
Abstract
Objective
Müller-Weiss disease (MWD) is a challenging condition involving the perinavicular region in the initial stages and subsequently the entire foot in the later stages. The goal of this article is to describe the pathomechanics, clinical evaluation, and nonoperative and operative treatment, including a treatment algorithm, based on current evidence and the combined authors’ experience.
Design
We review the related articles and summarize the information about this condition.
Results
A number of related articles reveal that the treatments should focus on the management of degenerative regions and deformity correction to restore normal foot alignment and provide pain relief.
Conclusion
This systematic review proposes a treatment algorithm that is comprehensive and practical to apply for the management of MWD.
Introduction
Müller-Weiss disease (MWD) is a pathological condition characterized by a dysplastic navicular bone and its related consequences. 1 The definite cause is still unknown. 1 Its prevalence seems to be rare with regional variations in frequency. Approximately 0.6% of patients at the foot and ankle clinic presented with this condition based on registry data collected by the first author of this article. Regarding the cause, deformity of the navicular bone with signs of compression, condensation, and fragmentation led Konrad Weiss to believe that MWD was due to osteonecrosis. 2 However, osteonecrotic changes have not been consistently found in histological examinations, except for isolated fragments or when another cause for osteonecrosis was present.3-9 Advanced MWD results in arthritis of adjacent joints, including the talonavicular and/or naviculocuneiform joints. These abnormalities lead to abnormal biomechanics, collapse of the medial column of the foot, and severe deterioration in form and function. 1 Consensus regarding treatment guidelines has not yet been reached due to its rare prevalence. In addition, there is still a lack of data on the prognosis and outcomes following current treatments from the similarly mentioned reason.
This article aims to describe the pathomechanics, clinical evaluation, and nonoperative and operative treatment, including a treatment algorithm, based on a review of the current evidence and the combined authors’ experience to help understand and manage this uncommonly challenging condition.
Pathomechanics
MWD is a challenging condition that involves the navicular bone. The Monteagudo and Maceira’s study hypothesized that its incidence was high in populations after stressful conditions such as war or poverty. 1 It was postulated that growing bones underwent ossification changes caused by malnourishment during severe environmental conditions. However, a study by Doyle et al. did not identify any environmental or social factors as being predisposing. 10 Several entities have been proposed to cause MWD, including the abovementioned factors as well as traumatic factors.1,11 Nevertheless, any condition that creates a lateral shift in net compressive forces on the navicular bone will result in flattening and eventually fragmentation of its dorsolateral aspect. This leads to a secondary lateral shift of the talar head and hindfoot varus, both of which are constant findings in MWD. 11 Change of the navicular bone’s shape creates a perinavicular shape alteration and/or degeneration leading to talonavicular and/or naviculocuneiform arthritis, midfoot collapse, flattening of the medial longitudinal arch, and/or paradoxical pes planus varus. 11 These changes could result in a biplanar (in mediolateral and superoinferior directions) or triplanar deformity (biplanar plus rotational deformity of the talonavicular joint).
Clinical Evaluation
Clinical evaluation of MWD includes a comprehensive history and physical examination. Patients usually present with a history of chronic midfoot and hindfoot pain and might recall history of previous trauma. History regarding other medical conditions and medication should be obtained. Clinical examination often reveals swelling and tenderness over the dorsomedial aspect of the midfoot, as well as hindfoot varus with a normal or low medial longitudinal arch, depending on the severity of the disease.
11
The paradoxical combination of pes planus and hindfoot varus suggests advanced disease.
11
Gait and standing examinations are crucial for understanding the foot shape seen in MWD (

Clinical evaluation during the standing position as top view (
Imaging is necessary in MWD to plan appropriate treatment. Plain weightbearing radiographs indicate that a patient can tolerate pain while standing. Collapse of the lateral aspect of the navicular bone appears as a comma shape on radiographs.
