
Abstract
Objective
Ex vivo nanoindentation measurement has reported that elastic modulus decreases as cartilage degenerates, but no method has been established to macroscopically evaluate mechanical properties in vivo. The objective of this study was to evaluate the elastic modulus of knee joint cartilage based on macroscopic methods and to compare it with gross and histological findings of degeneration.
Design
Osteochondral sections were taken from 50 knees with osteoarthritis (average age, 75 years) undergoing total knee arthroplasty. The elastic modulus of the cartilage was measured with a specialized elasticity tester. Gross findings were recorded as International Cartilage Repair Society (ICRS) grade. Histological findings were graded as Mankin score and microscopic cartilage thickness measurement.
Results
In ICRS grades 0 to 2 knees with normal to moderate cartilage abnormalities, the elastic modulus of cartilage decreased significantly as cartilage degeneration progressed. The elastic modulus of cartilage was 12.2 ± 3.8 N/mm for ICRS grade 0, 6.3 ± 2.6 N/mm for ICRS grade 1, and 3.8 ± 2.4 N/mm for ICRS grade 2. Similarly, elastic modulus was correlated with Mankin score (r = −0.51, P < 0.001). Multiple regression analyses showed that increased Mankin score is the most relevant factor associated with decreased elastic modulus of the cartilage (t-value, −4.53; P < 0.001), followed by increased histological thickness of the cartilage (t-value, −3.15; P = 0.002).
Conclusions
Mechanical properties of damaged knee cartilage assessed with new macroscopic methods are strongly correlated with histological findings. The method has potential to become a nondestructive diagnostic modality for early cartilage damage in the clinical setting.
Keywords
Introduction
Articular cartilage injury due to osteoarthritis (OA) or trauma can cause joint pain and dysfunction. 1 It does not heal spontaneously due to lack of access to vasculature, nutrients, and progenitor cells.2,3 Therefore, various cartilage repair treatments such as osteochondral autograft transplantation and autologous chondrocyte implantation have been performed,4-6 but accurate assessments and repair of cartilage degeneration remain challenging. The International Cartilage Repair Society (ICRS) classification 7 has the intraclass coefficients (ICCs) of only 0.46 to 0.60 in porcine knees. 8 The Kellgren-Lawrence classification for the knee joint might underestimate gross findings of cartilage damage evaluated according to the ICRS classification. 9 Even with magnetic resonance imaging (MRI), knees with premorbid OA have similar cartilage thickness as healthy knees. 10
In addition, it remains unclear whether the mechanical properties of repaired cartilage are normalized because of lack of the clinically accessible evaluation devices in vivo. For instance, a previous study reported that the elastic modulus of ICRS grade 1 human knee cartilage was 0.50 ± 0.14 and 0.28 ± 0.12 MPa for ICRS grade 3 cartilage. 11 However, all studies of this kind are based on ex vivo testing with the nanoindentation test.12,13 The nanoindentation test is difficult to use in clinical practice with good reliability because the instruments are too large to use on knee joints in vivo. Indentation depth is only a few micrometers and is affected by vibrations from the surgeon. In addition, the relationship between histological score and the elastic modulus of articular cartilage has not been elucidated. This study involved the development of a new device that can directly quantify joint cartilage degeneration that is validated based on histological findings and elastic modulus status. The new elasticity tester has a compact size and deeper indentation depth than previous devices.
The primary aim of this study was to measure the elastic modulus of knee cartilage with various degrees of joint degeneration based on ICRS grade accurately using the new specialized elasticity tester as a preliminary evaluation for a future in vivo study. The second aim was to investigate the correlation between the elastic modulus of joint cartilage and cartilage thickness or degree of histological cartilage damage.
Materials and Methods
Recruitment of Participants
Patients with knee OA undergoing primary total knee arthroplasty (TKA) between December 2020 and December 2021 were included in the study. Patients with rheumatoid arthritis and those undergoing revision surgery were excluded. The study included 50 knees (43 varus knees and 7 valgus knees). All participants provided written informed consent. This study was approved by institutional review board (R2596-1). Patient demographic data were extracted from electronic medical records. Lower extremity alignment was evaluated based on hip-knee-ankle angle (HKAA) in weight-bearing anteroposterior full-leg radiographs.
Sample Collection
All TKAs were performed using the medial parapatellar approach. The distal femur was resected using a cutting guide that was placed perpendicular to the mechanical and anatomical axes for the coronal and sagittal planes, respectively. Femoral rotational alignment of the cutting guide was aligned with the surgical epicondylar axis. In this study, the medial distal and lateral distal femoral joint surfaces and the posterior medial and posterior lateral femoral joint surfaces, including cartilage and subchondral bone, were collected. The thickness of the samples obtained from the distal medial and lateral joint surfaces and posterior medial and lateral joint surfaces were 7.9 ± 1.4, 7.6 ± 1.8, 10.2 ± 1.2, and 7.6 ± 1.8 mm, respectively.
Gross Evaluation According to the ICRS Classification
The degree of cartilage damage was grossly evaluated according to the ICRS classification 7 just after the specimens were collected: 75% of the medial condyles were ICRS grade 3 or 4 due to varus deformity and 87% of the lateral condyles were grade 0 or 1 ( Table 1 ). The total number of specimens at each ICRS grade does not add up to 50 because in some cases the bone fragments were crushed during the surgical procedure and could not be evaluated ( Table 1 ).
Distribution of ICRS Grade in Four Areas According to the ICRS Mapping System and Histological Evaluation.
