
Abstract
Background
This study explores the impact of subchondral bone plate necrosis on the development of the osteonecrosis of femoral head (ONFH) and its joint collapse.
Methods
This retrospective study included 76 ONFH patients (89 consecutive hips) with Association for Research on Osseous Circulation stage II who received conservative treatment without surgical intervention. The mean follow-up time was 15.60 ± 12.29 months. ONFH was divided into 2 types (I and II): Type I with a necrotic lesion involving subchondral bone plate and Type II with a necrotic lesion not involving subchondral bone plate. The radiological evaluations were based on plain x-rays. The data were analyzed using SPSS 26.0 statistical software.
Results
The collapse rate in Type I ONFH was significantly higher than that in Type II ONFH (P < 0.001). The survival time of hips with Type I ONFH was significantly shorter than those with Type II ONFH and with the endpoint of the femoral head collapse (P < 0.001). The collapse rate of Type I in the new classification (80.95%) was higher compared with that of the China-Japan Friendship Hospital (CJFH) classification (63.64%), and the difference was statistically significant (χ2 = 1.776, P = 0.024).
Conclusion
Subchondral bone plate necrosis is an important factor that affects ONFH collapse and prognosis. Current classification using subchondral bone plate necrosis is more sensitive for predicting collapse compared with the CJFH classification. Effective treatments should be taken to prevent collapse if ONFH necrotic lesions involve the subchondral bone plate.
Introduction
Osteonecrosis of the femoral head (ONFH) is a pathological process of the death of bone cells, bone marrow hematopoietic cells, and fat cells in the femoral head caused by different etiologies. Non-traumatic ONFH is a refractory and progressive disease that commonly affects young patients and has a poorly understood etiology and pathogenesis. 1 It is estimated that approximately 8.12 million people over the age of 15 have ONFH in China, leading to loss of employment and causing an unbearable economic burden for patients, their families, and society. 2 Without effective treatment, ONFH can progress and might eventually cause femoral head collapse and degenerative changes to the hip joint, resulting in total hip arthroplasty (THA). However, THA is not suitable for young, highly active patients with ONFH because most will likely outlive their prosthesis and require a revision.
The key to ONFH treatment is whether it can be identified early and to control the expansion of necrotic foci, preserve the hip joint and delay THA. The femoral head collapse marks a watershed in treatment choice and patients’ prognosis. Therefore, predicting the potential risk of collapse and timely treating high-risk patients are critical for the disease prognosis. To predict collapse, many clinical ONFH staging and classification methods have been proposed, including the Association for Research on Osseous Circulation (ARCO) phase, 3 Ficat classification, 4 Japanese Investigation Committee (JIC) classification, 5 and our previously proposed China-Japan Friendship Hospital (CJFH) classification. 6 Most prediction methods of osteonecrosis femoral head collapse are assessed via imaging, the location, size, and volume of necrosis focus using x-ray and magnetic resonance imaging.7,8 In addition, some studies have found that 18F-fluoride positron emission tomography can predict the collapse of the femoral head using SUVmax (maximum standardized dupe value), 9 and the SUVmax value increases with the increase of osteonecrosis severity. Zhao et al. 10 and Li et al. 11 reconstructed the ONFH model using finite element technology and predicted the collapse by the volume and the stress distribution of the necrotic part. Kang et al. 12 found that bone mineral density can better reflect the biomechanical characteristics of the femoral head and the microstructure of cancellous bone and can be used to predict ONFH collapse. Liu et al. 13 analyzed the regional distribution of ONFH cystic lesions using 3-dimensional reconstruction and found that the distribution of cystic lesions was related to stress and could accelerate the femoral head collapse.
Although a variety of methods for predicting femoral head collapse have been put forward, conservative treatments have generally been ineffective at preventing progression, and the outcomes of joint-preserving surgeries are still not satisfactory in clinical practice. In our earlier study, we observed the clinical efficacy of porous tantalum rod implantation for ONFH, which showed a failure rate of 26.2% in ARCO stage II patients and as high as 61.3% in ARCO stage III patients. 14 As for bone impaction graft surgery, which is widely used clinically, about a quarter of ARCO stage II patients still end up receiving total hip replacement. 15 As a consequence, it is necessary to establish a new classification method to assisting in treatment selections, improve the existing treatments, and guide the development of new treatment methods.
Currently, the prognostic methods in clinical application mainly consider whether the necrotic site involves the lateral column, as well as general conditions such as necrotic volume, and size. And in clinical practice, we also found such a phenomenon: through MRI evaluation, if the necrotic site involves the femoral head subchondral bone plate, the prognosis of joint-preserving surgery for such patients is very poor and most patients will have femoral head collapse. However, if necrosis does not involve the subchondral bone plate, such patients can exhibit good therapeutic effects through conservative or surgical treatment, and the incidence of femoral head collapse is much lower than patients with subchondral bone plate involvement.
The good biomechanical properties of the subchondral bone play an essential role in maintaining the femoral head morphology. The subchondral bone plate is composed of rod-like and plate-like trabeculae in an appropriate proportion, supporting and dispersing stress.
To our knowledge, there is currently no classification method using subchondral bone plate involvement although relationship of ONFH and subchondral bone quality is already known. At the same time, subchondral bone plate is important for prognosis and treatment selection of ONFH. According to the current classification using subchondral bone plate necrosis, we can develop more basic research on the subchondral bone plate and explore new treatment methods to delay subchondral bone plate necrosis or even reconstruct the subchondral bone plate structure to prevent ONFH. Therefore, this study aimed at exploring the effect of subchondral bone plate necrosis on ONFH collapse and development.