11
These radiographs help to evaluate the integrity of the navicular bone and its surroundings, including the arch change (

Radiographic examination on anteroposterior view (
Nonoperative Treatments
Initial treatment of MWD is conservative and involves pain relieve and quality of life improvement using mechanical offloading orthoses, rehabilitation, and medication. Duration of conservative treatment varies greatly between authors, ranging from 2 to 60 months.14-16 The main conservative treatment option is mechanical offloading. As the pathology of MWD mainly involves the talonavicular joint and occasionally the naviculocuneiform joint, mechanical offloading using orthoses and gait aids can relieve pain over the affected joints and improve the ability to perform activities of daily living. Choosing an appropriate orthosis depends on the type and flexibility of the MWD deformity, which includes a decreased medial longitudinal arch due to perinavicular joint sagging and subtalar supination. Therefore, an orthosis with medial arch support and a lateral hindfoot wedge will provide temporary deformity correction and mechanical offloading in a patient with a flexible deformity. 1 In advanced disease with rigid deformity, an accommodative orthosis with a rocker sole shoe is more appropriate. The success rate of orthoses in all stages of MWD is approximately 80% without need for future surgery. 1 An orthosis with appropriate plantar support will also improve gait dynamics and limit disease progression. 17
Currently, a small number of studies report on the results of rehabilitation in MWD. As long-term subtalar supination could lead to tightness of the Achilles tendon, consistent and effective stretching exercises should be encouraged in all patients. Stretching exercises have also been suggested as an option for conservative treatment. 1 The use of magnetotherapy has successfully reduced pain in half of MWD patients. 1
Medication in MWD mainly provides short-term pain relief and is an option for conservative treatment. 1 In addition, patients should be counseled on effective lifestyle modifications, including reduction of body mass index.
The success rate of conservative treatment in MWD has been previously reported.17-19 Harnroongroj et al. studied the 5-year survivorship of conservative treatment in 32 patients with Maceira stage 3 MWD. The endpoint of survivorship was defined as the conversion to surgical treatment due to pain disturbing activities of daily living. Results showed that 5-year survivorship of conservative treatment was 56.3%. 17 Harnroongroj et al. also conducted a retrospective study on 68 MWD patients of which 29 patients failed and 39 patients succeeded on conservative treatment. The study determined that factors associated with failure of conservative treatment included an abducted midfoot (radiographic Meary angle more than 13°) and radiographic talonavicular arthritis. 19 Patients presenting with these descriptive factors should be informed about the increased likelihood of surgery. 19
There are no definite guidelines for the timeframe of follow-up for MWD patients treated conservatively. The authors recommend regular follow-up at 6 weeks, 3 months, 6 months, and annually from the initial visit to monitor the success of conservative treatment.
Operative Treatments
Generally, indications for orthopedic surgery are based on the severity of symptoms rather than the severity of deformity. Surgical patients usually have Maceira stage 3 and above disease. 11 Goals of surgical treatment are: (1) pain relief via arthrodesis of symptomatic degenerative joints and (2) restoration of the medial longitudinal arch and normal foot alignment.
