
Abstract
Objective
To analyze the prognostic factors for clinical outcomes and cartilage regeneration after the implantation of allogeneic human umbilical cord blood mesenchymal stem cell (hUCB-MSC) for treating large-sized cartilage defects with osteoarthritis.
Design
This study is a case-series with multiple subgroup analyses that divides the included patients into multiple subgroups based on various factors. Overall, 47 patients who underwent hUCB-MSC implantation were included. The patient-reported outcomes, magnetic resonance imaging (MRI), and second-look arthroscopy were used to assess the outcomes.
Results
Combined realignment surgery significantly correlated with clinical outcomes, particularly pain. No other factors significantly influenced the clinical outcomes in short-term period. Subgroups with large defect sizes or meniscal insufficiency showed significantly poor MRI and arthroscopy outcomes (MRI, P = 0.001, P = 0.001; arthroscopy, P = 0.032, P = 0.042). The logistic regression showed that patients with a 1 cm2 larger defect size were 1.91 times less likely to achieve favorable MRI outcomes (P = 0.017; odds ratio [OR], 1.91). Cut-off value to predict the poor outcome was >5.7 cm2 (area under the curve, 0.756). A cartilage defect size >5.7 cm2 was the major poor prognostic factor for cartilage regeneration on MRI (P = 0.010; OR, 17.46). If the postoperative alignment shifted by 1° opposite to the cartilage defect, it was 1.4 times more likely to achieve favorable MRI outcomes (P = 0.028; OR, 1.4).
Conclusion
Combining realignment surgery showed a better prognosis for pain improvement. Cartilage defect size, meniscal function, and postoperative alignment are significant prognostic factors for cartilage regeneration. A cartilage defect size >5.7 cm2 was significantly related to poor cartilage regeneration.
Introduction
Articular cartilage defects have poor potential for spontaneous healing, often leading to the development of osteoarthritis.1,2 Various cartilage repair procedures, including bone marrow stimulation and cell-based techniques, are currently being employed to address cartilage defects.3,4 Among emerging cartilage treatments, mesenchymal stem cell (MSC) treatment has drawn considerable attention and interest. MSCs play a role in chondrogenesis owing to their chondrogenic potential and paracrine actions that migrate cells into injury sites and create a favorable environment for cartilage regeneration.5,6 MSCs have different characteristics depending on the harvest site.3,7 Human umbilical cord blood mesenchymal stem cells (hUCB-MSCs) have several distinct advantages over other MSCs as a source for therapeutic use, including noninvasive cell collection, low immunogenicity, and high expansion capacity. 8 Due to these favorable characteristics, hUCB-MSCs can serve as off-the-shelf allogeneic stem cell products. Therefore, the possibility of a 1-stage surgery without the requirement for autologous tissue harvesting can present significant benefits to patients.
Current cartilage treatment options are more suitable for treating localized, focal defects in relatively young patients rather than large, full-thickness cartilage defects in the osteoarthritic joints of older patients. Bone marrow stimulation techniques, such as microfracture, are commonly used, but have demonstrated inferior outcomes for large cartilage defects in osteoarthritic patients.9-11 Autologous chondrocyte implantation (ACI) is typically recommended for treating larger lesions, especially in young patients. However, ACI procedures are less frequently recommended for older patients because of the diminished reparative potential of autologous chondrocytes.10,12 Treatments using autologous mesenchymal stem cells are not exempt from concerns associated with cell senescence when used in older patients.13,14 Therefore, in these contexts, hUCB-MSC implantation was developed and clinically utilized, showing promising results.15-19
Several established risk factors are associated with unfavorable outcomes following current cartilage repair procedures.2,20,21 Old age, cartilage defect size, malalignment, and meniscal insufficiency are the commonly mentioned risk factors. However, since hUCB-MSC implantation is indicated for large cartilage defects with degenerative changes, it is likely that most patients undergoing this treatment have multiple risk factors. The specific factors that have a significant impact on the clinical outcomes and cartilage regeneration in patients with multiple risk factors remain unclear.
Therefore, we hypothesized that the factors that actually act as poor prognostic factors could be different in situations in which there is only one risk factor in the treatment of focal cartilage defects and in situations in which there are multiple risk factors in the treatment of large-sized defects with osteoarthritis. This study aimed to analyze the prognostic factors for poor clinical outcomes and cartilage regeneration after hUCB-MSC implantation for the treatment of large-sized defects in osteoarthritis.
Methods
Patient Selection
Patients who underwent allogeneic hUCB-MSC implantation between July 2018 and February 2022 were retrospectively evaluated. Patients lost to follow-up or with no patient-reported outcomes were excluded. The implantation of hUCB-MSCs was performed in patients over 40 years of age with full-thickness International Cartilage Repair Society (ICRS) grade IV cartilage lesions on the femoral condyles. 22 A combined realignment surgery was performed when the malalignment was more than 5 degrees. Patients with Kellgren and Lawrence grade IV osteoarthritis, 23 knee ligament injuries, metabolic arthritis, or joint infections were excluded. A total of 51 consecutive patients who underwent hUCB-MSC implantation during this period, 47 and 33 patients, were included in the 1-year and 2-year outcome analyses, respectively. Follow-up magnetic resonance imaging (MRI) was performed in 43 patients at a mean follow-up of 12.7 months and second-look arthroscopy was performed in 34 patients at a mean follow-up of 13.2 months. This study was reviewed and approved by the institutional review board of our institution (Gangnam Severance Institutional Review Board, 3-2023-0289).
Preparation of hUCB-MSCs
For hUCB-MSCs, CARTISTEM® (Medipost, Seongnam-si, Gyeonggi-do, South Korea), an off-the-shelf cartilage regeneration product, was used. This product was approved for cartilage regeneration by the Korea Food and Drug Administration in January 2012 and consists of 1.5 mL of hUCB-MSCs (7.5 × 106 cells/vial) and 4% hyaluronic acid hydrogel. The therapeutic dose was determined by preoperative measurement of the cartilage defect size on MRI. Notably, 500 μL/cm2 was recommended according to the manufacturer’s instructions. After hUCB-MSCs and HA were combined, the mixture was transferred to a syringe for implantation.
Surgical Technique and Postoperative Management
The surgical procedures were performed by a single senior surgeon. Diagnostic arthroscopy was performed, and articular cartilage and meniscus status were evaluated. After inspection of the intra-articular structures, procedures such as arthroscopic meniscectomy or debridement were performed, if needed. In cases of malalignment, an additional combined realignment surgery was performed before the implantation of hUCB-MSCs. Biplanar medial open-wedge high tibial osteotomy (HTO) was performed for medial compartment cartilage lesions. 24 Contrastingly, medial closed-wedge distal femoral osteotomy (DFO) was performed to address cartilage lesions for the lateral compartment. After all necessary procedures were completed, hUCB-MSCs were implanted. A mini-arthrotomy was performed on the parapatellar area of the involved compartment through a longitudinal incision measuring approximately 3 to 5 cm. The cartilage lesions on the femoral condyles were exposed via further dissection and arthrotomy ( Fig. 1A ). After preparing the cartilage lesions by curettage of the damaged cartilage, multiple drill holes of 2 different sizes (4 mm × 7 mm and 2 mm × 7 mm [diameter × depth]; approximately 2 mm apart) were made in the subchondral bone ( Fig. 1B and C ). The prepared mixture of hUCB-MSCs and HA was subsequently implanted into the holes and articular surfaces ( Fig. 1D ).
