
Abstract
Objectives
Viscosupplementation with hyaluronic acid (HA) is a commonly used intra-articular treatment for osteoarthritis (OA). We performed a Delphi consensus process to formulate guidelines for the use of intra-articular hyaluronic acid (IAHA) knee injection according to the patient’s characteristics.
Methods
The EUROVISCO group consists of 12 members who had expertise in clinical and/or research in the field of OA and IAHA treatment. This group drafted issues through an iterative process and subsequently voted according to a Delphi process on their level of agreement (LoA) on these recommendations. The scores were pooled to generate a median agreement score for each recommendation. The strength of the recommendation (SOR) was classified as strong if the median agreement score was ≥8. The level of consensus (LOC) was also obtained. The level of evidence was given for each recommendation.
Results:
A total of 34 statements were evaluated by the expert group. A unanimous or high LoA was obtained in 16. IAHA can be considered irrespective of the age in patients with symptomatic knee OA. It can be used in patients with diabetes and/or moderate to severe obesity. It can also be used in knee OA patients with a history of gout, meniscocalcinosis and with mild-to-moderate varus/valgus malalignment. The group recommended against the use of VS in pregnant women and in OA flare.
Conclusion
In summary, the working group provided strong recommendations for the use of IAHA injection that will facilitate individualized treatment decision algorithms in the management of knee OA.
Keywords
Introduction
Osteoarthritis (OA) of the lower limbs is ranked as the 11th cause of global disability and the 38th highest in disability-adjusted life years (DALYs). 1 Globally, 595 million people had OA in 2020, equal to 7.6% of the global population. The global age-standardized rate of years lived with disability (YLDs) for total OA was 255.0 YLDs per 100,000 in 2020. For adults aged 70 years and older, OA was the seventh ranked cause of YLDs. Age-standardized prevalence in 2020 was more than 5.5% in all world regions. The knee was the most common site of OA, with a 2020 global age-standardized prevalence of 4,307.4 cases (3,844.5-4,913.3) per 100,000 people. In 2050, there will be an estimated 642 million (95% confidence interval [CI] = 574-722) individuals with knee OA 2 , and consequently an increased economic burden due to a growing number of joint arthroplasties.3,4
Repeat intra-articular hyaluronic acid (IAHA) injections (also named viscosupplementation) (VS) are used in millions of patients every year worldwide for alleviating pain and decreasing disability due to OA of the knee. 5 The favorable benefit/risk ratio of VS was evidenced by the conclusions of numerous recent meta-analysis.6-10 In the network meta-analysis of Bannuru et al., 10 HA VS was ranked as the most effective treatment for knee OA, evidenced by an effect size of 0.63, much higher than that of non-steroidal anti-inflammatory drugs (NSAIDs). Several studies have also suggested that repeated VS may postpone the joint replacement.11-13 However, despite increasing success in terms of prescriptions, as evidenced by the growth of the viscosupplement market (the global VS market was valued at $4.4 billion in 2021, and is projected to reach $10.9 billion by 2031), 14 the level of evidence (LoE) reported in the literature remains questionable and some continue to assert that IAHA should not be recommended in the treatment of knee OA.15,16
Knee OA is an extremely polymorphic condition, in terms of location of joint space narrowing (involvement of 1 or more compartments of the knee), clinical severity, and comorbidities. Some attempt to classify patients with knee OA based on clinical, imaging, and laboratory data, as it has been shown that treatment responses can be influenced by the patient’s phenotype. 17 As HA only targets a few pathological mechanisms, it cannot be effective in all clinical situations. Rather than challenging the effectiveness of IAHA in the general population, we must distinguish the good, bad, and poor indications and identify the characteristics of patients which can influence the response to this treatment. Current data in the literature are poor on this issue. It has been demonstrated that the radiological severity of OA and obesity are prognostic factors of poorer response to IAHA,18,19 but little is known about the disparity in results relative to the involved compartment(s), MRI features (bone edema, meniscus lesion), types of pain (nociceptive, neuropathic, nociplastic), comorbidities, and lifestyle habits of patients.
Hence, the members of the EUROVISCO group 20 had chosen to discuss this issue in their annual meeting. Focus was on the characteristics of patient and OA disease. Recommendations were proposed for the use of IAHA based on both the literary evidence and the clinical and research experience of the 12 members of the task force.
Methods
Experts
The EUROVISCO working group brings together 12 physicians of 8 European nationalities (Belgian, British, French, Italian, Portuguese, Spanish, Swedish, and Turkish). This working group comprises 6 rheumatologists, 2 orthopedic surgeons, 3 rehabilitation specialists, and 1 interventional radiologist. All have expertise in the treatment of OA, in particular VS, as well as in clinical research methodology. All types of medical fraternity (private practice, public hospital, university hospital) were represented.
The working group met in Lyon on September 7 and 8, 2023. Nine of 12 members attended the meeting and 3 participated remotely. At each meeting since 2014, 1 member of the group [T.C.] was appointed chairman who directed the debate and acted as a moderator to mediate divergence of opinion between members.
