
Abstract
Objective
To evaluate the efficacy of fibroblast growth factor-18 (FGF-18) augmentation for improving articular cartilage healing following surgical repair in preclinical (in vivo) animal models.
Design
A systematic review was performed evaluating the efficacy of FGF-18 augmentation with cartilage surgery compared with cartilage surgery without FGF-18 augmentation in living animal models. Eligible intervention groups were FGF-18 treatment in conjunction with orthopedic procedures, including microfracture, osteochondral auto/allograft transplantation, and cellular-based repair. Outcome variables were: International Cartilage Repair Society (ICRS) score, modified O’Driscoll histology score, tissue infill score, qualitative histology, and adverse events. Descriptive statistics were recorded and summarized for each included study.
Results
In total, 493 studies were identified and 4 studies were included in the final analysis. All studies were randomized controlled trials evaluating in vivo use of recombinant human FGF-18 (rhFGF-18). Animal models included ovine (n = 3) and equine (n = 1), with rhFGF-18 use following microfracture (n = 3) or osteochondral defect repair (n = 1). The rhFGF-18 was delivered via intra-articular injection (n = 2), collagen membrane scaffold (n = 1), or both (n = 1). All studies reported significant, positive improvements in cartilage defect repair with rhFGF-18 compared with controls based on ICRS score (n = 4), modified O’Driscoll score (n = 4), tissue infill (n = 3), and expression of collagen type II (n = 4) (P < 0.05). No adverse events were reported with the intra-articular administration of this growth factor, indicating short-term safety and efficacy of rhFGF-18 in vivo.
Conclusion
This systematic review provides evidence that rhFGF-18 significantly improves cartilage healing at 6 months postoperatively following microfracture or osteochondral defect repair in preclinical randomized controlled trials.
Introduction
Articular cartilage has limited repair potential, and focal chondral lesions constitute a challenge for current standard clinical procedures. Current cartilage restoration procedures are varied and include marrow stimulation techniques, osteochondral transplants, cellular-based repair, and synthetic or biological scaffolds.1 -3 Despite technological advancements in cartilage restoration procedures, many shortcomings exist, and many ultimately do not provide long-term benefit. Many of these procedures can benefit from improvement, including enhancement of integration of repair tissue with the chondral defect site.4,5
The main problem in defect repair, such as osteochondral allograft transplantation (OCA), is cartilage-cartilage integration of the defect wall. Various growth factors (e.g., fibroblast growth factor 18 [FGF-18], bone morphogenic protein, transforming growth factor β) have been suggested for use as augmentative therapies for enhancing cartilage and bone regeneration in orthopedic procedures.5 -10 One of the growth factors with well-known anabolic effects on cartilage is FGF-18, which is a member of the fibroblast growth factor family and has shown to play a central role in skeletogenesis. Prior studies have demonstrated the capacity of FGF-18 to increase collagen type II and reduce collagen type II breakdown following cartilage injury.11 -13
In vitro studies investigating FGF-18 have demonstrated increased chondrocyte proliferation, increased proteoglycan and collagen synthesis, increased cartilage phenotype preservation, and enhanced cartilage thickness.14 -17 Sennett et al. 10 demonstrated proof-of-concept using recombinant human FGF-18 (rhFGF-18) as an augmentation to enhance cartilage-cartilage integration in an in vitro osteochondral autograft model. However, the reported efficacy of FGF-18 for improving cartilage regeneration in vivo as an augmentative therapy to cartilage repair surgery is less known and more important regarding clinical translation to humans. Therefore, the purpose of this study was to perform a systematic review evaluating the efficacy of FGF-18 augmentation for improving articular cartilage healing following surgical repair in preclinical (in vivo) animal models. It was hypothesized that surgical repair augmented with FGF-18 would result in significantly improved articular cartilage healing compared with surgical repair without FGF-18 augmentation.
Methods
Study Identification and Selection
A systematic review evaluating the efficacy of FGF-18 in improving articular cartilage healing following surgery compared with surgery without augmentation was performed using the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, PubMed (2000-2021), Medline (2000-2021), and Embase (2000-2021); the queries were performed in August 2021. The study protocol was registered with the International Prospective Register of Systemic Reviews (PROSPERO) (CRD42021274671). A series of keyword combinations (Medical Subject Headings [MeSH]) were used: “FGF-18,” “rhFGF18,” “Sprifermin,” and “cartilage regeneration.”