A wide variety of surgical procedures have been proposed in the literature.10,11,15 These procedures include open or arthroscopic-assisted isolated talonavicular arthrodesis (
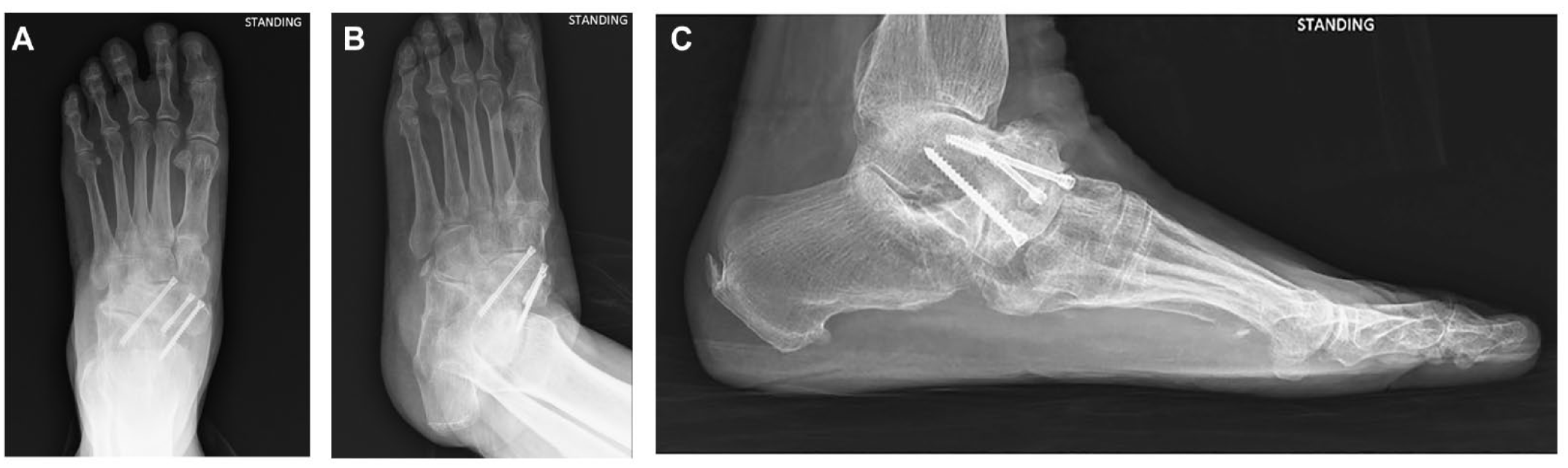
Postoperative radiographs on anteroposterior view (
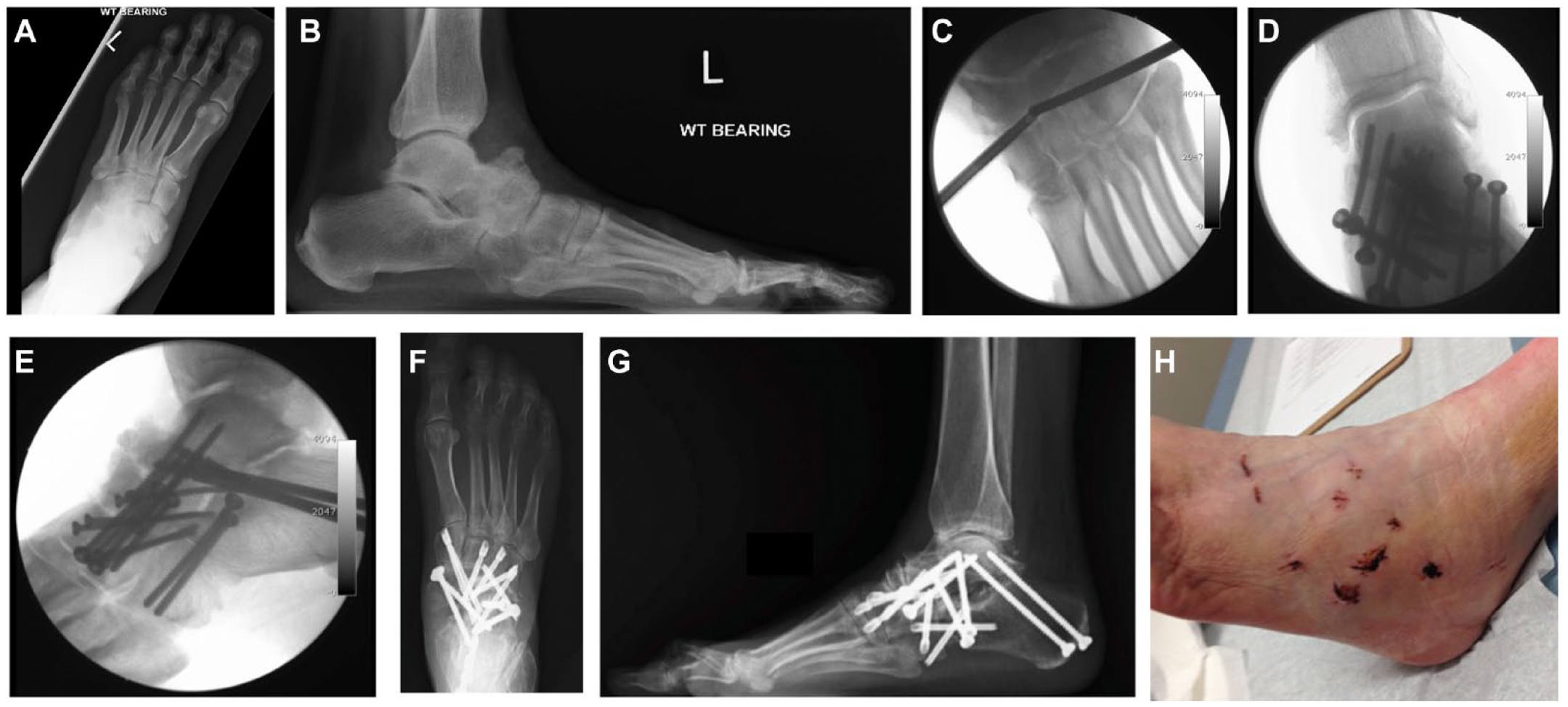
Preoperative radiographs on AP view (
In addition to the previously reported treatments, other adjunct procedures include Achilles tendon lengthening and removal of talar and ankle osteophytes, particularly if the arch is restored. Ahmed et al. 21 recommended that early diagnosis of MWD with pes planus permitted non-fusion treatment options. Calcaneal lengthening osteotomy in selected cases achieved satisfactory outcomes. 21 A navicular prosthesis might also be an option for lateral collapse of the navicular bone provided the articular surfaces of the talonavicular and naviculocuneiform joints are still spared. Angthong et al. 22 proposed in a study of data gathered from cadaveric specimens that the contralateral navicular bone can be used as a template to make a navicular bone prosthesis that could have built-in attachment holes for the posterior tibial tendon and spring ligament, serving as an alternative option for sparing joint motion. This prosthesis could be the treatment modality in the future as fusions continue to have limitations in the treatment of MWD. Isolated talonavicular arthrodesis usually fails to resolve the incongruence of the naviculocuneiform joint and carries a high risk of pseudoarthrosis.14,23 Talonavicular joint reduction is difficult to achieve with extensive scarring and ligamentous contraction at the subtalar joint level. 