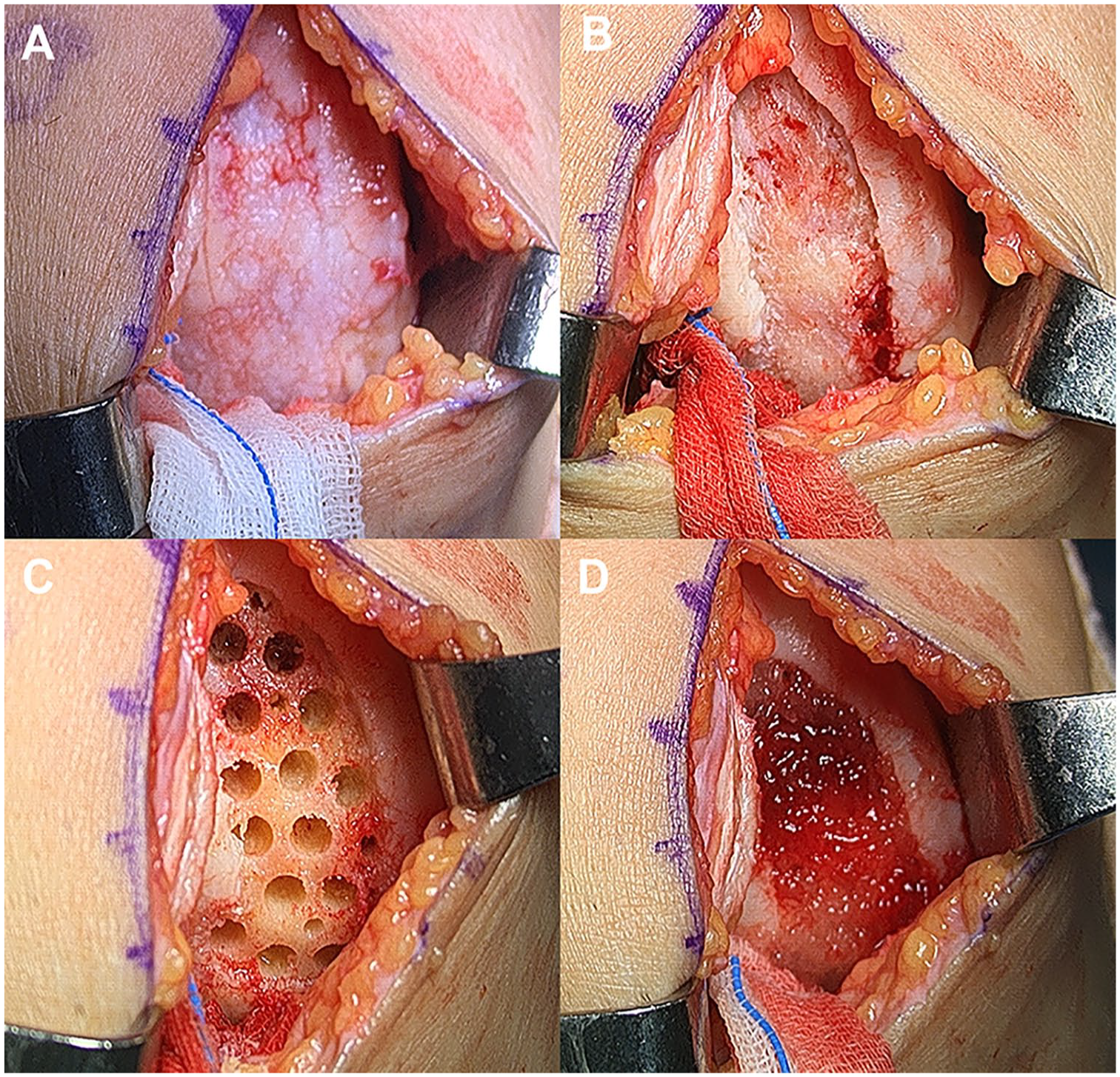
Implantation of hUCB-MSCs: (
Postoperatively, knee motion was restricted during daily activities using a hinged knee brace for a total of 10 weeks. Continuous passive range of motion exercise was recommended immediately after surgery, starting at 60 degrees and increasing by 30 degrees every two weeks, with the goal of achieving 120 degrees to full range of motion by six weeks postoperatively. Weight-bearing was restricted for 10 weeks using crutches. Toe-touch weight bearing was allowed for initial 4 weeks, and partial weight bearing of approximately 50% was allowed for extra 6 weeks.
Clinical, Radiologic, and Arthroscopic Evaluations
Clinical assessments were performed preoperatively and at 1 and 2 years postoperatively using the visual analogue scale (VAS), Lysholm score, 25 International Knee Documentation Committee (IKDC) subjective score, 26 and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. 27 We defined minimal clinically important differences (MCID) for clinical outcome scores as 27 for VAS, 10.1 for Lysholm, 16.7 for IKDC, and 11.5 for WOMAC, according to previous studies.28,29 Each patient was assessed to determine whether they met the MCID criteria 1 or 2 years postoperatively.
Standing whole lower extremity radiographs were obtained preoperatively and 1 year postoperatively to evaluate the lower limb alignment. Mechanical tibiofemoral angles (mTFAs) were measured and denoted as positive if the weightbearing line passed through the compartment opposite to the cartilage defects ( Fig. 2 ).
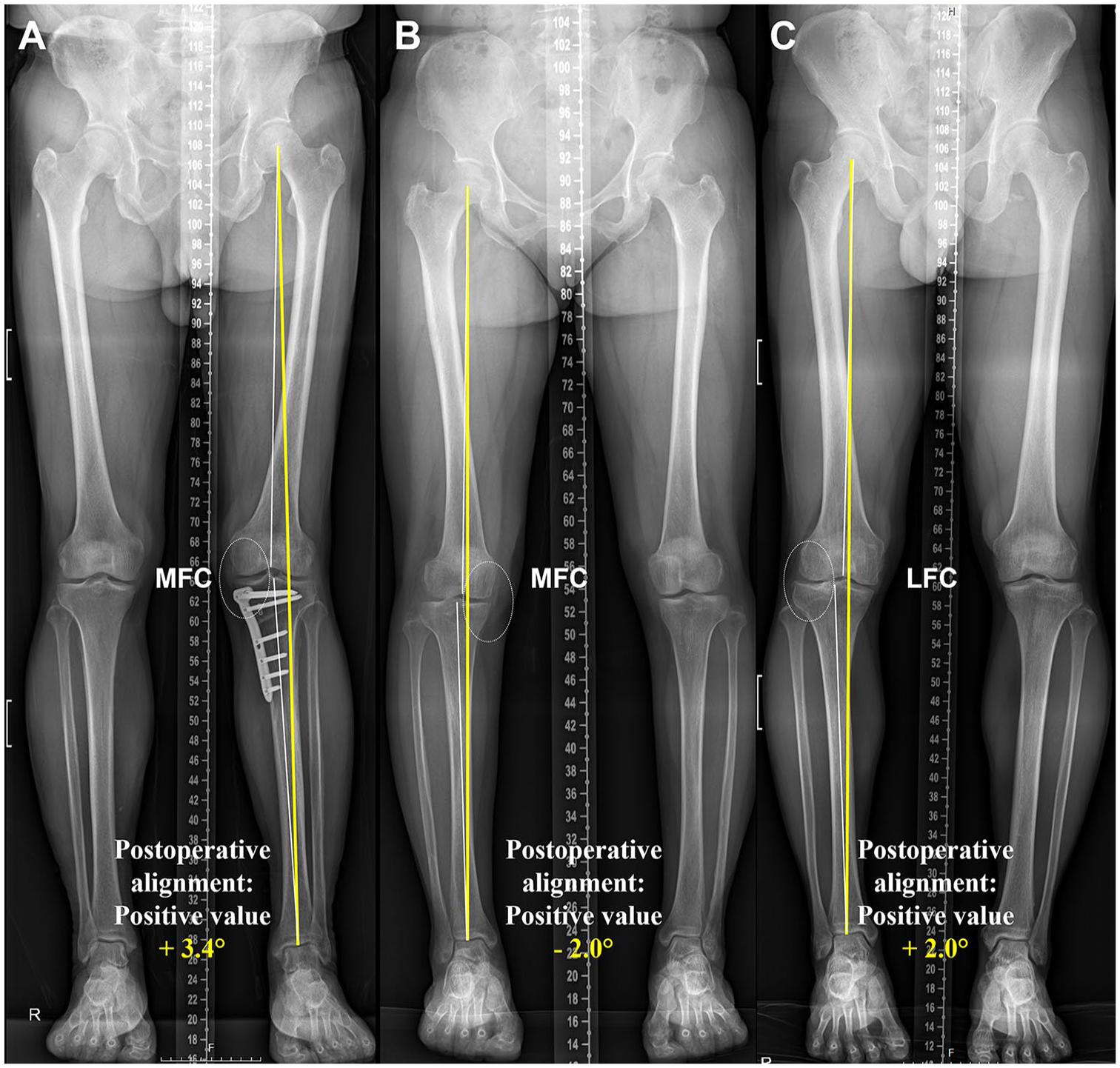
Measurement and denotation of postoperative alignment: (
Definition of Meniscal Extrusion/Function and Kissing Lesions
MRI evaluation included meniscal extrusion and the abundance of meniscal substances to comprehensively assess meniscal function. Meniscal extrusion was measured using the methods described in a previous study. 30 Meniscal extrusion >3 mm was defined as pathological meniscal extrusion.31,32 Patients with pathological meniscal extrusion or a definite meniscal substance deficiency due to abrasive destruction or subtotal meniscectomy during the surgical procedure were defined as having meniscal insufficiency. The remaining patients were assigned to the positive meniscal function group. During the arthroscopic procedure, the cartilage defect size was measured by length and width using a probe, and the severity of the cartilage lesions was classified according to the ICRS grading system. 33 Kissing lesions were defined as ICRS grade III or higher on both tibial and femoral articular surfaces.
