rottapharm Madeus GmbH, Monza, Italy), 60 μg/ml triamcinolone (Acros Organics, Verona, Italy), 6 ng/ml diclofenac (Novartis, Basel, Switzerland), and 17.5 ng/ml PDGF-BB (Gibco) were mixed each with 2 ng/ml TNF-α and 2 ng/ml IL-1b, to mimic the treatment on an inflamed cartilage.18-21 The inflamed control consists of 2 ng/ml TNF-α and 2 ng/ml IL-1b and the untreated control of complete media only. The medium was changed every 2 days, generating intermittent shear stress, which serves as a form of mechanical stimulation important for chondrocyte function and extracellular matrix production.
16
The pipetting scheme and the structure of the chip, which consists of 32 individual chambers, can be seen in
Figures 1
and
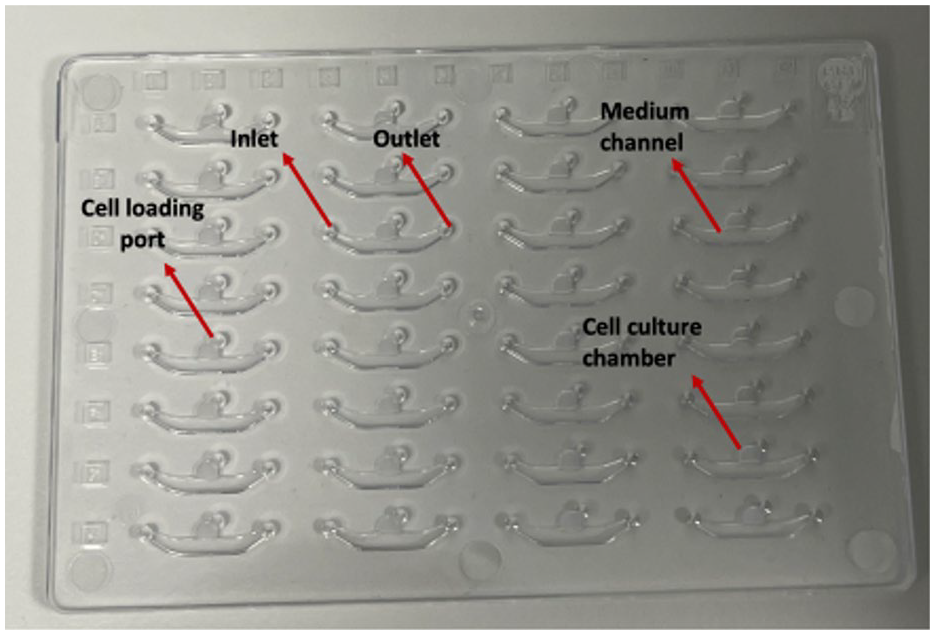
Schematic structure of the chip. The chip is produced by Pregenerate GmbH. It consists of 32 individual chambers, each consisting of an inlet and outlet for adding medium or treatment. In the center of this ship-like chamber is the opening for loading the cell matrix.
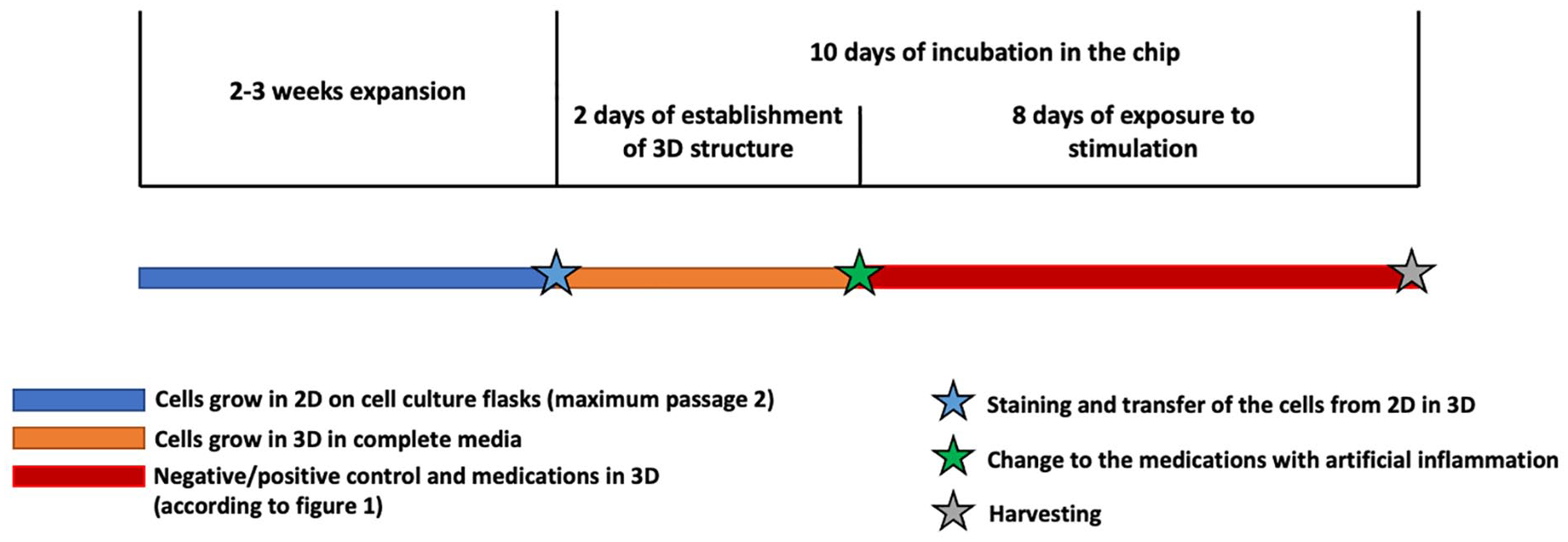
Timeline. Chondrocytes were seeded in complete medium (blue line) for expansion for 2-3 weeks, but not longer than Passage 2. The cells were seeded in 3D in complete media (orange line) for 2 days so that the 3D structure can form. Afterward, the cells were treated with the medications mixed with the inflammation agents (red line). The cells were harvested after 10 days inside the chip.
Fluorescence Microscopy