Inclusion criteria consisted of English language studies and in vivo preclinical studies using FGF-18 in conjunction with cartilage repair surgery with specific outcomes of chondrogenesis and collagen synthesis. Eligible intervention groups were FGF-18 treatment in conjunction with orthopedic procedures, including microfracture, osteochondral auto/allograft transplantation, and cellular-based repair. Inclusion criteria for control groups were surgically treated models without FGF-18 augmentation. Exclusion criteria for control groups were all other control conditions (e.g., no treatment, nonsurgical models, or surgical interventions with other active biological growth factors).
Exclusion criteria for the screening of studies were the use of FGF-18 specific to non-musculoskeletal-related conditions, in vitro or ex vivo study designs, non-cartilage conditions, nonsurgical models, human studies, clinical trials, studies using FGF-18 in spinal disorders, the effect of FGF-18 on mesenchymal stem cells, genetic studies, embryonic developmental studies, epidemiology studies, editorials, review articles, case reports (Level V evidence), and studies published before the year 2000. In addition, diseased models such as surgically induced posttraumatic osteoarthritis or osteopenia were excluded to isolate the direct effects of FGF-18 on improving cartilage healing for focal chondral defects. Reference lists from the included studies were reviewed and reconciled to verify that all eligible articles were considered. Two authors (N.N.D. and Z.S.A.) independently reviewed all eligible studies using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18
Quality and Risk-of-Bias Assessment
A risk-of-bias assessment was performed on all included preclinical studies. The quality of included preclinical studies was assessed using SYRCLE’s risk-of-bias assessment tool. 19 This risk-of-bias tool for animal studies contains 10 entries related to selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. Following the SYRCLE guidelines, a “yes” judgment indicated a low risk of bias, a “no” judgment indicated a high risk of bias, and a judgment was “unclear” if insufficient details have been reported to assess the risk of bias properly. No summary score for risk of bias was calculated per the SYRCLE guidelines. All studies were scored by 1 author (initials blinded for review), and when applicable, discrepancies were resolved by consensus of 2 additional authors (initials blinded for review).
Data Collection and Statistical Analysis