The working session took place in 3 parts. The first part was devoted to the appropriateness or otherwise offering VS based on patient characteristics, and the second part was dedicated to the characteristics of knee OA. Finally, the third part addressed the appropriateness of VS according to the pain phenotypes. For each issue, the members discussed the literature data and compared them to their personal clinical experience. A total of 39 issues were debated during working sessions. For each issue, the members of the working group must rate their level of agreement (LoA) using the 9-point numeric scale. Scores 1 to 3 indicated “I disagree,” scores 4 to 6 “I agree, not in the majority of cases but under certain conditions only,” and scores 7 to 9 “I agree in the majority of cases.” The vote was conducted using interactive software (Quizzbox©, Clermont-Ferrand, France). The results of the vote were therefore available in real-time for the group as a whole and for each member. The software generated a median agreement score for each question. The strength of recommendation was scored STRONG FOR if the median score was 9, MODERATE FOR when the score was 8, and WEAK FOR in case of a score of 7. A median score of 6 to 4 meant CONDITIONALLY RECOMMENDED. Similarly, the strength of recommendation was scored STRONG AGAINST if the median score was 1, MODERATE AGAINST for a score of 2, and WEAK AGAINST for a score of 3.
The level of consensus (LOC) was calculated from the number of experts giving a similar score to the issue. It was classified as UNANIMOUS if all the experts agreed with the proposal and classified as HIGH if 11 or 10 experts agreed on a common response. Finally, it was considered as MODERATE and LOW if only 9 and 8 to 7 experts, respectively, gave a similar rating. After each proposition of recommendation, the result was discussed by the group. Each member presented his opinions (conflicting or otherwise), and a joint consensus was sought if possible. After hearing all arguments a new vote could be requested by one of the members wishing to modify their initial response. The LoE was given for each recommendation. 21
Results
The 40 recommendations submitted to the vote are given in detail in the following. The recommendations retained by the working group were those which obtained unanimous or high LOC, and a strength of recommendation—for or against—rated as strong or moderate ( Table 1 ).
Recommendations That Obtained Both Strength of Recommendation Strong or Moderate and a Level of Consensus Unanimous or High.
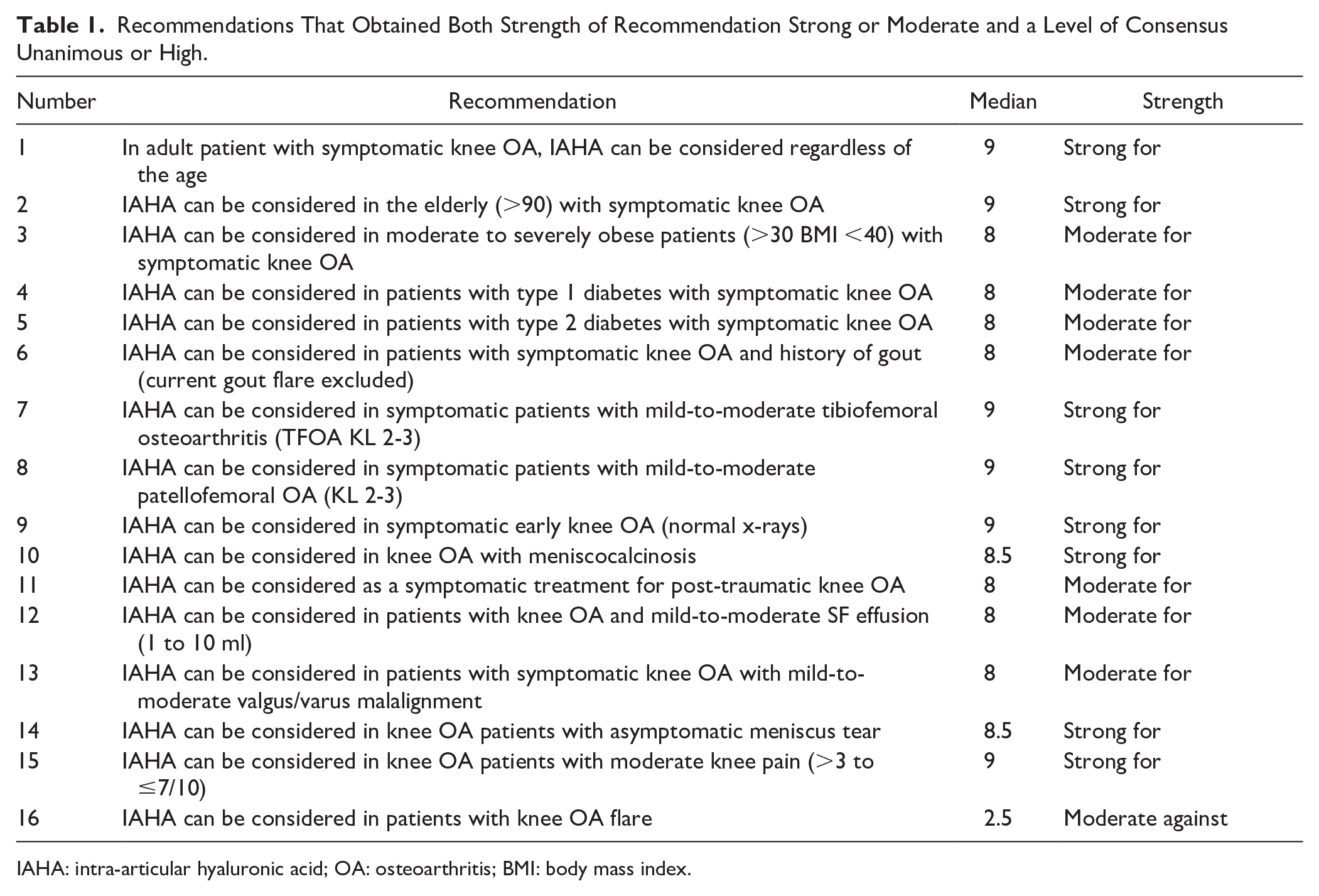
IAHA: intra-articular hyaluronic acid; OA: osteoarthritis; BMI: body mass index.