Evaluation of Cartilage Regeneration
Cartilage regeneration was evaluated by MRI evaluation and second-look arthroscopy approximately 1 year postoperatively. Follow-up MRI was performed using a 3.0-T MRI scanner. The MOCART 2.0 scoring system was used to evaluate the repaired cartilage 34 ( Fig. 3A ). To avoid potential bias, an independent observer, a musculoskeletal radiologist, who was not involved in the patients’ care and was blinded to the study’s intentions, evaluated the repaired cartilage. Patients who needed hardware removal due to combined realignment surgery or additional arthroscopic surgery underwent diagnostic second-look arthroscopy ( Fig. 3C ). Cartilage regeneration was evaluated macroscopically using the ICRS Cartilage Repair Assessment (CRA) grading system. 35
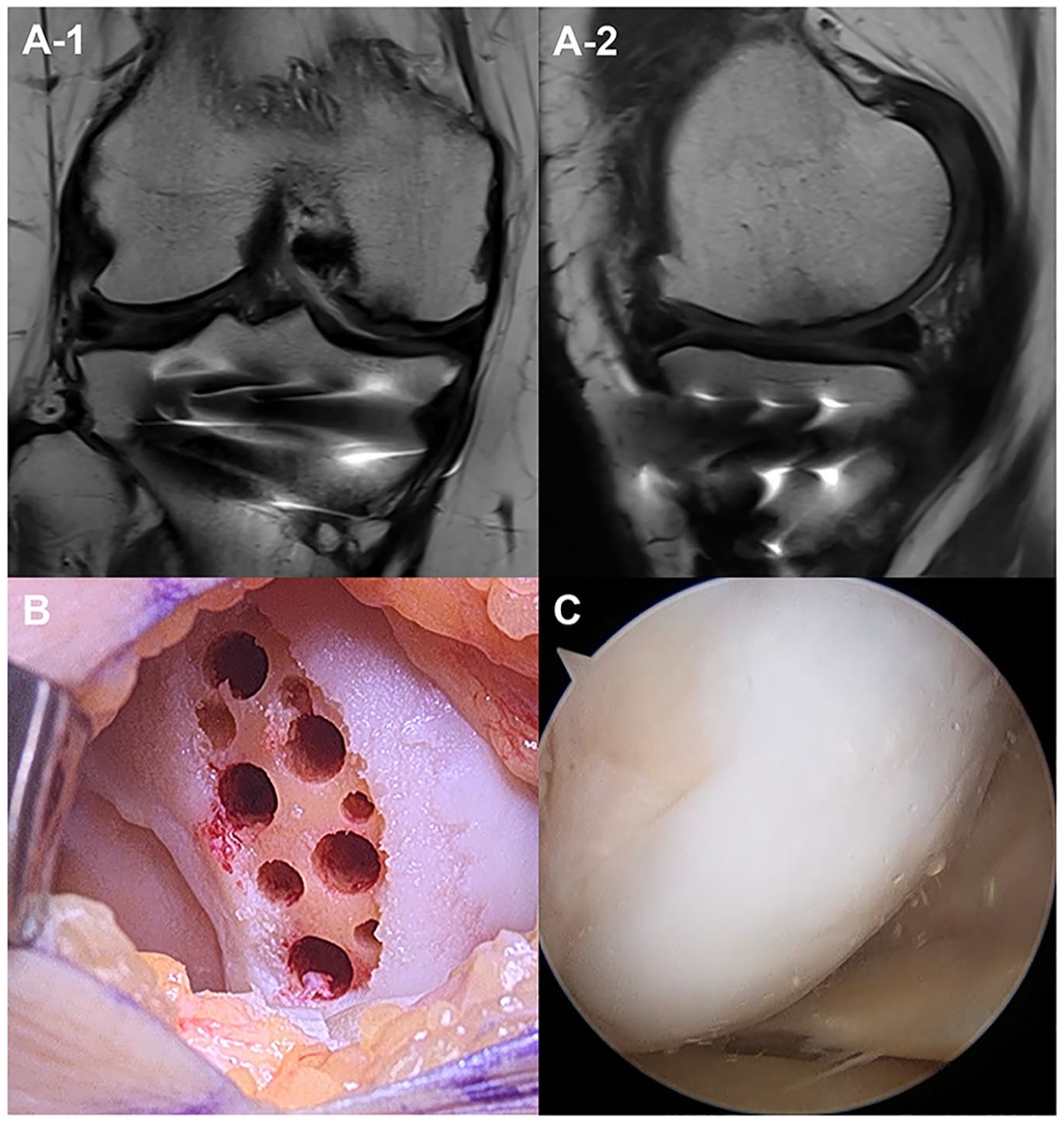
Postoperative assessment of cartilage regeneration. A 66-year-old woman with a cartilage defect on the medial femoral condyle was treated with implantation of hUCB-MSC and combined high tibial osteotomy. (
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (IBM, Armonk, NY), with statistical significance defined as P < 0.05. Values are presented as mean ± standard deviation unless otherwise indicated. The VAS, Lysholm, IKDC, and WOMAC scores were used as the primary dependent variables for clinical outcomes. MOCART and ICRS CRA scores were the dependent variables for assessing cartilage regeneration. The Shapiro-Wilk test was used to check the normality of the variables. A paired t test was used to evaluate the differences between preoperative and postoperative values. The patients were divided into subgroups based on 5 factors (age, combined realignment surgery, cartilage defect size, presence of kissing lesions, and meniscal function). We defined the old age group as age >55 years because the mean age of the patients was approximately 55 (55.4 ± 7.4) years. The criterion for cartilage defect size was set at 600 mm2 because the mean cartilage defect size was approximately 600 mm2 (626.1 ± 241.5 mm2). Differences in the clinical and cartilage regeneration scores between the groups were analyzed using the independent t test or Mann-Whitney U test. Differences in the MCID achievement rates were statistically analyzed using the chi-square tests. Multivariate logistic regression analyses were used to assess the factors independently associated with the MCID achievement rate for each clinical outcome.
Pearson’s correlation tests were performed to determine the factors that correlated with the follow-up MOCART and ICRS CRA scores. A multiple linear regression analysis was used to assess the factors independently associated with the MOCART and ICRS CRA scores as continuous dependent variables. A favorable follow-up MOCART score was set at >60. A multivariate logistic regression analysis was used to assess the factors independently associated with favorable follow-up MOCART scores. A receiver-operating characteristic (ROC) curve analysis was applied to obtain the optimal cut-off value for cartilage defect size, which can predict favorable cartilage regeneration on follow-up MRI.
Results
The demographic data of the included patients and the profiles of the cartilage defects and limb alignment were documented ( Tables 1 and 2 ).
Demographic Characteristics.