Materials and Methods
Patient Data
We retrospectively analyzed 76 patients (89 consecutive hips) with ONFH who visited the Department of Orthopaedics of CJFH from January 2016 to January 2019. The study was conducted following the Declaration of Helsinki and approved by the Ethics Committee of CJFH. These patients were diagnosed with ONFH using x-ray and staged as ARCO stage II. No collapse of the femoral head occurred. Then, the initial MRI examination was performed to determine the extent of necrosis. There were 55 males and 21 females with an average age of 38.42 ± 8.27. The average follow-up time of these patients after the initial MRI examination was 15.60 ± 12.29 months, and the average body mass index was 24.90 ± 3.31. Among these patients with ONFH, 27 patients were due to alcohol abuse, 39 patients were due to glucocorticoid, and 10 patients were idiopathic ONFH. The patients above refused the surgical intervention treatment and conservative treatment was provided, including protective weight-bearing, oral medicine, or extracorporeal shock wave therapy. All baseline data are shown in Table 1.
Patient Demographics.
All qualitative variables are presented as numbers except age, which is presented as mean ± SD.
ONFH Classification in MRI Evaluation
The ONFH location was divided into 2 types (I and II) according to the involvement of necrosis in the subchondral bone plate in a mid-coronal section on hip MRI: I, necrotic lesion involving the subchondral bone plate; II, necrotic lesion not involving the subchondral bone plate ( Fig. 1 ). Using this type to predict the prognosis of the patients with ONFH and the efficacy of joint-preserving surgery for ONFH, the Type I was 63 hips and the Type II was 26 hips. During the follow-up period, 53 hips collapsed, including 51 of Type I and 2 Type II. In the non-collapsed ONFH hips, there were 12 Type I and 24 Type II. To ensure that the above classification using subchondral bone plate necrosis would be better than the current clinical approach, all the subjects with ONFH were also classified according to CJFH based on 3 pillars. ONFH location was divided into 3 types (M, C, and L), and the intact degree of the lateral pillar was divided into subtypes (L1, L2, and L3). The CJFH types were Type L1 in 12 hips, Type L2 in 45 hips, Type L3 in 32 hips, and types M and C in 0 hips. In the collapsed ONFH hips during the follow-up period, there were 4 L1, 27 L2, and 22 L3.
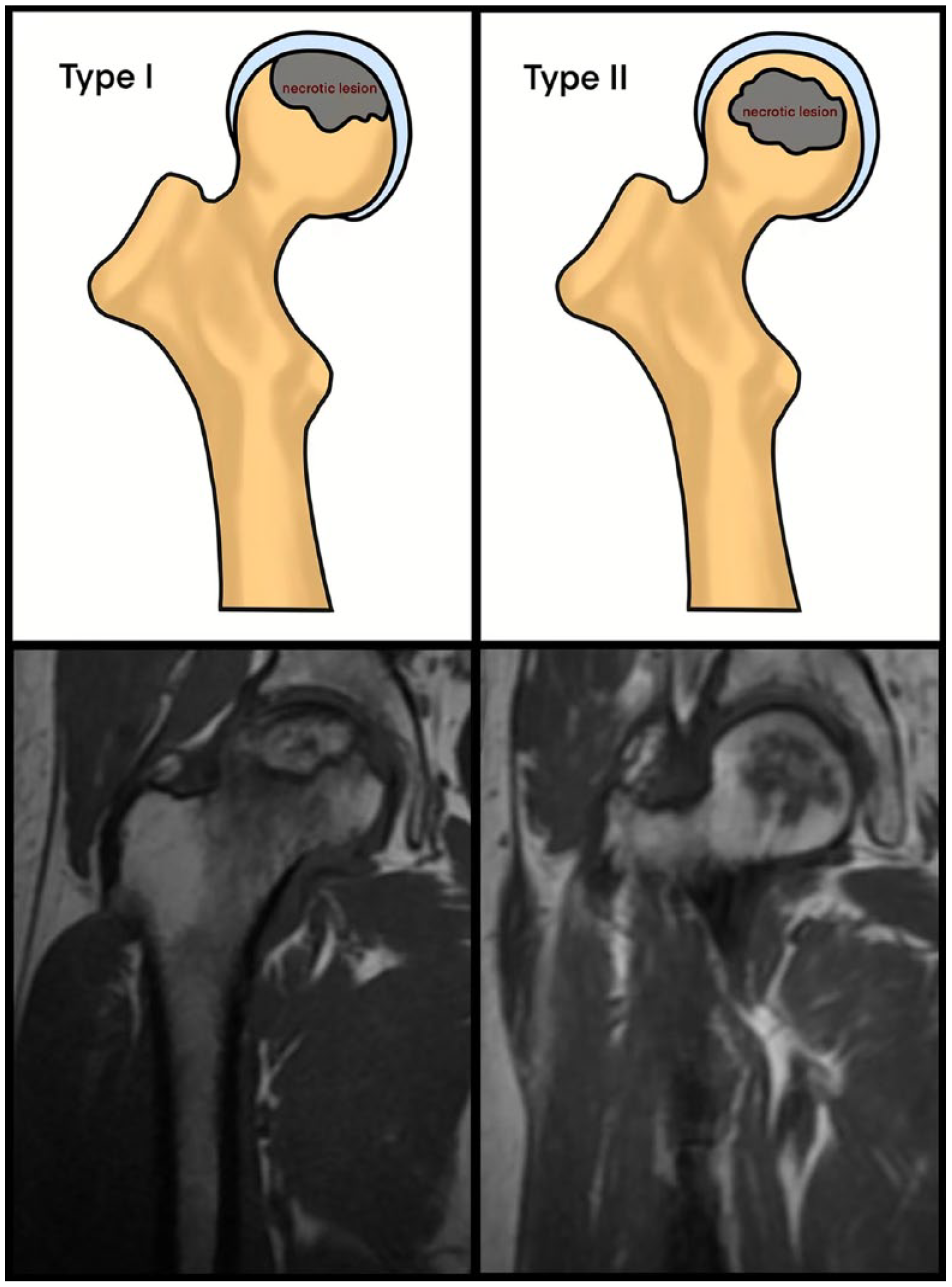
The new classification of osteonecrosis according to the involvement of subchondral bone plate. I: necrotic lesion involving the subchondral bone plate; II: necrotic lesion not involving the subchondral bone plate.
Statistical Analysis
The data were analyzed using the SPSS version 26.0 statistical software (IBM Corp, Armonk, NY). Mean ± standard deviation and frequencies were calculated for all general demographic and routine clinical data.