In adult patient with symptomatic knee OA, IAHA can be considered regardless of the age
Median/Strength of recommendation: 9/Strong for Level of consensus: Unanimous
Level of evidence: 1A
Comment: All members of the group considered that age was not a criterion in the decision to use VS. Clinical studies do not demonstrate a poorer response in elderly subjects.18,22-26 In addition, there is no evidence showing a subdued effect in young adults.26,27
IAHA can be considered in the elderly (>90) with symptomatic knee OA
Median/Strength of recommendation: 9/Strong for Level of consensus: High
Level of evidence: 2B
Comment: All experts, but 1, agreed with this recommendation. Given its excellent tolerance 24 and the absence of drug interactions, IAHA injections can be used in this frail population. VS is recommended by the British Geriatric Society that concludes IAHA is effective and free of systemic adverse effects in elderly people. Its use should be considered in patients for whom systemic treatment is contraindicated or poorly tolerated. 25
IAHA can be considered in adolescents with idiopathic or post-traumatic chondropathy
Median/Strength of recommendation: 6/ Conditionally recommended Level of consensus: No consensus
Level of evidence: 4
Comment: Anterior knee pain is a common condition among adolescents. Various theories have been proposed for explaining this disorder which are still not completely understood. 28 A histological study on patellar chondropathy in 83 adolescents with anterior knee pain showed histological lesions similar to those found at the early stages of knee OA. 28 These findings support the use of HA injections in adolescents suffering from idiopathic anterior knee pain in whom conventional treatment failed. Despite a case series of 16 adolescents 29 and a prospective study including young patients reporting very promising results, 30 the experts failed to agree on a common position and considered that the decision to use IAHA in this clinical situation should be decided on a case-by-case basis. However, they all agreed that IAHA was not harmful to children and adolescents.
IAHA can be considered in moderate to severely obese patients (>30 body mass index [BMI] <40) with symptomatic knee OA
Median/Strength of recommendation: 8/Moderate for Level of consensus: High
Level of evidence: 1B
Comment: Although obesity has been demonstrated to be associated with a lower rate of response to treatment, 18 the authors considered that moderate obesity should not refute the indication for VS. Although the success rate is reduced, the magnitude of the effect is satisfactory in responding patients. 19 Furthermore, many treatments are contraindicated in obese people who often suffer from high blood pressure and/or diabetes. HA has a very good safety profile that allows these patients to be treated harmlessly.
IAHA can be considered in morbid obese patients (BMI >40) with symptomatic knee OA
Median/Strength of recommendation: 5/Conditionally recommended Level of consensus: High
Level of evidence: 5
Comment: The authors agreed that morbid obesity is a very poor prognostic factor of IAHA response. However, they concluded that in the lack of other therapeutic solutions, IAHA can be conditionally recommended, provided that the patient is clearly informed of the risk of treatment failure.
IAHA can be considered in pregnant women with symptomatic knee OA
Median/Strength of recommendation: 3/Weak against Level of consensus: Low
Level of evidence: 5
Comment: In vitro, in vivo, ex vivo, and clinical studies on gestational models suggest that oral high molecular weight (HMW)-HA administration can be beneficial in physiological pregnancy, preventing miscarriage and pre-term birth. 31 Although the use of HA during pregnancy is considered safe and can be used liberally, 32 the task force recommended that IA steroid injections must be preferred to VS. As pregnancy has a finite time period, it is almost always possible to wait until childbirth before considering an IAHA injection. However, in the event of severe knee pain and a risk of gestational diabetes, VS may be considered if the obstetrician ratifies it.
IAHA can be considered in breastfeeding women with symptomatic knee OA
Median/Strength of recommendation: 4.5/Conditionally recommended Level of consensus: No consensus
Level of evidence: 5
Comment: In the absence of published data, the experts did not recommend the use of VS in breastfeeding women. However, they highlighted the safety profile of IAHA allows the use of VS without significant risk, in exceptional circumstances to avoid resorting to potentially more dangerous medications.