Data involving preclinical studies were collected and extracted from each included study. The main outcomes of interest were related to chondrogenesis, collagen synthesis, animal functional outcome scores, and radiographic outcomes. Specifically, the primary outcome variables were the International Cartilage Repair Society (ICRS) score, the modified O’Driscoll histology score, tissue infill score, and quantitative and qualitative histology (collagen staining). Secondary outcome variables were mechanical properties (e.g., stiffness of cartilage), functional outcomes (e.g., weightbearing, lameness), and adverse events. Other variables of interest extracted from each included study were experimental focus, animal model type, route of administration, and dosage (including frequency and duration). Descriptive statistics were recorded and summarized for each study. When applicable, continuous numerical data were grouped for comparison and reported as mean and range.
Results
Study Characteristics
A total of 493 studies were identified, and after application of the exclusion criteria, 4 studies were included in the final analysis (
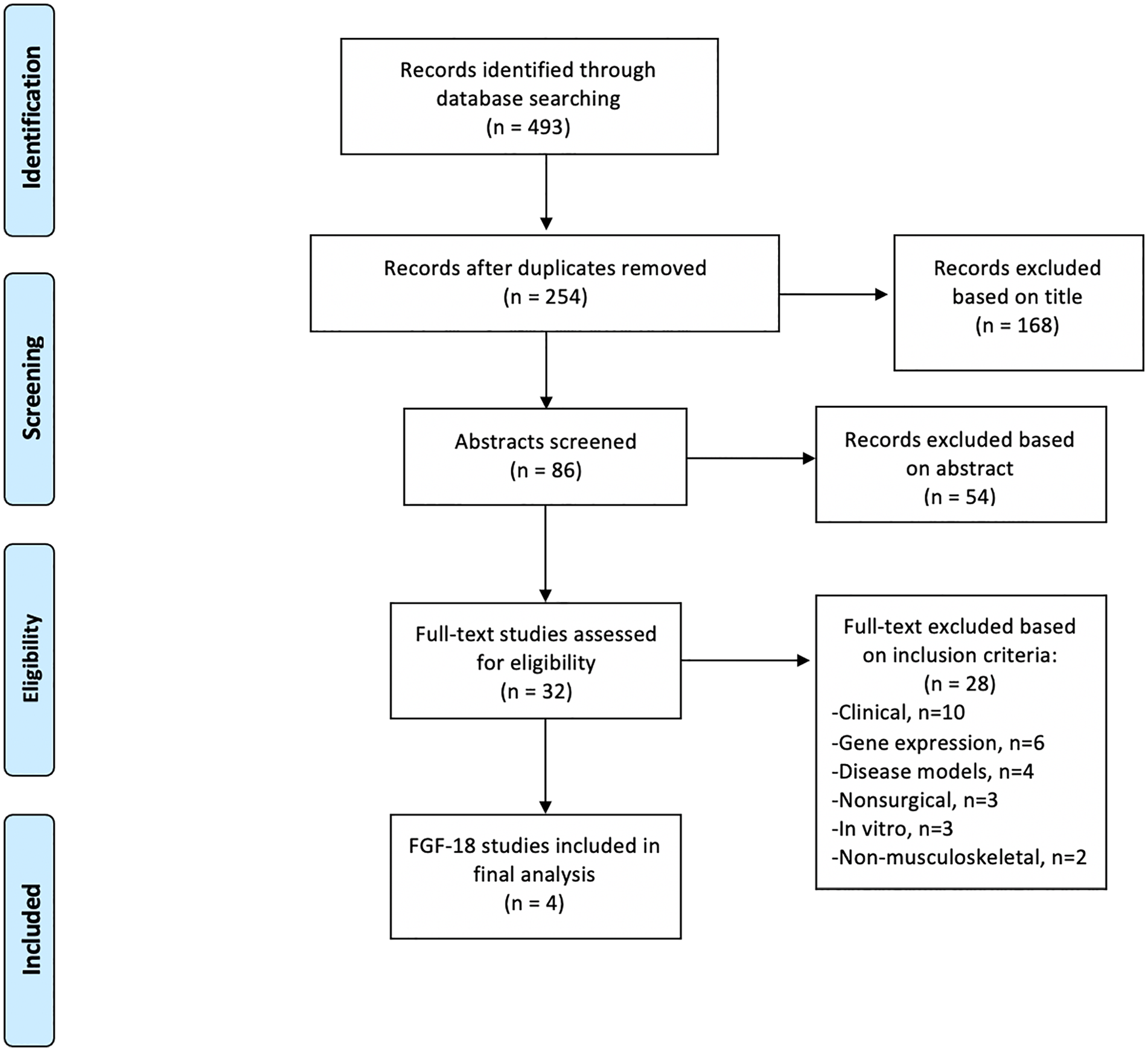
PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guidelines showing the application of selection criteria to the studies identified with the search strategy.
Study Characteristics for Preclinical Use of FGF-18 for Cartilage Defect Repair (n = 4).
