
Abstract
Objective
In contrast to osteochondral lesion (OCL) of the ankle, OCLs in other joints of the foot, such as subtalar joint, talonavicular joint, calcaneocuboid joint, and the midfoot, are rare conditions, but they can also lead to significant morbidity. The objective of this systematic review was to summarize the clinical evidence for the treatment of OCLs of the subtalar, talonavicular, calcaneocuboid, and the other midfoot joints.
Design
A systematic search of the MEDLINE, EMBASE, and Cochrane Library databases was performed in January 2021 based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines by 2 independent reviewers. Included studies were evaluated with regard to LOE (level of evidence) and QOE (quality of evidence). Variable reporting outcome data, clinical outcomes, and complications were evaluated.
Results
Seventeen studies with 21 patients were included, all of which were case reports (level 5) without any case series reporting greater than 3 patients. There were 5 patients with OCL in the subtalar joint, 15 patients in the talonavicular joint, and 1 patient in the calcaneocuboid joint. Thirteen case reports (4 subtalar joint, 8 talonavicular joint, and 1 calcaneocuboid joint) reported surgical treatment. Surgical procedures mainly included debridement, bone marrow stimulation, fixation, and bone grafting, through open or arthroscopy, all of which resulted in successful outcomes. Four case reports (1 subtalar joint, 3 talonavicular joint) reported successful conservative treatment. Other 13 case reports reported successful surgery after failed conservative treatment. No complications and reoperations were reported.
Conclusions
The current systematic review revealed that there is no available evidence to ascertain clinical outcomes of both conservative and surgical treatments for cartilage lesions in the talonavicular joint, subtalar joint, and the midfoot joints, owing to the extreme paucity of literature. Both nonoperative and operative treatments can be considered, but no treatment strategies have been established.
Introduction
Articular cartilage is a highly specialized connective tissue that serves to lubricate joint surfaces and distribute loads across the joint. Osteochondral lesions (OCLs) involve damage to the articular cartilage and the underlying subchondral bone. In the foot and ankle, these lesions are most commonly found in the talar dome. The general consensus in the treatment of talar dome OCLs is that bone marrow stimulation (BMS) is indicated for smaller lesions, resulting in good clinical outcomes. 1 Other surgical options for symptomatic talar OCLs are internal fixation (particularly for acute osteochondral fractures), retrograde drilling, osteochondral autograft transfer, chondrocyte implantation, and biological augmentations. 2
In contrast to talar dome OCL, OCLs in other joints of the foot, such as subtalar joint, talonavicular joint, and calcaneocuboid joint, are rare conditions, but they can also lead to significant morbidity. While traumatic cartilage injury and its sequelae in these joints are well recognized,3,4 there is a lack of published literature describing the treatment outcomes of the treatment for OCLs in these joints, most of which are case reports.5,6 We are not aware of any systematic review reporting clinical outcomes for OCLs, focusing on the subtalar, talonavicular, and other midfoot joints, in part due to the low number of studies reporting these pathologies. Therefore, it is important to investigate and summarize the clinical evidence on the treatment strategies for OCLs in these joints.
The purpose of this systematic review was to investigate and summarize the clinical evidence for the treatment of OCLs of the subtalar, talonavicular, and other midfoot joints, analyzing the LOE and quality of evidence (QOE) of the studies, and to evaluate the clinical and radiological outcomes of both conservative and surgical treatments for the OCLs of these joints.
Methods
Search Strategy
A systematic review of the PubMed, EMBASE, and Cochrane Library databases was performed by 2 authors (Y.S. and S.R.) according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines on January 13, 2021. 7 The search terms employed were as follows: (Talonavicular OR Subtalar OR Talocalcaneal OR Midfoot OR Calcaneus OR Lisfranc OR Chopart OR Naviculocuneiform OR Tarsometatarsal OR Cuboid OR Calcaneal) AND (Cartilage injury OR Cartilage lesion OR Osteochondral lesion OR Osteochondral dissecans). The titles, abstracts, and full-texts were screened in the stepwise fashion, with the full-texts subsequently matched to the specific eligibility criteria for inclusion. Studies were included based on the agreement of both authors, with disagreements resolved by the senior author (M.T.).
