
Abstract
Objective
Distraction treatment for severe osteoarthritis below the age of 65 successfully postpones arthroplasty. Most patients have been treated with a general external fixator or a device specifically intended for knee distraction. This study compares clinical efficacy of both devices in retrospect and their mechanical characteristics.
Design
Clinical efficacy 2 years posttreatment was compared using retrospective data from patients with severe knee osteoarthritis treated with knee distraction; 63 with the Dynamic Monotube (Stryker GmbH, Switzerland) and 65 with the KneeReviver (ArthroSave BV, the Netherlands). Changes in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain, stiffness, and function, general well-being (SF-36), cartilage thickness by radiographic joint space widening, and adverse events during treatment were assessed. Axial stiffness of clinically feasible configurations was assessed by bench testing for the Dynamic Monotube triax system and the KneeReviver.
Results
No differences were observed in clinical efficacy, nor in mechanical characteristics and adverse events between the two devices. Although with large variation, both showed a clinically relevant improvement. In mechanical testing, contact between articular surfaces was observed for both devices at physiological loading. Stiffness of applied configurations strongly varied and primarily depended on bone pin length.
Conclusions
Patients treated with a general intended-use device or a distraction-specific device both experienced clinical and structural efficacy although with significant variation between patients. The latter may be the result of varying mechanical characteristics resulting from differences in clinical configurations of the devices and actual loading. The exact role of full/partial mechanical unloading of the joint during distraction treatment remains unclear.
Introduction
Total knee arthroplasty (TKA) is the established and effective surgical intervention for end-stage knee osteoarthritis (OA) above the age of 65 years. For younger patients, joint preservation treatment strategies are desirable.1,2 Knee distraction (KD) is a surgical technique that increases the joint space width (JSW) a few millimeters for a period of 6 to 8 weeks using an externally placed distraction device fixed on bone-pins placed proximal and distal from the joint. This treatment for end-stage knee OA patients under the age of 65 years is clinically effective in reducing pain and improving function, and results in joint tissue repair activity.3,4 On average, effects of distraction reach an optimum between the first and second year of follow-up and sustain for a prolonged period in a significant number of the treated patients, even up to 10 years.5-10
Three open-prospective or randomized studies (n = 20, 20, and 23), have been performed with the same “proof-of-concept” device intended for a wide variety of orthopedic and trauma applications (Dynamic Monotube Triax, Stryker GmbH, Switzerland, further referred to as Dynamic Monotube).5,11-14 More recently, a larger study (n = 65) was conducted where a distraction device specifically intended for KD treatment was used (KneeReviver; ArthroSave BV, Culemborg, The Netherlands).15,16 In all studies, cartilage repair and pain relief were seen following treatment, but these were not clearly associated, and both parameters showed a high degree of variation between treated individuals.
Both distraction devices are applied to create absence of mechanical stresses on the articular surfaces during the distraction period (6-8 weeks), 17 considered essential for improving joint homeostasis. This absence of mechanical stresses is also considered to be accompanied by intra-articular fluid oscillation during loading and unloading of the joint, provided by the displacement enabled by the built-in springs in the distraction devices. 4
The clinical application of both distraction devices is similar, with surgical techniques both distracting the joint 5 mm using similar fixation sites and bone pins. Also, both the Dynamic Monotube and the KneeReviver device have built-in springs enabling 3-mm internal axial displacement. However, the exact fixation configuration during clinical application differs between the devices. The KneeReviver allows for a slightly less bulky configuration and for axial alignment of the built-in springs, while the Dynamic Monotube may require more protruding bone pins for fixation, specifically at the femoral sites, without the ability to adjust alignment of the built-in springs. 16 As such, axial displacement within the distraction devices is considered comparable between both devices. However, the exact configuration of both devices during clinical application may vary between patients.
Neither the clinical benefit obtained with the two devices nor the effects of variation in actual placement of the devices on mechanical performance have been compared. Therefore, this study compares for KD with the two most often used devices: (1) the clinical efficacy based on retrospective data on changes in pain, function, and stiffness, general well-being, changes in radiographic JSW parameters, and adverse events during distraction and (2) the axial stiffness with a focus on potential mechanical contact between the articular surfaces during loading of the distracted joint in different clinically relevant configurations of placement of the devices.
Methods
Retrospective Clinical Comparison
The first part of this study concerned a retrospective clinical comparison. To evaluate whether clinical efficacy after treatment with the KneeReviver distractor was similar to that of the Dynamic Monotube, retrospective clinical comparison was performed using data from multiple clinical trials, with ethical approval in place. Clinical and structural outcome were compared, for which respectively the total Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and minimum joint space width (min-JSW) were the primary outcome. The required sample size was calculated to ensure enough patients would be included to evaluate changes over time and to evaluate noninferiority of the KD systems (KneeReviver compared to the Dynamic Monotube).
For the comparison of changes over time, G-Power 3.1.9.7 was used with a two-tailed analysis, a power of 0.8, alpha of 0.05, and effect size of 0.73 (calculated from published data),13,18 the minimum number of patients required was 31 per group.
For the noninferiority, the Sealed Envelope online power calculator was used with an alpha of 0.05, power of 80%, and standard deviation (SD) based on the 2-year changes in WOMAC and min-JSW in the previous studies. Based on the WOMAC noninferiority test, two-third of the minimal clinically important difference (MCID) was chosen as noninferiority limit, that is, 10 points for the WOMAC 19 ; the required sample size was 40 patients per group, calculated with an SD of 17.8 for the 2-year WOMAC change over time that resulted from previous studies. 13 For the min-JSW, the smallest detectable change (0.88 mm) 20 was chosen as noninferiority limit, and with an SD of 1.5 from previous studies, 13 this resulted in a required sample size of at least 36 patients per group.
As the largest required sample size for the primary analyses was 40 patients per group, it was decided to use all available data from both devices to ensure a minimum number of 40 at both baseline and follow-up. For patients treated with the Dynamic Monotube, data up to 2 years of follow-up from an open-prospective study (n = 20) and two randomized controlled trials (vs TKA n = 20, vs high tibial osteotomy n = 23) were combined and used for comparison with 2-year follow-up data of patients treated with the KneeReviver in an open-prospective study (n = 65). See Suppl. Fig. S1 for inclusion numbers and loss to follow-up.