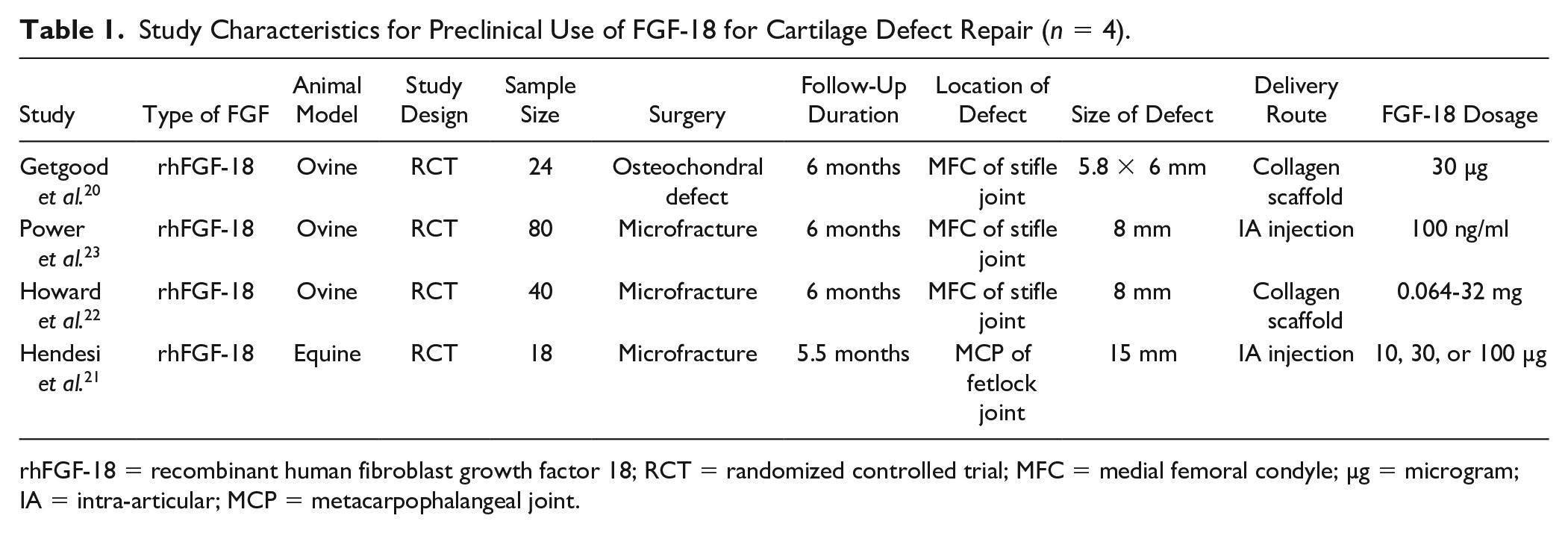
rhFGF-18 = recombinant human fibroblast growth factor 18; RCT = randomized controlled trial; MFC = medial femoral condyle; µg = microgram; IA = intra-articular; MCP = metacarpophalangeal joint.
Experimental Design
All studies reported randomized designs with total follow-up ranging from 5.5 to 6 months following interventions. There was heterogeneity among the experimental groups and protocols utilized across studies, including type of comparative groups and dosage regimens of rhFGF-18 (
Experimental Treatment Groups for Randomized Controlled Trials Using rhFGF-18.
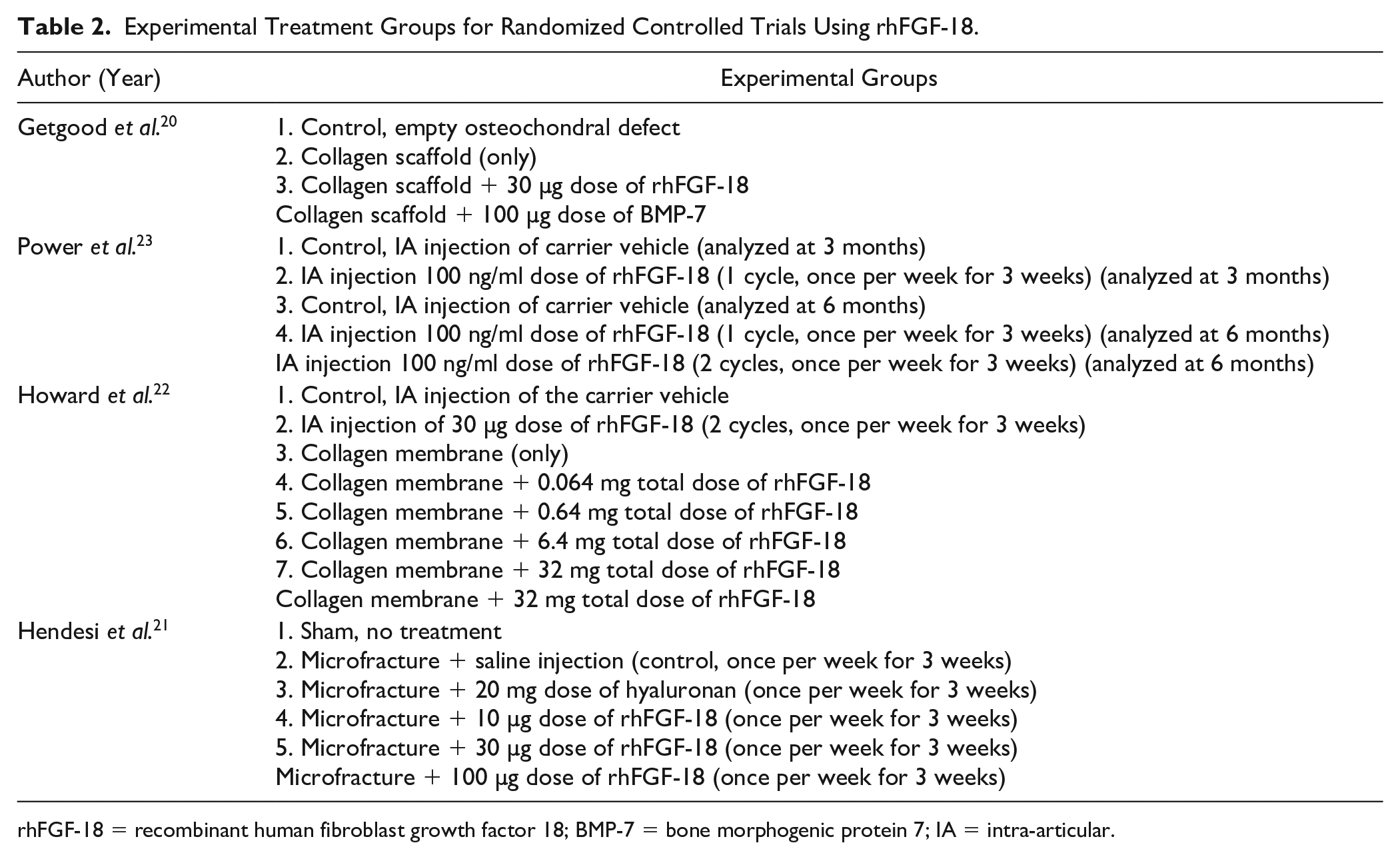
rhFGF-18 = recombinant human fibroblast growth factor 18; BMP-7 = bone morphogenic protein 7; IA = intra-articular.
Preclinical Efficacy
All 4 studies reported significant, positive improvements in cartilage defect repair with rhFGF-18 compared with controls based on a combination of the ICRS score, modified O’Driscoll score, tissue infill, and expression of collagen type II (P < 0.05) (
Outcome Metrics for Preclinical Efficacy of rhFGF-18 versus Control Following Cartilage Repair.
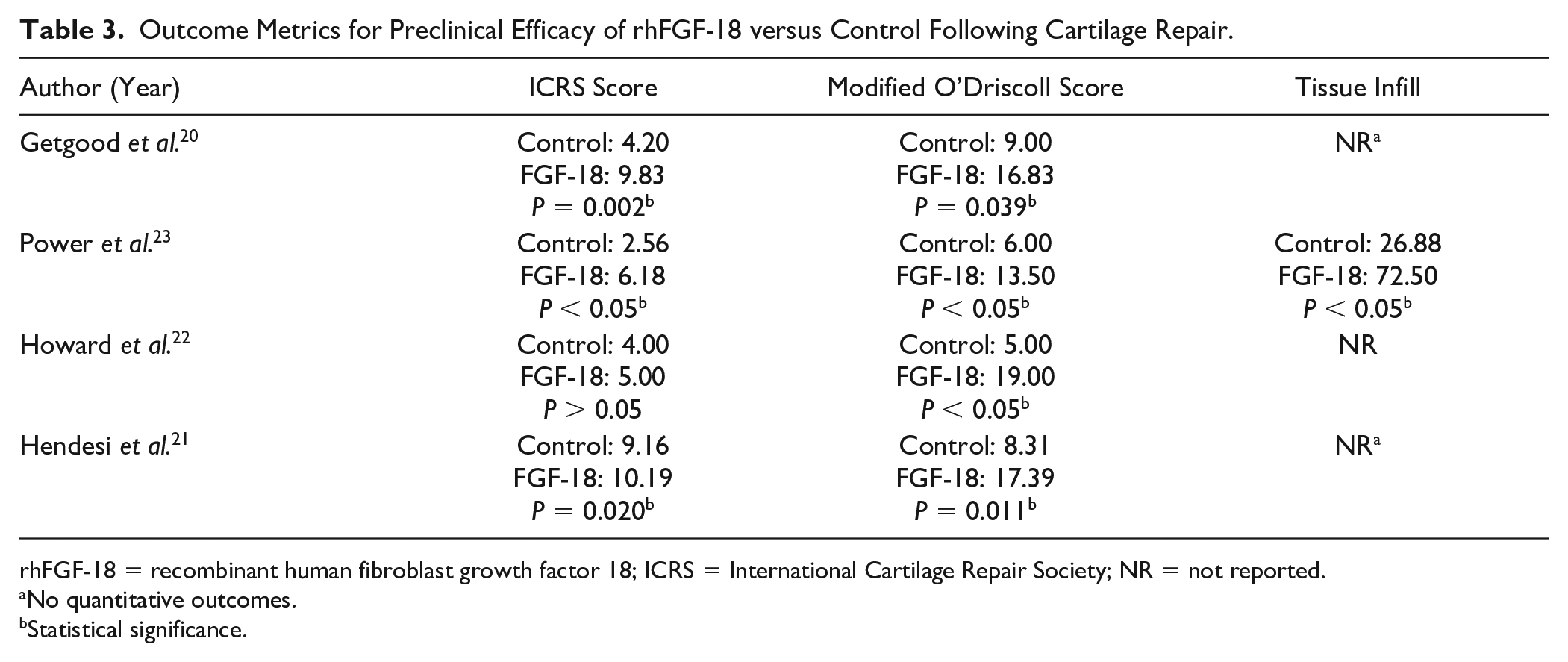
rhFGF-18 = recombinant human fibroblast growth factor 18; ICRS = International Cartilage Repair Society; NR = not reported.