Eligibility Criteria
The inclusion criteria were as follows: (1) clinical studies reporting outcomes for talonavicular, subtalar, talonavicular, and other midfoot joints; (2) follow-up ≥12 months; (3) full-text studies available; (4) published in a peer-review journal; and (5) written in English. Due to the expected low number of the studies, we primarily included both case reports and case series. The exclusion criteria were as follows: (1) animal studies, (2) cadaver studies, (3) in vitro studies, and (4) reviews.
Data Extraction
Data were extracted from each of the included studies by 2 independent authors (Y.S. and S.R.). A standardized datasheet was used to collect the following variables: number of patients, gender (male/female), age, duration of symptom, follow-up, lesion location, lesion size, and treatment. Outcomes were also collected, including the clinical outcome scores, radiological findings, return to sports, complications, and revisions.
Assessment of Evidence
The level of evidence (LOE) was assessed using the criteria published by The Journal of Bone & Joint Surgery. 8 The methodological QOE was determined to assess using the Newcastle-Ottawa scale. 9
Statistical Analysis
A simplified pooling method was planned to be utilized to combine data from the included studies, and descriptive statistics were going to be calculated and presented for all continuous and categorical variables. Time units were converted to either months or years. A Microsoft Excel datasheet (Microsoft Excel, Microsoft, Redmond, WA) was utilized.
Results
The literature search, based on the search strategy, identified a total of 1,396 studies, with 17 studies that met the inclusion and exclusion criteria (
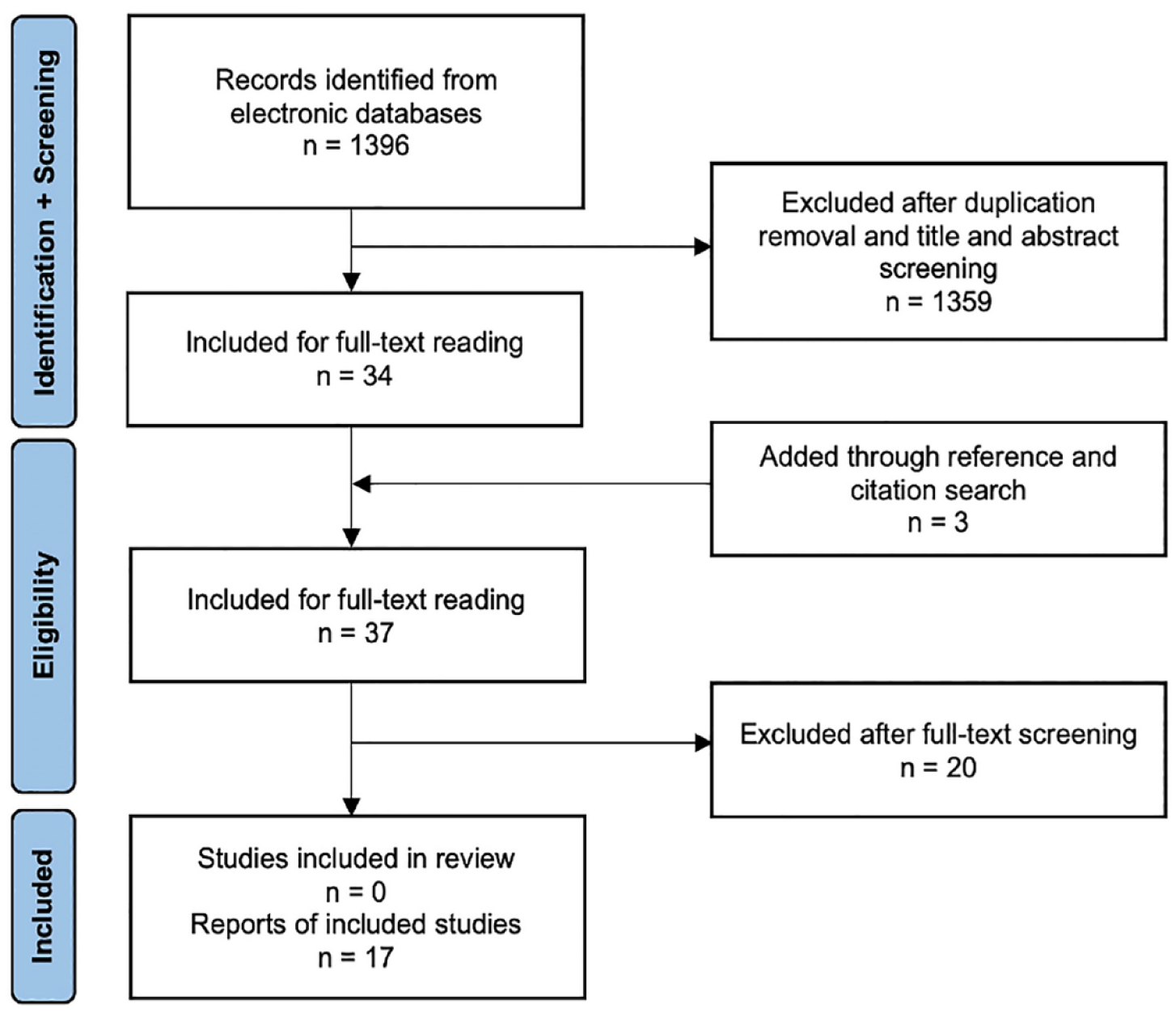