Microscopy was utilized to determine morphology and cell count using the Thermo Fisher Scientific EVOS 7000M imaging equipment. CMFDA green (Thermo Fisher Scientific) staining was performed before loading the cells, and images were taken to track the cells on days 1, 3, and 8 after loading onto the chip. Calcein/ethidium homodimer-1 (Thermo Fisher Scientific) was used for live-dead staining. The EVOSTM LED Cube (Thermo Fisher Scientific) with excitation (Ex): 482/25 and emission (Em): 524/24 wavelengths was used. The 4× and 10× EVOS 8.4 objective was used to accomplish a maximal intensity projection of a z-stack 1-channel overlay.
RNA Extraction and Reverse Transcription-Polymerase Chain Reaction (RT-PCR) Performance
After the 3D cultivation, the cells were harvested with a lysis buffer (from in-house high-performance RNA bead isolation Kit) and 1% ß-mercaptoethanol (EMD Millipore Corp., Billerica MA, USA), mRNA was converted into cDNA (Maxima H-Minus RT, Thermo Fisher). Taqman probes and Taqman Fast Advanced Master Mix (Thermo Fisher) were used for qPCR analysis according to the manufacturer’s recommendations (GAPDH—Hs00899658_m1, MMP13—Hs00942584_m1, Eef1—Hs02339452_g1, MMP3—Hs00968305_m1, Acan—Hs00153936_m1, Col2—Hs00264051_m1, Col10—Hs00166657_m1, AdamTS5—Hs01095518_m1, Sox9-Hs00165814_m1, Col1A1- Hs00164004_m1, MMP1-Hs00899658_m1, and IL-6-Hs00174131_m1).
Data Analysis
The delta Ct technique was applied to analyze gene expression and to normalize the data the housekeeping genes GAPDH and Eef1 were used.22,23 Calculated by housekeeping gene (ref cq)—gene of interest (mean cq) = △ct and afterward 2△ct. 24 Data were expressed as boxplots and a Kruskal-Wallis test was performed like described in the figure legend. The diagrams were made using the GraphPad Prism software 9.
Results
Morphology of 3D Cultivated Chondrocytes
Chondrocytes derived from osteoarthritic cartilage were isolated and subjected to observation of growth and viability within the chip over a 28-day period.