Patients
Relatively young patients with end-stage knee OA, as defined by persisting, conventional treatment-resistant pain with cartilage tissue damage seen in general practice and considered for (total or compartmental) knee arthroplasty or high tibial osteotomy (with limited axis deviation), were offered KD treatment by the orthopedic surgeon as joint-preserving treatment. The following criteria enabling the present comparison were applicable. Inclusion criteria: adults ≤65 years of age; body mass index (BMI) <35 kg/m2 with max 110 kg body weight; radiographic signs of joint damage (Kellgren-Lawrence grade 2-4); VAS (visual analogue scale) pain >40/100 (conservative treatment resistant); normal-good physical condition; sufficient knee joint stability; sufficient range of motion (last three criteria arbitrarily defined by orthopedic surgeons). Exclusion criteria: comorbidities that would compromise the efficacy of KD (arbitrarily defined by orthopedic surgeons); history of inflammatory or septic arthritis; knee malalignment of more than 10°; previous surgical interventions of the index knee <6 months ago; the absence of any radiographic JSW on both sides (medial and lateral); the presence of an endo-prostheses elsewhere. Patients were excluded in case of psychosocial condition not enabling the distraction treatment. For inclusion details for each of the studies, see original publications.11,12,14
All studies were granted ethical approval by the medical ethical review committee of the University Medical Center Utrecht (protocol numbers 04/086, 10/359, 11/072, and 17/293) and, except for the first study, registered in the Netherlands Trial Register (trial numbers NL2680, NL2761, and NL7986). All patients in all trials gave written informed consent.
Treatment
KD was performed according to a standardized surgical protocol similar for both devices. 21 The distraction device was fixated to the femur and tibia medially and laterally using half pins, placed in pairs at four different locations (tibia/femur and medial/lateral). A distraction distance of 2 mm was applied intraoperatively after fixation of the device. After surgery, patients were discharged when feasible, commonly within 2 to 3 days during which the distraction was gradually increased to 5 mm. During the distraction period un-protocolized weight-bearing was encouraged, supported by crutches if needed. After 6 to 8 weeks, the distraction device and pins were removed at day treatment and knee manipulation under anesthesia (MUA) was performed.
Variant Procedures
For the open-prospective study performed with the Dynamic Monotube (n = 20), 8-week distraction was applied instead of 6 weeks. 14 In the 8-week distraction period, patients returned to the hospital every 2 weeks for temporary removal of the device and had continuous passive motion of the joint for 3 to 4 hours after which the device and distraction was applied again. Although in a previous comparison between 6 and 8 weeks of distraction without repeated removal, no statistically significant differences were found, 17 a separate analysis was performed where these specific patients were left out of the comparison (see Suppl. Table S1).
Clinical Evaluation
Data were collected at screening, directly before placement of the KD device, 1 and 2 years after treatment. WOMAC data for pain, function, and stiffness (directly or deduced from the Knee injury and Osteoarthritis Outcome Score [KOOS] questionnaire), a numeric rating scale for pain (NRS-pain), directly or deduced from a VAS for pain, and data for quality of life by the Short-Form 36 (SF-36) were collected. For the WOMAC and NRS, the results at screening and directly before surgery were averaged to obtain the baseline values. For SF-36, only one pretreatment data set was available. For the WOMAC and SF-36, higher values indicate a better condition, while for the NRS-pain, lower values indicate a better condition.
Radiographic Evaluation
Standardized weight-bearing, semiflexed posterior-anterior radiographs were performed according to the Buckland-Wright protocol at screening and at 1-year and 2-year follow-up. 22 The most-affected compartment (MAC) and least-affected compartment (LAC) were determined visually from the radiographs (by M.J. and F.L.). Images were evaluated using knee images digital analysis (KIDA) software to analyze the JSW; an aluminum step wedge was used as a reference standard. 23 Calculated JSW parameters were the minimum JSW (min-JSW), the mean MAC JSW and mean LAC JSW, and the mean JSW. All image analyses were performed by a single, experienced observer, blinded to patient characteristics, and the intraobserver variation of this measurement method was shown to be good (for all JSW parameters, ICC = 0.82-0.97). 20
Data collection and evaluation with respect to the mentioned outcome measures were identical for all studies, except for the SF-36, which was not collected in the open-prospective study performed with the Dynamic Monotube.
Statistical Analysis
Independent t-tests, or chi-square tests in case of categorical parameters, were used to compare baseline characteristics between groups. Primary outcomes were the total WOMAC and min-JSW; secondary outcomes were the SF-36 and radiographic MAC JSW; tertiary outcomes were NRS-pain, the WOMAC subscales for pain, stiffness, and function, the radiographic LAC JSW, the mean JSW, and adverse events. Paired t-tests were used to calculate changes at 1 and 2 years compared to pretreatment for all parameters. Differences between groups over 1- and 2-year changes were calculated with linear regression, correcting for statistically significant different baseline characteristics. Noninferiority was calculated for the primary outcomes using linear regression, using the unstandardized B coefficient as mean difference and 90% confidence interval (90% CI). The calculation was performed corrected for baseline values and the between both groups statistically significantly different characteristics. The noninferiority limit was 10 points for the WOMAC and 0.88 mm for the min-JSW, as explained above. A p value <.05 was considered statistically significant. IBM SPSS 25 was used for all analyses.
Adverse events were documented during and after treatment over the 2 years of follow-up and are presented in different categories. Adverse events were defined as any undesirable experience occurring to a subject during the study, potentially related to the treatment. All events reported spontaneously by the subject or observed by the investigator or staff were recorded.
Data on axial displacement upon loading (see below) of three repetitive load cycles was provided with mean and standard error (SEM) for comparison between the devices.
Mechanical Bench Testing
The second part of this study concerned a mechanical bench test comparison. The two distraction devices were used in a configuration with bone pin positions according to the instructions for use provided by suppliers and corresponding to clinical practice (Suppl. Fig. S2A-B).
Tibia and femur bone structures were substituted by two polyvinylchloride (PVC) pipes (40 mm diameter and 2 mm wall thickness, designated throughout the text as femur and tibia), solely for providing fixation of the bone pins and considered not to contribute to the measured deformation of the system. In the standard configuration femoral bone pins were placed in the frontal plane at 180° between the medial and lateral position and tibial pins at 45° toward the sagittal plane with 90° between lateral and medial pins. The bone pin length between the pin clamps of the distraction device and the bone substitute were for a standard configuration set at a distance of 60 mm for the femoral sites and 25 mm for the tibial sites, mimicking clinical application to an average-sized upper and lower leg, respectively.