24 Yuan et al. 25 observed that intraoperative restoration of talus rotation was key to normal alignment of the subtalar joint/talonavicular joint. For severe deformity Tan et al. 20 has described complete excision of the diseased navicular bone and medial column tarsal reconstruction with a remodeled femoral head allograft. Fernández de Retana et al. 14 reported poor results for fracture reduction and internal fixation of the navicular bone in the presence of arthritic changes. Fernández de Retana et al. 14 further described TNC arthrodesis using trapezoid autologous graft to achieve arthrodesis and desired medial arch length. Cao et al. 23 have proposed TNC arthrodesis with a reverse V-shaped osteotomy as a dorsally based closing wedge osteotomy through the talonavicular joint.
However, a definitive treatment algorithm is needed. The present study collected evidence from the PubMed database using the following keywords: “Muller-Weiss or Müller-Weiss,” via a systematic review until August 2021 that yielded 40 studies. After applying the study inclusion criteria of at least 5 patients per study and a mean follow-up time of at least 1 year, 10 articles were included to determine the outcome of surgery for MWD (
Table 1
). Article selection and review were done by the first author as a nonblinded reviewer, rendering this a semi-formal version of a systematic review, which should be kept in mind with regard to its limitation in the level of evidence hierarchy. Based on this systematic review, the authors compiled a treatment algorithm for MWD (
Included Studies in the Systematic Review of the Eligible Studies about Surgical Procedures and Outcomes.