IAHA can be considered in patients with type 1 diabetes with symptomatic knee OA
Median/Strength of recommendation: 8/ Moderate for Level of consensus: High
Level of evidence: 5
Comment: Since HA injections are very safe and are used for wound healing in diabetic ulcers,33,34 the experts have considered that they can be recommended in type 1 diabetic patients. Viscosupplementation is even recommended as first-line treatment, before IA steroids and NSAIDs that can be potentially dangerous in these patients.
IAHA can be considered in patients with type 2 diabetes with symptomatic knee OA
Strength of recommendation: 8/Moderate for Level of consensus: Unanimous
Level of evidence: 5
Comment: For the same above reasons, the decision to recommend VS in type 2 diabetics was unanimous. Type 2 diabetes takes an important place in the cardiometabolic syndrome (MetS), 35 a complex interplay of insulin resistance, dyslipidemia, hyperuricemia, and hypertension, that limits the use of numerous therapies such as corticosteroids and NSAIDs.
IAHA can be considered in patients with symptomatic knee OA and a history of gout (current gout flare excluded)
Strength of recommendation: 8/Moderate for Level of consensus: High
Level of evidence: 5
Comment: All, but 1 member, recommended the use of IAHA VS in patients with knee OA and a history of gout, except for acute exacerbation of gout which should be treated with colchicine, NSAIDs, and steroids. 36 Despite an animal study showing HA was effective in gout flare, 37 there are no human data that suggest IAHA could be effective in treating acute gout arthritis.
IAHA can be considered in patients with symptomatic knee OA with MetS
Strength of recommendation: 8/Moderate for Level of consensus: Moderate
Level of evidence: 5
Comment: There is a clear association between metabolic factors and radiographic knee OA in individuals with knee pain, as well as in those with normal BMI. 38 Furthermore, MetS has been shown to be associated with more severe structural disease progression.39,40 In MetS-associated OA, low-grade inflammation plays a key role in the disruption of joint homeostasis and cartilage degradation. 41 Regarding the anti-inflammatory effects of HA,42,43 9 of 12 members voted that the treatment is recommended in patients with MetS, while the other 3 chose to vote on a conditional recommendation.
IAHA can be considered in patients with symptomatic knee OA and multiple comorbidities (i.e., arterial hypertension and/or renal failure and/or liver failure and/or diabetes and/or cardiac diseases, etc.)
Median/Strength of recommendation: 8/Moderate for
Level of consensus: Moderate
Level of evidence: 5
Comment: The vast majority of experts recommended VS in patients with multiple comorbidities. They justified their choice by the excellent risk-benefit ratio of hyaluronic acid (HA)5,9,44 especially in such frail patients.
IAHA can be considered in symptomatic patients with mild-to-moderate tibiofemoral osteoarthritis (TFOA KL 2-3)
Median/Strength of recommendation: 9/Strong for Level of consensus: Unanimous
Level of evidence: 1A
Comment: Unsurprisingly, all experts agreed to recommend IAHA in mild-to-moderate knee OA as previously recommended by most of guidelines9,45-49and demonstrated in clinical trials designed to identify predictors of failure and success.18,22,23,26,27,50
IAHA can be considered in symptomatic patients with advanced TFOA (KL 4)
Strength of recommendation: 7/Weak for Level of consensus: Low
Level of evidence: 1B
Comment: Although advanced radiographic OA has been clearly shown to be a major cause of failure of IAHA,18,22,51 numerous guidelines failed to specify the radiological stage that is ideally indicated for IAHA.49-53 The majority of voters considered that in the absence of another therapeutic alternative (e.g., contraindication to surgery), in the event of moderate pain or if the patient wishes it (desire not to have surgery or to delay), it is appropriate to offer IAHA in advanced radiological stages. They thus agreed with the opinion of Bhadra et al., 47 who insisted on the importance of considering the patient’s decision.
IAHA can be considered in symptomatic patients with mild-to-moderate patellofemoral OA (KL 2-3)
Median/Strength of recommendation: 9 /Strong for Level of consensus: High
Level of evidence: 2B
Comment: The response from 11 of 12 experts was that IAHA can be recommended in mild-to-moderate patellofemoral osteoarthritis (PFOA). The open-label studies that have been designed to assess the effectiveness of IAHA in patients with PFOA54,55 suggested beneficial effects up to 1 year. Similar findings were reported by Perruchet et al. 22 with a single injection of cross-linked HA, HANOX-M-XL. Conversely, a double-blind sham injection-controlled trial failed to demonstrate a beneficial effect of a single 6-ml injection of Hylan GF-20 in chondromalacia patella. 55
IAHA can be considered in symptomatic patients with advanced PF OA (KL 4)
Median/Strength of recommendation: 6/Conditionally recommended Level of consensus: High
Level of evidence: 2B
Comment: The use of IAHA in severe PFOA was conditionally recommended by 11 members. In 88 patients treated with 5 weekly IA injections of linear HA, Zhang et al. 54 found no difference in effectiveness between mild-to-moderate and advanced PF OA up to 4 weeks, but a much longer lasting effect in early than in advanced disease. Perruchet et al. 22 reported, in patients treated with a single IA injection of HANOX-M-XL, a similar duration of efficacy was observed in KL1-2 and KL3-4–isolated PFOA. However, in patients with PFOA associated with TFOA, a significant longer duration of efficacy was found in KL1-2 versus KL3-4. Nevertheless, treatment of severe PFOA, including surgery, is often disappointing. So, the taskforce concluded it is worth trying the injections before considering surgery, provided that the patient is informed of the risk of treatment failure.