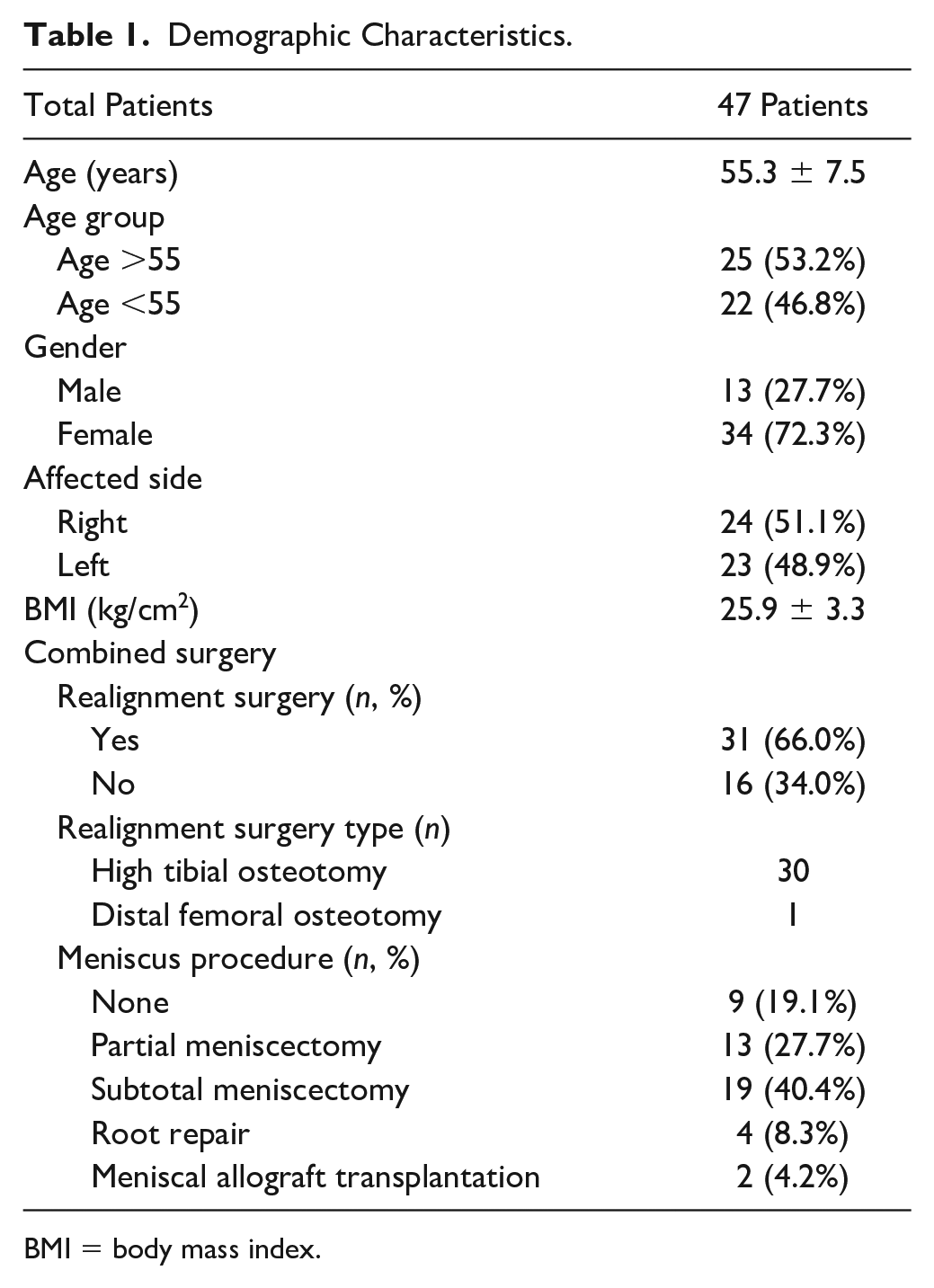
BMI = body mass index.
Profiles of Cartilage Defect, Meniscal Function, and Alignment.
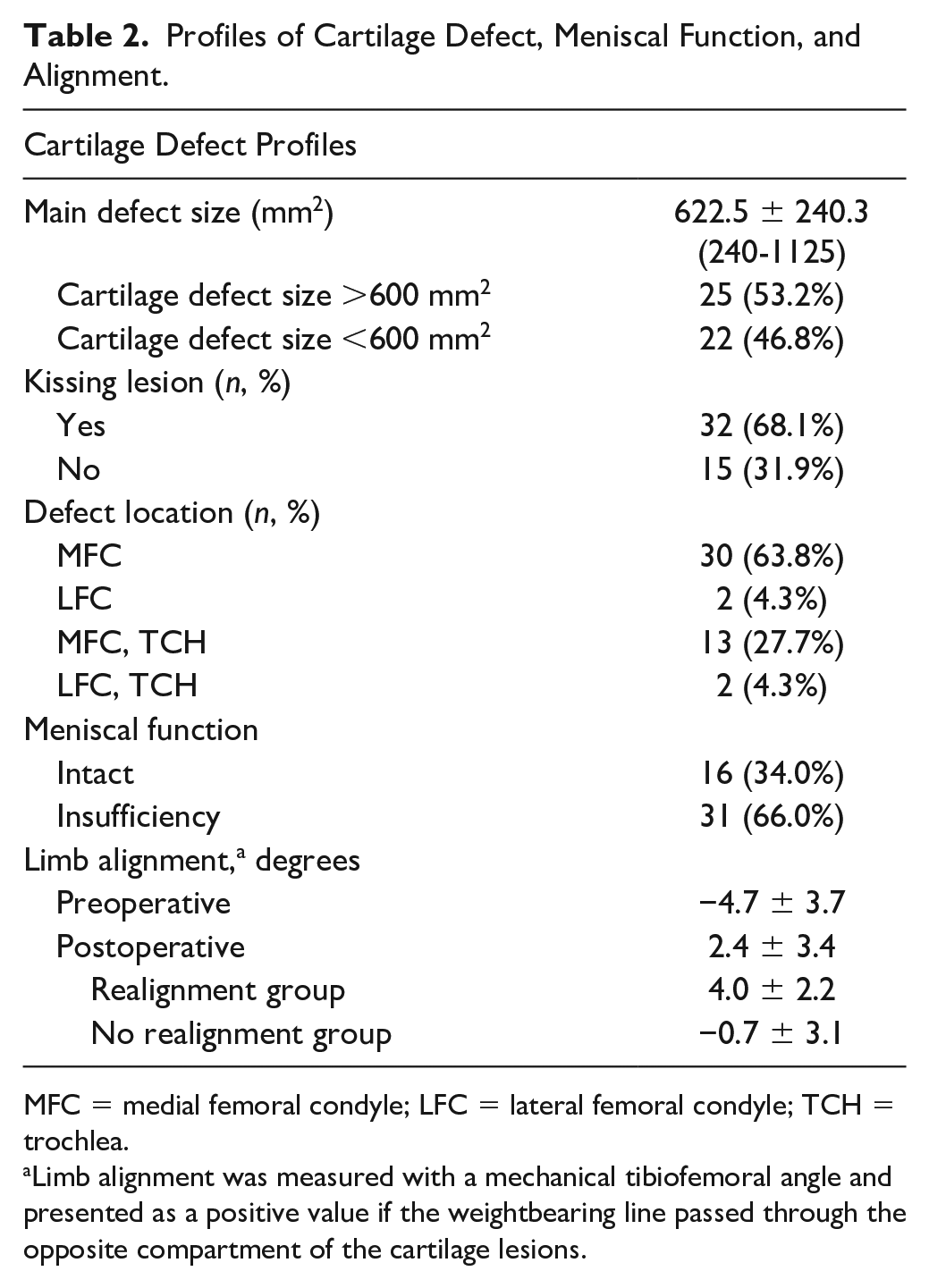
MFC = medial femoral condyle; LFC = lateral femoral condyle; TCH = trochlea.
Limb alignment was measured with a mechanical tibiofemoral angle and presented as a positive value if the weightbearing line passed through the opposite compartment of the cartilage lesions.
Clinical Outcomes and Subgroup Analysis
No major complications related to implantation or severe adverse events were observed during surgery or the follow-up period. Marked improvements in all clinical scores were observed postoperatively (1-year, P < 0.001; 2-year, P < 0.001) ( Fig. 4 ). No deterioration in clinical outcomes was seen between 1-year and 2-year postoperatively. The mean clinical scores improved between 1 and 2 years, with no statistical significance. None of the clinical outcomes differed significantly depending on defect location.