A manually operated actuator equipped with a digital scale was used to gradually apply 100 kg axial load, with full loading and relaxation in an approximately 3 minutes loading cycle (Suppl. Fig. S2C). Femur and tibia were axially aligned and fixated in the actuator with unrestricted rotational degrees of freedom at the femoral site.
The distance between femur and tibia was measured in millimeters with an accuracy of ±0.25 mm and axial load at steps of 5.0 kg with an accuracy of ±2.5 kg, providing curves of applied loading in kilogram with axial displacement in millimeter. The initial distance between femur and tibia was set at approximately 10 mm to provide for >5 mm axial displacement imposed during distraction. Resulting axial loads were measured and recorded. Average results of three independent cycles with SEM are provided.
Variations in Conditions During Mechanical Bench Testing
Because of the variance in configurations during clinical application, different bone pin lengths were tested to mimic varying soft-tissue volumes between patients. For the femoral sites 50, 60, and 70 mm were used, combined with 15, 25, and 35 mm, respectively, for the tibia (small: 50/15 mm, standard: 60/25 mm, wide: 70/35 mm). In case of the Dynamic Monotube also the 80/45 mm configuration was tested due to the limit degrees of freedom to place this device. Medial and lateral alignment were kept symmetrical.
Also, the change in axial stiffness from the built-in springs was tested between the devices by de-activating the springs. For the Dynamic Monotube, the springs were deactivated according to instructions for use. For the KneeReviver, no such option is available, and the springs were manually removed and substituted by a rigid element preventing internal displacement.
Results
Clinical Efficacy
The baseline characteristics of the compared groups—patients treated with the Dynamic Monotube and patients treated with the KneeReviver—are shown in Table 1 . In general, baseline characteristics were not statistically significantly different, except for the Kellgren-Lawrence grade (KLG), which was lower in patients treated with the KneeReviver. When excluding Dynamic Monotube patients included in the firstly conducted open-prospective study (with a slightly different treatment protocol as mentioned in the Methods section), the WOMAC function and total score were significantly different between groups whereas KLG was not (Suppl. Table S1).
Baseline Characteristics.
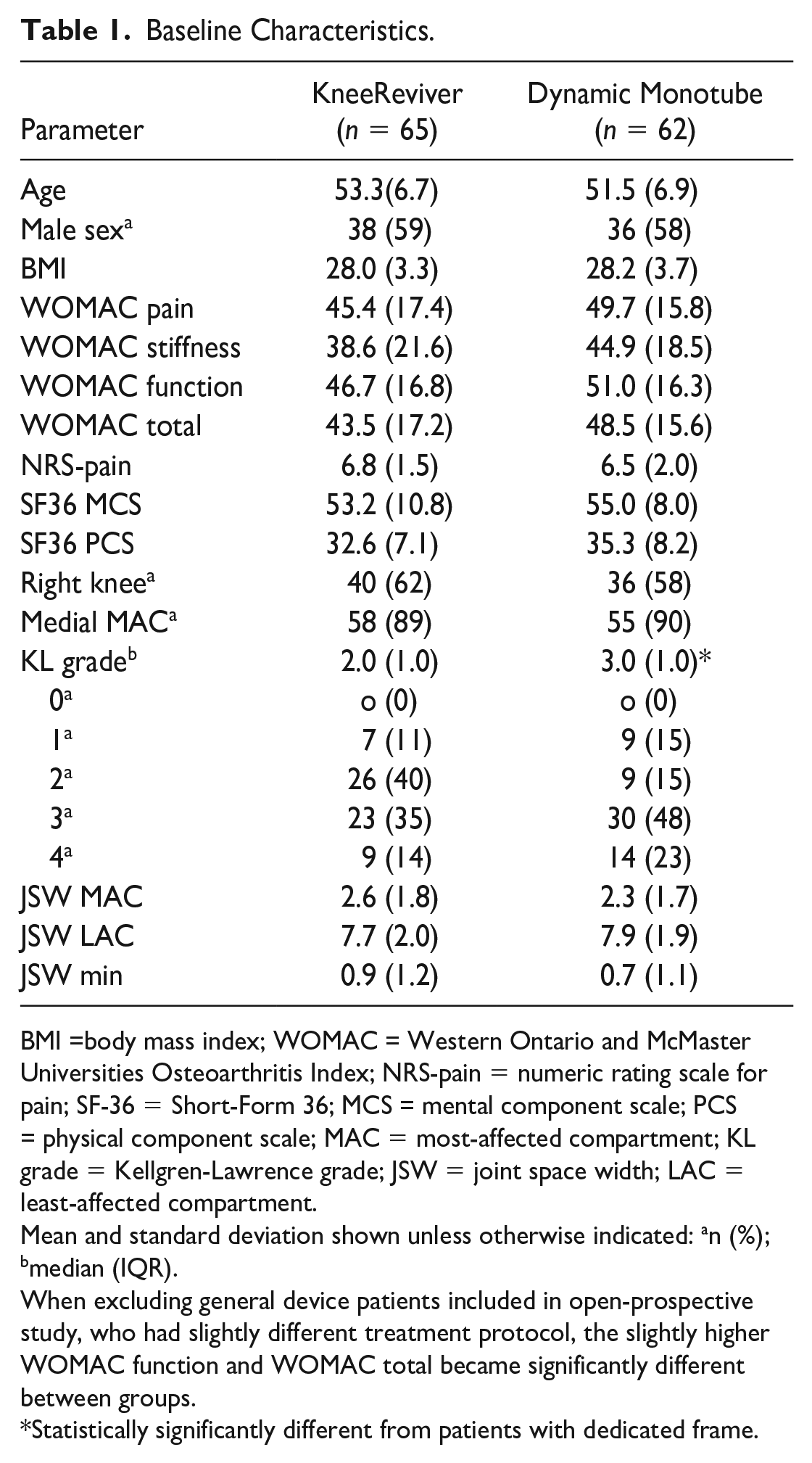
BMI =body mass index; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; NRS-pain = numeric rating scale for pain; SF-36 = Short-Form 36; MCS = mental component scale; PCS = physical component scale; MAC = most-affected compartment; KL grade = Kellgren-Lawrence grade; JSW = joint space width; LAC = least-affected compartment.