All hip joints were divided into 2 groups: hip joints that collapsed during the follow-up period (collapse group) and hip joints that did not collapse during the follow-up period (non-collapse group). Univariate logistic regression analysis was performed on clinical variables (independent variables, namely age, BMI, follow-up time, etiology, and imaging type) and femoral head collapse (dependent variable), with significance set at P < 0.05. Eligible variables (P < 0.05, BMI and imaging type) were analyzed by multivariate logistic regression. Forward stepwise regression based on maximum likelihood estimation was used to identify risk factors for collapse. Then, the patients of Type I and Type II were compared, and all continuous variables were tested for normality. After inspection, the age and BMI were in agreement with the normal distribution, and an independent sample t test was adopted. If follow-up time does not conform to normal distribution, a nonparametric test will be used. The χ2 test or Fisher’s exact test was used to classify variables, including gender, etiology, and bilateral lesions. The significance was set at P < 0.05. The collapse rates of Type I and Type II were compared using the χ2 test. Kaplan-Meier survival curve is produced with the occurrence of femoral head collapse as the endpoint. Finally, to determine whether the current classification using subchondral bone plate necrosis would be more sensitive for prediction than the CJFH classification, the accuracy of prognosis prediction was represented by the collapse rate. The χ2 test was used to compare the collapse rates of the 2 classification methods.
Results
In this study, there were 89 hip joint cases. During the follow-up period, 53 cases (59.56%) had a hip joint collapse, whereas 36 cases (40.45%) had no collapse. The average follow-up time was 16.87 months in the collapse group and 13.72 months in the non-collapse group. There was no significant difference between the 2 groups (P = 0.247). Univariate analysis showed that the 2 groups had no significant difference in sex (P = 0.731), age (P = 0.583), and etiology (P = 0.682). Univariate analysis showed that there were significant differences between collapse and non-collapse groups in BMI (P = 0.029) and subchondral bone plate involvement (P < 0.001). Further multivariate analysis showed that BMI (P = 0.01, adjusted odds ratio [OR] = 1.260, 95% confidence interval [CI] : 1.05-1.52) and subchondral plate involvement (P < 0.001, adjusted OR = 69.618, 95% CI: 12.54-386.48) remained closely related to the femoral head collapse ( Tables 2 and 3 ).
Univariate Analysis of 89 Hips With ONFH between Collapse Group and Non-Collapse Group.
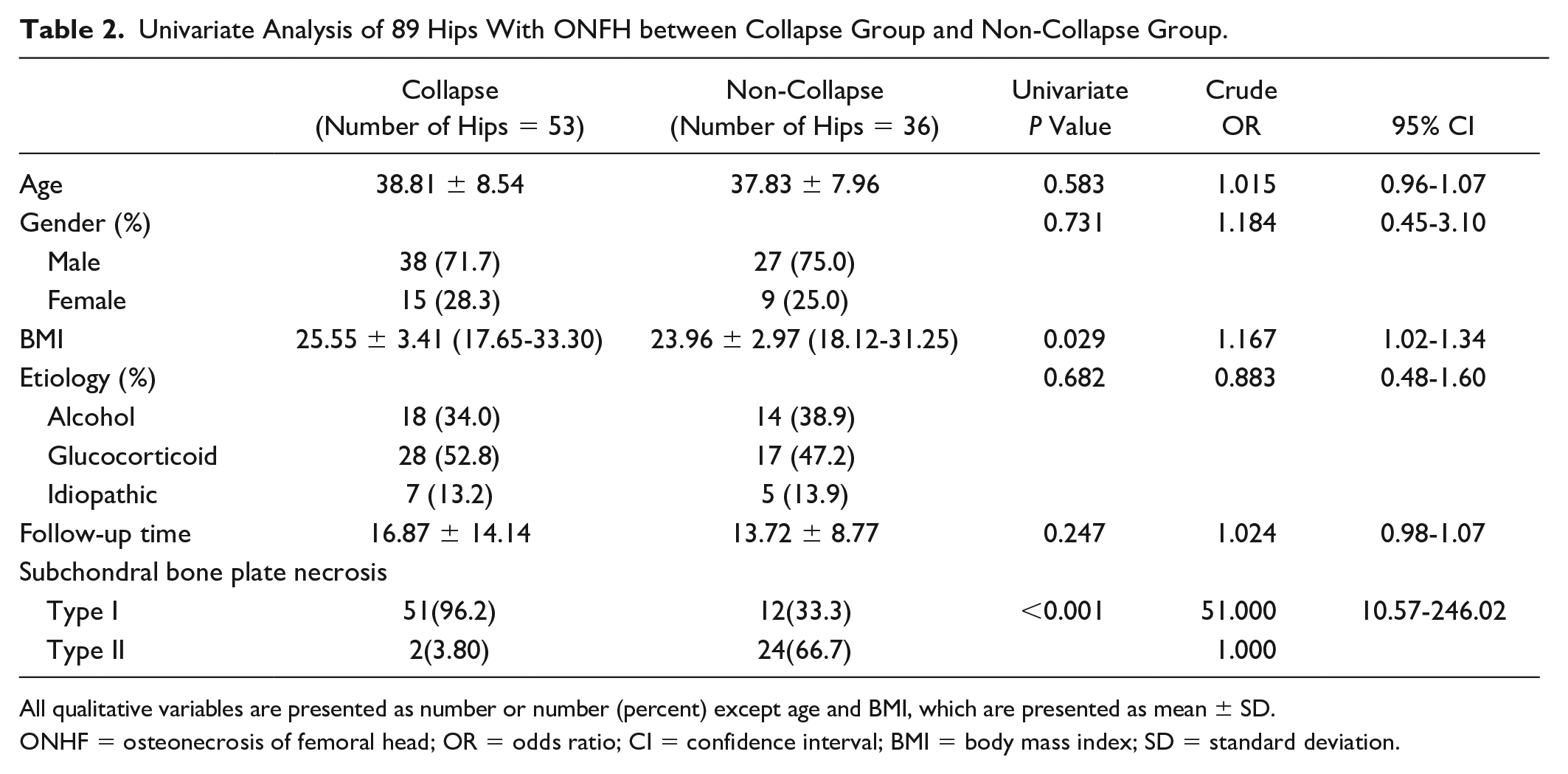
All qualitative variables are presented as number or number (percent) except age and BMI, which are presented as mean ± SD.