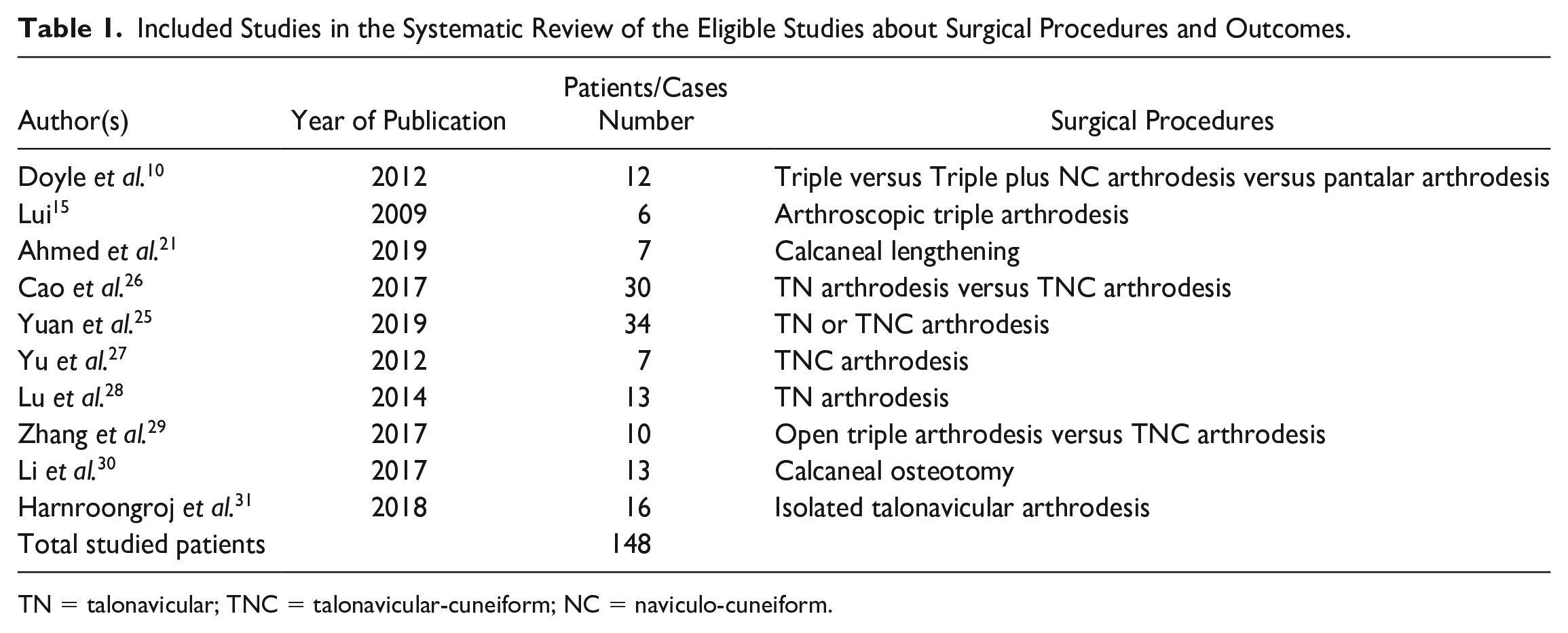
TN = talonavicular; TNC = talonavicular-cuneiform; NC = naviculo-cuneiform.