IAHA can be considered in symptomatic early knee OA
Median/Strength of recommendation: 9/Strong for Level of consensus: High
Level of evidence: 5
Comment: In symptomatic patients, VS can be considered as soon as the diagnosis has been made either based on radiological features or at an earlier pre-radiological stage at which OA lesions can only be detectable with MRI or computed tomography (CT) arthrography. The concept of early OA and its management have been the subject of numerous publications recently.57-60 We defined early OA based on 3 sets of criteria.(1) pain, symptoms/signs, self-reported function, and quality of life using tools such as the Knee injury and Osteoarthritis Outcome Score (KOOS): scoring ≤85% in at least 2 of these 4 categories; (2) clinical examination confirming joint line tenderness and or crepitus; and (3) knee radiographs: Kellgren and Lawrence (KL) grade of 0 or 1. The key point is the notion of “window of opportunity,” which should imply starting treatment as early as possible once diagnosis is made. All, but 1 member, subscribed to this theory.
VS can be considered in knee OA with meniscocalcinosis
Median/Strength of recommendation: 8.5/Strong for Level of consensus: High
Level of evidence: 5
Comment: The use of VS to treat knee OA patients with radiographic meniscocalcinosis (MC) was strongly recommended by the group. MC is frequent in subjects over 50 years, reaching 50% after 90 years. 61 Of total, 80% of the knees affected by MC are associated with OA. The experts, however, clarified that IAHA was not appropriate in the event of an attack of acute exacerbation of chondrocalcinosis.
IAHA can be considered as a symptomatic treatment in post-traumatic knee OA
Median/Strength of recommendation: 8/Moderate for Level of consensus: High
Level of evidence: 5
Comment: This recommendation was approved by 10 of 12 experts. Post-traumatic OA is the most frequent cause of knee OA in young adult patients. Worldwide, 10% to12% of the OA cases are post-traumatic in etiology. 62 After injury, in addition to the mechanical stress, inflammatory and catabolic mediators (tumor necrosis factor [TNF]-α, interleukin [IL]-1β, matrix metalloproteinase [MMP]-1,13) are released and have both immediate and longer lasting effects. Inflammatory cytokine levels gradually fall but remains above the normal values in synovial fluid (SF) long after the initial knee injury. Studies of SF demonstrated abnormalities in glycoaminoglycans, lubricin, and type 2 collagen beyond 1 year post-injury, leading to progressive cartilage loss and the development of post-traumatic OA. 63 The conclusion of the working group was that, due to the anti-inflammatory and potentially chondroprotective effects of the HA molecule, IAHA is indicated to treat post-injury OA, at the earliest.
IAHA can be considered for primary prevention in post-traumatic knee OA
Median/Strength of recommendation: 6/ Conditionally recommended Level of consensus: No consensus
Level of evidence: 5
Comment: Primary prevention means IAHA injection after injury before the development of cartilage lesion prevents the onset of OA. The participants failed to find common ground on this subject. Some have suggested that HA has chondroprotective potential.42-44 So despite the absence of formal proof, not using IAHA could be a lost opportunity for these patients. Others disagreed with this position and the proposed recommendation was not agreed upon. In summary, the LoE seems too low to recommend the use of IAHA to prevent the onset of OA following joint trauma.
IAHA can be considered for secondary prevention in post-traumatic knee OA
Median/Strength of recommendation: 5/Conditionally recommended Level of consensus: Low
Level of evidence: 5
Comment: In patients with a diagnosis of cartilage lesion after knee trauma, IAHA was recommended by the taskforce, only under certain conditions, to prevent progression of cartilage damage in professional sportsmen and in patients with multiple risk factors of OA progression.
IAHA can be considered in patients with knee OA and mild-to-moderate SF effusion (1 to 10 ml)
Median/Strength of recommendation: 8/Moderate for Level of consensus: High
Level of evidence: 1B
Comment: The working group considered, with a high LOC, that a synovial effusion of moderate volume was not obstacle contraindication for performing VS. Several studies have in fact demonstrated this.23,26
IAHA can be considered in patients with knee OA and large SF effusion (>20 ml)
Median/Strength of recommendation: 3/Weak against Level of consensus: Low
Level of evidence: 2B
Comment: Most experts recommended against using IAHA in patients with large SF effusion. In 137 knee OA patients with SF effusion evidenced by ultrasonography, IAHA after arthrocentesis led to an improvement in pain and function scores at 1 and 6 months after treatment, with a significant association of SF depth with the score variations. Each centimeter increase in the effusion diameter was associated with a decrease in the 1- and 6-month post-treatment improvement percentage. 64 In case of large SF effusion, the working group advised an IA injection of corticosteroid a few weeks (i.e., 2-6 weeks) prior to IAHA injections.