ONHF = osteonecrosis of femoral head; OR = odds ratio; CI = confidence interval; BMI = body mass index; SD = standard deviation.
Multivariate Logistic Regression Analysis of Risk Factor.
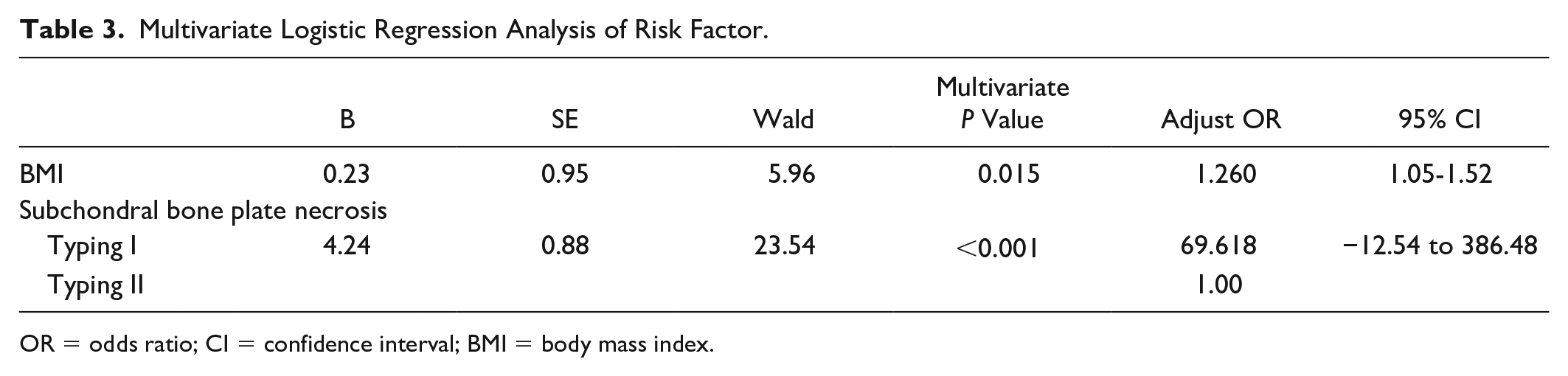
OR = odds ratio; CI = confidence interval; BMI = body mass index.
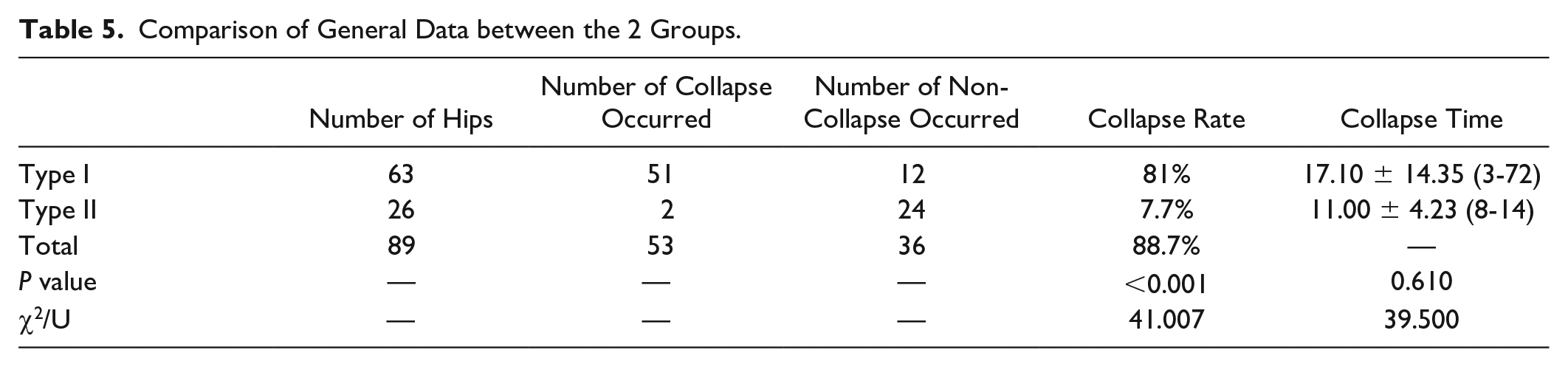
According to the imaging methods mentioned above, the included patients were divided into Type I and Type II groups. The 2 groups had no statistical difference in age, gender, BMI, etiology, bilateral involvement, and follow-up time. However, there was a significant difference in the collapse rate between the 2 groups, 81% for Type I and 7.7% for Type II (P < 0.001, χ2 = 41.00) ( Fig. 2 ), but there were insignificant differences in the collapse time between the 2 groups (P = 0.610) ( Tables 4 and 5 ).
