
Abstract
Objective
To characterize the effects of parathyroid hormone (PTH) and alendronate (Alend) on the osteochondral tissue of temporomandibular joint (TMJ).
Materials and Methods
Ninety-six male and female transgenic reporter mice, 4 to 5 weeks old were divided into 6 groups: (1) Control group: Saline was injected daily for 14 days; (2) PTH: PTH was injected daily for 14 days; (3) Alend: Alend was injected every alternate days for 14 days; (4) Combined PTH and Alend: PTH was injected daily and Alend injected every alternate days for 14 days; (5) PTH then Alend: PTH was injected daily for 14 days followed by Alend injections in alternate days for 14 days; and (6) PTH wait Alend: PTH was injected daily for 14 days. There was a waiting period of 1 week before administration of Alend in alternate days for 14 days. Mice were injected with 5-ethnyl-2′-deoxyuridine (EdU), 48 and 24 hours prior to euthanization.
Results
There was significant increase in bone volume and decrease in osteoclastic activity in groups in which Alend was administered after PTH in both gender. There was significant increase in cartilage thickness with PTH or Alend alone in females, whereas in males, PTH alone led to increase in cartilage thickness. Chondrocyte apoptosis was significantly decreased with PTH or Alend alone in both male and female. Matrix metallopeptidase 13, and aggreganase-2 (ADAMTS5) expression were significantly decreased with PTH and Alend alone in both gender.
Conclusion
PTH and Alend administration causes anabolic effects in the osteochondral tissue of TMJ.
Introduction
Temporomandibular joint osteoarthritis (TMJ-OA) is a degenerative joint disease characterized by synovial inflammation, cartilage loss, and sclerosis of the subchondral bone, causing pain and disability.1,2 The Clinical management of TMJ-OA is largely palliative and anti-inflammatory drugs; analgesics and lubricating supplements are primarily used for the treatment of TMJ-OA. Therefore, it is critical to develop and test new therapeutic agents that are anabolic for the TMJ cartilage and subchondral bone. Thus, agents which modify both the cartilage and subchondral bone are promising for TMJ-OA, including parathyroid hormone (PTH) and alendronate. Given the severity of TMJ-OA and the unique nature of the osteochondral tissues of the TMJ, it is not likely that a single therapeutic agent will be able, on its own, to promote or restore the anabolic responses in TMJ-OA. Accordingly, identifying signals that can synergize to produce anabolic functions in the cartilage and subchondral bone are essential for the development of clinically feasible treatments for TMJ-OA.
The cells in the TMJ cartilage expresses Collagen type 1 (Col1a1), Collagen type 2 (Col2a1), and Collagen type 10 (Col10a1). 3 Usually Col2a1 is found in the knee cartilage, 4 and Col1a1 is predominantly expressed in the bone. 5 Col1a1 cells are predominantly located in the proliferative zone of the TMJ cartilage, 6 and Col10a1 cells are located in the hypertrophic zone of the TMJ cartilage.6-9
Intermittent administration of PTH (I-PTH) is a United States Food and Drug Administration (FDA)–approved anabolic treatment for osteoporosis in clinical practice. Our previous data suggest that I-PTH promotes an anabolic effect at the mandibular condyle of mice, and there was significant increase in the cartilage thickness with the I-PTH administration. 10 In fact, I-PTH is commonly used in association with anti-resorptive agent bisphosphonates in the treatment of osteoporosis,11,12 whereas the effects of this treatment modality in TMJ osteoarthritis are largely unknown. Therefore, it is now crucial to determine the effects of this combination in the cartilage and subchondral bone of the TMJ and its underpinning molecular mechanisms.
To the best of our knowledge, there is no study comparing the individual and synergistic effects of the I-PTH and alendronate on the cartilage and the subchondral bone of the TMJ. The purpose of this project was to study whether the use of I-PTH and alendronate together would provide a therapeutic advantage by combining different mechanism and have an anabolic effect on the cartilage and the subchondral bone. Our objective was to determine the effects of I-PTH and alendronate treatment on the microarchitecture of the cartilage and the subchondral bone of the TMJ. In addition, we also studied the effects of independent and simultaneous treatment with I-PTH and alendronate.