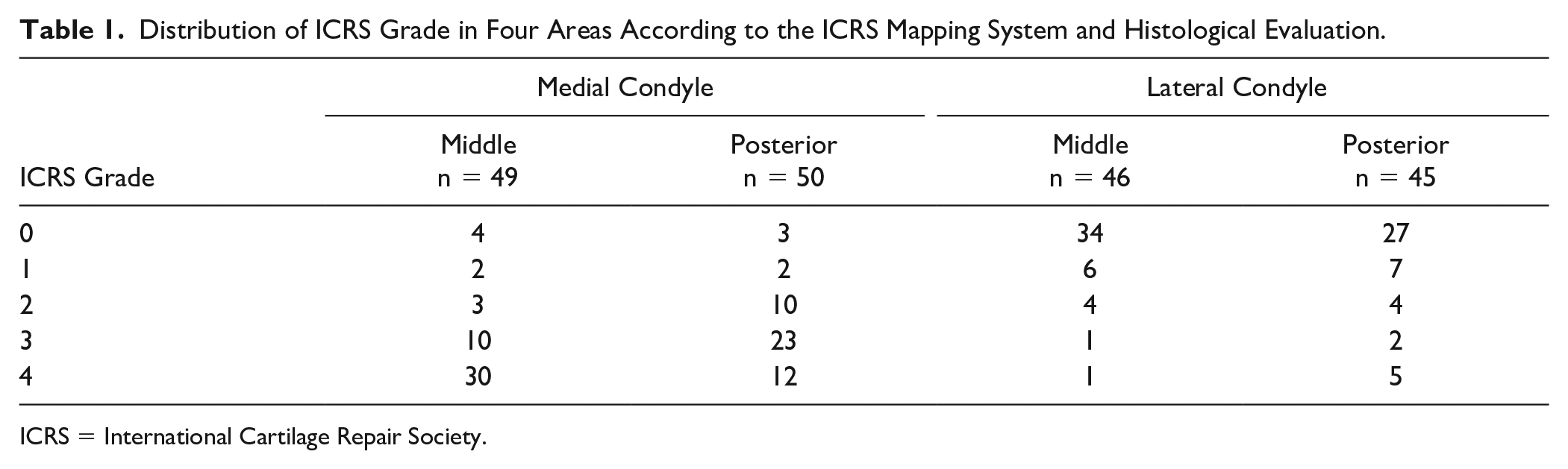
ICRS = International Cartilage Repair Society.
Evaluation of Mechanical Properties
Immediately after the specimens were collected, the central part from each of 18 sites of the specimen based on the ICRS mapping system
7
(
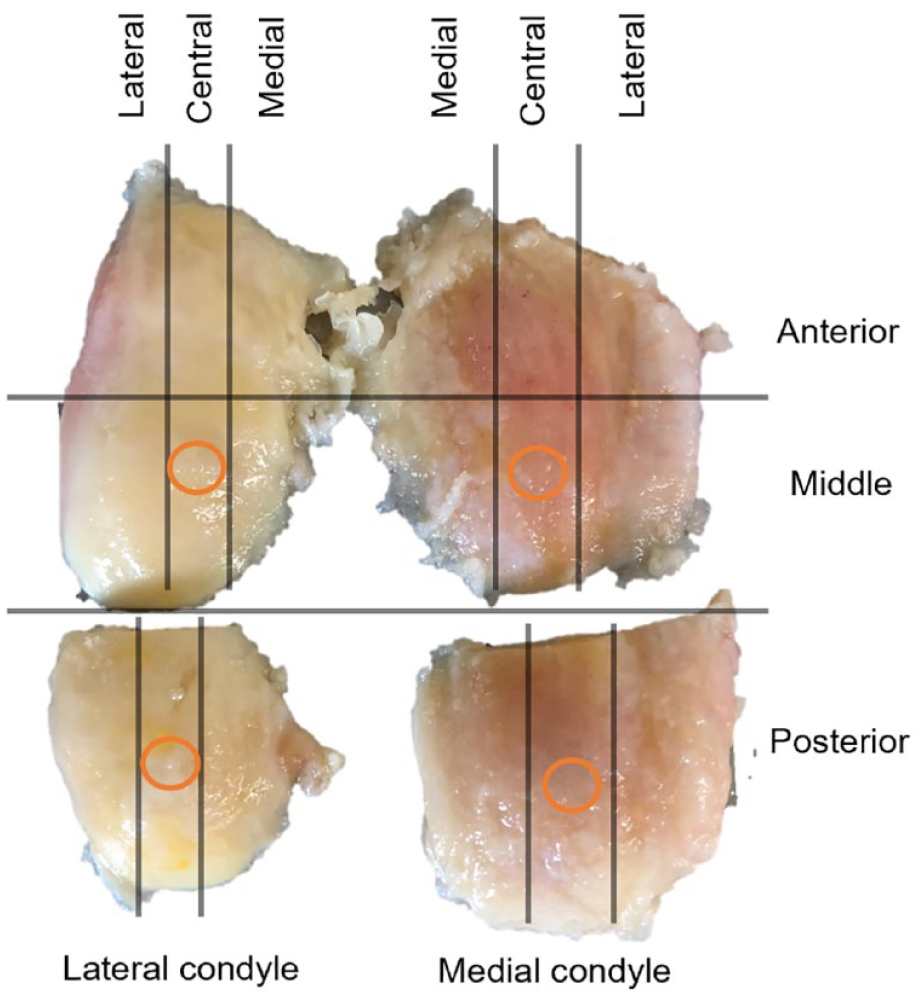
Distribution of regions of interest according to the International Cartilage Repair Society (ICRS) classification. Orange circles indicate areas that underwent histological evaluation.