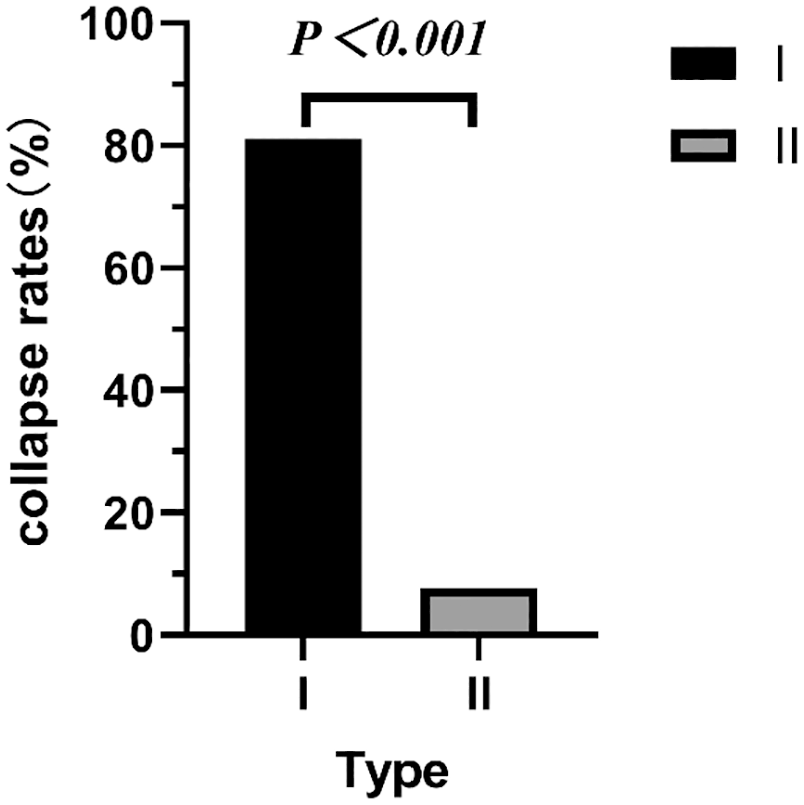
The collapse rates were significant higher in Type I than that in Type II.
Comparison of General Data between the 2 Groups.
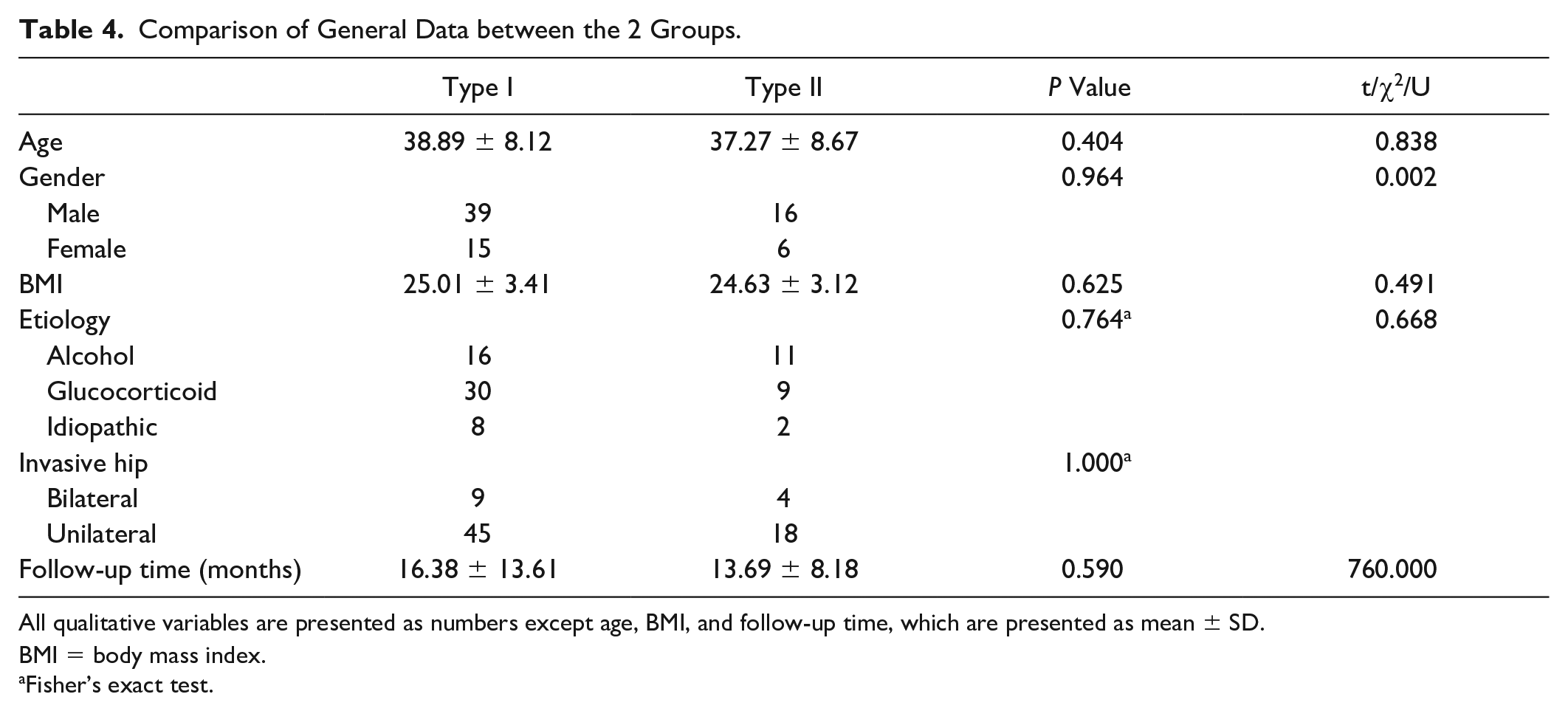
All qualitative variables are presented as numbers except age, BMI, and follow-up time, which are presented as mean ± SD.
BMI = body mass index.
Fisher’s exact test.
Comparison of General Data between the 2 Groups.
In the Type I group, the influence of the involvement of the lateral femoral column on the collapse rate was further analyzed. The results showed that there was no statistical correlation between the lateral column involvement and the collapse rate of the Type I femoral head (P > 0.05) ( Table 6 ).
Relationship between Lateral Column Involvement and Femoral Head Collapse in Type I.