Materials and Methods
Ethical Statement
All the experimental protocol used in this research involving triple transgenic reporter mice were reviewed and approved by the Institutional Animal Care Committee of the University of Connecticut Health Center. Our study followed the ARRIVE guidelines for in vivo experiments using these mice.
Triple Transgenic Mice
Ninety-six 4- to 5-week-old male and female triple transgenic reporter mice (Col1a1 × Col2a1 × Col10a1) on a CD-1 background6,13 were used for this study. The Col1a1-GFP cyan contains a 3.6-kb fragment of the rat type 1 collagen promoter that is strongly expressed in bone and the mandibular condylar cartilage (MCC). The Col2a1-CFP contains a 1-kb fragment of the type 2-collagen promoter that is expressed in the pre-hypertrophic zone of the MCC. The Col10a1-RFP is fused to mCherry fluorescent protein and is expressed in the hypertrophic zone of the MCC.
In Vivo Study Design
All the mice received subcutaneous injection of saline or PTH [1-34] (60 μg/kg body weight, Prospec, East Brunswick, NJ, USA) or/and Alendronate (Alend, alendronate sodium trihydrate, 50 μg/kg, Sigma Aldrich, St. Louis, MO).
Mice were divided into 6 groups and equal number of males and female mice were used in each group (n = 8 male and 8 female per group). Groups were divided as described below:
Control group: Saline was injected daily for 14 days;
PTH group: PTH was injected daily for 14 days;
Alendronate (Alend) group: Alendronate was injected every alternate day for 14 days;
Combined PTH and Alend group: PTH was injected daily combined with Alend injected every alternate days for 14 days;
PTH then Alend group: PTH only was injected daily for 14 days followed by Alend only injections in alternate days for another 14 day;
PTH wait Alend group: PTH only was injected daily for 14 days. There was a waiting period of 1 week before initiation of Alend only injections in alternate days for another 14 days (
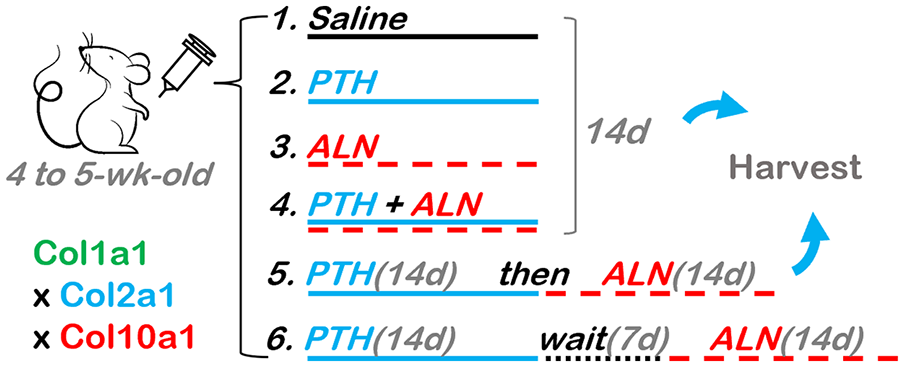
Schematic diagram of the experimental procedure. PTH = parathyroid hormone; Alend = Alendronate.
We used these experimental groups as we wanted to clearly decipher the effects with different combinations of I-PTH and alendronate. Furthermore, we needed to determine how alendronate can be optimally used in conjunction with I-PTH for the anabolic effects. Mice were injected with EdU (5-ethnyl-2′-deoxyuridine, Life Technologies, Grand Island, NY, USA) (30 mg/kg body weight) 48 and 24 hours prior to euthanization. All animals in the control and experimental groups were healthy and gained weight during the entire duration of the study. All mice were euthanized 24 hours after the last injection of EdU.