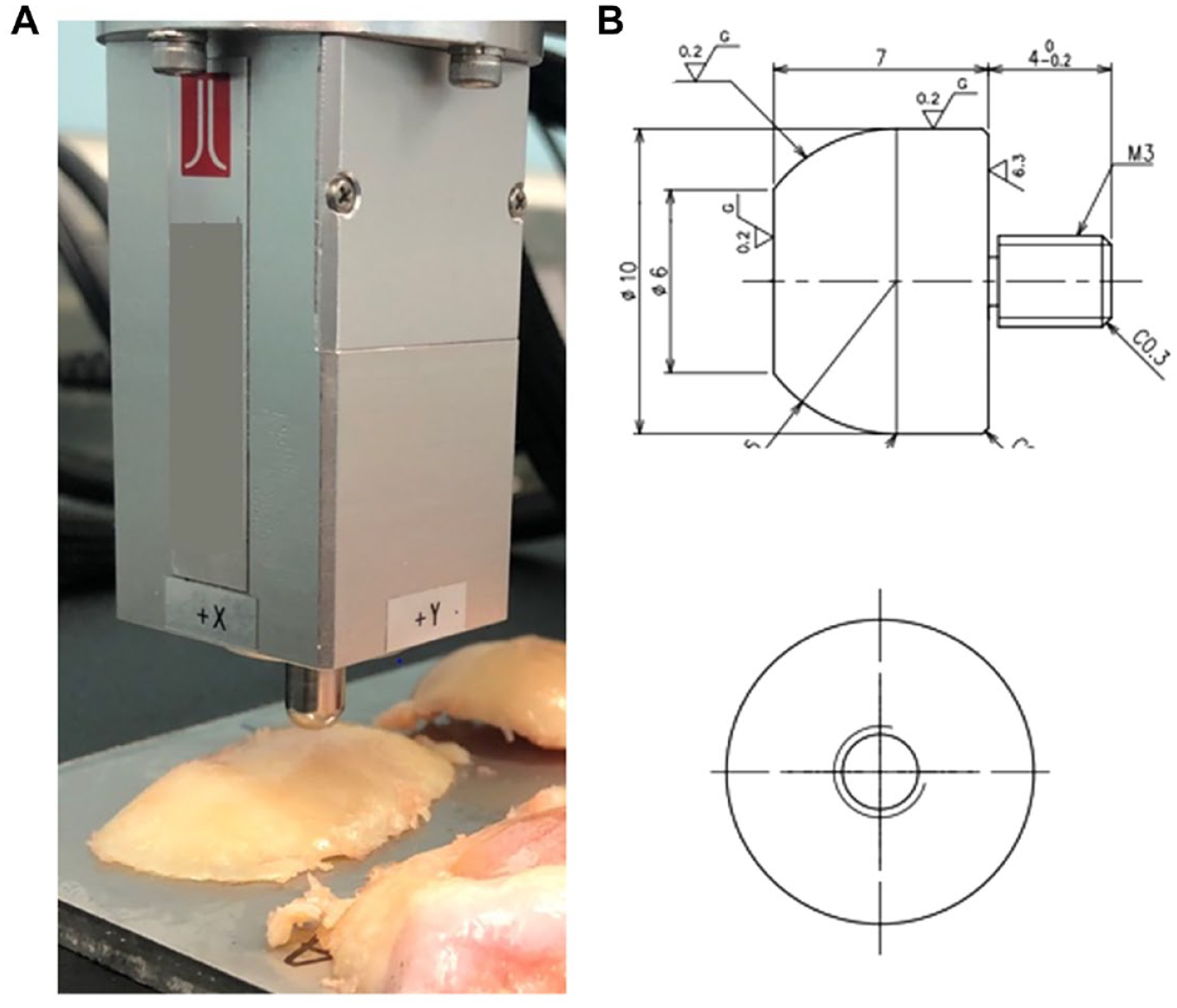
Instrument for measuring elastic modulus (A) and indentation probe (B).
The rationale for these measurement and analysis conditions is as follows. The thickness of normal human knee cartilage is approximately 2 mm. 15 It deforms elastically 7% to 23% during the walk cycle. 16 Based on these previous studies, the rate of cartilage deformation was set at 10%, and elastic modulus was calculated for the interval of 0.01 to 0.20 mm with an indentation depth of 0.25 mm. Since the number of steps per minute in a normal person is approximately 100, and the period from heel-strike to toe-off is 62% of the walk cycle, 17 the time from the start of pushing to the end of pushing was calculated to be 0.7 seconds. Therefore, the push-in speed was set to 0.7 mm/second to achieve a start-to-finish time of 0.7 seconds.
In addition, in a preliminary study, the same specimens were measured at various indentation speeds. In the preliminary study in 11 regions of interest from three knees, each site was measured five times at nine different speeds (45 times in total). The average of these measurements was defined as the true elastic modulus. The ratio of the measured elastic modulus at each speed to the true elastic modulus was calculated. The measurement results were highly consistent from 0.5 to 1.3 mm/second, but the results were unreliable at indentation speeds outside of this range (
Table 2
). In order to evaluate intraobserver reliability, the ICC was calculated by based on five measurements of the same area. The results were recorded at a frequency of 100 Hz. A graph depicting indentation depth and indentation force was generated with a dedicated application (
Ratio of Measured Elastic Modulus at Each Speed to True Elastic Modulus.
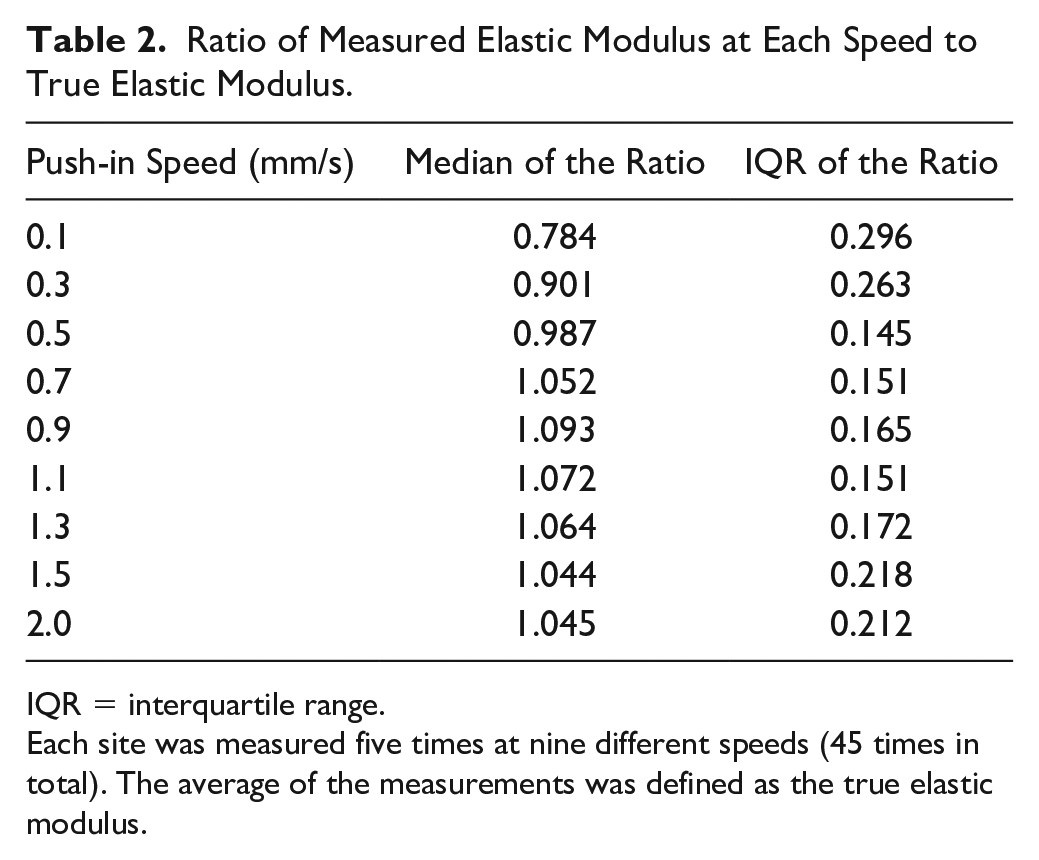
IQR = interquartile range.