No quantitative outcomes.
Statistical significance.
Regarding gene expression of collagen type II, only 1 study quantified gene expression with real-time polymerase chain reaction; there was no significant increase in average collagen type II expression (housekeeping genes (HKGs)) with 100 µg of rhFGF-18 compared with controls (4,885 vs. 3,031 %HKGs, P < 0.05). 21 However, this study did demonstrate an increase in average collagen type II expression in 5 out of 6 animals (while not significant). Based on immunohistochemistry staining, 3 studies reported that the repair tissue with rhFGF-18 was strongly stained for collagen type II, indicating a mature hyaline-like cartilage repair tissue had been produced.20,22,23
Three studies reported on mechanical testing following treatments to determine changes to the cartilage surface surrounding the chondral defect area. No significant differences in mean cartilage stiffness were found between rhFGF-18 and controls.20,22,23 One study evaluated peak vertical force on the operative limb using force plate analysis and found that animals that had received rhFGF-18 had increased weightbearing at 2 and 4 weeks postoperatively compared with controls (P < 0.05) and had returned to preoperative levels of weightbearing by 8 weeks postoperatively. 22 In addition, in the equine model, authors reported significant improvements in lameness scores in rhFGF-18 groups compared with controls (P < 0.05). 21
Complications and Dosage
There were no major adverse events reported with the administration of intra-articular rhFGF-18 across all 4 studies.20 -23 Adverse events were considered osteophyte formation or joint degeneration in all studies. Synovial fluid analysis was performed in 2 studies. Hendesi et al. 21 found no effect of rhFGF-18 on total synovial fluid white cell counts or total protein. Howard et al. 22 reported that no rhFGF-18 was detected in the synovial fluid after week 1, and no rhFGF-18 was detected in the serum at any time point, indicating no systemic effects and that rhFGF-18 was retained in the joint.
The most common reported dosages of rhFGF-18 were 30 and 100 µg, with experimental dosages ranging from 0.064 to 100 µg. The most common frequency of intra-articular administration of rhFGF-18 was once per week for 3 consecutive weeks. Regarding dose-dependent benefits, significant increases in cartilage healing were detected with 6.4, 30, 32, and 100 µg of rhFGF-18 (compared with controls, P < 0.05).20 -23 Hendesi et al. 21 reported a concentration-dependent benefit in rhFGF-18 treatment, with the highest benefit in 100 µg dose. However, no single dose of rhFGF-18 showed a statistically significant advantage over control (microfracture + saline). 21
Overall, the quality of the included animal studies was high, with a relatively low risk of bias. A summary of the risk-of-bias assessment is provided in
SYRCLE’s Tool for Assessing Risk of Bias of Preclinical Animal Studies Using rhFGF-18.