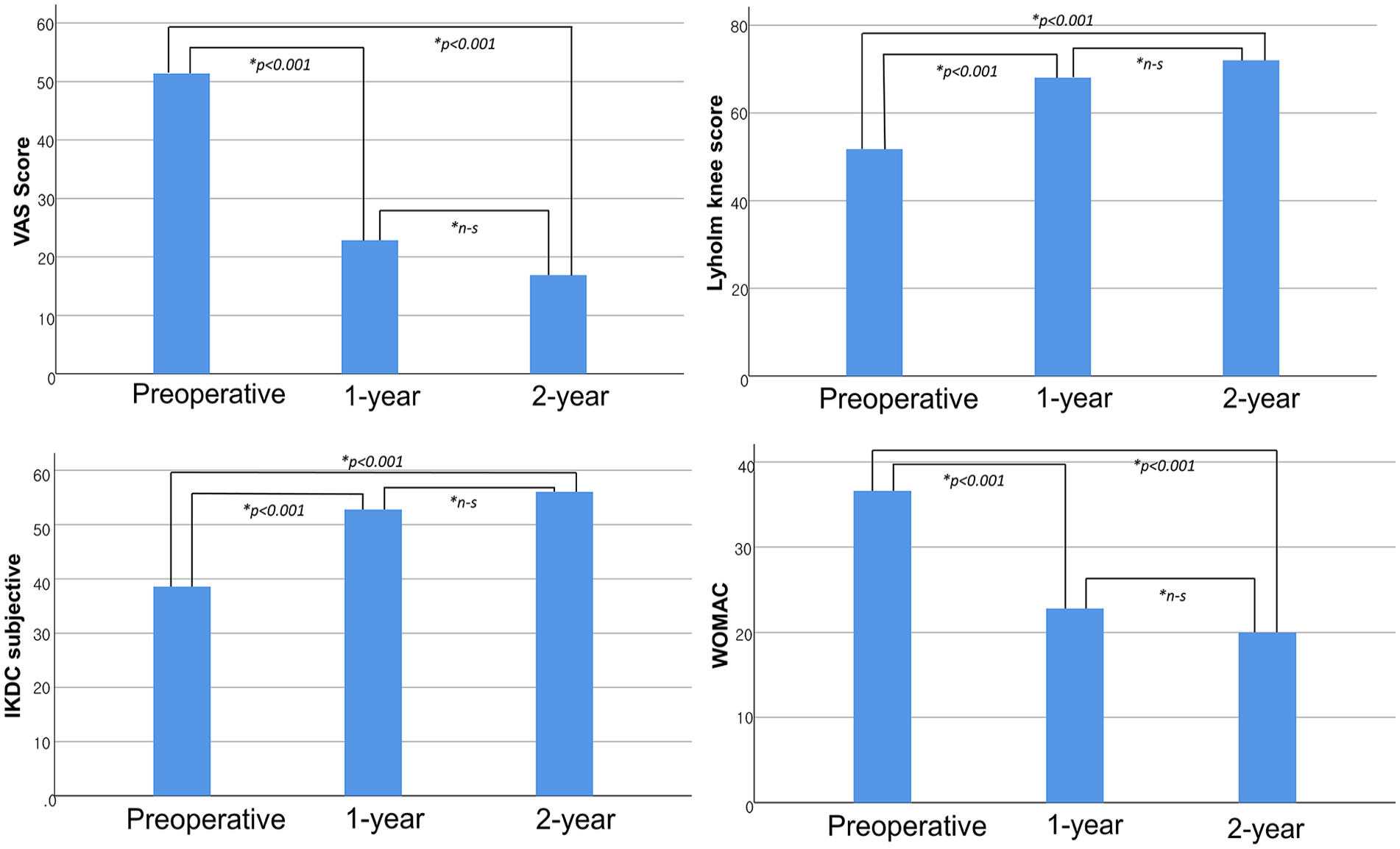
Mean clinical outcome scores at preoperative period, at 1-year follow-up, and at 2-year follow-up. n-s = not significant; VAS = visual analogue scale; IKDC = International Knee Documentation Committee; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index. *P-values were presented if values were significantly different.
In the subgroup analysis for patient age (age >55, <55 years), the preoperative VAS score was significantly higher in the old age group (59.1 ± 19.3 vs. 42.6 ± 17.6, P = 0.004) ( Table 3 ). The other preoperative and postoperative clinical scores at 1 year and 2 years were not significantly different between the groups. The improved VAS score was significantly higher in the older age group at 1 year (P = 0.015), but not at 2 years, because of the considerably poorer preoperative baseline VAS score.
Clinical Outcomes by Subgroups.
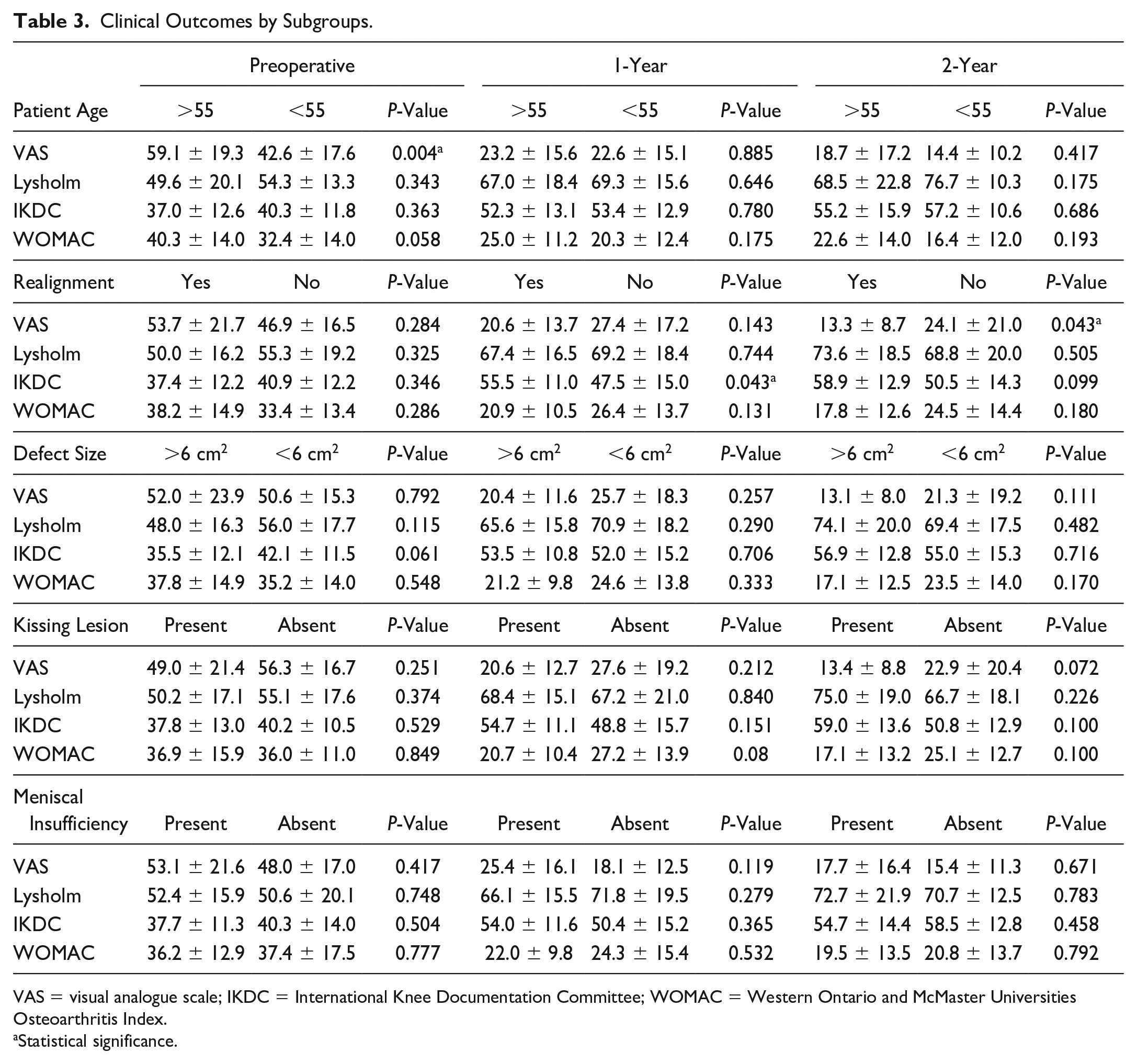
VAS = visual analogue scale; IKDC = International Knee Documentation Committee; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
Statistical significance.
In the subgroup analysis for combined realignment surgery, preoperative and postoperative 1-year clinical scores were not statistically different, except the postoperative IKDC score (55.5 ± 11.0 vs. 47.5 ± 15.0, P = 0.043). Postoperative 2-year clinical scores were not statistically different between the groups, except the VAS score (13.3 ± 8.7 vs. 24.1 ± 21.0, P = 0.043) ( Table 3 ). Improved outcome scores (compared with preoperative scores) were statistically higher in the realignment group in terms of IKDC and WOMAC score at 1 year (P = 0.037 and P = 0.026), but only in the VAS score at 2 years (P = 0.011) ( Table 4 ).
Improved Clinical Outcome by Realignment Group.