IAHA can be considered in patients with knee OA flare
Median/Strength of recommendation: 2.5/Moderate against Level of consensus: High
Level of evidence: 5
Comment: For the same reasons, there was a high LOC for recommending against the use of IAHA in patients with knee OA flare. Acute flare must be treated with ice, NSAIDs, and IA steroids. 45 However, 1 study showed beneficial effects of IAHA versus arthrocentesis in flare patients with no safety concerns. 65
IAHA can be considered in patients with symptomatic knee OA with mild-to-moderate valgus/varus malalignment
Median/Strength of recommendation:8/Moderate for Level of consensus: High
Level of evidence: 5
Comment: TFOA is often associated with mild or moderate valgus or varus malalignment and increased risk of knee OA progression is demonstrated in these patients with varus or valgus malalignment. 66 A high LOC was obtained for recommending IAHA in patients with mild or moderate malalignment.
IAHA can be considered in patients with symptomatic knee OA with severe valgus/varus malalignment
Median/Strength of recommendation: 5/Conditionally recommended Level of consensus: Low
Level of evidence: 5
Comment: Significant malalignment, whether the cause or the consequence of OA, causes significant mechanical stress on the tibiofemoral compartment involved leading to a higher risk of disease progression. 66 The experts concluded that IAHA could be offered conditionally, if the patient refuses or does not respond favorably to other therapeutic modalities.66-69
IAHA can be considered in knee OA patients with asymptomatic meniscus tear
Median/Strength of recommendation: 8.5 /Strong for Level of consensus: High
Level of evidence: 5
Comment: Meniscal tear is a very frequent feature in knee OA 70 strongly associated with cartilage loss but weakly associated with knee pain. 71 The experts concluded IAHA can be considered in knee OA with asymptomatic meniscal tears.
VS can be considered in knee OA patients with symptomatic meniscus tear
Strength of recommendation: 7/Weak for Level of consensus: Low
Level of evidence: 5
Comment: A low LOC was obtained for recommending IAHA in patients with knee OA and symptomatic meniscus tear. The experts proposed to use of IAHA only after achieving a multimodal conservative treatment including physical and/or manual therapy, NSAIDs, and IA steroid injection.72,73
IAHA can be considered in knee OA patients with symptomatic meniscus extrusion
Median/Strength of recommendation: 6.5/Weak for Level of consensus: No consensus
Level of evidence: 5
Comment: Medial and lateral meniscal extrusions are strong predictors of progression of knee OA and the need for total knee replacement. 74 Meniscal extrusion disrupts the hoop stress mechanism necessary for load distribution and force of transmission through the meniscus leading to increased stress on the joint 75 which favors cartilage degradation. As meniscal extrusion is associated with a higher risk of bone marrow lesion (BML), 76 the working group members were unable to agree on the benefit of using IAHA in these patients. Those who were in favor of IAHA emphasized the risk of rapid OA progression due to meniscal extrusion, as it has been shown that longitudinal increase in meniscal extrusion and reduction in tibial plateau coverage and overlap distance were associated with structural, but not with symptomatic OA progression. 76 Those who recommended against pointed out that the mechanism of action of HA made it unlikely to be effective in such circumstances.
IAHA can be considered in patients with knee OA with mild-to-moderate femoral and/or tibial bone marrow edema
Median/Strength of recommendation: 7/Weak for Level of consensus: Low
Level of evidence: 5
Comment: BMLs, including bone marrow edema (BME), are very frequent MRI features in knee OA. The precise causes of OA-BMLs are uncertain, but several risk factors have been identified for their presence or progression, varus TF malalignment, obesity, dietary lipid intake, and high physical activity 77 to name a few. BMLs are associated with pain and subjects with knee OA who have BMLs are 2 to 5 times more likely to have knee pain than those without. 78 Nevertheless, despite a significant association between BMLs and pain, the extent to which BMLs contribute to OA pain remains unclear and varies between patients and over time. 79 For this reasons, the task force recommended considering IAHA in patients with mild-to-moderate BME.
IAHA can be considered in patients with knee OA with large femoral and/or tibial BME
Median/Strength of recommendation: 4.5/Conditionally recommended Level of consensus: Moderate
Level of evidence: 5
Comment: The experts conditionally recommended IAHA in patients with large tibial and/or femoral BME. In an animal model of OA, subchondral BME-induced hypersensitivity of the sensory afferents innervating the bone marrow is probably responsible, at least in part, for OA pain. 80 However, Cai et al. 80 showed that neither enlargement nor regression of total BME size over 6 and 24 months was associated with a change in knee pain and function over the same time intervals.