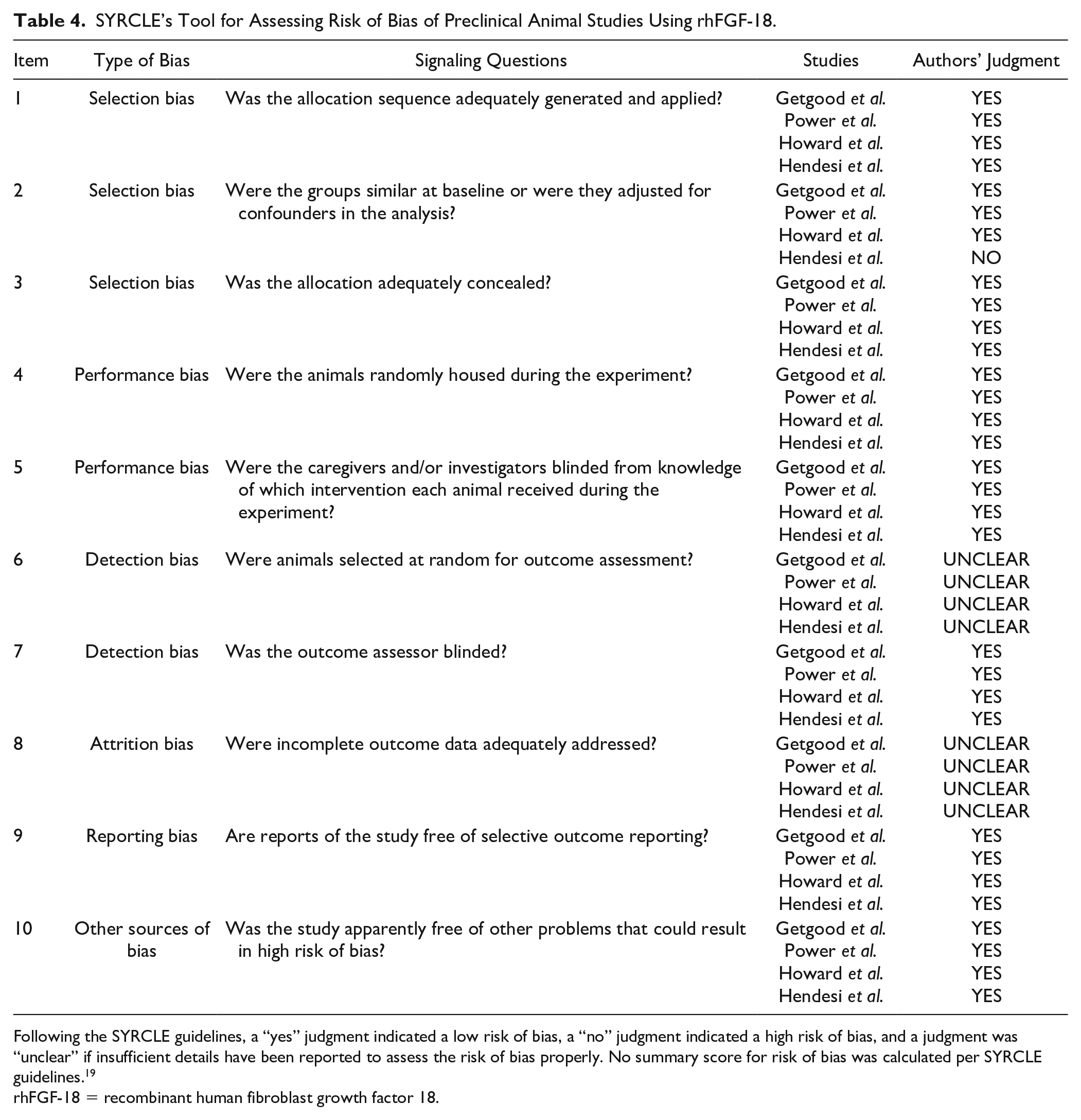
Following the SYRCLE guidelines, a “yes” judgment indicated a low risk of bias, a “no” judgment indicated a high risk of bias, and a judgment was “unclear” if insufficient details have been reported to assess the risk of bias properly. No summary score for risk of bias was calculated per SYRCLE guidelines. 19
rhFGF-18 = recombinant human fibroblast growth factor 18.
Discussion
The main finding of this systematic review was that the augment of rhFGF-18 to cartilage repair procedures demonstrated significant, positive improvements in cartilage regeneration compared with controls in preclinical, large animal models. Importantly, no adverse events were reported with the intra-articular administration of this growth factor at doses and timeframes evaluated; therefore, no safety concerns were determined. Although a limited number of preclinical studies were available, collectively these results suggest strong potential clinical translation of rhFGF-18 as an augment to enhance articular cartilage repair procedures.