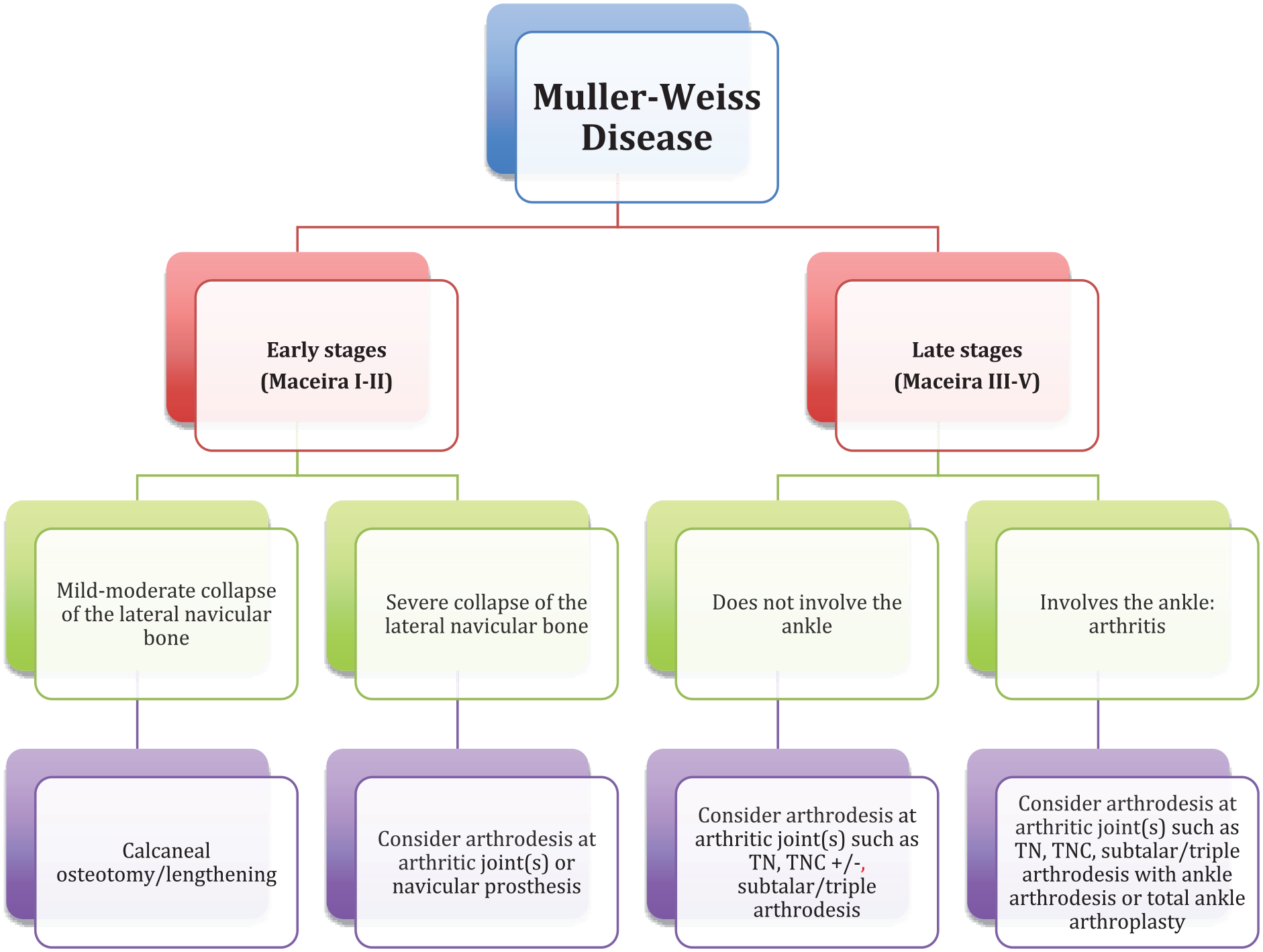
The present study’s proposed algorithm of surgical treatments for the Müller-Weiss Disease. TN = talonavicular; TNC = talonavicular-cuneiform.
Summary
MWD is a challenging condition involving first the perinavicular region and subsequently the entire foot in its later stages. Treatments should focus on the management of degenerative regions and deformity correction to restore normal foot alignment and provide pain relief. This systematic review proposes a treatment algorithm that is comprehensive and practical to apply for the management of MWD.
Footnotes
Authors’ Note
Name of the institution where the work reported was done: Faculty of Medicine, King Mongkut’s Institute of Technology Ladkrabang (KMITL), Bangkok, Thailand.
Acknowledgments and Funding
The authors would like to propose special thanks to Dr. Prasit Rajbhandari who assisted in drafting this paper. The present paper was edited by the English editing service (Editage). The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.