Each site was measured five times at nine different speeds (45 times in total). The average of the measurements was defined as the true elastic modulus.
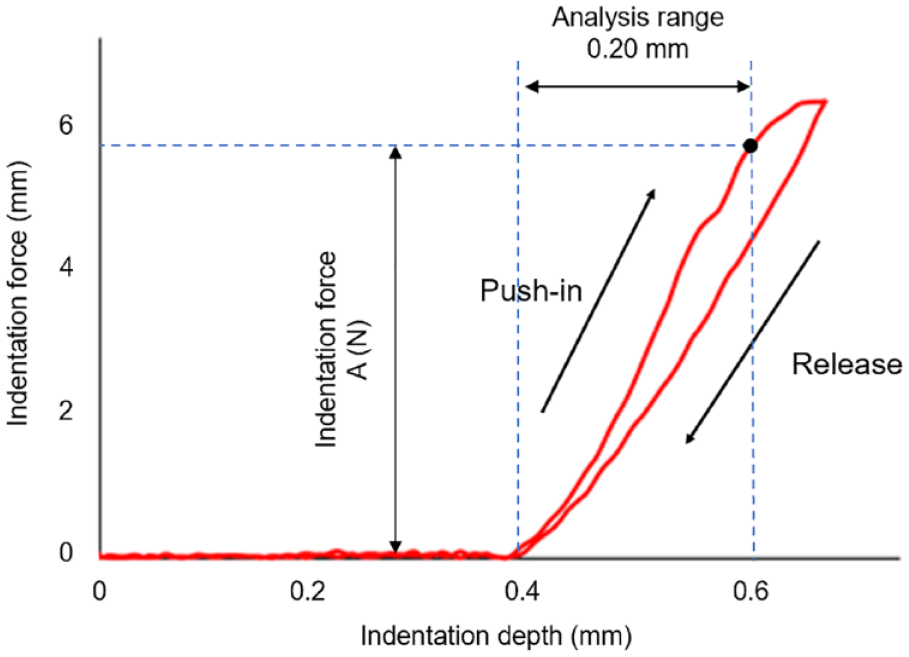
Graph for indentation depth and indentation force depicted on the dedicated application. Elastic modulus (N/mm) was calculated as A (N)/0.2 (mm).
Histological Evaluation
Of the four sections collected during TKA, the middle central and posterior central areas of the medial and lateral condyles, whose mechanical properties were evaluated, were cut out with a 6 mm diameter for histological evaluation. In
Figure 1
, the resected areas are shown in orange circles. The sections were fixed in 4% paraformaldehyde for 24 hours and then dipped in Morse solution (FUJIFILM Wako Pure Chemical Corporation; Osaka, Japan) for approximately 2 weeks for demineralization. Demineralized specimens were dehydrated in alcohol and permeabilized with xylene substitute. The specimens were then embedded in paraffin, cut into 5-μm sections, and deparaffinized with xylene substitute. Safranin O staining and fast green staining were performed. Each section was observed in quadruplicate under a microscope. The Mankin score was assessed and cartilage thickness was measured (
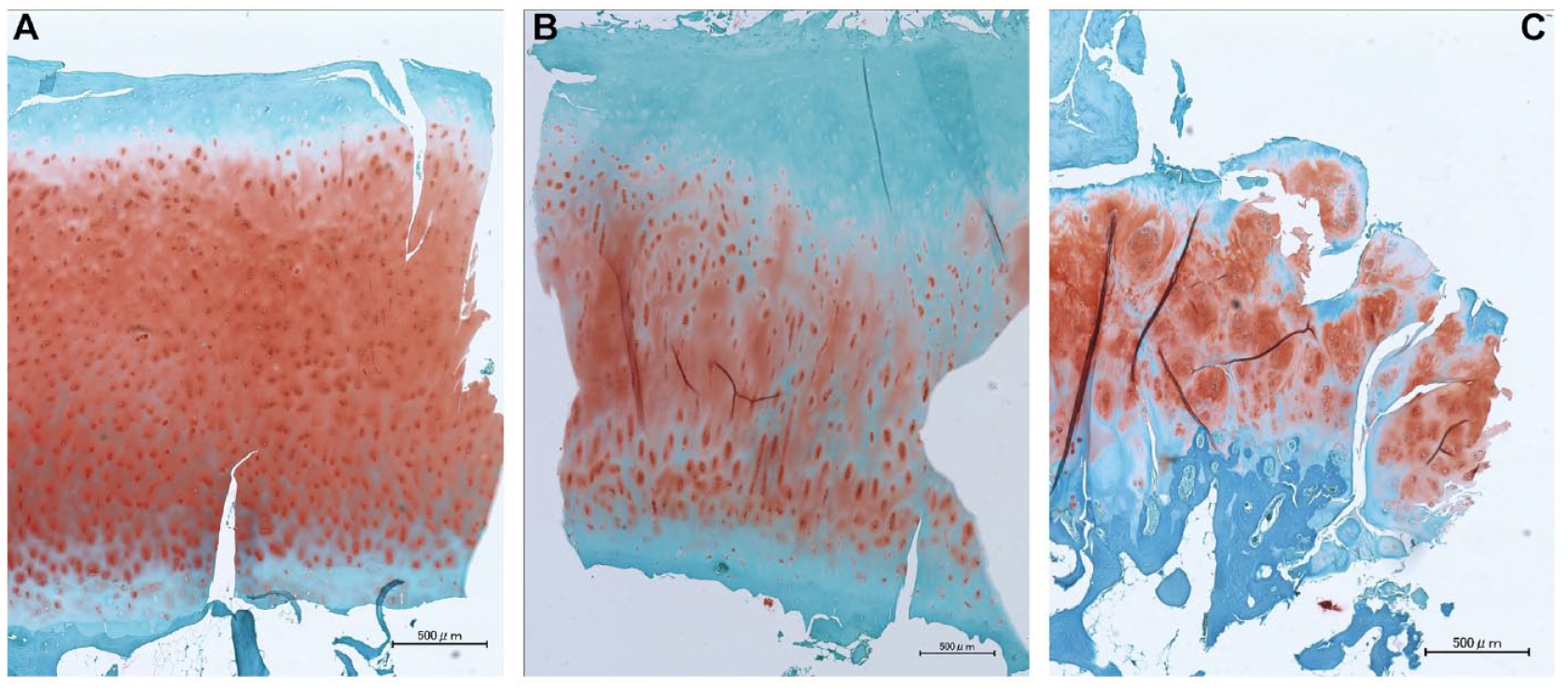
Typical histological findings. Micrographs of areas determined to be International Cartilage Repair Society (ICRS) grade 0 (A), grade 1 (B), and grade 2 (C). The surface of the cartilage is at the top of the image, and the subchondral bone side is on the bottom. The elastic modulus of cartilage was 14.3, 6.7, and 3.3 N/mm, respectively. Cartilage thickness was 2.6, 3.4, and 1.8 mm, respectively. Mankin score was 0, 3, and 7, respectively.