PRISMA flowchart outlining the systematic review. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Subtalar Joint
A total of 5 patients with OCLs of the subtalar joint were identified from 5 case reports.6,10-13 The mean age was 23.8 years (range, 10-37 years) and the mean follow-up was 2.0 years (range, 1-2 years). Three lesions were located in the lateral process of the talus, which were all described as osteochondritis dissecans (OCD). Two lesions were located in the posterior facet of the talus. All patients were primarily treated with conservative treatments. One patient aged 10 years, with OCD in the lateral process of the talus, had successful outcomes following cast immobilization for 6 weeks, with complete healing of the fragment on MRI, 12 but the other 4 patients required surgery. Surgical treatments included debridement only, debridement with bone grafting, or BMS. Cugat et al. 10 described arthroscopic technique for the lesion in the posterior facet and Kadakia and Sarkar 11 utilized arthroscopy for lesion evaluation, followed by mini-arthrotomy and drilling procedures. All patients experienced good clinical outcomes that were evaluated by varieties of outcome scoring scale. Only 1 case report treated with surgery (debridement and bone grafting for OCL in lateral process of the talus) reported the radiological outcome, which showed full bone consolidation and satisfactory articular alignment on computed tomography. 6 The details of these case reports are shown in Table 1. In addition, Ahn et al. 25 reported on a total of 6 cases with subtalar OCL that represented a subgroup of 115 subtalar arthroscopies. However, no exact outcomes on these cases were provided and therefore they could not be included into this analysis.
Summary of Cases Reported in the Subtalar Joint.
