
Abstract
The cartilage repair potential of bone marrow–derived stem cells has been well described. Harnessing this potential for human articular cartilage repair remains challenging. Accessing bone marrow repair cells through marrow stimulation techniques such as microfracture is readily achieved with generally good but inconsistent results. Animal and human studies show feasibility for ex vivo processing of bone marrow to isolate, concentrate, and culture mesenchymal stem cells. Nevertheless, it has been difficult to show consistent and clinically meaningful improvement using bone marrow cell preparations above what has been achieved with microfracture. Consequently, microfracture continues to be the simplest and most commonly used method to enhance repair of focal articular cartilage defects. Emerging preclinical work in the equine model suggests a role for enhancing marrow-stimulation techniques through the use of natural scaffolds such as autologous platelet enriched fibrin as well as optimization of joint biology through localized gene therapy to support cartilage repair. In contrast to joint replacement where inert materials of known mechanical properties are used, host biology determines the relative success, failure, and durability of cartilage repair. As such, development of personalized strategies to improve the quality and durability of bone marrow cell–based articular cartilage repair represent exciting new areas of inquiry. Continued advances in stem cell biology, scaffold technologies, and methods to delineate and enhance host biology, both systemically and within the joint, hold promise for harnessing the full power of bone marrow cells to facilitate cartilage repair and regeneration.
Introduction
Articular cartilage injuries do not heal well and are an important cause of early osteoarthritis that can disable individuals during the prime work years. In 2004, the estimated direct cost of medical care for arthritis and joint pain was $281.5 billion. 1 Indirect costs of lost wages, lost independence, lost mobility, and poor physical and mental health due to early disability and pain significantly add to this amount. New clinical strategies to improve the evaluation, repair, and regeneration of damaged articular cartilage are needed to prevent or delay the onset of disabling pain and osteoarthritis.
Current treatment options in the United States include debridement, osteochondral grafting, autologous chondrocyte implantation, minced cartilage tissue grafting, and marrow stimulation procedures. Although good to excellent clinical results have been reported for each technique, clinical studies have not shown any technique to be superior to the others. 2 Marrow stimulation to access repair cells from the bone marrow has evolved from abrasion arthroplasty and subchondral drilling to microfracture, where disruption of the subchondral bone plate has been minimized. 3 Because microfracture is minimally invasive and the simplest of current treatment techniques, it remains the most widely used cartilage resurfacing procedure in the United States and has remained the de facto standard by which new treatments are compared. Microfracture is, however, inconsistent and generates a fibrous to fibrocartilaginous repair tissue of variable durability.1,4 Therefore, new strategies to further improve bone marrow cell–based articular cartilage repair beyond microfracture alone are needed.
For reasons of proximity to the cartilage wound bed, related mesenchymal lineage, and substantial scientific and clinical history, accessing the healing potential of bone marrow stem cells to repair full-thickness cartilage defects remains a valuable and attractive treatment option. The four strategies discussed in this perspective range from widely studied to emerging lines of inquiry. The widely studied techniques include use of cultured mesenchymal stem cells (MSCs) isolated from bone marrow and culture-enhanced bone marrow cell preparations with and without scaffolds of varying compositions. In part due to substantial scientific and regulatory barriers for human translation of cultured and manipulated bone marrow cells for cartilage repair, there has been several studies in the past decade to introduce minimally manipulated bone marrow concentrate as well as the use of cell free scaffolds to enhance microfracture. Finally, principles of personalized medicine will be introduced in relation to improving the variable results observed in large animal and human studies of bone marrow cell based cartilage repair.
Tissue Engineering: Culture Enhanced Bone Marrow Cells with Scaffold and Growth Factors
As described by Langer and Vacanti, tissue engineering is an “interdisciplinary field that applies the principles of engineering and life sciences toward the development of biological substitutes that restore, maintain, or improve tissue function or a whole organ.” 5 Early investigators of cartilage regeneration employed tissue engineered cell-polymer constructs. Examples include Vacanti et al., 6 where chondrocytes within PLGA were implanted in the dorsum of nude mice, and Chu et al., 7 where MSCs within PLA were implanted into rabbit osteochondral defects. Although the mechanical and structural properties of synthetic polymers can be precisely controlled in the laboratory, in vivo effects are less certain and require extensive testing for safety and efficacy. Thus, the use of naturally occurring and minimally manipulated materials offer improved potential for clinical translation. Significantly, Wakitani et al. showed superb osteochondral repair in rabbits using natural bovine collagen to encapsulate bone marrow–derived stem cells (BMSC). 8
The use of natural collagen scaffolds seeded with bone marrow–derived stem cells by Wakitani et al. facilitated clinical feasibility studies for human cartilage repair. Stem cells isolated and culture expanded from bone marrow have been widely studied for the ability to undergo chondrogenesis in vitro and to improve in vivo cartilage repair. Numerous basic and mostly small animal studies show that the consistency and quality of bone marrow–based cartilage repair can be improved by processing the bone marrow to select and implant pluripotential cell fractions also known as mesenchymal stem cells.9,10 Equine cultured MSCs obtained in a similar fashion from the bone marrow have also shown chondrogenic potential with collagen II and GAG synthesis. 11