Statistical Analysis
The analysis was conducted in JMP Pro 15 (SAS Institute Inc., Cary, North Carolina, USA). Welch’s t-test was performed to assess the difference between two variables. The correlation coefficient between two variables was evaluated by Spearman’s rank correlation coefficient. Intraexaminer reliability was evaluated based on the ICC. ICCs of 0 to 0.20, 0.21 to 0.40, 0.41 to 0.60, 0.61 to 0.80, and 0.81 to 1.00 were considered to indicate slight, fair, moderate, substantial, and almost perfect reliability, respectively. 19 Differences were considered statistically significant when the P value was smaller than 0.05. Using the results of previous studies that measured the elastic modulus of normal and damaged cartilage using the nanoindentation test as a reference (normal, 9.81 ± 8.88 MPa; damaged, 4.46 ± 4.44 Mpa), 12 a power analysis performed using G*Power (University of Kiel; Kiel, Germany) determined that 38 normal and 38 abnormal samples were required, respectively. Therefore, the goal was to recruit 50 patients for this study. Four samples from the medial (distal and posterior) and lateral (distal and posterior) femoral joint surfaces can be taken from each patient. At least one or two samples might include cartilage that has not yet reached ICRS grade 4. Linear regression was performed to examine the factors associated with elastic modulus. Given the sample size, the explanatory variables were body mass index (BMI), age, Mankin score, and cartilage thickness.
Results
Of 50 knees, 30 were right knees and 39 patients were female. The average age, height, weight, BMI, and HKAA were 75.9 ± 6.1 years, 154.4 ± 8.4 cm, 62.7 ± 11.8 kg, 26.1 ± 3.4 kg/m2, and 7.6 ± 9.9º varus, respectively. The relationship between elastic modulus and ICRS grade is shown in
Figure 5
. Elastic modulus decreased significantly as ICRS grade worsened from 0 to 2 (
Table 3
). For ICRS grade 3 knees, there was a large variation. ICRS grade 4 knees had significantly higher elastic modulus than knees of other grades. The ICC of elastic modulus measurement was 0.98. The elastic modulus of ICRS grade 0 to 2 cartilage at 18 sites based on the ICRS mapping system is shown in a heat map (
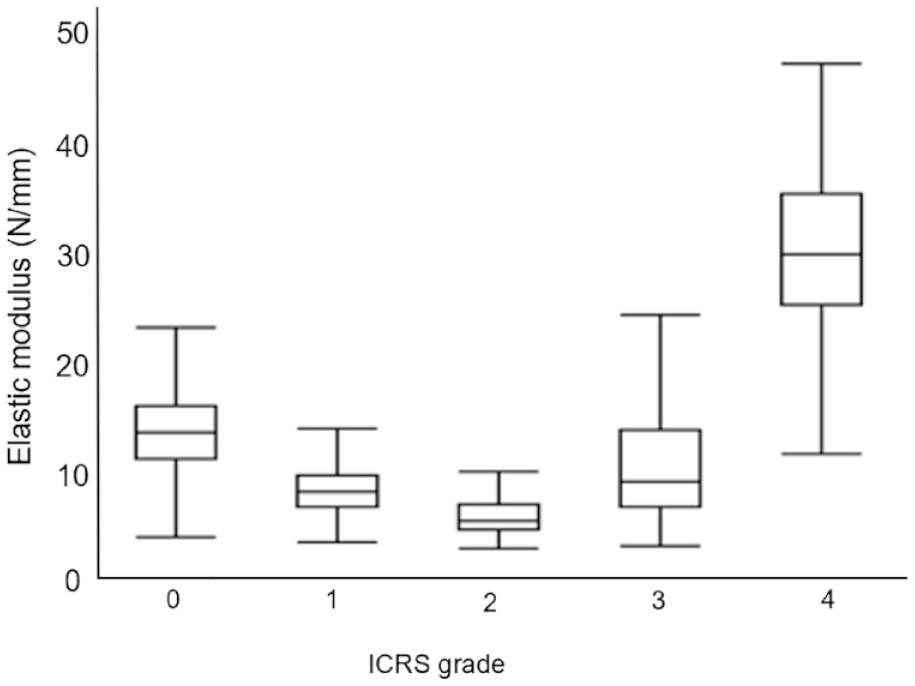
Relationship between the elastic modulus of cartilage and International Cartilage Repair Society (ICRS) grade. The interquartile range (IQR) is shown by the box. The horizontal line in the box indicates the median. The two ends of the whiskers indicate the minimum and maximum values of the points that fall within the following range: (first quartile − 1.5 × IQR) to (third quartile − 1.5 × IQR). There was a statistically significant difference (P < 0.001) between all groups based on the Wilcoxon rank sum test.
Elastic Modulus and Histological Cartilage Thickness by ICRS Grade.