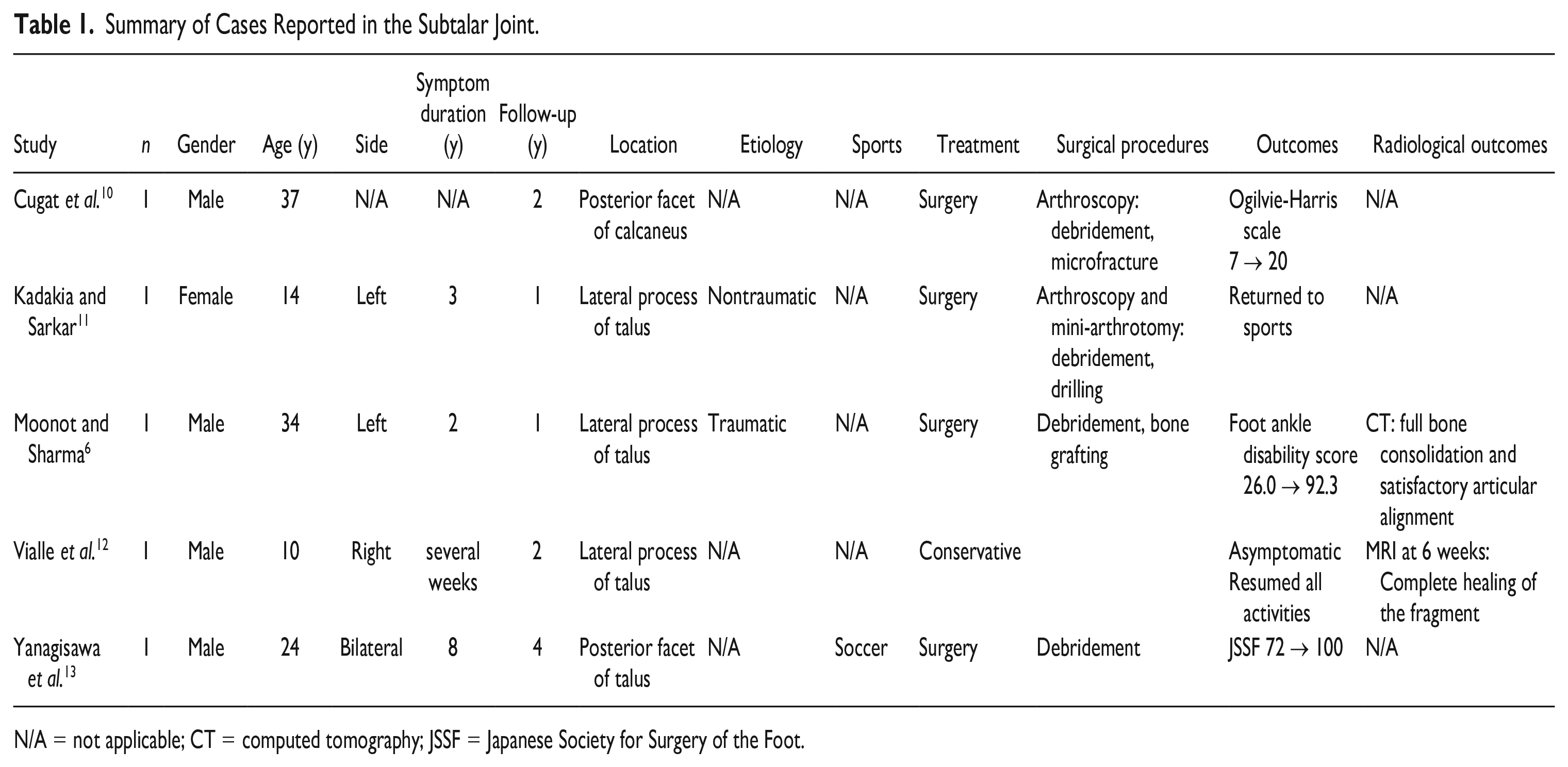
N/A = not applicable; CT = computed tomography; JSSF = Japanese Society for Surgery of the Foot.
Talonavicular Joint
A total of 15 patients with OCLs of the talonavicular joint were identified from 11 case reports.5,14-23 The mean age was 21.3 years (range, 9-43 years) and the mean follow-up was 30.1 months (range, 6-84 months). Ten lesions were located in the navicular bone, of which 4 cases were described as OCD. Five lesions were located in the head of the talus, all of which were children (age, 9-16 years). All patients were primarily treated with conservative methods. Only 1 patient succeeded in conservative treatment in the navicular lesions, but 3 of 5 patients with talar head lesions were successfully treated conservatively. Of those 3 children, 2 patients demonstrated complete radiographical healing. Surgical treatments included debridement, bone grafting, BMS, and biologics. Two case reports demonstrated arthroscopic technique using joint distraction technique for OCLs of talonavicular joint.17,20 All of the patients experienced good clinical outcomes. Nine case reports showed the radiological outcomes. The details are shown in Table 2.