The extensive basic science literature and the demonstrated clinical potential for articular cartilage repair using culture-expanded BMSCs in small and large animals provide support for translation to human clinical studies. A review of the world literature up to 2012, however, showed only seven published reports using cultured bone marrow–derived MSCs contributing data from a total of 61 patients. 12 Four of the seven reports are from Wakitani and colleagues using culture-expanded BMSCs suspended in a collagen scaffold, similar to their preclinical rabbit study with the exception that the treated defects in human subjects were additionally covered with autologous periosteum.13-16 Three of these were case reports and only one, Wakitani et al. was a prospective cohort study that showed superior arthroscopic and histological grades for the BMSC group but no differences in patient-reported outcomes between the BMSC and cell free groups. 15 At 10 years follow-up, clinical outcomes were again similar between BMSC and cell free subjects.16,17 The largest study was by Nejadnik et al., where patient-reported outcomes from 36 patients treated with autologous chondrocytes were compared with 36 patients treated with cultured BMSC. 18 This study showed greater improvement in Physical Role Functioning among subjects treated with BMSC. Whereas patients younger than 45 years of age scored better than older patients in the ACI group, age did not make a difference in outcomes in the BMSC group. 18 The remaining two reports also showed feasibility and the presence of cartilage repair tissue in human cartilage defects treated with cultured BMSC.19,20
Although overall positive, these studies primarily show clinical proof of concept by demonstrating feasibility and relative safety of transplanting cultured BMSC into human cartilage defects. For reasons including the heterogeneity in size, location, bone involvement, and joint environment of the lesions treated along with the general insensitivity of patient-reported outcomes to structural measures, systematic reviews have not shown cell transplantation to be superior to microfracture in humans.2,21,22 The difficulty in showing a definitive positive clinical effect of cultured autologous BMSC in humans supported moving forward with a randomized controlled study in horses. Use of an equine model permits standardization of lesion size, location, and bone involvement. 23 Arthroscopic, MRI, histological, and biomechanical evaluations can be also performed at defined time points in this model. To reduce bias, an appropriate scaffold or carrier appearing identical in cell-seeded and cell-free preparations permits blinding of the surgeons and all evaluators to the treatment used.
Consistent with tissue engineering concepts, a three-dimensional environment is important to induction of BMSC chondrogenesis. 8 Additionally, scaffolds and matrix materials also facilitate in vivo implantation of BMSC by encapsulating and supporting adherence of the cells to the cartilage defect. Fibrin glues have long been used clinically in humans for a variety of indications to include cartilage repair according to the classic ACI technique. 24 Fibrin is particularly effective at localization and containment of cells to chondral defects, and fibrin has been successfully used to generate three-dimensional MSC-fibrin constructs in situ within the equine femoropatellar chondral defect. 11 These studies show MSC can be delivered and localized to the cartilage wound during minimally invasive arthroscopic surgery using fibrin scaffold. The use of fibrin scaffolds optimized for MSC delivery, therefore, additionally has high translational potential in the clinical treatment of cartilage injuries in humans.
Recently, Haleem et al. used platelet-enriched fibrin gels to suspend cultured BMSC for implantation into full-thickness cartilage defects in humans. 19 In this work, the addition of platelets provided growth factors to support repair processes. Growth factors represent the third major component in the tissue engineering trifecta of cells, scaffold, and bioactive factors. Sustained release of chondrogenic growth factors such as TGF-Β1 have been shown by Pagnotto et al. to promote in vivo cartilage repair of human BMSC ( Fig. 1 ). 25 Whereas Ferretti et al. and numerous other investigators have engineered biocompatible polymers into scaffolds for sustained and controlled release of bioactive substances, 26 fibrin scaffolds for delivery of cells and bioactive factors have enhanced clinical relevance because of the well-established use of both autologous and allogenic fibrin glues in human medicine.
Human bone marrow stem cells improve in vivo cartilage repair. A three-dimensional environment and chondrogeneic growth factors are important to enhancing human bone marrow stem cell–mediated in vivo cartilage repair. When implanted into osteochondral defects within the diarthrodial environment, human bone marrow stem cells transduced with AAV-TGF-Β1 and implanted in three-dimensional culture persisted to participate in and improve cartilage repair (P = 0.0047). (
One of the impediments to endogenous cartilage repair relates to the limited mobility of chondrocytes and chondroprogenitor cells within the cartilage matrix. Fibrin has been shown to be effective at localized delivery of chondrogenic repair cells to full-thickness cartilage defects.11,27 However, if the cells remain encapsulated in fibrin gels, they are less available to participate in the actual repair. Dilute fibrin glue was shown by Lee et al. to promote release of bioactive substances. 28 When evaluating fibrin glue as a carrier for cells, Hale et al. showed that MSC migrate poorly out of undiluted 100% human fibrin glue formulations whereas dilution of the fibrinogen component significantly increased migration potential. 29 In equids, encapsulating cells in a dilute fibrin hydrogel resulted in a greater than 10-fold increase (P < 0.05) in MSC migration. Furthermore, a markedly higher number of cells migrating from dilute fibrin carriers showed morphology strongly correlated with high differentiation potential. 29 These studies support use of fibrin, where the fibrinogen content is reduced to promote cell migration and movement of bioactive factors, to for in vivo cartilage repair.