IAHA can be considered in knee OA patients with symptomatic popliteal cysts
Median/Strength of recommendation: 4.5/Conditionally recommended Level of consensus: No consensus
Level of evidence: 5
Comment: No consensus was obtained. The group advised to manage symptomatic popliteal cysts with ultrasound-guided percutaneous aspiration followed by intra-articular or intra-cyst corticosteroid injection. 82
IAHA can be considered in knee OA patients with moderate knee pain (>3 to ≤7/10)
Median/Strength of recommendation: 9/Strong for Level of consensus: Unanimous
Level of evidence: 1A
Comment: Not surprisingly, unanimous agreement was obtained to recommend the use of IAHA in knee OA patients with mild-to-moderate knee pain, as evidenced by a pain level of 3 to 7 on a 1- to 10-point numerical scale.
IAHA can be considered in knee OA patients with very little knee pain (≤3/10)
Median/Strength of recommendation: 7/Weak for Level of consensus: Low
Level of evidence: 5
Comment: On the contrary, the LOC was much lower regarding the recommendation to treat patients having only a very low level of pain with IAHA. Experts nevertheless highlighted that patient choice was paramount and that it was unethical (or unfair) to refuse the treatment if the patient requested it.
IAHA can be considered in knee OA patients with very severe knee pain VAS
Median/Strength of recommendation: 7/Weak for Level of consensus: Low
Level of evidence: 5
Comment: High level of pain being mostly associated with very advanced OA and OA flare, the experts recommended to use VS only in patients not falling within the scope of these 2 conditions
IAHA can be considered in knee OA patients with inflammatory pain
Median/Strength of recommendation: 3/Weak against Level of consensus: Low
Level of evidence: 5
Comment: Inflammatory pain, characterized by pain at rest causing nocturnal pain associated with loss of sleep, prolonged morning stiffness, and often associated with effusion, joint swelling, and increased warmth in the knee, are signs of an OA flare-up. Experts agreed that OA flare should be treated with rest, ice, NSAIDs, and IA steroid injections and recommended not to use IAHA, despite 1 study showing improvement in 31 patients with OA flare treated with repeated injections of Hylan GF-20. 65
IAHA can be considered in knee OA patients with neuropathic pain
Median/Strength of recommendation: 5/Conditionally recommended Level of consensus: No consensus
Level of evidence: 2B
Comment: Chronic inflammation due to OA can cause alterations in the peripheral nervous system of the joint as a whole. The subchondral bone, rich in sensory nerve fibers, is subjected to increasing stress in advanced stages of OA, developing a neuropathic pain component. 82 It is estimated that 20% to 28.6% of patients suffering from knee OA have neuropathic pain. 83
No consensus was obtained to recommend IAHA in patients with neuropathic pain. A study by Tiendrebeogo et al. 84 found that neuropathic pain was associated with pain severity but did not influence the response to IAHA, in a post hoc analysis of a 6-month prospective randomized study comparing 2 HA viscosupplements. Furthermore, the authors showed that IAHA reduced some neuropathic pain features, especially itching, sting hypoesthesia, and burning.
IAHA can be considered in knee OA patients with widespread nociplastic pain (i.e., fibromyalgia)
Median/Strength of recommendation: 4/Conditionally recommended Level of consensus: Low
Level of evidence: 5
Comment: Widespread pain is a common symptom in OA. 86 Pain mechanisms in knee OA are multifactorial with sensitization of the peripheral and central nervous system, poor sleep, and psychological variables that add to the nociceptive component due to synovial inflammation and structural changes in the subchondral bone.56,87,88 Carlesso et al. 88 showed that the frequency and severity of knee pain contribute to the occurrence of widespread pain independently of structural severity. However, the same authors showed that the initial presence of widespread pain was not associated with worsening knee pain (adjusted OR = 1.15, 95% CI = 0.89-1.48, P = 0.30) in 1,772 subjects studied for 2 years. 89 The prevalence of widespread pain was 30% and was associated with worse scores in all KOOS subscales after adjustment for age, gender, and radiographic changes. 86 The working group conditionally recommended the use of IAHA in patients with widespread pain. They emphasized the need for multimodal care, based on the treatment of sleep disorders, rehabilitation, individualized physical activity, psychotherapy, and therapies aimed at treating chronic pain using duloxetine. 90
Discussion
The main question today regarding IAHA VS is not whether it works, but rather in whom it works or in what type of patients it is most likely to be effective. These new recommendations from the EUROVISCO group focus on the use of IAHA according to the individual characteristics of each patient. Indeed, OA is an extremely polymorphic disease and affects an extremely heterogeneous population. Individualized care based on the specific characteristics of each patient is essential both to ensure a good result and to obtain good patient compliance with treatment. It is obvious to say that we do not treat incipient post-traumatic OA in a young subject without any comorbidity the same way as an advanced OA in an elderly patient with multiple treatments and comorbidities and with multiple joints affected by OA.
These recommendations are only intended to help practitioners in their decision whether or not to carry out IAHA VS in different clinical situations that they encounter in their daily activities.