Summary of Cases Reported in the Talonavicular Joint.
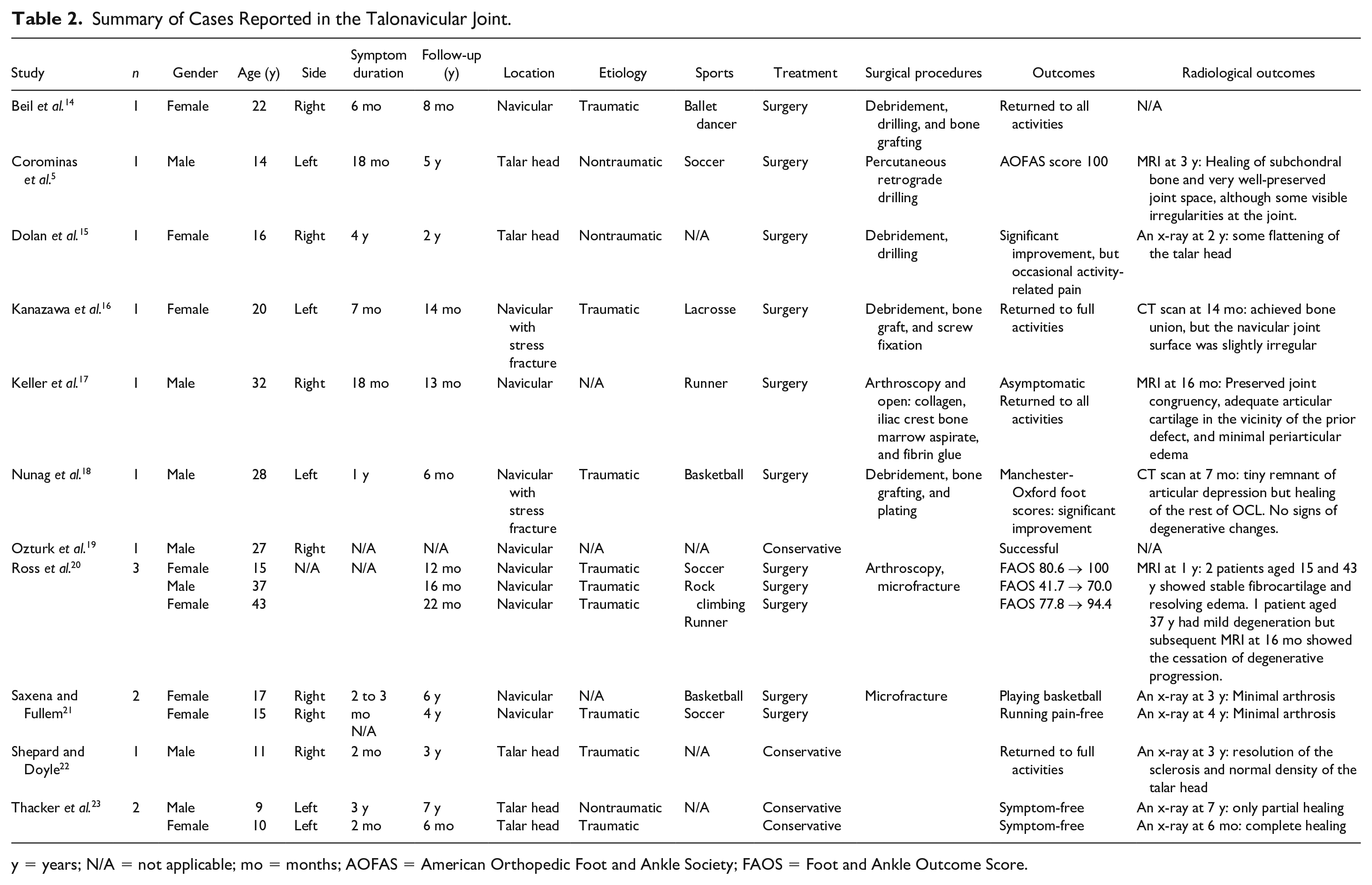
y = years; N/A = not applicable; mo = months; AOFAS = American Orthopedic Foot and Ankle Society; FAOS = Foot and Ankle Outcome Score.