Mean and standard deviation shown unless otherwise indicated: an (%); bmedian (IQR).
When excluding general device patients included in open-prospective study, who had slightly different treatment protocol, the slightly higher WOMAC function and WOMAC total became significantly different between groups.
Statistically significantly different from patients with dedicated frame.
When comparing clinical and structural changes over time between groups, linear regression models are used corrected for significant baseline differences (KLG and, in case of SF-36, also WOMAC total, since SF-36 is not available in general device patients included in open-prospective study). Both devices showed statistically significant increases in the primary clinical (
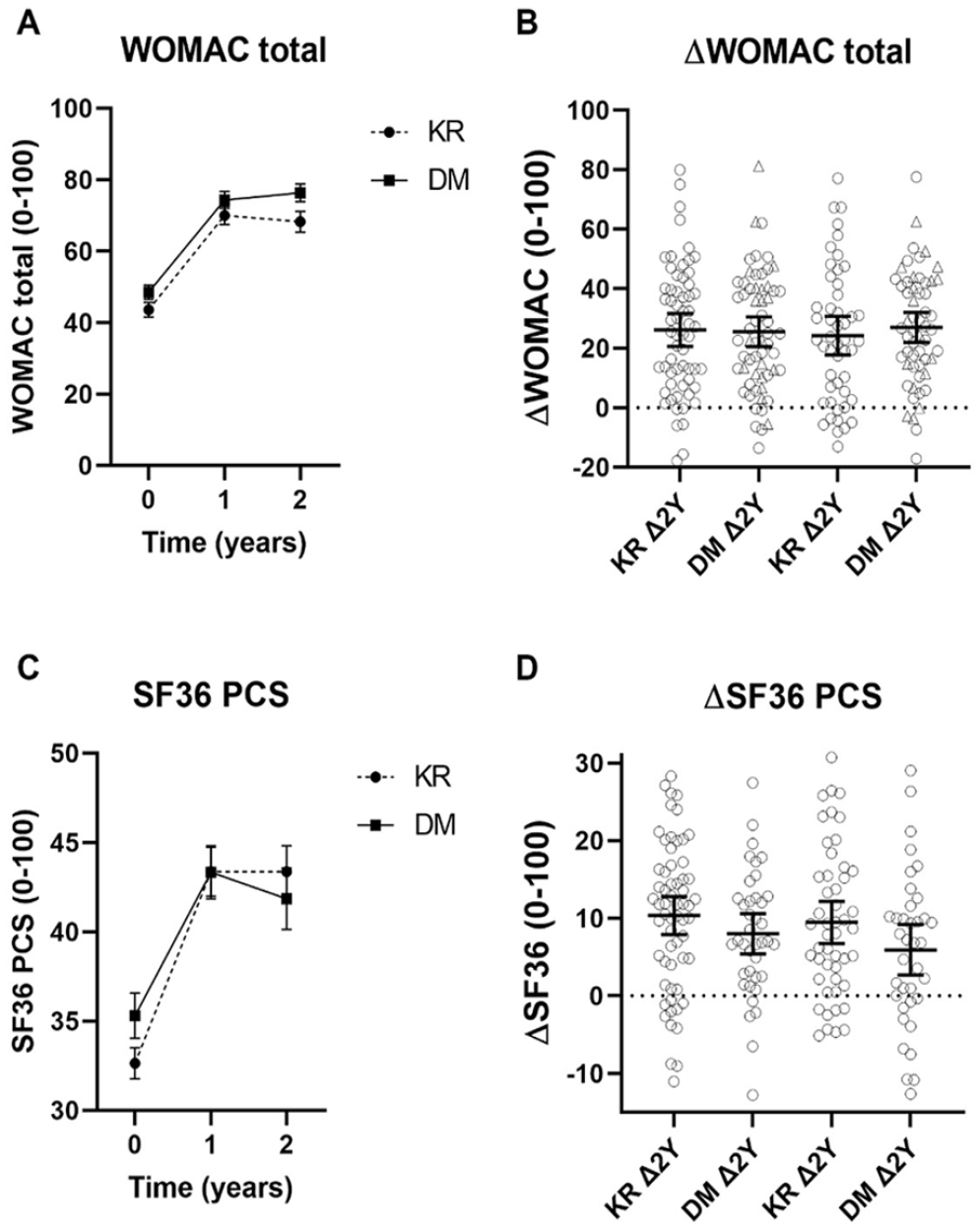
Total WOMAC score (A) and SF-36 PCS (C) at baseline (pre-treatment) and 1- and 2-years follow-up for both the Dynamic Monotube and the KneeReviver, as well as the delta change from baseline to 1 year and baseline to 2 years of follow-up for both parameters (B and D, respectively). For WOMAC total triangle markers indicate distraction patients in the open-prospective study. The mean and standard error (SEM) are shown in panel A and C and data of individual patients with the mean and 95% confidence interval in panel B and D. Changes at 1 and 2 years were statistically significant different from baseline values. Differences between both devices in absolute values at both follow-up time points and changes at 1 and 2 years were not statistically significant different. WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index ; SF = Short-Form ; PCS = physical component scale.