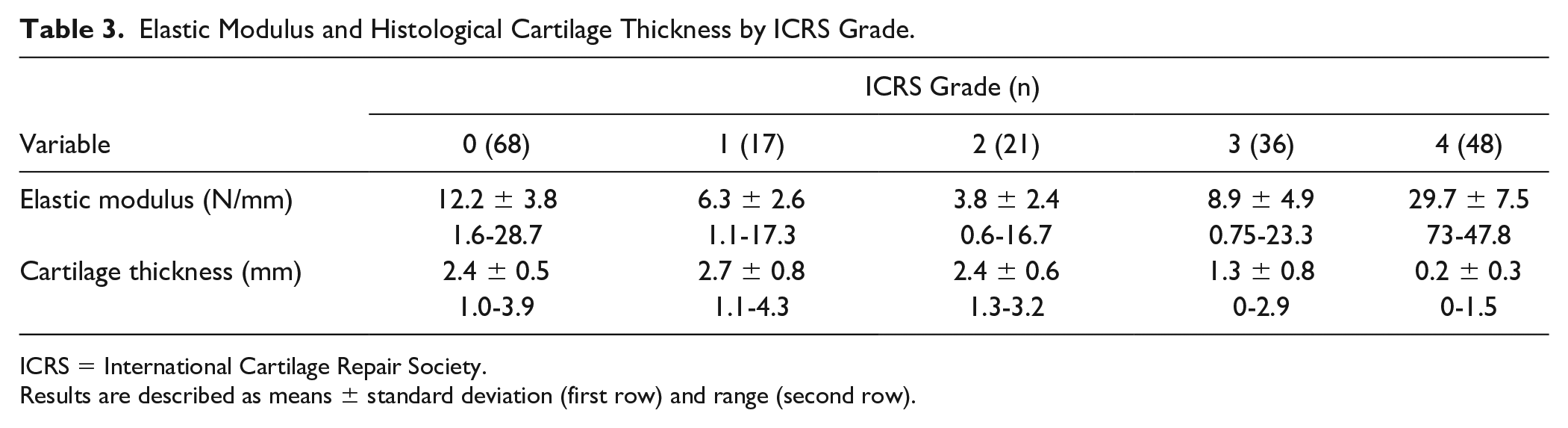
ICRS = International Cartilage Repair Society.
Results are described as means ± standard deviation (first row) and range (second row).
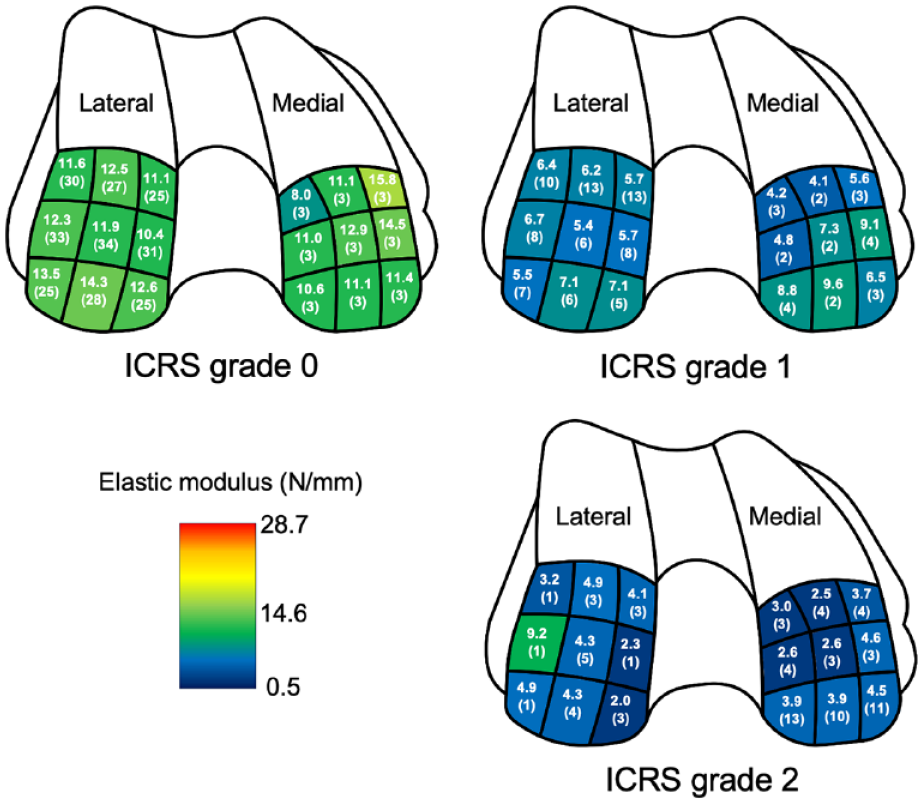
Elastic modulus of International Cartilage Repair Society (ICRS) grade 0–2 cartilage for each of the 18 sites according to the ICRS mapping system. The upper values are the average elastic modulus for each site. The lower values in parentheses are the number of samples measured. Colors in the heat map range from the minimum (blue, 0.5 N/mm) to the maximum (red, 28.7 N/mm) elastic modulus of cartilage values measured in this study.
The relationship between ICRS grade and histological cartilage thickness is shown in Figure 7 . Cartilage thickness was greatest in ICRS grade 1 specimens, but there were no significant differences in cartilage thickness between ICRS grades 0 and 2 ( Table 3 ).
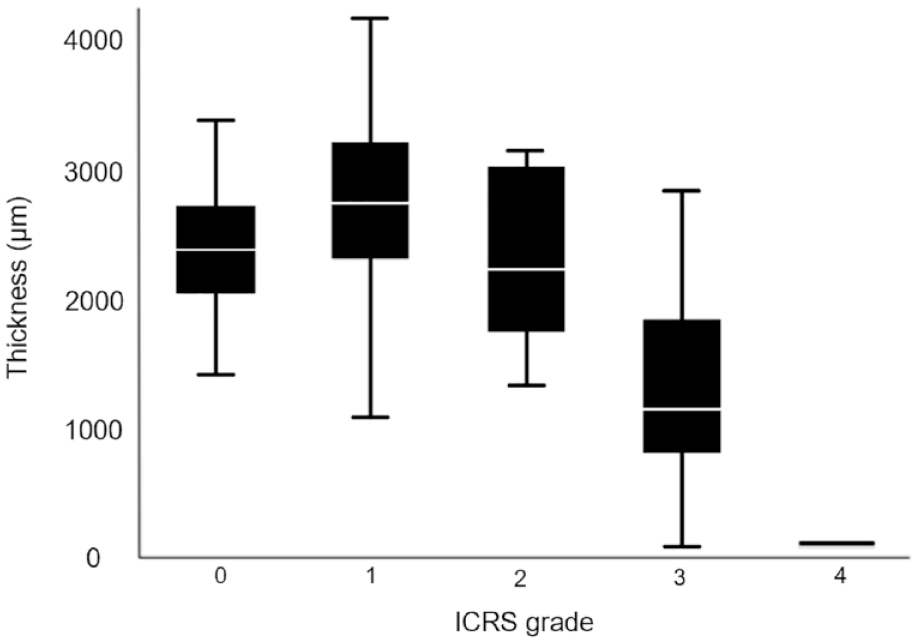
Relationship between histological cartilage thickness and International Cartilage Repair Society grade (ICRS). The interquartile range (IQR) is shown by the black box and the white horizontal line in the box indicates the median. The two ends of the whiskers indicate the minimum and maximum values of the points that fall within the following range: (first quartile − 1.5 × IQR) to (third quartile − 1.5 × IQR). There were no statistically significant differences between ICRS 0, 1, or 2 based on the Wilcoxon rank sum test.