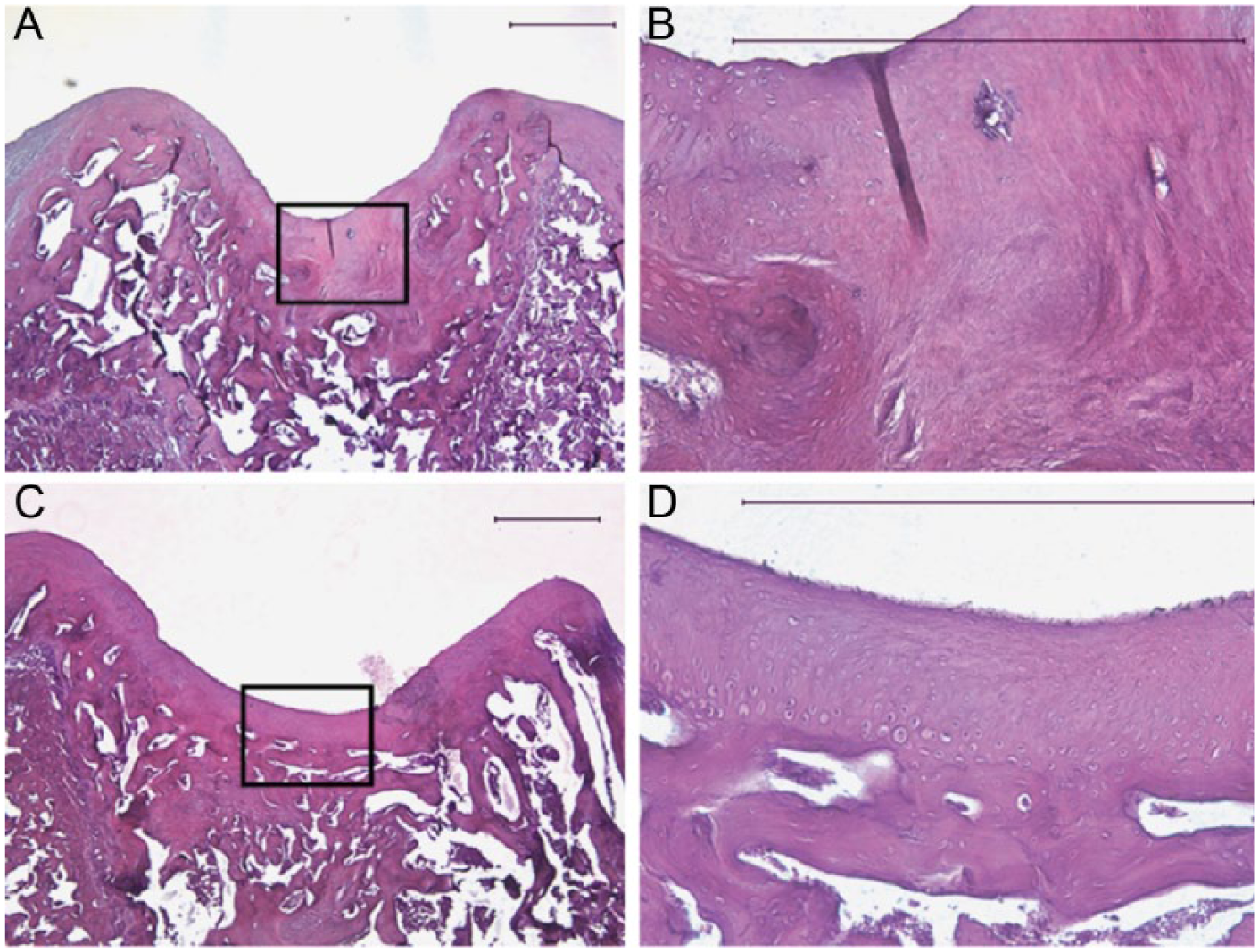
To test these concepts, the equine trochlear ridge model was selected because of its close parallel with the human condition in terms of critical defect size and cartilage thickness ( Fig. 2 ). In a 1-year equine study, these concepts were tested through arthroscopic treatment of full-thickness chondral defects using platelet-enriched fibrin scaffolds with and without the addition of cultured BMSC. The addition of the platelet concentrate both supplied growth factors and served to reduce the fibrinogen component resulting in a dilute fibrin scaffold.30,31 Bilateral surgery was performed to provide an internal control with assignment of the autologous cell–seeded preparation to right or left stifles performed in a randomized fashion. The surgeons and all evaluators of outcome metrics were blinded to the treatment groups. This work showed a potential for autologous platelet-enriched fibrin (APEF) to support cartilage repair (unpublished data). Whether this is due to facilitating migration of repair cells into the cartilage wound, release of growth factors, or a combination of factors requires further study.