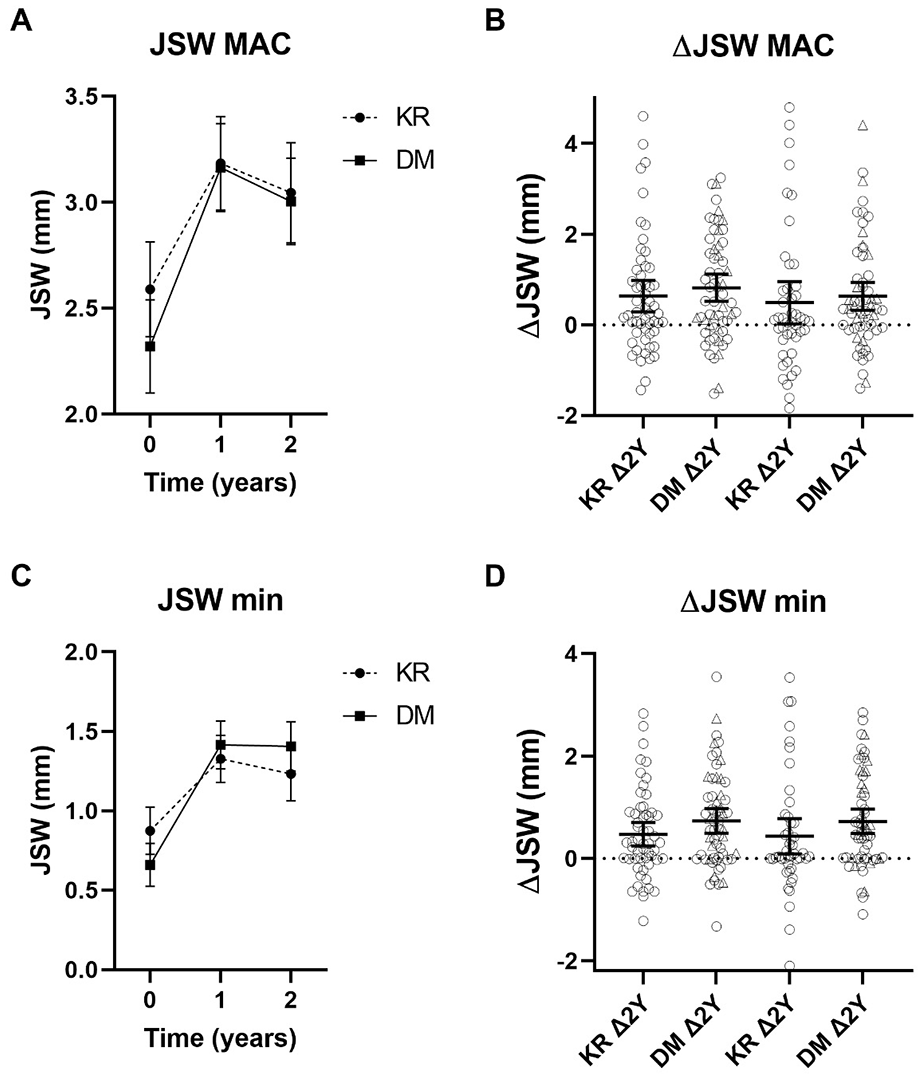
Min-JSW (A) and MAC mean JSW (C) at baseline (pretreatment) and 1- and 2-years follow-up for both the Dynamic Monotube and the KneeReviver, as well as the delta change from baseline to 1 year and baseline to 2 years of follow-up for both parameters (B and D, respectively). Triangle markers indicate distraction patients in the open-prospective study, respectively. The mean and standard error (SEM) are shown in panel A and C and data of individual patients with the mean and 95% confidence interval in panel B and D. Changes at 1 and 2 years were statistically significant different from baseline values. Differences between both devices in absolute values at both follow-up time points and changes at 1 and 2 years were not statistically significant different. JSW = joint space width; MAC = most-affected compartment; KR = KneeReviver; DM = Dynamic Monotube.
Uncorrected for baseline variables, both the total WOMAC and min-JSW changes over 1 and 2 years were noninferior for the KneeReviver compared to the Dynamic Monotube (data not shown). After correcting for baseline values and KLG, the change in min-JSW was still noninferior for the KneeReviver, but results for the 2-year total WOMAC change were in favor of the Dynamic Monotube but inconclusive, as the lower limit of the 90% CI crossed the 10-point noninferiority level (
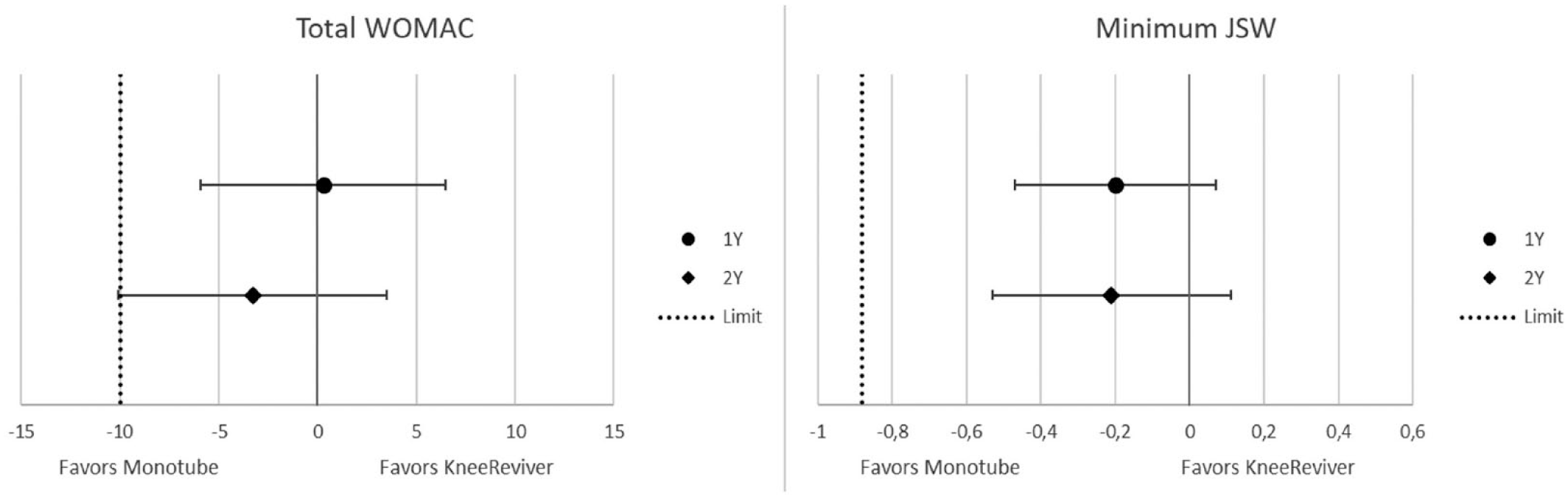
Noninferiority results at 1 (dot) and 2 (diamond) years follow-up for the KneeReviver compared to the Dynamic Monotube, for (A) the change in total WOMAC and (B) change in min-JSW, both corrected for KLG (which was statistically significant between groups). The dotted line indicates the noninferiority limit. JSW = joint space width; KLG = Kellgren-Lawrence grade.
For both devices, pin tract skin infections were the most occurring complications, with 66% of patients experiencing these for both groups, in most cases (>85% of cases) treated with oral antibiotics. Other complications occurred only sporadically, and no clear differences between devices could be observed ( Table 2 ).
Registered Complications.