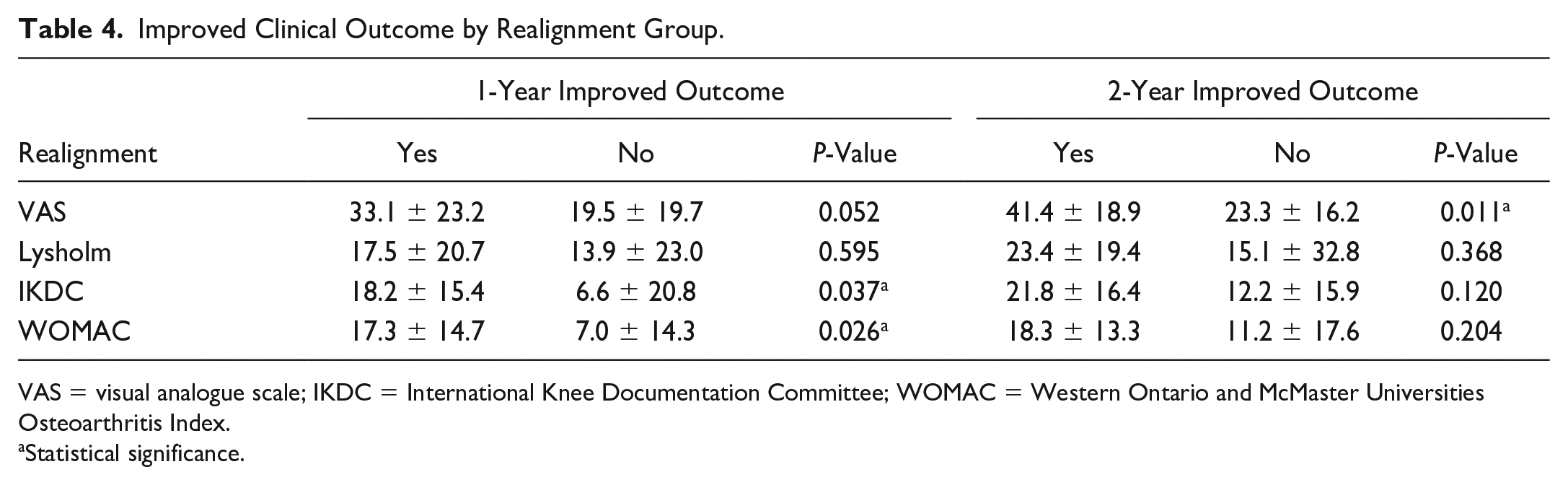
VAS = visual analogue scale; IKDC = International Knee Documentation Committee; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
Statistical significance.
In the subgroup analysis of cartilage defect size (size >600 and <600), the preoperative and postoperative clinical scores were not significantly different between the groups. No significant differences were observed in improved outcome scores. In the subgroup analyses, in which patients were grouped according to the presence of kissing lesions or meniscal function, no significant differences were observed in the preoperative, postoperative, and improved clinical scores between the groups.
Proportion of Patients Achieving MCID (MCID Achieving Rate)
In the realignment group, the VAS and WOMAC MCID achievement rates were higher than those in the realignment group at the 1-year follow-up (VAS, P = 0.003; WOMAC, P = 0.009; other scores, P > 0.05). At the 2-year follow-up, the VAS MCID achievement rate was significantly higher in the realignment group (VAS, P = 0.009; other scores, P > 0.05). No significant differences were observed in the MCID achievement rates between the groups divided by the other factors included in this study.
In the multivariate logistic regression analyses, patients who underwent combined realignment surgery were 26.5 times more likely to achieve VAS MCID (P = 0.007, odds ratio = 26.5). No other significant factors affected the MCID achievement rate in the logistic regression analysis.
Cartilage Regeneration on MRI
The mean total MOCART score was 54.6 ± 10.0. The mean total MOCART score was significantly lower in patients with a cartilage defect size more than 600 mm2 (49.7 ± 6.8 vs. 59.8 ± 10.4, P = 0.001). The patients with meniscal insufficiency showed significantly lower mean total MOCART scores (50.9 ± 8.3 vs. 60.9 ± 9.7, P = 0.001) ( Table 5 ).
Evaluation of Cartilage Regeneration.
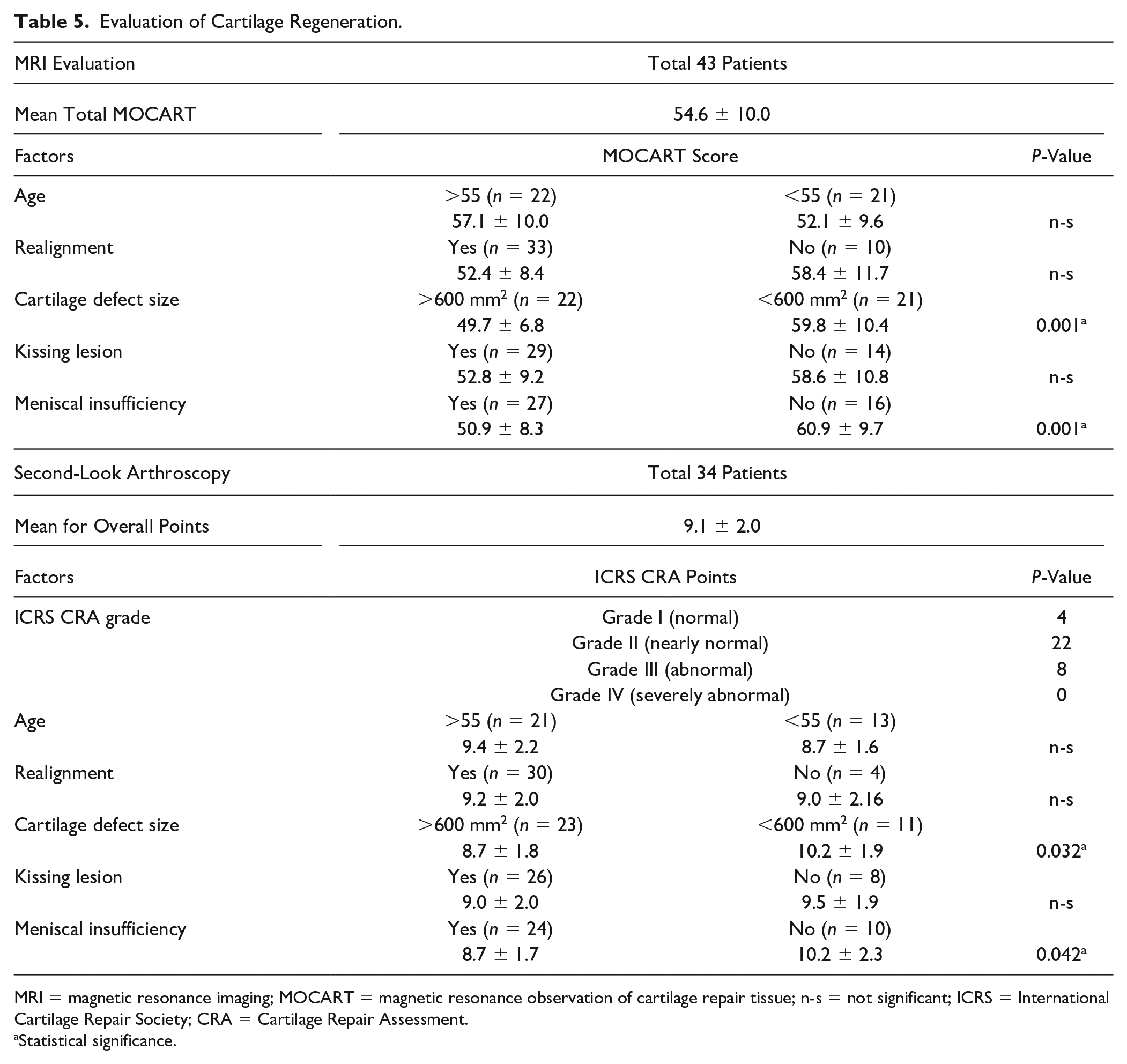
MRI = magnetic resonance imaging; MOCART = magnetic resonance observation of cartilage repair tissue; n-s = not significant; ICRS = International Cartilage Repair Society; CRA = Cartilage Repair Assessment.
Statistical significance.
In the Pearson correlation test, meniscal insufficiency, cartilage defect size, and cartilage defect size >600 mm2 were significantly correlated with the total MOCART score (meniscal insufficiency, R = −0.489, P = 0.001; cartilage defect size, R = −0.435, P = 0.004; cartilage defect size >600 mm2, R = −0.504, P = 0.001). The presence of kissing lesions and combined realignment surgery were not correlated with the MOCART score.