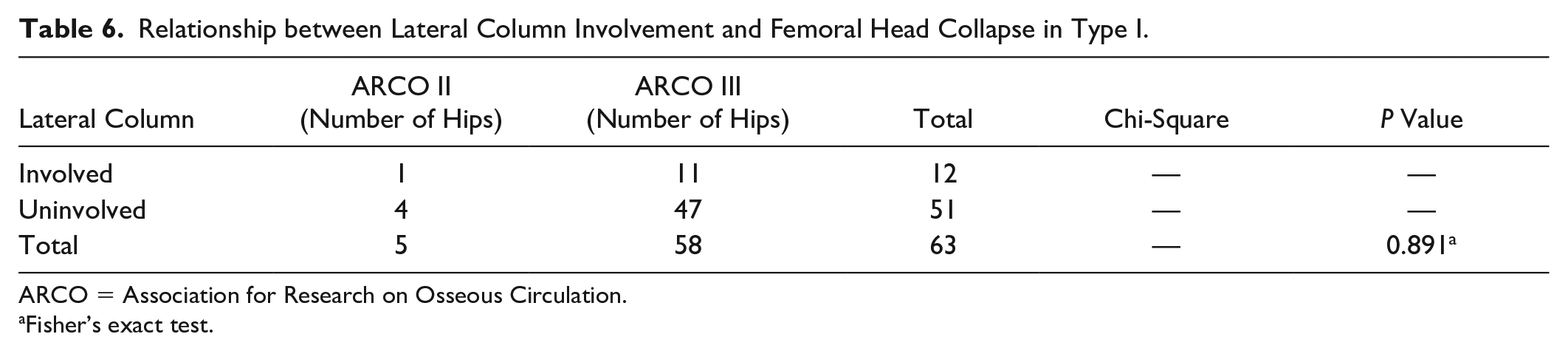
ARCO = Association for Research on Osseous Circulation.
Fisher’s exact test.
Kaplan-Meier survival analysis showed that the survival time of Type I with necrosis involving a subchondral bone plate was significantly shorter than that of Type II without subchondral bone plate involvement (log rank P < 0.001) ( Fig. 3 ).
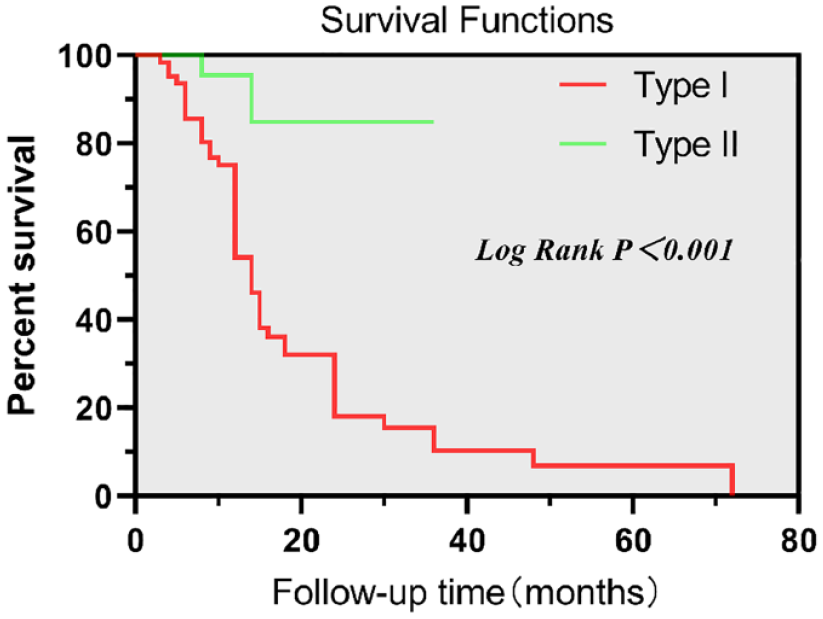
The survival time of Type I was significantly shorter than that of Type II.
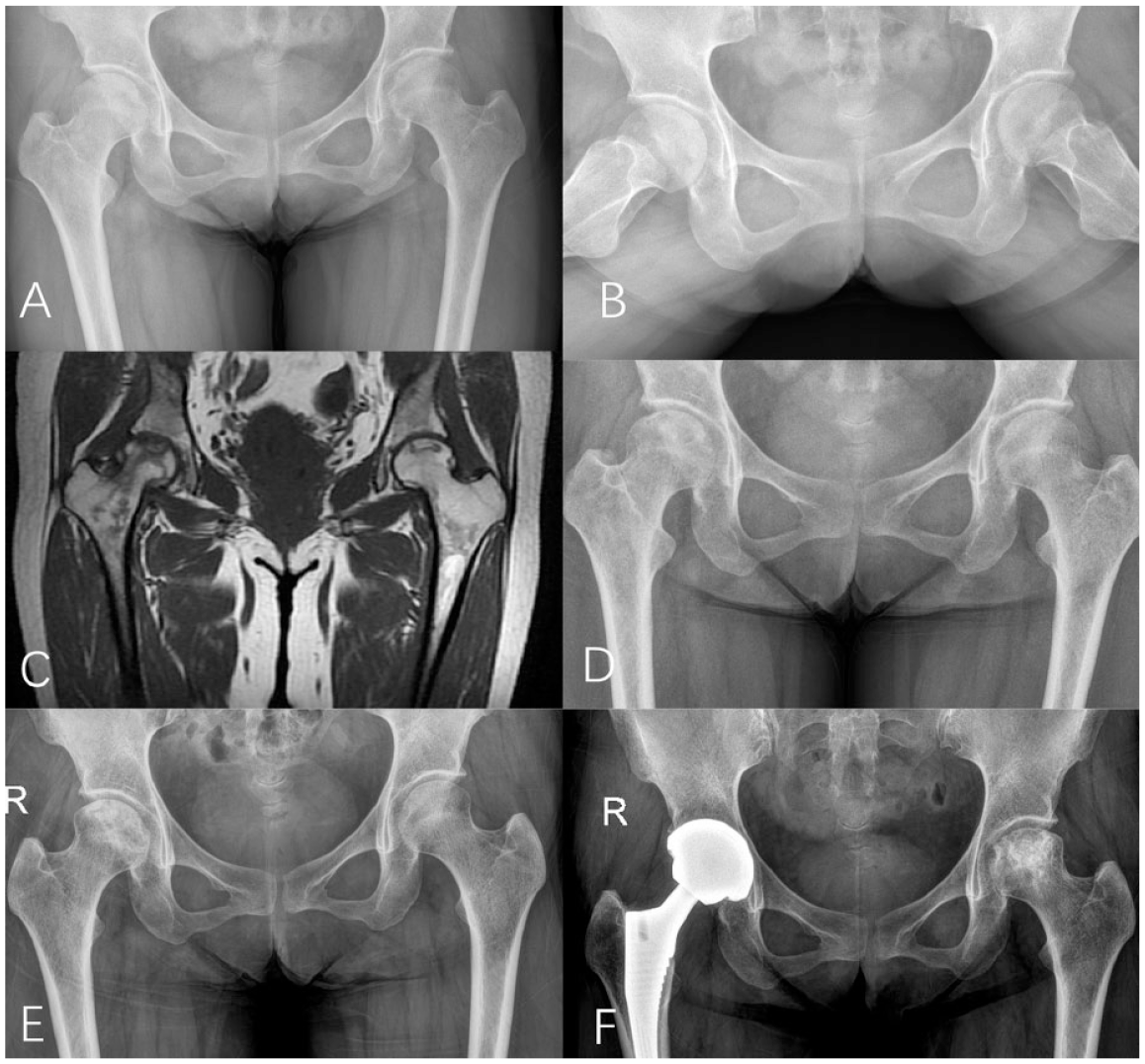
Female, 55 years old, bilateral ONFH, bilateral Type I. At initial diagnosis, anteroposterial and lateral radiographs of both hips showed no collapse of bilateral femoral head (ARCO stage II) (
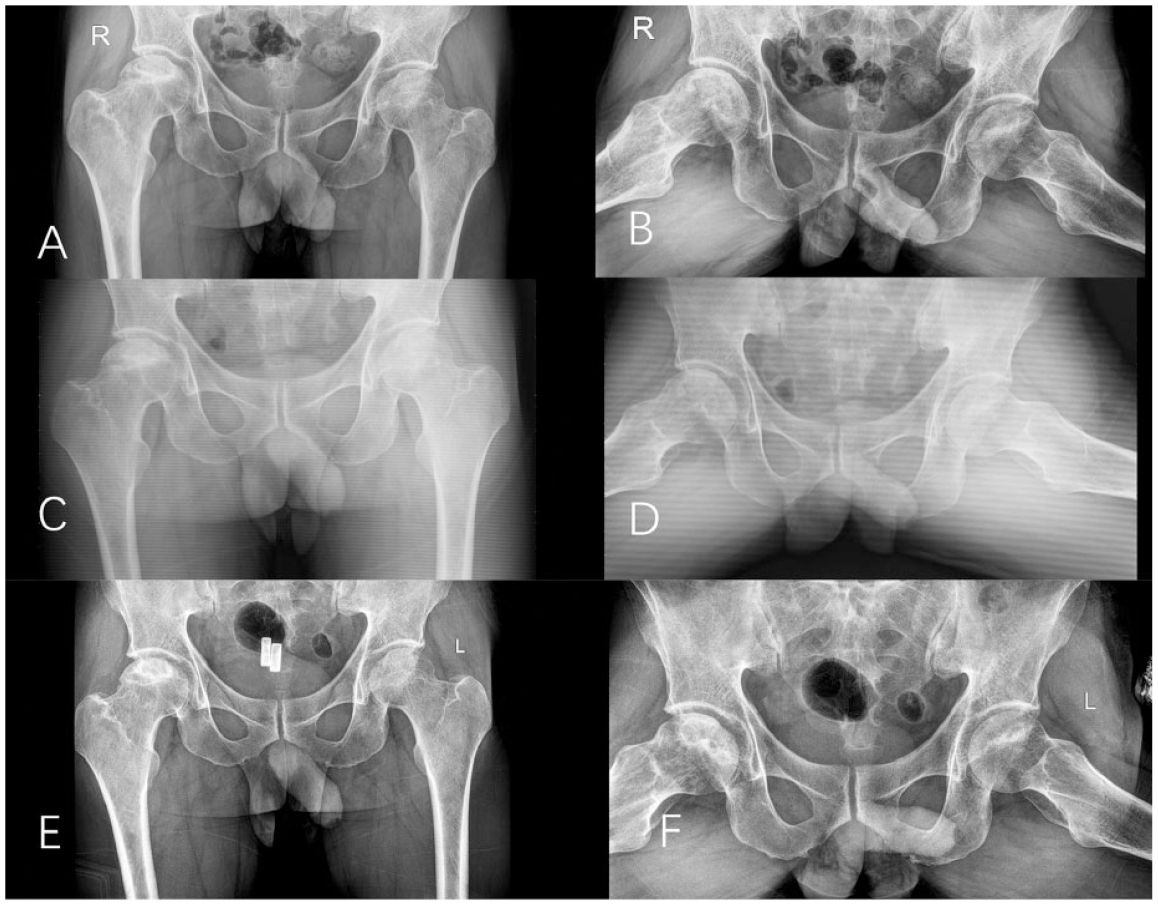
Male, 55 years old, bilateral ONFH, left ARCO I stage, right ARCO stage II, bilateral Type II, no surgical intervention. Conservative treatment was given. At the time of initial diagnosis, anteroposterial-lateral radiographs of both hip joints showed necrosis of the right hip without involving subchondral bone, and the femoral head was intact (
According to the characteristics of the 2 classification methods, types L2 and L3 in the CJFH classification were combined and compared with Type I in the current classification. The collapse rate of Type I in the current classification (80.95%) was higher than that of the combined CJFH classification (63.64%), and the difference was statistically significant (χ2 = 1.776, P = 0.024) ( Table 7 ).
Comparison of Collapse Rate between the Current Classification and CJFH Type.

ARCO = Association for Research on Osseous Circulation.
Discussion
Presently, the prediction of the femoral head collapse is mostly based on imaging, and the risk of collapse is predicted by evaluating the scope and size of the necrotic focus. With the progress of the research on the subchondral bone complex, we found that it plays a vital role in the mechanical support of the whole femoral head after ONFH occurrence. During our clinical treatment, we found that the collapse rate of the femoral head of Type I ONFH (necrosis involving the subchondral plate) was much higher than that of Type II. Our study also confirms our findings.