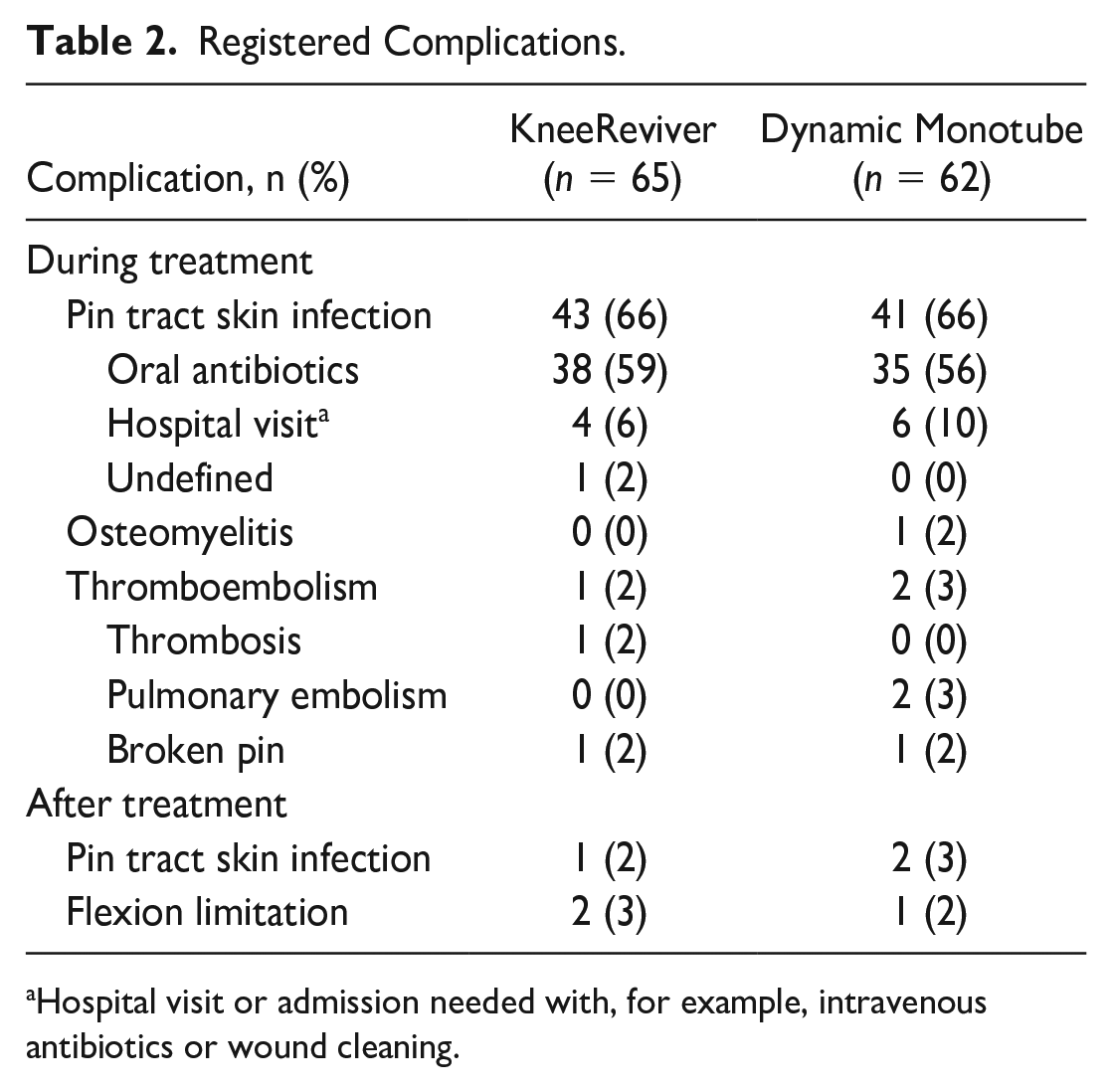
Hospital visit or admission needed with, for example, intravenous antibiotics or wound cleaning.
When excluding Dynamic Monotube patients included in the firstly conducted open-prospective study (triangles in
The Mechanical Properties
Both devices show similar axial stiffness for loads up to 100 kg (
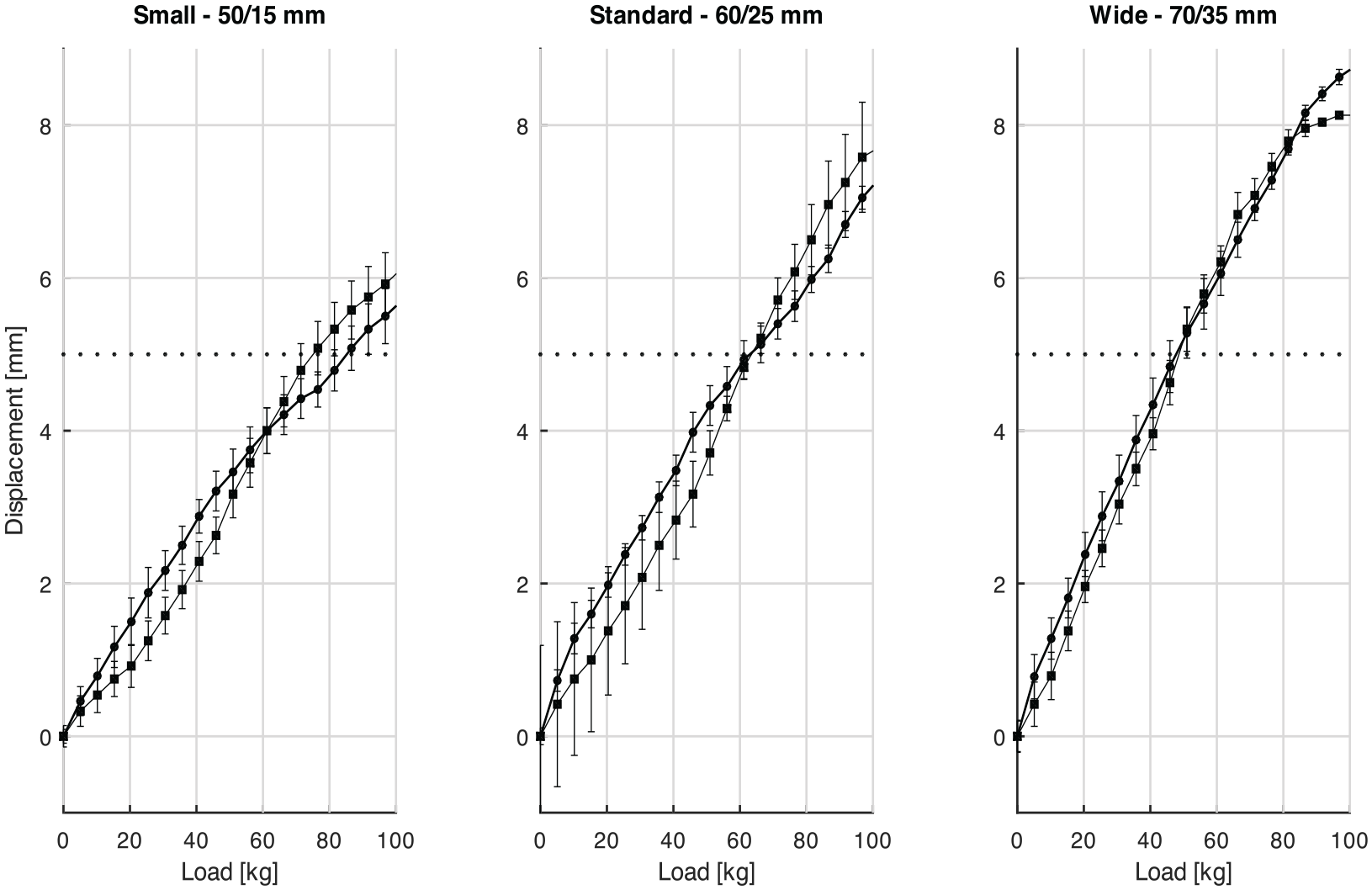
Displacement-load curves for the small, standard, and wide bone pin configuration, in panel A, B, and C, respectively (protruding femoral/tibial bone pin length in mm; small: 50/15 mm, standard: 60/25 mm, wide: 70/35 mm) for the Dynamic Monotube configurations straight line (square markers) and KneeReviver dashed line (round markers) in the three panels. Averaged data of three load cycles with SEM is provided. The clinically applied amount of 5 mm distraction is indicated by the dotted lines. SEM = mean and standard error.
The axial displacement was dependent on the length of the bone pins between bone substitute and pin clamp (
Axial displacement of 5 mm (dotted horizontal line,
Interesting, it was observed that for both devices compression of the built-in springs increased up to an axial load of ~75 kg in the standard configuration in parallel with deflexion of the pins. At full compression of the springs, around 3 mm, further deflection of bone pins was observed, confirming the added value of the springs in reducing deflection of the bone