Figures 4A
and
B
illustrate the incorporation of calcein and ethidium homodimer, depicting the diffusion gradient. The gradual diffusion of these reagents within the matrix is evident, with the outer edge displaying greater brightness than the inner body. The observed survival rate after 28 days exceeded 80%. Notably, the cells exhibited a rounded morphology reminiscent of their natural state within the body (
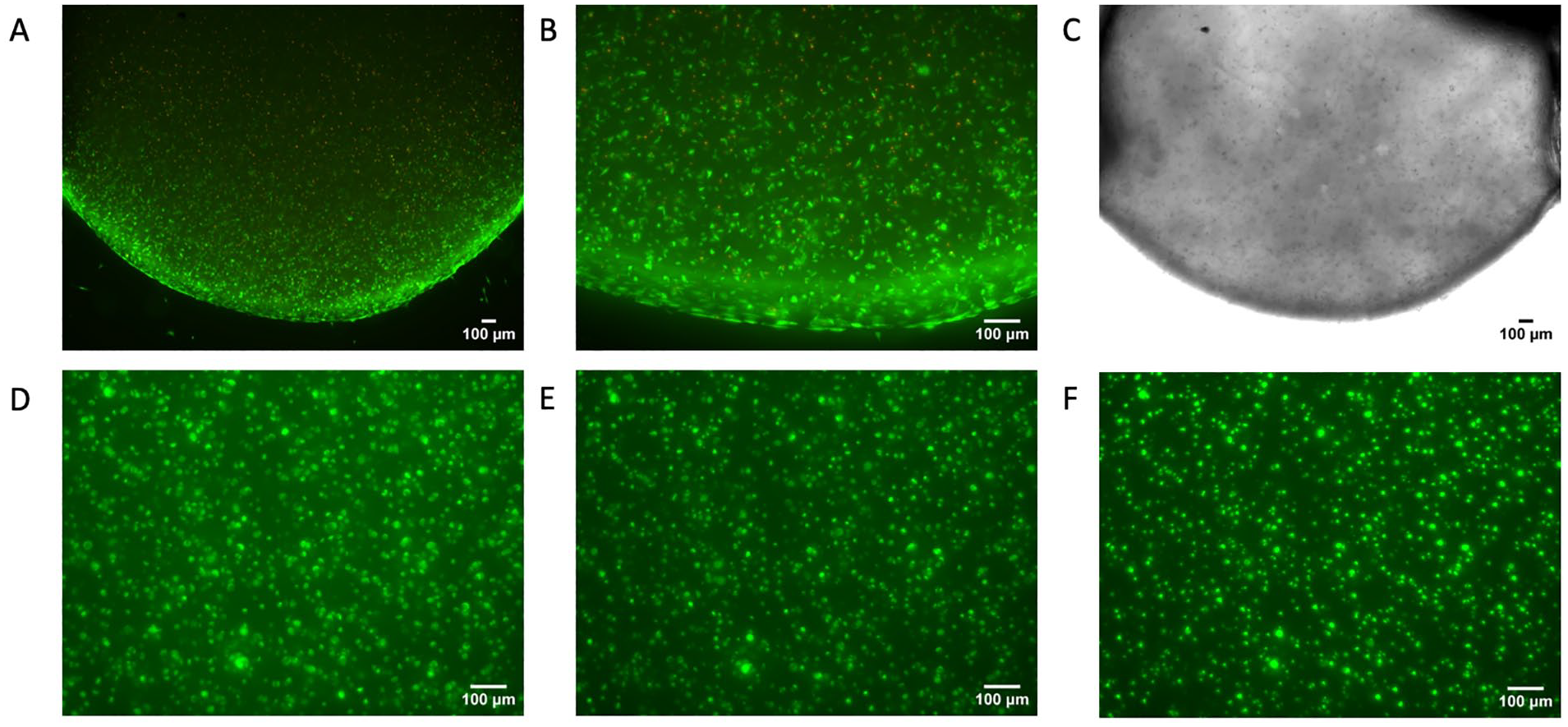
Morphology of chondrocytes. Z-stack fluorescence overlay of chondrocytes, which were loaded in the chip (A) after 28 days stained with calcein (green) and ethidium homodimer-1 (red) magnification 4×, (B) magnification 10×. (C) Brightfield image of the matrix with chondrocytes, magnification 4×. D-F should demonstrate the movement of the cells inside the chip after 1 day (D), 3 days (E), and 8 days (F) stained with CMFDA green, 10×, maximal intensity projection of a z-stack overlay Microscope: EVOS 7000M.