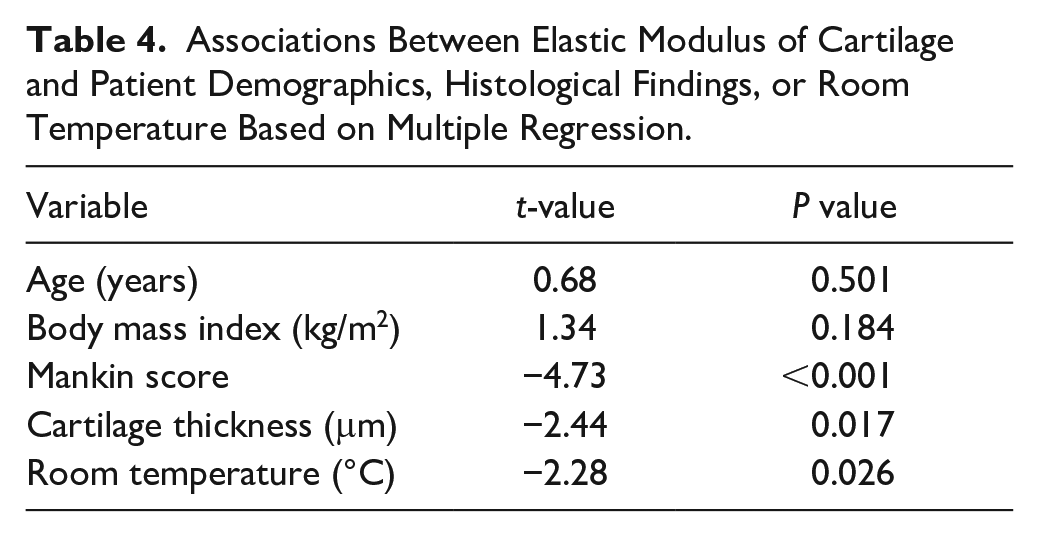
The relationship between Mankin score and elastic modulus of ICRS grade 0 to 2 samples is shown in Figure 8 . There was a negative correlation between Mankin score and elastic modulus. The strongest correlation was found between Mankin structural subscale score and elastic modulus (r = −0.612). Normal cartilage could be detected with a sensitivity of 88% and specificity of 70% when elastic modulus of 8.0 N/mm was used as the cutoff. Multiple regression analysis of elastic modulus, age, BMI, Mankin score, room temperature, and histological cartilage thickness showed that Mankin score are the most significant contributing factors, followed by histological cartilage thickness and room temperature ( Table 4 ). When sample collection site was added to the analysis, cartilage thickness was the most important contributor, followed by Mankin score.
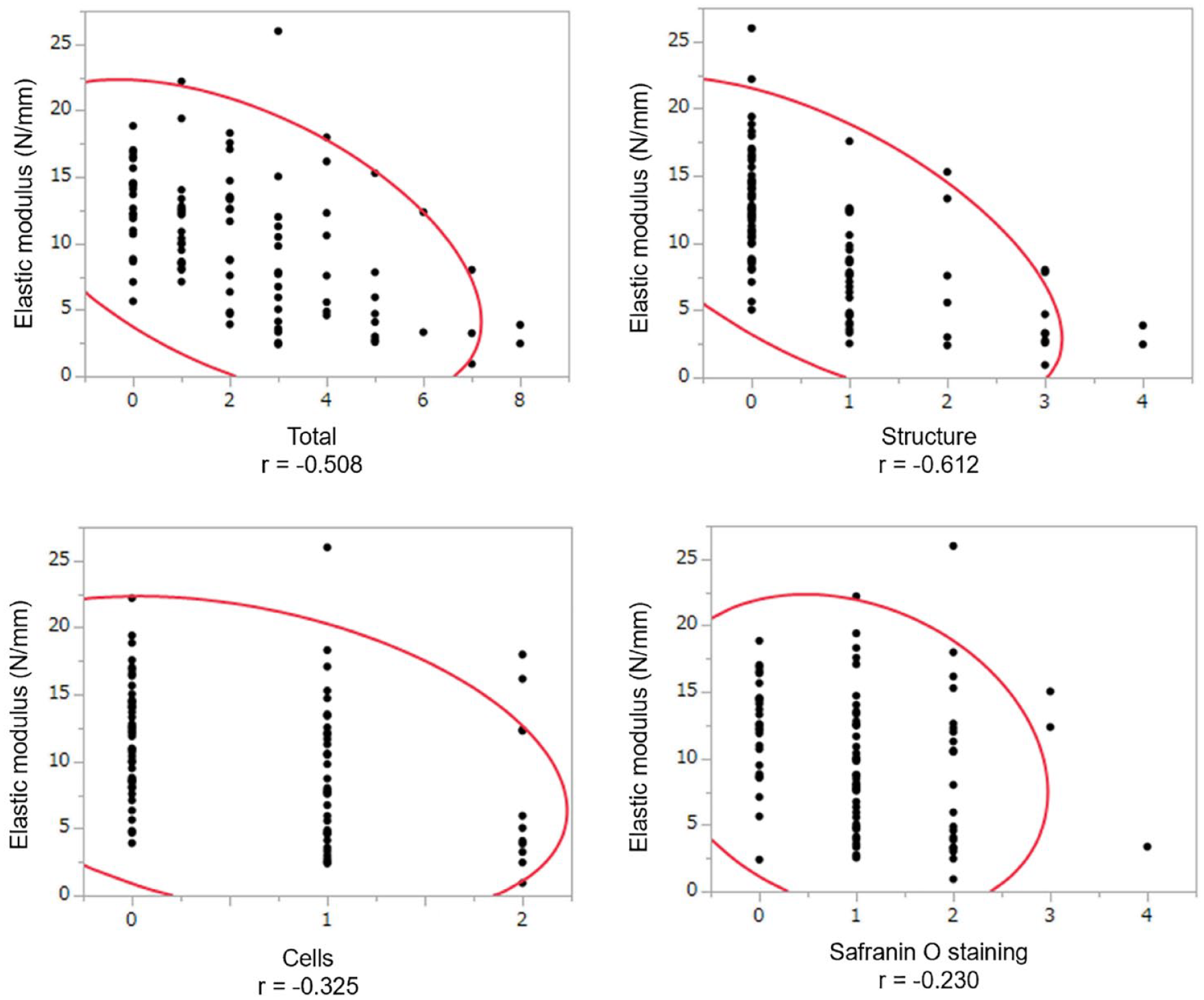
Relationship between Mankin score and elastic modulus. The horizontal axis shows the total score and the subscores for structure, cells, and safranin O staining, respectively. The red curve is the 95% probability ellipse.