pins (data not shown). Also, no plastic deformation of the bone pins was observed in the standard configuration at loads up to 100 kg. Clearly, in case of a 5 mm distraction distance (the clinically reported standard), the femur and tibia will be in contact during static loading at levels of around 60 kg.
A slight tilting of the femur relative to the tibia in the sagittal plane was observed for both devices during axial loading, resulting in minimal narrowing between the dorsal femur and tibia. Also, minimal dorsal shifting of the tibia occurred, primarily originating from rotation along the femoral bone pins was observed (data not shown).
Relevance of the Springs in the Distraction Systems and Pin Length
For both devices, deactivation of the built-in springs results in similar stiffening of the configuration (Figure 5). Loading of around 100 kg was required for 5-mm axial displacement in case springs were blocked.
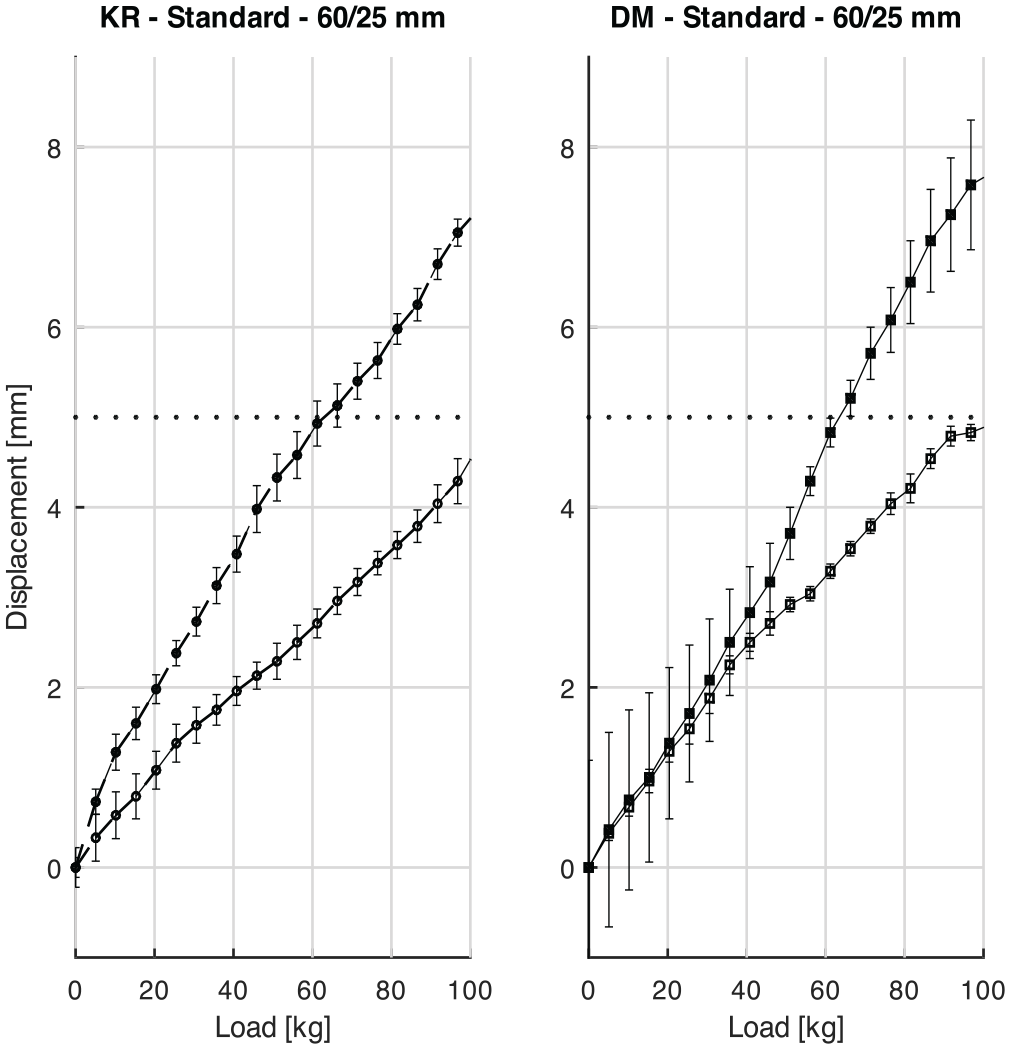
Standard bone pin configuration (60/25 mm bone pin lengths for femur and tibia pins, respectively) with 5-mm bone pins and springs active (filled markers) or blocked (open markers) for the KneeReviver (KR; left panel) and the Dynamic Monotube (DM; right panel). Averaged data of three load cycles with SEM is provided. The clinically applied amount of 5-mm distraction is indicated by the dotted lines. SEM = mean and standard error; KR = KneeReviver; DM = Dynamic Monotube.