Expression of Degenerative Gene Markers
The analysis of the gene expression markers took place after a 10-day experiment, the process can also be seen in
Figure 3
. We categorized the biomarkers into 2 distinct groups: degenerative markers and regenerative markers. The degenerative markers encompass MMP1, MMP3, MMP13, ADAMTS5, IL-6, and Col10, as their roles are pivotal in the degradation of cartilage matrix, the promotion of inflammation, and the remodeling of tissues in OA.
25
Notably, the MMP family demonstrates consistent behavior, enabling the discernment of triamcinolone’s inhibitory impacts. Substantial deviations from the inflamed control are observable in the cases of MMP1 (
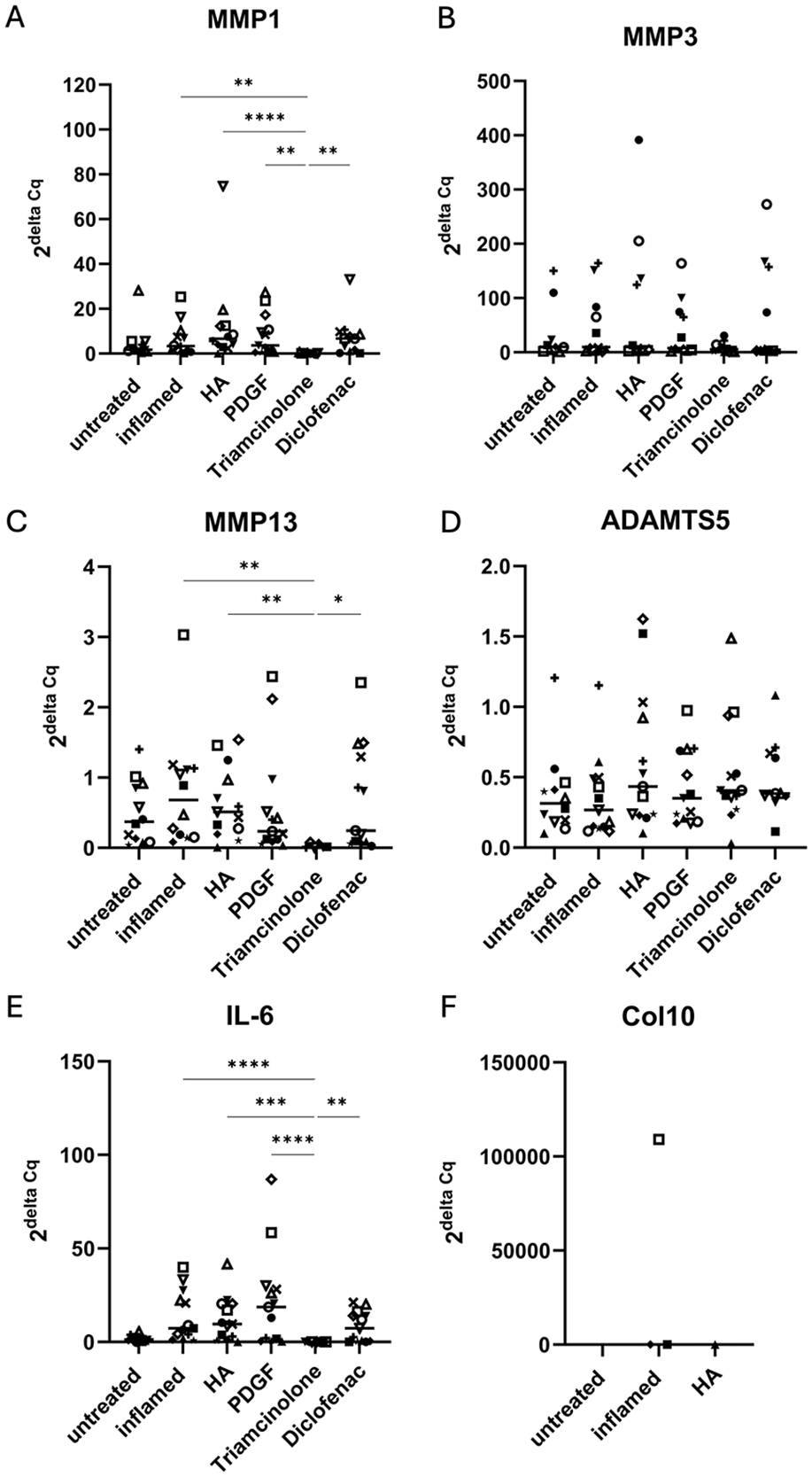
Expression of degenerative gene markers. A total of 13 post-transplant osteoarthritic samples were used for gene expression analysis of (A) MMP1, (B) MMP3, (C) MMP13 (D) ADAMTS5, (E) IL-6, and (F) Col10. The samples were grown in 3D and then treated in an inflamed environment with the different medications hyaluronic acid (HA), platelet-derived growth factor (PDGF), triamcinolone, or diclofenac. Expression rates resulting from the 2delta Cq method normalized with the mean of the housekeeping genes GAPDH, Eef1. Each patient is represented as a symbol, the median is represented with a line. Kruskal-Wallis test. *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001, ****P ≤ 0.0001.