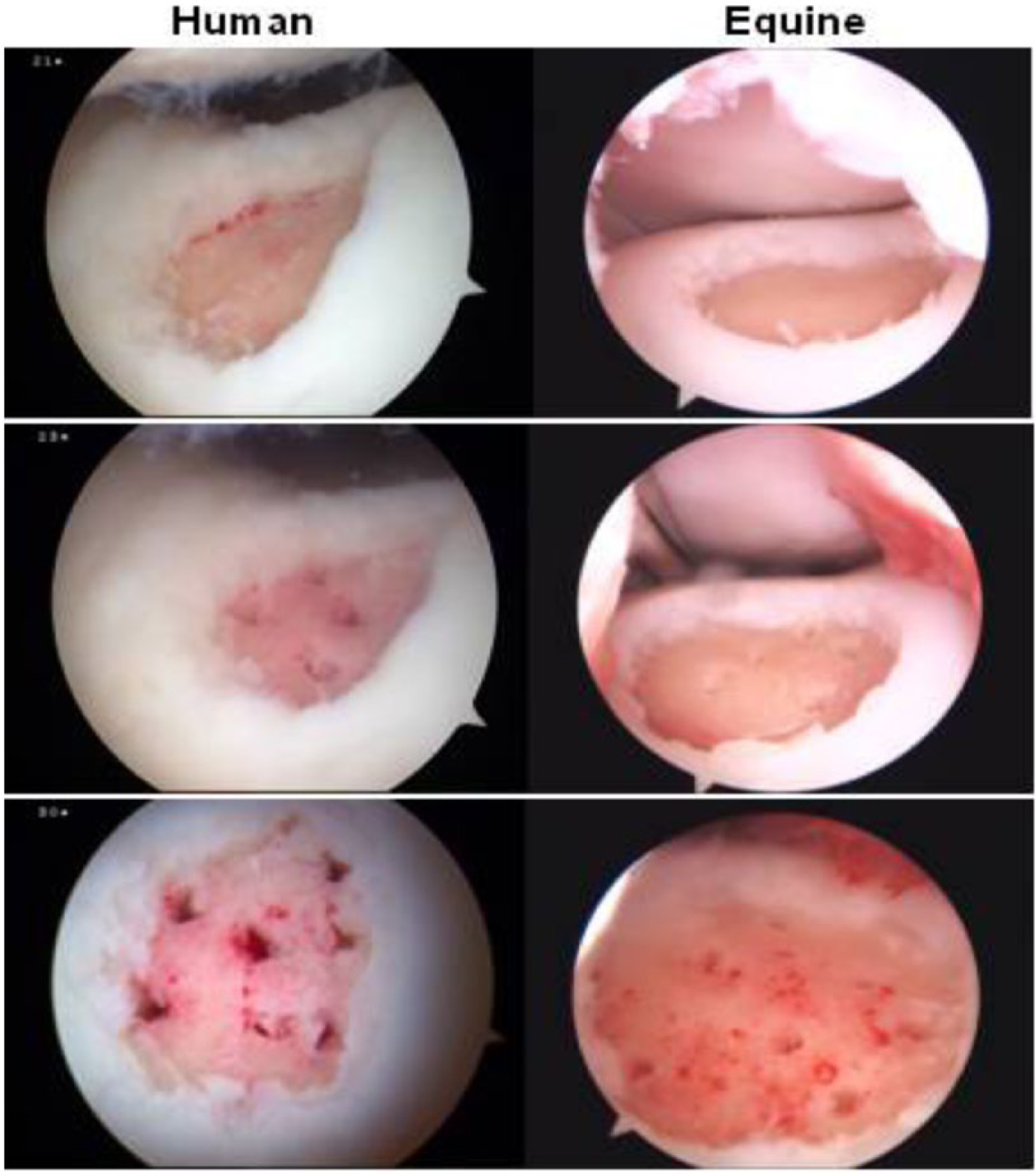
Equine trochlear groove model. The equine model offers cartilage defects of a size and depth more closely approximating humans than other commonly used large animal models. A lateral trochlear lesion in a human patient (
Minimally Manipulated Animal Studies (Bench to Bedside)
The clinical use of “minimally processed” autologous blood and tissues that can be prepared in an office setting or on the surgical back table has gained traction in recent years as a means for introduction of cells and bioactive substances to improve repair of musculoskeletal tissues. Concentrated bone marrow aspirate has been investigated as a source of MSC for regeneration of cartilage and other tissues of the musculoskeletal system. 11 Bone marrow aspirate is also a rich source of growth factors including factors important to cartilage repair such as IGF-1 and transforming growth factor-β.25,27,30 Increased concentrations of growth factor–rich platelets and mesenchymal cells were also shown in concentrated bone marrow (BMC) aspirate. Fortier et al showed an 8.7-fold increase in platelets, and that the nucleated cells from Gate 5 were negative for CD 45 and CD54, and positive for CD44, CD28, and CD172a. 32 In vitro comparison of cells cultured from equine bone marrow aspirate (simulating what can be obtained through marrow stimulation), BMC, and Ficoll gradient separation showed the BMC cells to be intermediate in chondrogeneic potential between the unprocessed aspirate and the Ficoll gradient isolation (unpublished). When cartilage repair following microfracture alone was compared with repairs following microfracture augmented with BMC using the equine lateral trochlear ridge chondral defect model, Fortier et al. showed that arthroscopic addition of BMC improved structural characteristics through 8 months after surgery. 32 In this equine study, histology and MRI showed improved fill and higher quality matrix in the BMC plus microfracture–treated defects compared with the contralateral defects treated with microfracture alone. No gross or histological sign of inflammation or synovial reaction to BMC was observed. These data suggested that addition of autologous BMC could potentially provide surgeons with a simple, cost-effective, and single-step arthroscopic procedure to improve clinical treatment of cartilage injuries beyond what can be expected with microfracture.