In the present review of preclinical large animal models, applying rhFGF-18 in conjunction with either microfracture or osteochondral defect repair resulted in significantly improved quality and quantity of repair tissue at 6 months postoperatively compared with controls. These findings are consistent with other in vitro and ex vivo studies that suggest an anabolic role for rhFGF-18 in cartilage healing and homeostasis.10,15 All 4 studies reported no adverse events with intra-articular administration of rhFGF-18, which is similar to human clinical trials that have demonstrated that rhFGF-18 is safe when treating patients with osteoarthritis.24 -26 Despite the observation of concentration-dependent benefits with rhFGF-18 reported within the studies of this review, the ultimate best dosage of rhFGF-18 for long-term benefit cannot be determined from these preclinical data. Additional long-term studies are needed to further evaluate the safety, efficacy, and sufficient dosage regimen for augmenting cartilage defect repair with rhFGF-18.
The majority of prior research and development of rhFGF-18 has focused on its use in treating patients with osteoarthritis. Sprifermin, a truncated version of rhFGF-18, has shown meaningful promise through phase II clinical trials as a potential disease-modifying osteoarthritis therapeutic; however, sprifermin is not yet Food and Drug Administration–approved as a pharmaceutical drug for human use.27,28 In in vitro and in vivo studies, sprifermin has shown to promote the proliferation of articular chondrocytes, promote synthesis of extracellular matrix, increase cartilage thickness in a dose-dependent manner, and also inhibit the activity of proteolytic enzymes and slow down the degeneration of cartilage.7,11,13,25 Preclinical results of this systematic review offer a unique perspective of using rhFGF-18 as an augmentative therapy to existing cartilage repair procedures which may allow for accelerated and complete cartilage integration. Despite the unique advantages of using rhFGF-18 in repairing cartilage injury and restoring cartilage homeostasis, further clinical trials are needed to further elucidate the safety and efficacy of rhFGF-18 as an augment to cartilage repair surgery for focal chondral defects.
Despite all 4 studies reporting significant, positive improvements in cartilage repair with rhFGF-18, there are limitations of traditional drug delivery methods for joint disease, which may pose a major therapeutic challenge when translating drug injectables from preclinical to clinical use.20 -23 Specifically, and inherent to all intra-articular injectables, the unique environment of musculoskeletal joints limits drug efficacy due to passive release of medications, rapid joint clearance, and lack of targeting specific tissues inside the joint.29,30 To overcome this problem, controlled drug delivery systems that can increase the residence time of medications inside the joint and allow for site-specific drug targeting have been developed.31 -33 In this current review, Getgood et al. 20 used a biphasic collagen scaffold containing rhFGF-18 to allow the growth factor to remain within the cartilage lesion to optimize its effect on chondrocytes and cartilage defect repair. Similarly, Howard et al. 22 reported that rhFGF-18 delivered via a collagen membrane is more likely to retain the growth factor locally, providing sustained release of the drug. While promising and perhaps favorable over traditional intra-articular injection, further translational research is needed to evaluate the various types of drug delivery vehicles to improve the efficacy and safety of active biological therapies and growth factors for intra-articular cartilage repair.
This systematic review is not without limitations. There was heterogeneity among studies regarding the dosage and delivery method of rhFGF-18, which may limit the direct comparisons of results. Although a relatively small number of studies were included, this is a result of strict and concise inclusion criteria which allowed for inclusion of high-quality, level I randomized controlled trials. Despite all studies using a randomized design, there were differences in the experimental groups, precise outcome metrics, and reporting of data variability, which did not allow for quantitative synthesis of variables and prevented meta-analysis which could have provided more objective inferences regarding the synthesized data. In addition, there were variations in animal models used (3 ovine, 1 equine) and cartilage repair procedures (3 microfracture, 1 osteochondral defect), which may limit the generalizability of these preclinical results to all cartilage repair procedures.
Conclusion
This systematic review provides evidence that rhFGF-18 significantly improves cartilage healing at 6 months postoperatively following microfracture or osteochondral defect repair in preclinical randomized controlled trials. The collective findings suggest that the benefit of rhFGF-18 as an augmentative therapy to existing surgical procedures may allow for accelerated and complete cartilage integration. The in vivo safety and efficacy of rhFGF-18 in preclinical studies warrant further nonhuman research to fully explore the clinical translational potential of this unique growth factor as an augment to improve cartilage repair.
Footnotes
Authors’ Note
Investigation was performed at University of Pennsylvania, Philadelphia, PA, USA
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review project (#21-210) was in part supported by a grant from the ON Foundation, Switzerland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not Applicable.