Expression of Regenerative Gene Markers
The regenerative markers ACAN, Sox9, Col1, and Col2 are key elements in the composition, structure, and maintenance of cartilage.
27
A decrease in ACAN expression was observed within the context of inflammation (
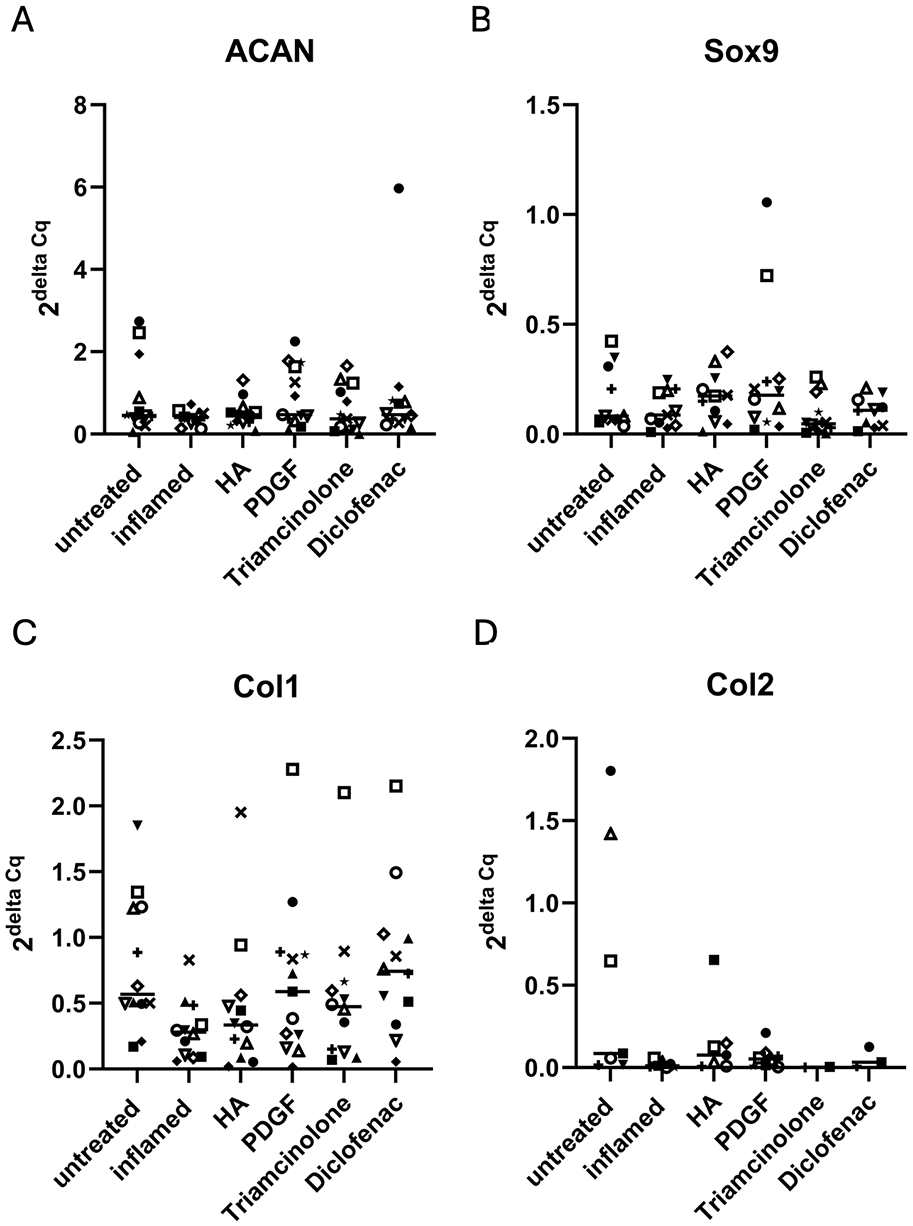
Expression of regenerative gene markers. A total of 13post-transplant osteoarthritic samples were used for gene expression analysis of (A) ACAN, (B) Sox9, (C) Col1, and (D) Col2. The samples were grown in 3D and then treated in an inflamed environment with the different medications hyaluronic acid (HA), platelet-derived growth factor (PDGF), triamcinolone, or diclofenac. Each patient is represented as a symbol, the median is represented with a line. Expression rates resulting from the 2delta Cq method normalized with the mean of the housekeeping genes GAPDH, Eef1.