Multivariate logistic regression analyses were used to assess factors independently associated with poor MOCART scores (<60). Defect size (cm2) and postoperative alignment (°) were significantly associated with poor cartilage regeneration on MRI (P = 0.017, odds ratio [OR] = 1.91; P = 0.028, OR = 0.67). Meniscal insufficiency showed borderline significance (P = 0.067; OR = 5.85).
In the ROC curve analysis, the cut-off value of the cartilage defect size for favorable cartilage regeneration on MRI was 570 mm2 (area under the curve, 0.756; sensitivity, 70.4%; specificity, 81.2%) ( Fig. 5 ). The possibility of poor MRI outcome was 17.46 times higher when the cartilage defect size was >570 mm2 (P = 0.010, odds ratio = 17.46) ( Table 6 ).
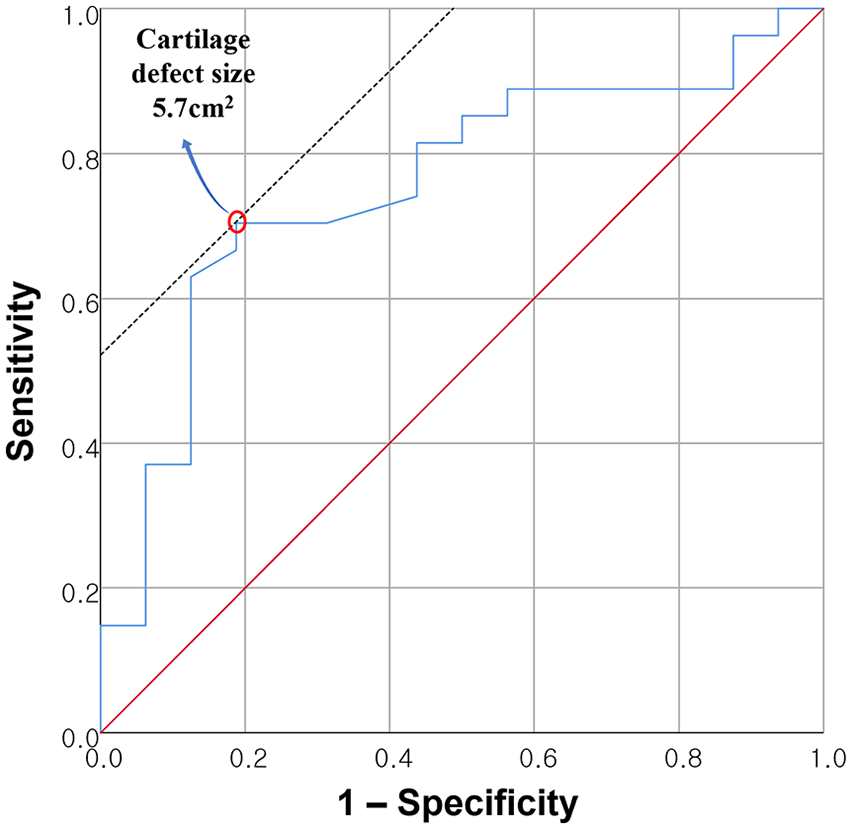
Receiver-operating characteristic curve analysis of cartilage defect size. 570 mm2 was the cut-off value for predicting poor prognosis after cartilage regeneration (area under the curve, 0.756; sensitivity, 70.4%; specificity, 81.2%).
Association Between Factors and Poor Cartilage Regeneration on MRI.
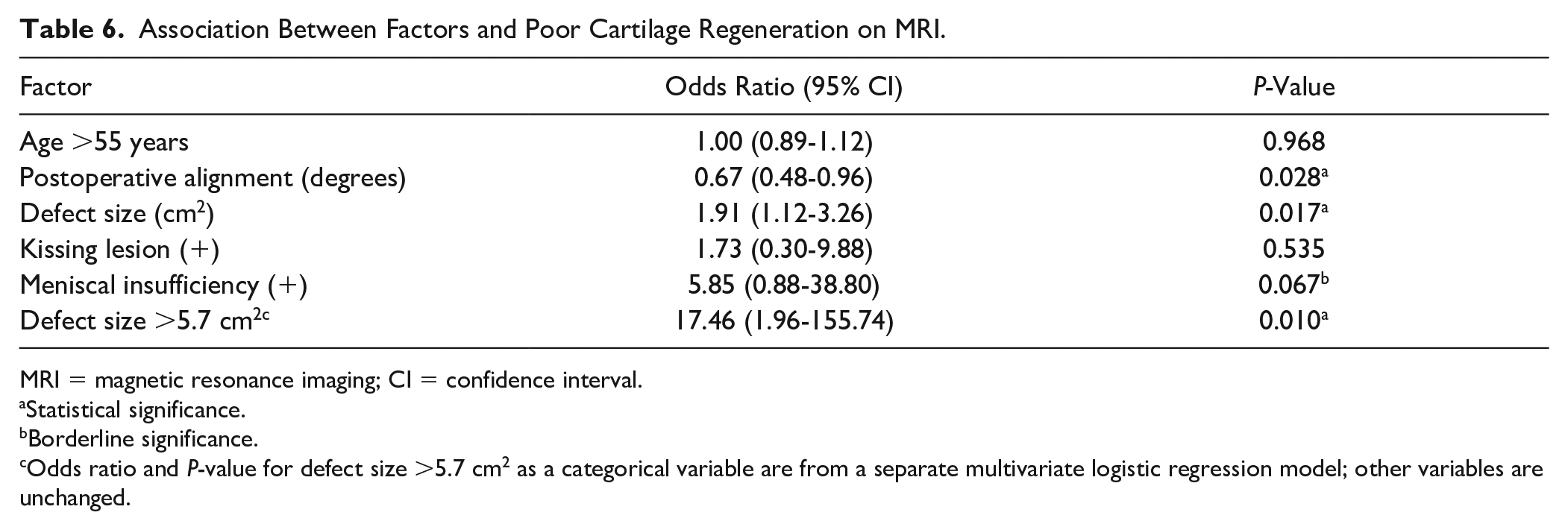
MRI = magnetic resonance imaging; CI = confidence interval.
Statistical significance.
Borderline significance.
Odds ratio and P-value for defect size >5.7 cm2 as a categorical variable are from a separate multivariate logistic regression model; other variables are unchanged.
Cartilage Regeneration on Second-Look Arthroscopy
A total of 76.5% of patients scored as Grade I (normal) or Grade II (nearly normal) of ICRS CRA grade on second-look arthroscopy. Patients with a larger cartilage defect size (>600 mm2) and meniscal insufficiency had lower ICRS CRA scores (P = 0.032 and P = 0.042, respectively) ( Table 5 ).
Discussion
The principal findings of this study are as follows: (1) A significant improvement in the short-term clinical outcomes was observed within a 2-year follow-up after the implantation of hUCB-MSCs in patients with large-sized cartilage defects with osteoarthritis. Subsequent evaluations revealed favorable cartilage regeneration on MRI and second-look arthroscopy. (2) Combined realignment surgery was correlated with favorable clinical outcomes, especially pain. No other factors had a significant impact on the clinical outcomes. (3) Prognostic factors for cartilage regeneration on MRI include the size of the cartilage defect, meniscal insufficiency, and postoperative alignment. A cartilage defect size >570 mm2 was the major poor prognostic factor for cartilage regeneration on MRI ( Table 6 ).
Implantation of hUCB-MSCs is a promising treatment option for large cartilage defects associated with osteoarthritis.15,17,18 Park et al. 16 reported a significant improvement in pain and functional outcomes after the implantation of allogeneic hUCB-MSCs, with no significant deterioration observed during the 7-year follow-up period. Song et al. 17 also reported favorable outcomes after a minimum 2-year follow-up period in their study, including 128 patients. The findings of our study are consistent with those of previous studies. These results indicated significant improvements in the clinical outcomes and favorable cartilage regeneration, further supporting the potential of hUCB-MSCs as a valuable therapeutic option for this patient population.