Discussion
Patients treated with a device with a general intended-use (Stryker’s Dynamic Monotube) or with a distraction-specific intended-use (ArthroSave’s KneeReviver) both experienced similar clinical and structural efficacy without relevant differences in adverse events. However, variation in clinical and structural response between patients was significant with a variation similar for both devices. This was the reason for the second part of this study regarding mechanical characteristics. These two most often used devices for KD, also showed no differences in mechanical characteristics in comparable clinically relevant configurations. Importantly, variation in configurations resulted in significant variation in mechanical characteristics, again similar for both devices. Specifically, variation in bone pin length had a significant effect on the stiffness of the total configuration. Irrespective of the exact configuration, the clinical degree of distraction (5 mm) was completely lost at physiological loading allowing for contact between the articular surfaces in clinical practice. As such, the large variation in clinical and/or structural outcome for both devices may originate from the variations in the applied configuration (amongst others depending on leg circumference and with that bone pin length) in combination with actual loading (including patients’ weight and activity during treatment). Although the degree of mechanical unloading of the joint during distraction is expectedly causal in the clinical and/or structural benefit, prospective studies should proof this assumption.
Although both devices showed very similar statistically significant differences in clinical and structural benefit, the noninferiority analyses resulted in inconclusiveness for WOMAC corrected for baseline variables as one of the two primary outcomes in favor of the Dynamic Monotube. For all other noninferiority analyses, the difference was also in favor of the Dynamic Monotube, although statistically noninferior. In case of omitting the data from the prospective open study with the Dynamic Monotube, which had a slightly aberrant protocol, both devices showed still similar (not statistically significant different and noninferior) outcomes on all parameters.
The variations in WOMAC changes and in min-JSW changes were for both devices comparable but significant considering the average change in WOMAC. In fact, 9% and 16% of patients showed a decline in WOMAC score for the Dynamic Monotube and the KneeReviver at 2 years, respectively. Similarly for the change in min-JSW a decrease was observed for 22% and 31% of patients for the Dynamic Monotube and the KneeReviver at 2 years, respectively. This variation in clinical effects in combination with adverse events and specifically pin tract infections warrants better selection of patients with a known benefit, or decrease in variation in benefit. The latter might be found at least partly in improvement/standardization of the distraction configuration and actual loading.
Combining the clinical data with the mechanical data, it was concluded that significant variation in degree of patient benefit is accompanied with variation in device configuration in clinical practice and the related stiffness. For example, the circumference of the upper leg will have a significant effect on the bone pin length of the upper leg and hence on the mechanical characteristics of the axial displacement during distraction. In general, it may be expected that those with the largest upper leg circumference will also have higher weights, which will further contribute to axial displacement during loading and (partial) contact between the articular surfaces during loading. In general, it may be considered that for both devices equally, the articular surfaces will contact during physiological loading (i.e. overcome 5 mm distraction). These patients’ characteristics of device configurations have never been documented in previous studies and cannot be deduced in retrospect reliably from available data sets. As such a direct causal relation between mechanical characteristics and consequently cartilage contact during loading with the clinical and structural benefit of the treatment remains hypothetical, but future studies clearly warrant proper registration of certain variables related to mechanical characteristics of the treatment. Implementation of the relatively burdensome treatment would benefit significantly from less variable and with that higher response rates.
Interestingly, both devices clearly do not provide full absence of mechanical contact between the articular surfaces in clinically feasible configurations and should be considered partially unloading with possibly similar unloading capacity as less invasive but permanent surgical options like the MISHA Knee System (Moximed, Fremont, USA). However, structural repair with system has not been demonstrated yet.
The built-in springs of the devices contribute similarly to the system stiffness. The variation in stiffness primarily depends on the fixation configuration, and bone pin material and dimensions (length and diameter). Future evaluation of dependency of the clinical outcome on the system stiffness requires standardization of mechanical characteristics during distraction, for example, with a personalized setup, supplemented with data on activity and/or loading during treatment.
In conclusion, patients treated with a general intended-use device, or a distraction, device specifically intended for distraction, both experienced clinical and structural meaningful efficacy although with significant variation between patients. The latter may be the result of the variation in mechanical characteristics dependent on actual placement of the devices in clinical practice. The exact role of mechanical (un)loading of the joint during distraction treatment therefore remains unclear.
Supplemental Material
sj-docx-1-car-10.1177_19476035231226418 – Supplemental material for Comparison of Clinical Efficacy and Mechanical Characteristics of Two Knee Distraction Devices With Relevance for Clinical Practice
Supplemental material, sj-docx-1-car-10.1177_19476035231226418 for Comparison of Clinical Efficacy and Mechanical Characteristics of Two Knee Distraction Devices With Relevance for Clinical Practice by T. Struik, M.P. Jansen, R.G.P. Lafeber, Distraction Study Group, F.P.J.G. Lafeber and S.C. Mastbergen in CARTILAGE
Footnotes
Acknowledgements and Funding
The authors thank M Melief (MM) for KIDA image analyses. The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was financially supported by ZonMw (grant nos. 95110008 and 95104003), the Dutch Arthritis Society (grant no. LLP-9), and the UMC Utrecht Utrecht University (Vrienden UMC Utrecht project no. 1814144).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM was financially supported by the Dutch Arthritis Society (LLP-9). The funders nor the suppliers of the distraction devices had any role in the study design, data collection, analysis, or interpretation of the data, or in the writing of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.