Translation to human studies was facilitated by the minimal processing needed to concentrate autologous bone marrow aspirate into a source of MSC and growth factors for cartilage repair. A one-step surgical procedure using autologous BMC covered by a collagen-based membrane sutured into the surrounding cartilage and sealed with fibrin glue was employed by Gobbi et al. in 15 human subjects followed for a minimum of 2 years. 33 This technique represents a hybrid between established procedures for ACI where a sutured collagen membrane sealed with fibrin glue is used to contain chondrocytes and substituting BMC for chondrocytes as a source of repair cells. In contrast to microfracture, the procedure required an arthrotomy and the subchondral bone plate was not violated. Mean lesion size of 9.2 cm2 was also much larger than that of lesions typically treated with microfracture. Patients in this study showed significant improvements in all of the clinical outcome scores used (Visual Analogue Scale, Knee Injury and Osteoarthritis Outcome Score, International Knee Documentation Committee, Short Form-36 Health Survey, Tegner, Marx, and Lysholm) at 2 years follow-up. Follow-up MRI showed complete cartilage defect filling in 80% of patients with no signs in any patients of repair tissue hypertrophy or subchondral bone edema, cysts, or sclerosis. Murawski and Kennedy have also shown feasibility in treating human osteochondral lesions in the talus with BMC. 34
Although the early animal and human data on concentration of bone marrow aspirate as an expedient means to introduce potential repair cells into full-thickness cartilage defects are promising, numerous questions remain concerning appropriate lesions to treat, surgical technique, or even whether the addition of these cells improves measurable outcomes beyond microfracture alone. The preclinical equine study employed an all-arthroscopic technique where microfracture was performed in both groups. There was not a comparator group in the human clinical studies. Carefully conducted randomized, controlled, large animal studies permitting creation of a uniform defect as well as ex vivo histological and biomechanical evaluation and comparison of structural characteristics will provide information concerning safety and efficacy not readily obtainable in human clinical study. Ultimately, adequately powered randomized controlled human clinical studies will be needed to determine whether clinically significant short- and long-term improvements justify the additional expenses and risks of adding bone marrow cells.
We All Heal Differently