In the natural course of ONFH without intervention, at least half of the femoral head will collapse,16,17 which is the direct result of the comprehensive effects of the biological and biomechanical characteristics of the necrotic femoral head in the repair stage. 18 Kenzora and Glimcher 19 believed that the subchondral bone plate plays a vital role in keeping the femoral head from collapsing after necrosis, and once a subchondral fracture occurs, collapse and subsequent degenerative arthritis is usually inevitable. The separation from necrotic bone tissue after subchondral fracture is so-called “the ubiquitous crescent sign” on x-ray. 3 Motomura et al. 20 believed that in the biomechanical weak points at the junction between necrotic and surrounding normal bone tissues, including subchondral bone plate, collapse usually occurs first in these areas.
In this study, we compared the ability of the new classification (whether necrosis involves subchondral bone) and our previously proposed CJFH classification to predict the collapse of the femoral head. The results of the retrospective analysis showed that the subchondral plate involved in necrosis was more sensitive in predicting the femoral head collapse (P = 0.024). The good biomechanical properties of the subchondral bone play an essential role in maintaining the femoral head morphology. The surface of the subchondral bone plate is irregular, and the cartilage tissue is fixed on the irregular surface of the underlying subchondral bone plate, similar to a jigsaw puzzle. 21 This allows the conversion of shear forces during compression and traction. Normal cartilage can withstand the deformation caused by the load due to walking about 2.5 times as much as walking. This is due to the presence of the subchondral bone: Normal subchondral bone reduces the load through the joint by approximately 30%. 22 According to Radin et al. and Pugh et al., the subchondral bone absorbs most of the mechanical force transmitted by the hip joint.23,24 The subchondral bone plate is composed of rod-like and plate-like trabeculae in an appropriate proportion, supporting and dispersing stress. 25 Inoue claimed that the structure of the subchondral bone is compatible with its damping function under mechanical stress. 26 The decrease in the mechanical properties of the subchondral bone in weight-bearing areas is directly related to the femoral head osteonecrosis collapse. Some scholars have proposed that the microfractures in the necrotic subchondral bone will not heal and may accumulate, resulting in obvious fractures and subsequent collapse, and microfractures may also occur in the areas around osteonecrosis. 27 Bone changes (hardening or absorption) may change the stress distribution conducive for the development and spreading of microfractures.
In this study, it was found that there was no significant difference in the collapse rate of the femoral head between the patients with an involvement of the lateral column of the femoral head and those with a non-lateral column involvement in the Type I patients with necrosis involving the subchondral bone plate. According to the previous research on osteonecrosis in our center and the CJFH classification based on the 3-column theory, the involvement of the lateral column is more likely to cause the collapse of the femoral head. This is not contradictory to the fact that the femoral head involved in the subchondral bone plate is more likely to collapse and that both of them are independent risk factors for the collapse of the femoral head caused by ONFH. The stress distribution of the lateral column is more concentrated in the negative weight position, and the insufficient support causes collapse after necrosis. Simultaneously, the anterolateral side is the most common site of ONFH, which explains why the lateral column is involved and prone to collapse.
After ONFH, if the necrosis does not occur directly in the subchondral bone area, but occur in the center of the femoral head, the entire mechanical support structure of the femoral head remains intact. Simultaneously, if timely conservative treatment is adopted, the blood supply of the necrotic area can be reconstructed, the lesions can be prevented from further expansion and development, and a very satisfactory therapeutic effect can be obtained. However, once necrosis involves the subchondral bone area, the blood supply of the subchondral bone complex is interrupted, and the structure of the subchondral bone complex is complex. Presently, there is no ideal treatment method to restore the biological integrity of subchondral bone, and the femoral head collapse is inevitable because the femoral head loses its complete mechanical support structure.
In addition, in our study, we found the influence of BMI on femoral head collapse. Some scholars believe that the femoral head collapse rate of ONFH patients with a BMI greater than 25 is significantly increased. 28 In our study, through receiver operating characteristic curve analysis, we found that a BMI greater than 24.68 is a risk factor for femoral head collapse. Combined with clinical practice, the bilateral hip joints of patients with high BMI are bound to bear more weight, the stress acting on the necrotic femoral head is bound to be greater, and the femoral head is more likely to collapse.
We admit that our research has several limitations. First, our research was a single-center retrospective study, and the sample size is relatively small, but the study was conducted through rigorous sample inclusion, exclusion, follow-up, and data analysis. Our findings confirm that retrospective studies can also yield meaningful conclusions. Second, our average follow-up time was relatively short, but significant statistical differences were observed. We would embark on a multicenter, large-scale, prospective study to confirm our findings.
Conclusion
The collapse rate of the femoral head of ONFH with subchondral bone plate involvement is significantly higher than that without involvement. In addition, the current classification using subchondral bone plate necrosis is more sensitive for predicting collapse than the CJFH classification. Therefore, in our clinical diagnosis and treatment, for type I patients with subchondral bone plate involvement, we can surgically reconstruct the subchondral bone plate of the femoral head or replace its spherical mechanical support structure, for example, osteochondral transplantation technology, stem cell transplantation technology and even partial femoral head replacement technology. To achieve the purpose of restoring function and preventing further development of ONFH. For type II patients, conservative treatment can achieve satisfactory results to some extent, such as weight-free therapy, extracorporeal shock wave, local microvascular perfusion, and core decompression techniques. Simultaneously, we need more basic research on the subchondral bone plate and explore new treatment methods to delay subchondral bone plate necrosis or even reconstruct the subchondral bone plate structure.
Footnotes
Acknowledgment and Funding
Thanks very much to Professor Qin Ling for his guidance and revision of the article in his busy schedule. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grants from Fundamental Research Funds for the Central Universities (3332021088), Elite Medical Professionals project of China-Japan Friendship Hospital (NO.ZRJY2021-TD01) Education and teaching reform project of capital Medical University (2023JYY388).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of CJFH (2022-KY-057).
Informed Consent
Informed consent was obtained from the individual participant included in the study.