Associations Between Elastic Modulus of Cartilage and Patient Demographics, Histological Findings, or Room Temperature Based on Multiple Regression.
Discussion
The elastic modulus of the articular cartilage decreases with degeneration and might be a useful indicator of cartilage quality.11,12 The nanoindentation test12,13 has been used to analyze cartilage ex vivo. However, the use of the conventional nanoindentation method in the actual surgical field is impractical due to the large size of the tabletop measurement device and the very small indentation depth of only approximately 10 mm. 12 In addition, the elasticity of joint cartilage normally functions only when subchondral bone is present, but previous studies12,13 have measured elasticity using small pieces of cartilage alone. In this study, a new portable and compact cartilage elasticity tester was developed for clinical use. It allows for nondestructive elasticity measurements of joint cartilage in the presence of subchondral bone. The device can also accurately measure cartilage in knee OA with an indentation depth of 0.2 mm. The ICC of the measurement was 0.98. Compared with ICRS grade 0 as the reference, elastic modulus was 48% lower for ICRS grade 1 and 69% lower for ICRS grade 2. These values are comparable to those of very sensitive nanoindentation tests performed previously and support the accuracy of the results of this study.12,13
The pre-OA phase is most receptive to various treatments, 20 but diagnosis remains difficult. For instance, concomitant knee cartilage damage with anterior cruciate ligament injury might affect the clinical outcome of arthroscopic reconstruction.21-23 If bone marrow lesions are present on preoperative MRI, slight cartilage damage might have occurred even if there are no gross findings on arthroscopy. During arthroscopic evaluation before high tibial osteotomy for medial OA,24-26 mild OA lesions in the lateral tibiofemoral compartment might also be missed with gross evaluation, while grossly identifiable cartilage damage has been reported to be more advanced histologically. 27 On the contrary, postoperative evaluation of osteochondral autograft transplantation and autologous chondrocyte implantation involves not only clinical scores and macroscopic findings 28 but also histological evaluation with biopsy to assess the extent of internal repair. 29 However, biopsy is a highly invasive procedure and damages cartilage, so a nondestructive technique is desirable. Therefore, this study employed an elastic modulus tester as an additional preliminary evaluation modality for early cartilage damage, considering its use during future arthroscopic surgeries.
It has been reported that ICRS grade, which is assessed based on gross findings, does not have sufficiently high reliability. 8 In Osteoarthritis Research Society International grade 1 lesions, histopathologic changes such as decreased safranin O staining occur, but the superficial structure is retained. 30 Therefore, it might be difficult to evaluate early cartilage damage grossly. We considered measurement of the elastic modulus of cartilage to be a new measurement modality for detecting early cartilage damage. We investigated the degree of reduction in the elastic modulus of cartilage in normal knees and knees with early cartilage damage. The elastic modulus measurements in this study had almost perfect intraexaminer reliability and a high correlation coefficient of −0.508 with histologic scores, so it might be more accurate in assessing early cartilage damage than other evaluation methods, such as ICRS classification of gross findings. There was a substantial negative correlation between Mankin score and elastic modulus (r = −0.612). However, we believe it to be accurate enough for clinical use. When cartilage with a Mankin score of 2 or less was considered normal, normal cartilage could be detected with a sensitivity of 88% and specificity of 70% when elastic modulus of 8.0 N/mm was set at a cutoff.
Furthermore, this study is the first to quantitatively demonstrate a relationship between cartilage thickness and elastic modulus or degree of histological damage in human articular cartilage. In this study, a slight increase in cartilage thickness was found in ICRS grade 1 lesions (2.7 ± 0.8 mm; range, 1.1–4.3 mm) compared to ICRS grade 0 lesions (2.4 ± 0.5 mm; range, 1.0–3.9 mm) (
This study has several limitations. First, although the results were consistent with previous studies, it is not certain that ex vivo results accurately reflect the intra-articular conditions. Second, despite the high correlation between the histological findings and elastic modulus, this study did not include molecular biological analysis, such as analysis of collagen fiber composition. Third, all of the elastic modulus of cartilage measurements were performed at room temperature in a controlled air-conditioned environment, but results might be different when measurements are performed during actual arthroscopic surgery. Fourth, the patients were older than 60 years and from a single ethnic group. It would be desirable to analyze other groups, including younger patients or participants from variable ethnicities to determine whether the same tendency could be confirmed in these populations. Fifth, samples of normal areas were provided by patients who underwent TKA, which might not be from truly normal knees. The elastic modulus of cartilage corresponding to ICRS grades 0 and 1 at the lateral femoral condyle was slightly higher in the posterior area than in the middle area. The number of medial samples was limited. Whether the posterior cartilage was originally harder or closer to a normal state is an issue for a future study. Sixth, it is unclear how these results relate to clinical outcomes. In vivo studies with arthroscopy are desirable to validate this study. Further development of arthroscopic probes or complete waterproofing and accessibility of the measurement device are needed.
In conclusion, this study demonstrated that mechanical property evaluation of knee cartilage damage using new macroscopic methods correlates very well with histological evaluation. Mechanical property evaluation can become a nondestructive diagnostic modality for early cartilage damage in the clinical setting.
Footnotes
Authors’ Note
This investigation was performed at Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University Hospital.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI (grant number. JP21K09322). This study received grants from Tech-Gihan (Kyoto, Japan).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The production of the indentation probe used in this study was supported by Tech-Gihan (Kyoto, Japan).
Ethics Approval
This study was approved by the institutional review board (R2596-1).