One of the major challenges for critical evaluation and implementation of biologic strategies for cartilage repair resides in the high variability between subjects. Similar to the human clinical situation, horses used in research are genetically diverse and exhibit differing healing potential. The equine trochlear ridge model highlights that similar-size lesions treated by the same surgical team may fail to heal, heal with fibrous scar tissue, or heal with a hyaline scar cartilage ( Fig. 3 ). Unlike prosthetic joint replacement where the material properties of the bearing materials are known, the quality of a biological repair is highly dependent on host biology. At a minimum, the individual patient’s age, sex, genetics, lesion size and location, as well as joint biology will affect the quality and completeness of the repair.
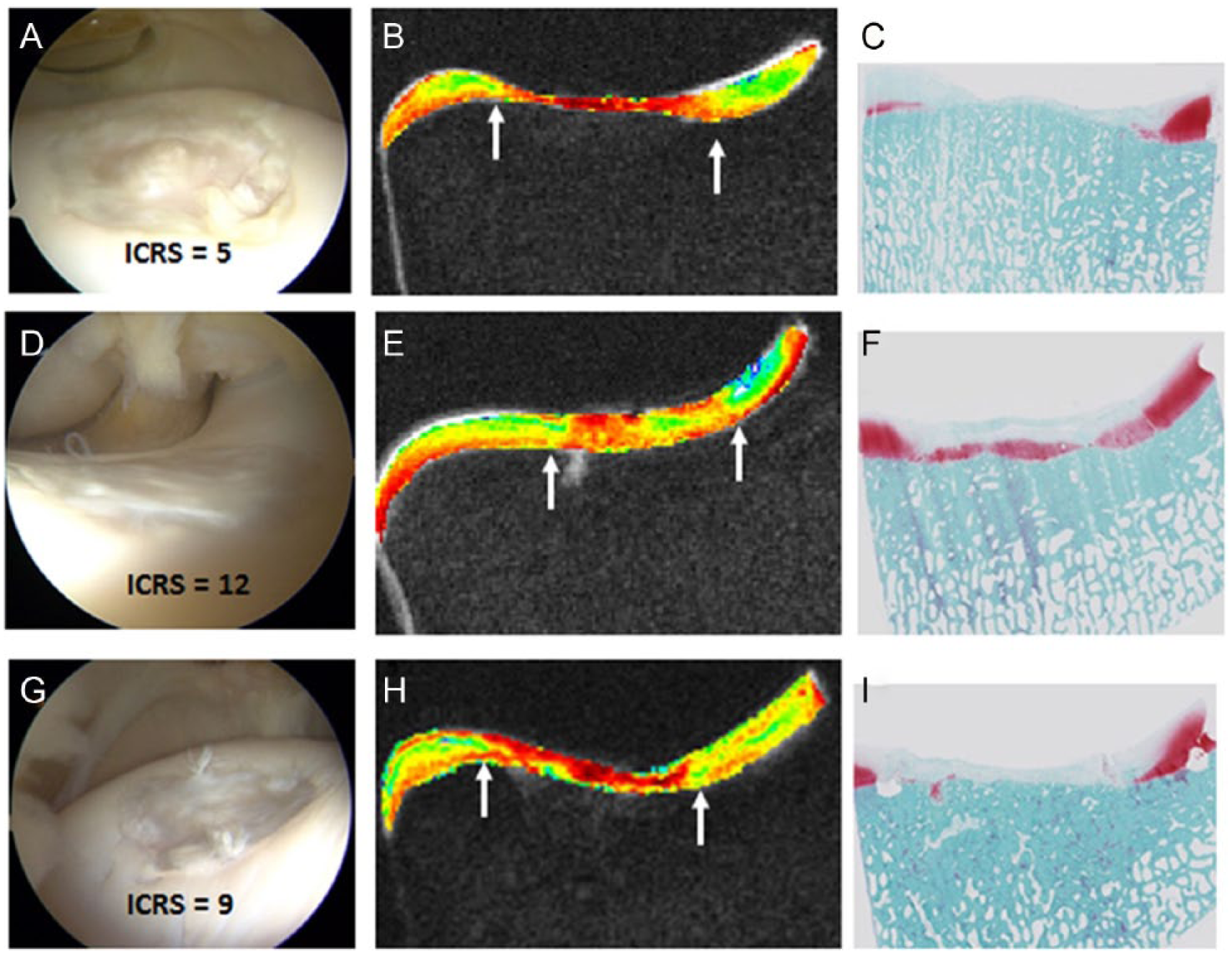
Diversity of repair tissue quality after microfracture. Similar to humans, equines are genetically and biologically diverse. One year after microfracture treatment of a uniformly created full-thickness chondral defect, repairs varied from Poor (top row,
Differences in joint, cartilage, and stem cell biology due to age and sex also affect articular cartilage repair. Although stem cell repair potential is generally thought to decline with age, Payne et al. showed this was observed primarily in males, with females showing an age-independent variability in BMSC chondrogenesis. 35 The in vitro data from this study suggest that bone marrow stem cells isolated from some elderly women undergo chondrogenesis to a degree comparable with that of many healthy young men ( Fig. 4 ). Yet microfracture is not generally considered an option for elderly women who present with qualifying cartilage lesions. The conclusion of one prominent clinical study was that patients aged 45 or younger showed improvement in pain and function after microfracture and that age was a predictor of functional improvement. 36 The study included only patients up to age 45 (range = 13-45) whereas patients under 35 had greater improvement in Lysholm score than those 35 to 45 (P = 0.48). That the majority of subjects in this study were male, where chondrogenic performance of bone marrow stem cells did show an age related decline, 35 may have additionally contributed to the results supporting this clinical recommendation. With increasing awareness of the potential for profound differences between male and female physiology, improved understanding of sexual dimorphism in stem cell, cartilage, and joint biology will be essential in clinical treatment of articular cartilage injury and degeneration.
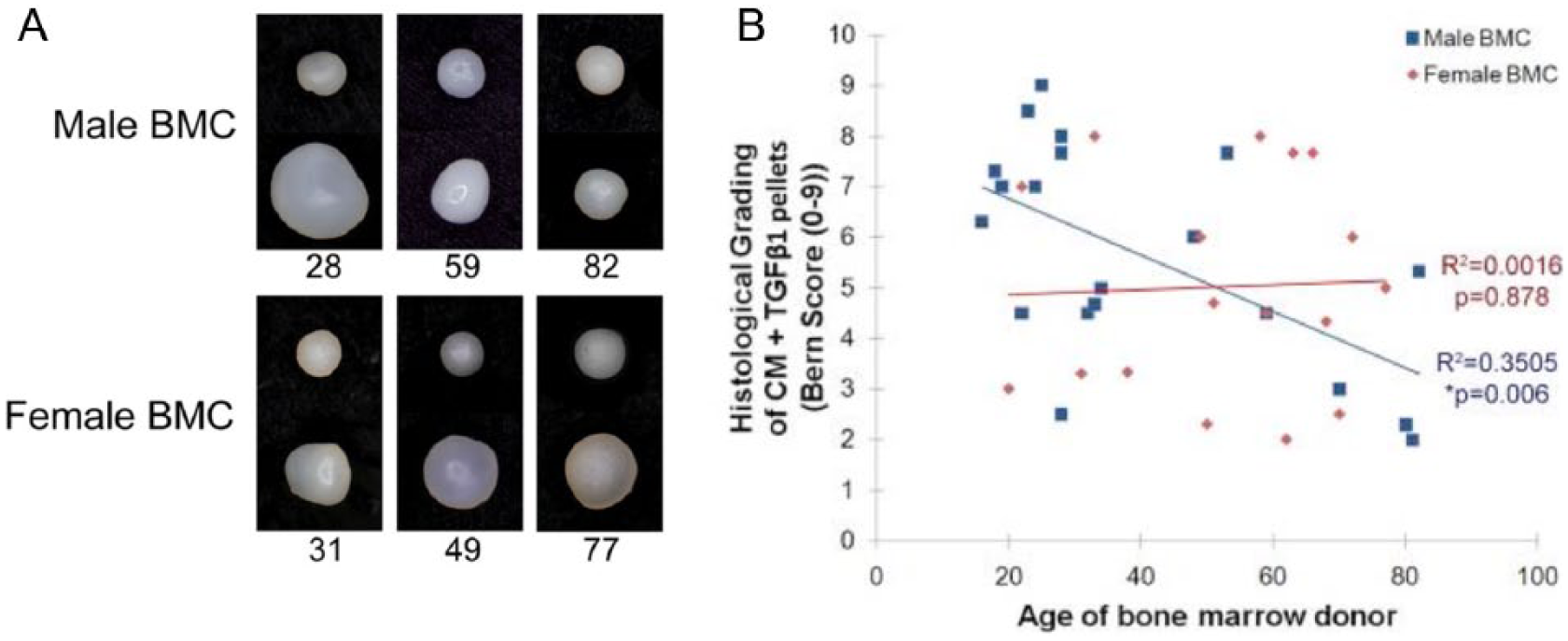
The chondrogenic potential of human bone marrow stem cells vary by age and sex. (
Systemic Biology
Systemic biology manifests itself as the overall state of health for a particular individual. Genetics plays a large role, and ongoing work in characterizing the human genome holds promise in assisting with patient selection and personalized treatment plans. Although genetic and many epigenetic factors are currently not modifiable, multiple personal factors such as obesity, comorbidities, and use of tobacco, alcohol, medications, or other biochemical inputs that alter physiological processes