Discussion
The findings presented in this study shed light on the intricate responses of chondrocytes within an OoC environment, providing insights into the complex interplay between cellular behavior, molecular responses, and potential therapeutic interventions for OA. Our approach extends existing research in the field, enhancing our understanding of OA pathogenesis and potential treatment strategies. Our use of an OoC approach is in line with the rising interest in creating improved in vitro models that more accurately replicate the physiological characteristics of the joint environment. This method is consistent with other research, such as, which used comparable microfluidic devices to analyze chondrocyte activity under controlled settings.28,29 However, the distinctiveness of our study lies in its emphasis on both degenerative and regenerative markers, affording a more holistic view of OA progression and therapeutic potential. We have listed the patient demographics in Table 1 , which include sex and age distributions among the participants. Specifically, 4 out of 13 patients were male, which aligns with the reported sex distribution of OA in the general population, reflecting the higher prevalence of OA among females.30,31 Additionally, 4 out of 13 patients were under the age of 60, which is consistent with the age range typically observed for patients undergoing arthroplasty due to OA. 32 While we acknowledge the importance of understanding how patient demographics might influence or relate to the experimental outcomes, our current sample size and demographic distribution limit the ability to draw definitive conclusions regarding these correlations. To elucidate any potential correlations between patient characteristics (such as sex, age, disease severity, and other factors) and the experimental outcomes, a larger, cross-sectional patient sample size would be required. This would enable a more comprehensive analysis and provide greater statistical power to detect any meaningful associations. In our study, we specifically obtained cartilage samples from the macroscopically osteoarthritic regions of the femoral condyle. We focused solely on these osteoarthritic areas to ensure consistency in cartilage quality and thickness, which can vary significantly between weightbearing and non-weightbearing regions. By selecting cartilage from the same general area, we aimed to minimize variability and provide a more uniform basis for patient-by-patient comparison.
The observed rounded morphology of chondrocytes inside the 3D chip environment, which is evocative to their in vivo condition, reflects observations described by Karim et al., 33 showing the significance of our model in capturing cellular behavior more accurately. The formation of the extracellular matrix and the expression of its building elements, such as the collagen family, depend on the permanence of chondrocytes in place over a period of days, underscoring the significance of stable cellular organization within such systems. 34
Examining the influence of common medications such as hyaluronic acid (major component of synovial fluid), triamcinolone (a glucocorticoid), diclofenac (a non-steroidal anti-inflammatory drug), and PDGF (a highly concentrated molecule in platelet-rich plasma) on OA, we utilized 10 biomarkers for our analysis. The cells were given another weak dose of TNF-α and IL-1b for the positive control and the medications. Triamcinolone exerts anti-inflammatory effects by binding to the glucocorticoid receptor, subsequently suppressing inflammatory gene expression. The inhibition of MMPs, particularly MMP1, MMP3, and MMP13, aligns with the known anti-inflammatory properties of glucocorticoids. In addition, Triamcinolone’s repression of IL-6 may involve interference with the NF-κB pathway and other inflammatory signaling cascades.35,36 However, clinical studies have shown that Triamcinolone increased volume loss. 37 Diclofenac develops its effects by inhibiting cyclooxygenases (COX), leading to reduced prostaglandin synthesis. Prostaglandins can modulate MMP expression. Diclofenac’s impact on MMPs may involve the COX-2 pathway, contributing to its anti-inflammatory effects. Additionally, non-steroidal anti-inflammatory drugs like Diclofenac are known to suppress pro-inflammatory cytokines, including IL-6, through the NF-κB pathway.38,39 We observed the anti-inflammatory effect on individual patients, noting variations in response. The effectiveness may also be influenced by the dosage, as different patients exhibited varying reactions. Diclofenac demonstrated