Calcaneocuboid Joint
There was 1 case report demonstrating OCLs of the calcaneocuboid joint, which occurred after an ankle sprain. 24 The patient required surgical treatment, which included debridement, drilling, and the use of juvenile particulated allograft cartilage. At 8 months postoperatively, the patient could ambulate without pain. On postoperative radiographs, appropriate uniform joint space with no significant degenerative changes was observed (Table 3).
Summary of a Case in the Calcaneocuboid Joint.
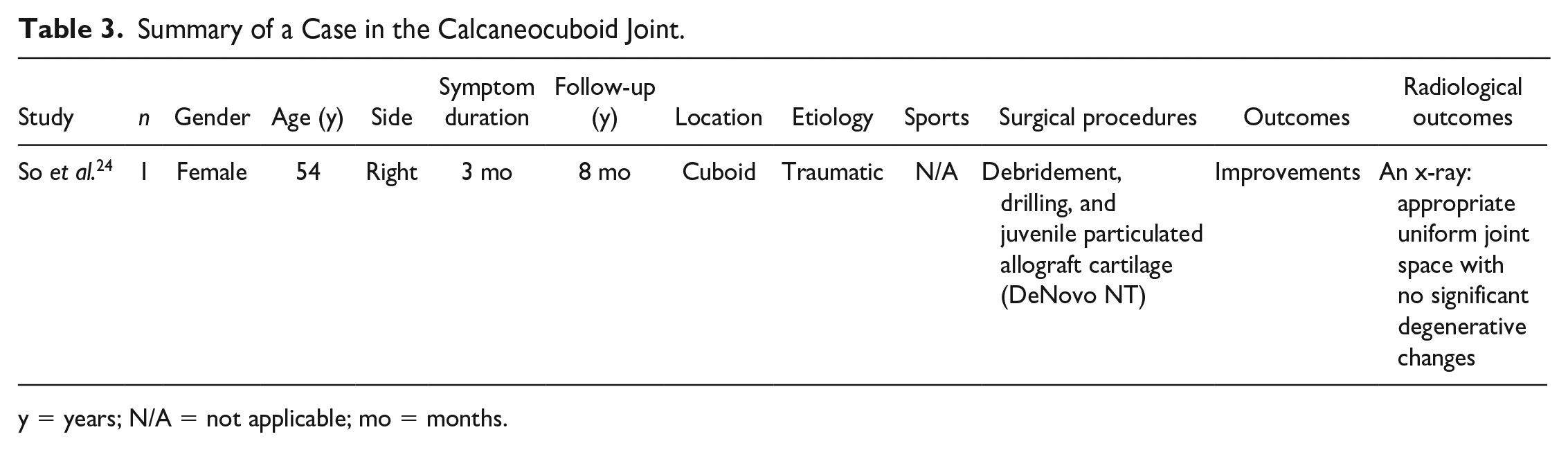
y = years; N/A = not applicable; mo = months.
Complications and Reoperations
No complications and reoperations were reported in the included case reports.
Discussion
This systematic review revealed that there is virtually no available evidence to ascertain clinical outcomes for cartilage lesions in the talonavicular joint, subtalar joint, and other midfoot joints, due to the paucity of literature describing treatment outcomes for the OCLs of these joints. Not even level-IV case series have been reported, which further underlines the need for more studies to investigate the efficacy and techniques for the treatment of OCLs in these joints. The etiology and pathology are also poorly reported. Possible pathomechanisms leading to OCL at these joints include shearing forces resulting from joint dislocations or subluxations and (temporary) interruption of local blood supply. Irregular OCLs may be observed with skeletal abnormalities.