all affect the repair potential of the host wound bed and host repair cells. The type and quality of an individual’s diet, exercise, and level of stress represent frequently overlooked inputs that profoundly affect biology. In a study of the composition of platelet-enriched plasmas (PRP) prepared from the same individual, Boswell et al. described variability seen both due to the equipment used as well as due to the effects of diet, activity, and time of day.30,37-39 Thus, protocols addressing these factors may be needed in addition to equipment selection to optimize autologous PRP composition for desired biological effects.
Finally, joint biology both influences and is affected by biological agents. Synovial fluids from animal and human subjects with injured and diseased joints show elevated levels of inflammatory mediators and catabolic factors as well as reduced lubrication and fragmentation of hyaluronic acid compared with healthy controls.40,41 These changes reflect altered joint biology that can adversely affect stem cell survival and cartilage repair processes. Following arthroscopic treatment of full-thickness chondral defects in horses with APEF, Grissom et al. showed a transient reduction in synovial fluid lubrication. 41 In a study of ACL-injured subjects, Cameron et al. show variability between individuals with some exhibiting prolonged elevation of inflammatory mediators. 40 Work by Lewis et al. showing improved intrinsic cartilage repair in superhealer mice that are able to rapidly dampen the initial inflammatory response after joint injury. 42 These studies suggest that strategies to reduce chronic inflammation after injury or due to degenerative processes may be important in facilitating biological repair processes. 43
Due to the morbidity associated with chronic systemic use of oral nonsteroidal anti-inflammatory medications, localized gene therapy may offer a novel solution. Using a viral vector not known to cause any human diseases, Payne et al. have shown that localized gene therapy via a single intra-articular injection of adeno-associated virus may be effective in sustained in vivo administration of bioactive substances ( Fig. 5 ). 44 When injected into injured joints with osteochondral defects, Lee et al. showed localization of transgene expression to the articular cartilage wound. 45 Moving to the equine model, Goodrich et al. have shown feasibility to generate sustained levels of interleukin receptor antagonizing protein, a potent anti-inflammatory agent, through intra-articular injection of AAV-IRAP. 46 Additional work to delineate individual joint biology after injury and in early degeneration will be important in identifying appropriate therapeutic targets for personalized biologic strategies that may involve stem cells, natural and engineered scaffolds, as well as growth factors and anti-inflammatory agents delivered by controlled release scaffolds or localized gene therapy.