a distinct effect on Col1 expression, deviating from the positive control. This unique impact suggests that Diclofenac may influence cartilage regeneration through mechanisms beyond its conventional anti-inflammatory properties. Previous studies have proposed that Diclofenac may modulate Wnt/β-catenin signaling, a pathway intricately involved in collagen synthesis and chondrogenesis.40,41 Hyaluronic acid is implicated in cartilage lubrication and anti-inflammatory processes. It may influence ADAMTS5, a key enzyme in cartilage degradation. The HA-CD44 signaling axis and its interaction with ADAMTS5 expression may be relevant, affecting the balance between anabolic and catabolic processes in cartilage. 42 Hyaluronic acid is known for its viscoelastic and anti-inflammatory properties, often utilized in the management of OA. PDGF is implicated in various cellular processes, including cell growth and tissue repair. In the context of OA, PDGF may influence matrix turnover by modulating MMPs. The PDGF pathway, activating tyrosine kinase receptors, can influence downstream signaling cascades involved in MMP regulation, impacting cartilage homeostasis.43,44 Except for a few individuals with MMP13, no other effect could be found with the MMPs. PDGF-BB exhibited a favorable impact on ACAN expression within the inflammatory context. PDGF is known for its role in cell proliferation, migration, and extracellular matrix synthesis, mediated through PI3K-Akt and MAPK pathways. 45 The positive influence of PDGF-BB on ACAN expression may be linked to its ability to activate these signaling cascades, promoting chondrocyte function and cartilage matrix synthesis. The variability in treatment responses in OA is attributed to disease heterogeneity and individual genetic factors. Polymorphisms in genes related to cartilage metabolism, inflammation, and drug metabolism may influence outcomes. The Wnt/β-catenin pathway, critical for cartilage homeostasis, is susceptible to genetic variations affecting individual responses.46,47 The observed decrease in ACAN expression within an inflammatory milieu aligns with previous studies implicating inflammatory processes in cartilage degradation. 48 As reported by Kang et al., 49 an increased number of passages has been shown to impact collagen expression. In a 2D culture, a decrease in Col2 expression is expected, leading us to avoid the use of chondrocytes beyond passage 2. This effect diminishes in a 3D culture. The experiment’s duration is crucial for both Col2 and Col10, and further investigation with an extended duration is still needed. Patient-specific factors like age, sex, and disease severity may influence cellular behavior, emphasizing the potential for personalized approaches in regenerative medicine. Our findings demonstrate that individual patients exhibit unique expression patterns and varied responses to the treatments.
In summary, by utilizing an OoC technology to unravel cellular responses and prospective therapeutic approaches, our study contributes to the expanding landscape of OA research. With this tool, we are able to give objective biomarker analysis of the patient-specific cartilage responses to approximately 80% of the osteoarthritic medication on the market. Moreover, we are able to perform the testing within 6 weeks of receiving the cartilage biopsy, which helps the clinician to make decisions within a reasonable clinical timeline. Unfortunately, this disease has many different facets, which is also represented in the classes of biomarkers analyzed in this study. Degenerative, regenerative, and inflammatory biomarkers may show additive or complementary response in the affected tissue, and this can be elucidated with our assay. Our findings provide the foundation for future research efforts that might capitalize on the promise of personalized therapies for OA, ultimately providing better outcomes for people suffering from this life-threatening ailment.
Footnotes
Acknowledgements
Faheem Ali, MSc. For his supportive roles throughout the work leading to this publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Material costs attributed to this work were partially funded within a grant from the Austrian FFG (grant no: 880934).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study received ethical approval from the Ethics Committee of Lower Austria (EK 1100/2020). Informed consent was obtained from all patients prior to their participation. The research was conducted in accordance with the World Medical Association's Declaration of Helsinki (1969), including all subsequent revisions.