OCLs are defined as lesions of the articular cartilage and underlying subchondral bone. As such, the term encompasses a variety of pathologies, including OCD, osteochondral defects, and osteochondral fractures. OCD is a focal idiopathic lesion of the subchondral bone with risk for instability and disruption of the adjacent articular cartilage.
26
In contrast to talar dome OCL, OCL of the subtalar joint is uncommon and not always symptomatic (
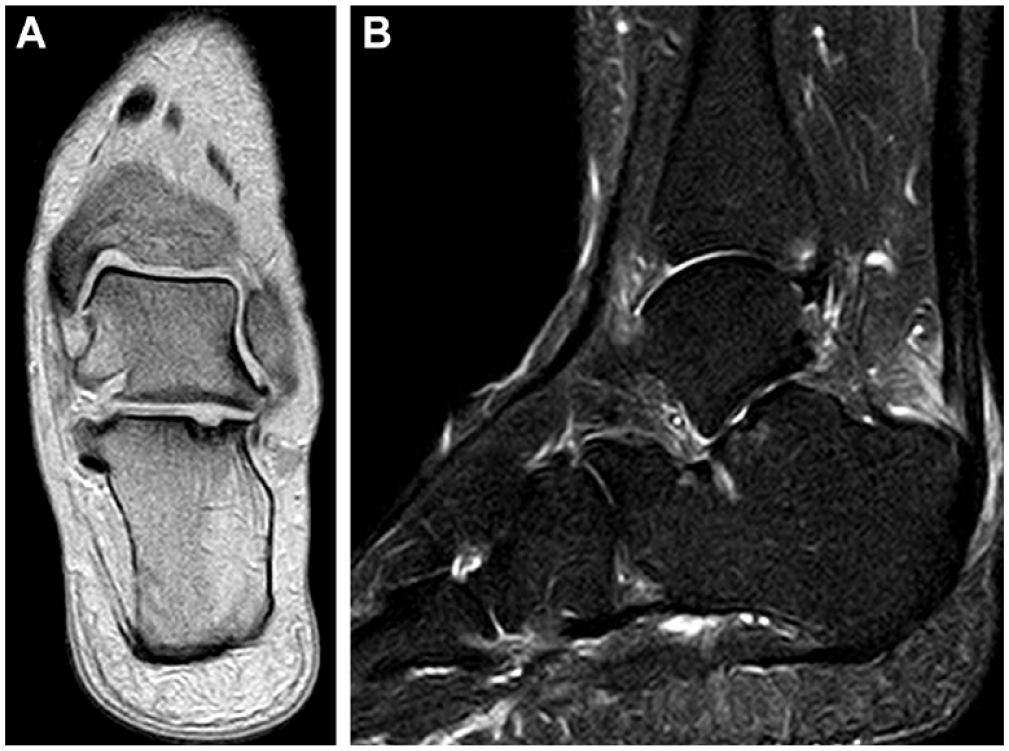
(A and B) Asymptomatic osteochondral lesion in the calcaneus at the posterior facet of the subtalar joint in a 48-year-old female. This was an incidental finding in a patient who was completely asymptomatic over the subtalar joint.
The choice of surgical treatment for OCL in the subtalar joint depends on a number of patient and surgeon factors and includes choosing between options such as debridement, fixation, repair technique, replacement technique, and use of biologics. Regarding the surgical approach, subtalar arthroscopy using the classic portals
28
offers a minimally invasive treatment option that enables the surgeon to directly inspect the lesions and it can help build treatment strategy, which may avoid unnecessary joint dissection. Subtalar arthroscopy has been established for the assessment, staging, and treatment of posttraumatic cartilage lesions following displaced intra-articular calcaneal fractures.