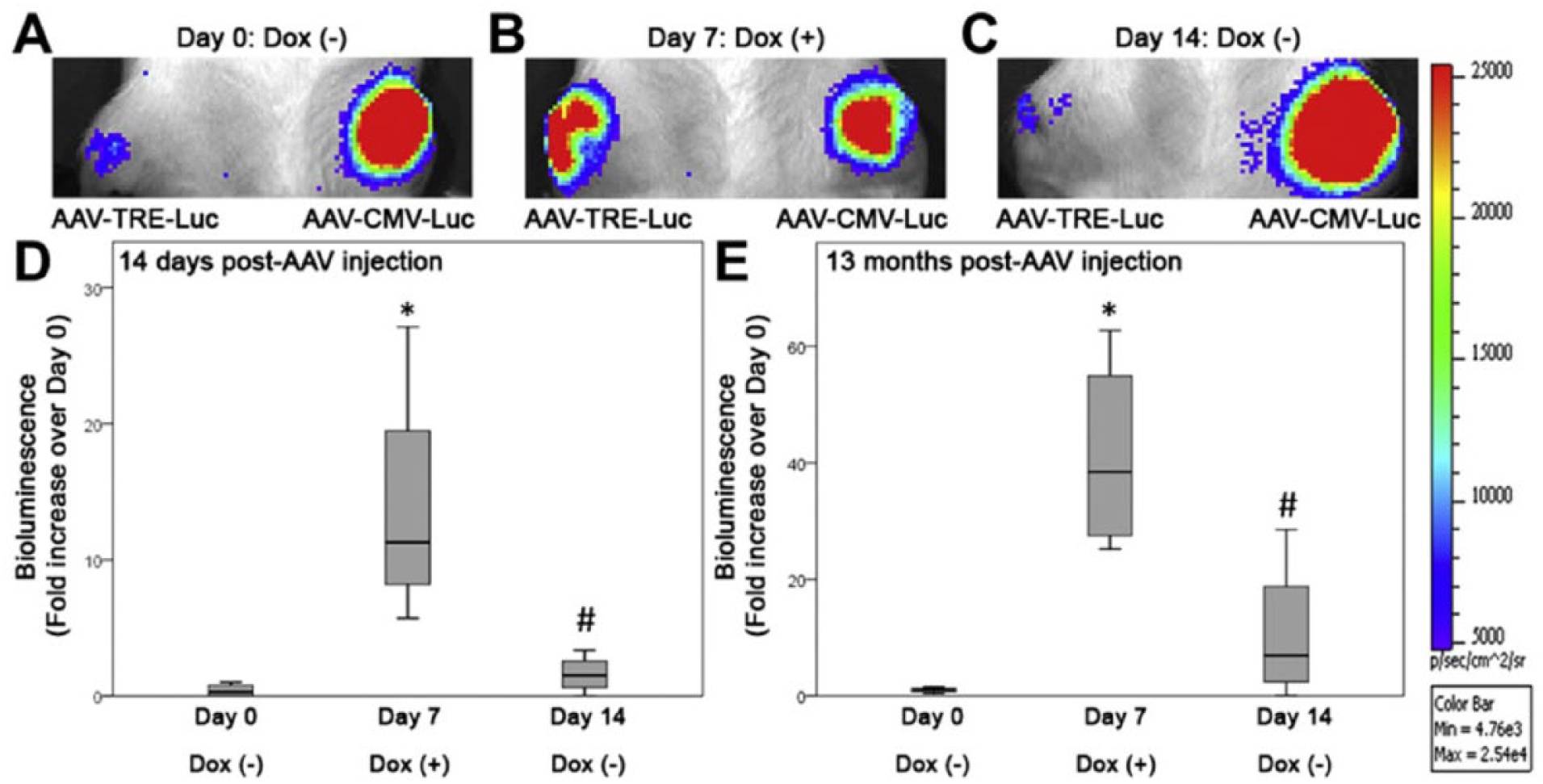
Localized gene therapy. Bioluminescent images of a representative rat shows both persistence of in vivo transgene expression following a single intra-articular injection of adenoassociated virus (AAV) to the left knee (A-C), as well as the ability to control in vivo transgene expression in the right knee which was injected with AAV controlled by a tetracycline response element (TRE). Addition of the TRE resulted in activation of transgene expression when doxycycline was added to the drinking water (B,D) and a return to baseline when doxycyline was withdrawn (C,D). These effects persisted through the 13 month study period (E). Reproduced from Payne et al. 44
Conclusions
The cartilage repair potential and multipotency of bone marrow–derived stem cells has been well described. Harnessing this potential for human articular cartilage repair has been both easy, through bone marrow stimulation techniques such as microfracture, and fraught with difficulty in showing consistent and clinically meaningful improvement over microfracture using additional processing to isolate, concentrate, and culture bone marrow–derived stem cells. For these reasons, microfracture continues to be the most commonly used method to enhance repair of full-thickness focal articular cartilage defects. Emerging work suggests a role for efforts to enhance marrow-stimulation techniques through the use of natural scaffolds such as autologous platelet-enriched fibrin and optimization of joint biology to support cartilage repair. In contrast to joint replacement where inert materials of known mechanical properties are used, the biology of the host determines relative success or failure of biological strategies to resurface damaged joints through effecting cartilage repair and regeneration. As such, personalized strategies will be needed to improve the quality and durability of bone marrow cell–based articular cartilage repair beyond what is currently obtainable through microfracture. Advances in stem cell biology, scaffold technologies, localized gene therapy, and methods to delineate and enhance host biology, both systemically and within the joint, hold promise for harnessing the full power of bone marrow cells to facilitate cartilage repair and regeneration.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH R01 AR059163 (CRC); NIH RC2 AR058929 (CRC); NIH R01 AR052784 (CRC).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional animal care and use approved procedures were followed for the equine work discussed in this manuscript.