The present study had several strengths. We conducted a comprehensive analysis of various factors that could potentially influence the clinical outcomes, MCID achievement rates, and cartilage regeneration based on MRI and second-look arthroscopy. We utilized various statistical methods and conducted a regression analysis to identify the independent influence of each factor on the outcomes, adjusting for other variables. To the best of our knowledge, there is a scarcity of studies that specifically analyzed prognostic factors in patients who have undergone hUCB-MSC implantation. Song et al. 17 previously reported that patient age, lesion size, and obesity did not affect clinical outcomes. However, they reported that cartilage defects on the medial femoral condyle showed inferior clinical outcomes compared with cartilage defects in other compartments. In our study, there was no significant difference in the clinical outcomes according to the defect location. In another study conducted by Ryu et al., 36 no statistically significant differences were observed in the clinical and MRI outcomes between patients above and below 45 years of age. In our result of comprehensively analyzing factors, such as patient age, combined realignment surgery (limb alignment), cartilage defect size, kissing lesions, and meniscal insufficiency, most factors did not significantly influence clinical outcome scores. Only combined realignment surgery was significantly associated with pain, showing a significant difference between the groups in VAS score and improved VAS scores (P = 0.043 and P = 0.011). Realignment surgery, such as HTO, is a widely performed and effective surgical option for treating osteoarthritis.24,37 Improved outcomes after realignment are especially associated with pain. Therefore, a combination of additional realignment surgeries can result in further improvements in clinical outcomes. Our results demonstrate this. While the mean limb alignment of the patients in the realignment group showed a neutral alignment (0.7 degrees to the ipsilateral compartment of the cartilage defect), suboptimal pain relief was observed compared with patients whose alignment was realigned to the contralateral compartment of the cartilage defect (4.0 degrees). However, no significant differences were noted in other clinical outcomes between the 2 groups. The clinical implications could be that various factors were not directly related to poor clinical outcomes in the short term, and in terms of clinical outcomes, there is no reason to avoid this surgery due to the presence of these factors. Studies with long-term follow-ups and larger populations are needed to further determine the influence of these factors.
ACI, autologous MSC, and hUCB-MSC treatments, which are cell-based therapies, share prognostic factors. Patient age and cartilage defect size are frequently mentioned as significant factors. In some in vitro and animal studies, older age negatively affected autologous MSCs, such as bone marrow-MSCs (BM-MSC) and adipose tissue-MSCs (AT-MSC).13,14 Kim et al. 38 previously investigated the clinical outcomes after AT-MSC implantation in patients with osteoarthritis and statistically analyzed the factors influencing the clinical outcomes. Their study reported that patient age, particularly >60 years, is a significant prognostic factor. Furthermore, they proposed that a cartilage defect larger than 6.0 cm2 represents the upper limit for achieving favorable outcomes. In another study, they also reported that patient age significantly affected the clinical and MRI outcomes after AT-MSCs implantation combined with HTO. 39 Several prognostic factors have been mentioned in relation to ACI as well.40,41 Filardo et al. 40 conducted a study mentioning the prognostic factors associated with the chronicity of the cartilage lesion, including symptom duration and injury origin (traumatic, osteochondritis dissecans, or degenerative). Lesion size and patient age have also been identified as prognostic factors of clinical outcomes. In a systematic review of ACI, Pareek et al. 41 reported that older age and increased defect size (>4.5 cm2) significantly correlated with an increased risk of reoperation and failure during long-term follow-up.
Patient age did not affect the clinical and MRI outcomes in this study. In our study, an improved VAS score was rather significantly higher in the older age group at 1 year because preoperative VAS score was higher in the old age group (59.1 ± 19.3 vs. 42.6 ± 17.6, P = 0.004). The other clinical scores at 1 year and 2 years were not significantly different. Cartilage regeneration on MRI and second-look arthroscopy was not significantly different between groups. This non-significance can be attributed to the advanced age of patients in this study (mean age, 55.3 ± 7.5 years) and the fact that allogeneic MSCs cannot be influenced by the patient’s age in their chondrogenic potential, unlike autologous cells, such as AT-MSCs or BM-MSCs.
The cartilage defect size did not significantly affect the clinical outcome in this study, which is inconsistent with previously reported results after autologous MSC implantation and ACI.38,40,41 However, the cartilage defect size was a significant prognostic factor for cartilage regeneration. The mean MOCART score was significantly lower in patients with a cartilage defect size more than 600 mm2 (49.7 ± 6.8 vs. 59.8 ± 10.4, P = 0.001). Although the criterion for a favorable MRI outcome of cartilage regeneration in this study population was not clear, we set a MOCART score >60 as favorable for cartilage regeneration. In ROC curve analysis, a cartilage defect size of 5.7 cm2 was the upper limit for achieving favorable cartilage regeneration. The area under the ROC curve was 0.786, indicating a fair discrimination ability. Multiple logistic regression analyses showed that patients with a cartilage defect size smaller than 5.7 cm2 were 17.8 times more likely to achieve favorable cartilage regeneration (P = 0.011, OR = 17.8). The cut-off value of 5.7 cm2 for hUCB-MSC implantation, which was first reported in this study, was consistent with values from previous studies on AT-MSCs (5.4-6.0 cm2). 39
Meniscal insufficiency is commonly mentioned as a relative contraindication for all types of current cartilage repair procedures. 21 However, to the best of our knowledge, few studies have analyzed the outcomes according to the presence of meniscal insufficiency or function in cell-based therapy for cartilage repair. Among the included patients, 66% (31/47) had meniscal insufficiency. In our study, meniscal insufficiency did not have a significant influence on the clinical outcome or MCID achievement rate. However, in terms of the cartilage regeneration, the meniscal insufficiency group showed statistically poorer cartilage regeneration on follow-up MRI (MOCART score, 50.9 ± 8.3 vs. 60.9 ± 9.7, P = 0.001). Meniscal insufficiency also showed a linear correlation with the MOCART score (R = −0.489, P = 0.001). In the logistic regression analysis, meniscal insufficiency showed borderline significance, with an odds ratio of 5.85 the possibility of poor cartilage regeneration (P = 0.067). Based on the results of this study, meniscal insufficiency is likely to be a prognostic factor for cartilage regeneration.
In this study, we identified an important prognostic factor of cartilage regeneration. Malalignment is a commonly mentioned factor as a relative contraindication for all types of current cartilage repair procedures, such as meniscal insufficiency. 21 If malalignment is present, realignment surgeries, such as HTO or DFO, are considered to be combined for a better outcome.42,43 In the logistic regression analysis, combined realignment surgery was not a significant prognostic factor for poor cartilage regeneration. However, postoperative alignment itself as a continuous variable was significantly correlated with favorable cartilage regeneration on follow-up MRI (P = 0.03, OR = 1.4). If the postoperative alignment (mTFA) shifted by 1° opposite to the cartilage defect, it was 1.4 times more likely to achieve favorable MRI outcomes.
This study had some limitations. First, the sample size was relatively small. There is a possibility of limited power to detect other significant prognostic factors. However, we believe that the statistically significant data acquired from this study are sufficiently valuable to inform surgeons about the prognostic factors that influence clinical outcomes and cartilage regeneration after hUCB-MSC implantation. Second, this was a retrospective study with possible selection bias. Third, this study was an exploratory retrospective cohort study that divides included patients into multiple subgroups by various factors. Given that a simple comparison between groups cannot exclude the influence of confounding factors, only the results identified as statistically significant through regression analysis were described as prognostic factors in this study. Fourth, our study only covered short-term outcomes of 2 years. Further long-term studies are needed to analyze long-term prognostic factors. Finally, follow-up MRI and second-look arthroscopy, which are the main parameters for cartilage regeneration, were performed in a short-term period of approximately 1 year postoperatively. Although MRI findings are thought to correlate with clinical outcomes after cartilage repair surgery,44,45 it is doubtful whether well-regenerated cartilage can guarantee long-term results. In a 10-year study of HTO and combined microfracture for osteoarthritis, complete defect filling group in second-look arthroscopy has shown a statistically higher survival rate compared with the incomplete or no defect filling group. 46 Based on the data from this study, we anticipate that patients demonstrating favorable cartilage regeneration will exhibit superior long-term outcomes and survival rates.
Conclusion
The clinical outcomes significantly improved after the implantation of hUCB-MSCs in large cartilage defects with osteoarthritis. Combining realignment surgery showed a better prognosis for pain improvement. Cartilage defect size, meniscal function, and postoperative alignment are significant prognostic factors for cartilage regeneration. A cartilage defect size >5.7 cm2 was significantly related to poor cartilage regeneration.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and approved by the institutional review board of our institution (Gangnam Severance Institutional Review Board, 3-2023-0289). Due to the retrospective nature of the study and the minimal risk involved, patient consent was waived by the instititional review borad approval.