29
Arthroscopic and open subtalar arthrolysis combined with implant removal, debridement of adhesions, removal of loose bodies (
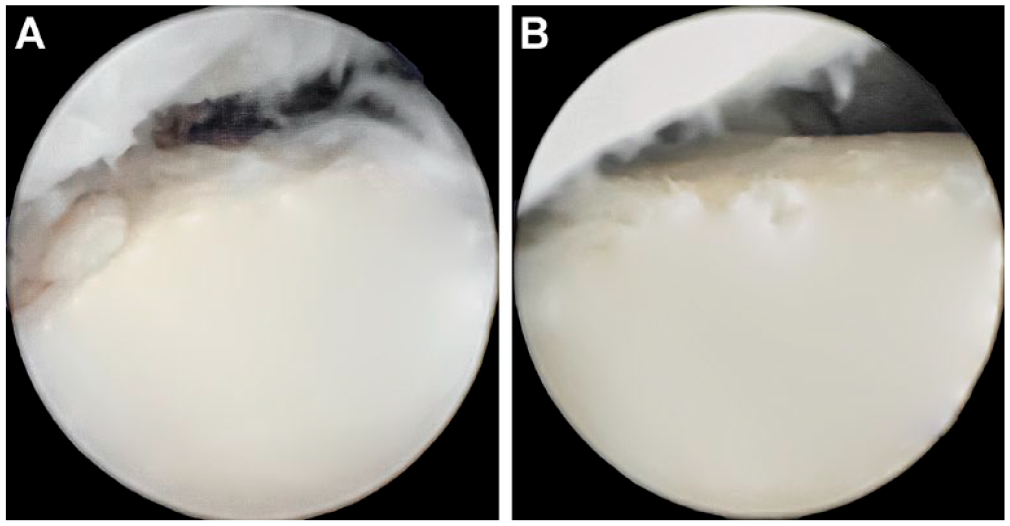
(A and B) Arthroscopic debridement of adhesions and a loose body from the subtalar joint.
Talonavicular OCLs are also uncommon
20
and a total of 15 cases have been identified in this review, consisting of 10 cases in the navicular and 5 cases in the talar head. All patients were primarily treated with conservative treatments and 10 cases eventually required surgeries, mainly including BMS. Although the exact cause of navicular OCL is unknown, it is thought to be associated with repetitive trauma to a poorly vascularized bone or residuals of a partial avascular necrosis (Köhler’s disease;

Symptomatic osteochondral lesion in the talonavicular joint of a 16-year-old female patient with a history of Köhler’s disease. The OCL was treated with curettage and drilling. OCL = osteochondral lesion.
There is an extreme paucity of literature describing OCLs of the calcaneocuboid joint. 24 Consequently, the specific mechanism of injury leading to the calcaneocuboid joint has not been also described, as well as for subtalar, talonavicular, and midfoot joints. It is conceivable, however, that any rotational or abduction/adduction force across the Chopart joint potentially exerts focal compression and shearing forces in the calcaneocuboid joint, leading to osteochondral damage. 3 The treatment methods should be considered depending on severity and chronicity of patients’ symptoms, and lesions characteristics. Both conservative and surgical management can be considered, but no conclusions can be made as to what treatments should be indicated depending on cases.
There were a number of limitations concerning this review. First, the low quality of the included studies with only case reports account as major limitations, which do not enable us to evaluate any data and make any conclusions. It was not possible to perform even a simplified pooling method. Second, the search criterion was limited to MEDLINE, Embase, and Cochrane Library Database reports. The clinical relevance of this review is that it first revealed the paucity of literature regarding cartilage lesions in the subtalar, talonavicular, and the midfoot joints. It is due to the nature of rare pathology in these joints, but this systematic review prompts further clinical studies.
Conclusion
This systematic review revealed that there is no available evidence to ascertain clinical outcomes of both conservative and surgical treatments for cartilage lesions in the subtalar joint, talonavicular joint, and other midfoot joints, owing to the extreme paucity of literature. Both nonoperative and operative treatments can be considered, but no treatment strategies have been established at this point. The etiology and pathology are also poorly reported.
Footnotes
Author Contributions
Y.S., S.R., and M.T. have made substantial contributions to the conception and design of the study, acquisition of data, and analysis of data. Y.S. and S.R. have been involved in the acquisition of data. Y.S. drafted the manuscript. All authors contributed to revising the manuscript and have given final approval of the version to be published.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was exempt from IRB (institutional review board) approval.