The main limitation of these recommendations is that they rely more on expert opinion than on evidence-based medicine (26 of 35 recommendations). This means that more efforts are required to study the effects of IAHA in different OA phenotypes to better understand which subgroup of patients are IAHA responders. Another limitation is that certain pathologies associated with OA have probably not been identified and addressed. For example, we have not made a recommendation for patients with widespread pain such as in fibromyalgia or for patients with sarcopenia or muscle impairment resulting from post-traumatic immobilization or surgery. Furthermore, we have not addressed the use of IAHA in patients with radiological OA but presenting with pain generated by muscle spasms or tendinopathy. The indication of IAHA in the presence of fixed flexion of the knee remains also questionable.
The major limitation of these recommendations is that many of the factors discussed here frequently coexist. The most common example is the presence of large bone marrow lesion on the MRI. Indeed, the presence of BMLs is frequently associated with severe joint space narrowing, obesity, and significant mechanical stresses such as those due to a meniscal lesion or a varus deformity. While recommendations have been given for individual scenarios, they may not be applicable in multiple coexisting presentations. Another limitation of this type of recommendation is that it does not take into account the characteristics of the IAHA viscosupplements used. However, the literature shows that HA products are different from each other and that it is not possible to formally extrapolate the results obtained with one product to other viscosupplements 90 for any given clinical presentation. The key strengths of our expert consensus guidelines are that they provide answers to questions that physicians address every day in their daily practice. One example is that IAHA can be used at any age, particularly in the elderly due to its excellent benefit/risk ratio. Another key message is that IAHA is recommended in patients with comorbidities (i.e., type I or type II diabetes) due to both its excellent tolerance and its ability to reduce the use of NSAIDs. VS is particularly recommended in moderate OA, both symptomatically and radiologically, but can be used conditionally in severe OA situations because we lack studies on older people with severe OA. Moderate valgus or varus, as well as moderate joint effusion, are not contraindications to VS. It is not recommended to use IAHA in OA flare, which must be treated with cryotherapy, IA corticosteroids, and anti-inflammatory drugs. Surprisingly, the experts were much more divisible in their opinions regarding the use of IAHA in patients with little or no symptoms and for the prevention of anatomical worsening, despite increasing evidence of a potentially chondroprotective effect40,91-97 and the ability to postpone knee replacement. 11
It is nevertheless essential to specify that VS is only 1 element of the management of knee OA that must be integrated into a combination of non-pharmacological and pharmacological modalities adapted to the individual situation of patients.44,51 The experts were also complimentary of the fact that the effectiveness of IAHA could be improved if combined with manual therapy including muscle strengthening exercises.
In conclusion, this is the first time that recommendations have been made to assist physicians in their decision to use IAHA to treat knee OA in patients with comorbidities. These recommendations will help improve the effectiveness of IAHA and patient satisfaction by giving physicians guidelines to select the best candidate for this treatment.
Footnotes
Authors’ Note
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing, we confirm that we have followed the regulations of our institutions concerning intellectual property.
Acknowledgment and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We wish to draw the attention of the Editor to the following facts that may be considered as potential conflicts of interest related to the subject and to significant financial contributions to this work. Yves Henrotin: received honorarium from Menarini, Flexion Therapeutics, IBSA, Bioiberica, Expanscience, Royal Canin, Magpharm, Pfizer, Fidia, LABRHA, and Tilman SA and Grunenthal, Artialis, KiOmed Pharma, and Genequine for consultant services. Pascal Richette received fees from BioIbérica, Fidia, IBSA, Expanscience, Genévrier, Sanofi, Rottapharm, Servier, Flexion Therapeutics, and Ménarini. Hervé Bard received speaker and expert fees from Sanofi, Pfizer, Labrha, Expanscience, and TRB Chemedica. Thierry Conrozier received honorarium from Sanofi, MEDAC, Fidia, and Labrha for expert or consultant services. Xavier Chevalier received fees as a Genevrier Board member, Sanofi-Aventis expert, member of the IBSA foundation, speaker in IBSA and Labrha meetings, and Moebius and Flexion Therapeutics consultant. Alberto Migliore received consulting fees from AbbVie, BMS, MSD, Fidia, Sanofi, IBSA, Pfizer, and Labrha, for national and international studies and courses. Jordi Montfort received consulting fees from Sanofi and Bioiberica. Dominique Baron received speaker fees from LCA and Expanscience. Demirhan Diraçoglu received speaker fees from LABRHA. Mats Brittberg is a Member Advisory board of Episurf Medical AB, Xintela AB, Magellan Stem Cells PTY Ltd, Cline Scientific AB, Askel Healthcare Ltd, and Vanarix SA; Participation Speaker’s bureau for Arthrex and for Anika Therapeutics; and Member editorial board Osteoarthritis & Cartilage, Editor-in-Chief CARTILAGE.
Ethical Approval
This review did not require an ethical board approval because patients were not involved in the design or conduct or reporting or dissemination plans of this research.
Patient Consent for Publication
Not required.