Tissue Preparation and Histological Sectioning
After euthanasia, the mandibles were dissected by cutting the muscular attachment without removal of the cartilage of the condyle. The MCC along with subchondral bone were fixed in 10% formalin for 24 hours, placed in 30% sucrose in phosphate-buffered saline (PBS) overnight, then embedded in cryomedium (Thermo Shandon, Pittsburgh, PA, USA) using disposable base molds (Thermo Shandon, Pittsburgh, PA, USA). The medial surfaces of the samples were embedded parallel to the floor and against the base of the mold. Specimens were stored at –20°C until sectioning with a Leica cryostat (Nussloch, Germany). Transfer of frozen sagittal sections of the condyles (5-7 μm) to slides was completed with tape transfer method. 14
Micro–computerized tomography (Micro-CT)
The MCC and subchondral bone of condyles were analyzed using micro-CT (SCANCO Medical AG, Brüttisellen, Switzerland) at 55 kV and 145 μA, with a voxel size of 6 μm. The samples (n = 8 per group) were scanned in 70% alcohol, and serial tomographic projections were acquired at 1,000 projections per rotation at 300,000 μs. An automated algorithm using local threshold segmented the reconstructed gray scale images to distinguish calcified tissue from non-calcified tissue (Scanco MicroCT software). The mushroom-shaped condylar head was the region of interest. Bone volume fraction (BVF [%]) was assessed.
Histomorphometry and Histological Staining
Our histological sections were stained and analyzed as previously described. The 5 to 7 μm sagittal sections of mandibular condyles were adhered to glass slides through the entire processes of staining and imaging. The sections were first imaged for fluorescent signals Col1a1 (green) and Col10a1 (red). Baseline imaging of the sections was performed with an observer ZI fluorescent microscope (Carl Zeiss, Thornwood, NY, USA) using a yellow fluorescent protein filter (eYFP, Chroma Cat 49003ET, EX: 500/20, EM: 535/30) and a RFPcherry filter that was also used for detecting alizarin complexone staining (mCherry, Chroma Cat 49009ET, EX: 560/40, EM: 630/75). Subsequently, the coverslip was removed by soaking slides in PBS and stained for EdU (Life Technologies, Grand Island, NY, USA) then imaged. Sections were then stained for tartrate-resistant acid phosphatase (TRAP) using ELF97 (Life Tech, Waltham, MA, USA), generating a yellow fluorescent signal. Finally, the slide was rinsed in distilled water then stained with Toluidine blue (TB) and reimaged using bright field microscopy to examine the proteoglycans.
We also performed fluorescent TUNEL (R&D systems, Minneapolis, MN, USA) as well as immunohistochemistry for degeneration markers, matrix metallopeptidase 13 (MMP13; Abcam, Cambridge, MA, USA), and ADAM metallopeptidase with thrombospondin type 1 motif 5 (ADAMTS5; ThermoFisher).
Histological Analysis and Quantification
ImageJ (National Institutes of Health, Bethesda, MD) was used to quantify green and red pixels within the cartilage of the mandibular condyle to analyze Col1a1 and Col10a1 expression in sagittal sections of condyles. Percentages were obtained by dividing the number of green or red cells over the total number of 4′,6-diamidino-2-phenylindole (DAPI) cells. Similarly, we examined TRAP activity by dividing the area of yellow pixels over the area of the subchondral bone region. EdU and TUNEL were quantified as the ratio of EdU or TUNEL positive cell number to DAPI positive cell in the TMJ cartilage, respectively. The thickness of all layers of cartilage was assessed by averaging the measurements at 5 different locations throughout the middle portion of MCC using TB staining.
Statistical Analysis
Descriptive statistics were used to examine the distribution of BVF, tissue density, and histological analysis. Statistically significant differences among means were determined by 1-way analysis of variance (ANOVA) and Tukey’s multiple comparisons test. All statistical tests were 2 sided, and a P value of <0.05 was deemed to be statistically significant. Statistical analysis was computed using Graph Pad Prism (San Diego, CA, USA).
Results
Bone Volume and Remodeling
We first analyzed bone volume in the MCC and subchondral bone of condyles of experimental and control mice by Micro-CT. All these 3 types of combination uses of PTH and Alend caused a significant increase in bone volume when compared with PTH alone, in both females and males (females: PTH vs. PTH + Alend: P = 0.005; PTH vs. PTH then Alend: P < 0.05; PTH vs. PTH wait Alend: P = 0.05; males: PTH vs. PTH + Alend: P = 0.001; PTH vs. PTH then Alend: P < 0.005; PTH vs. PTH wait Alend: P < 0.0005. Figs. 2A,
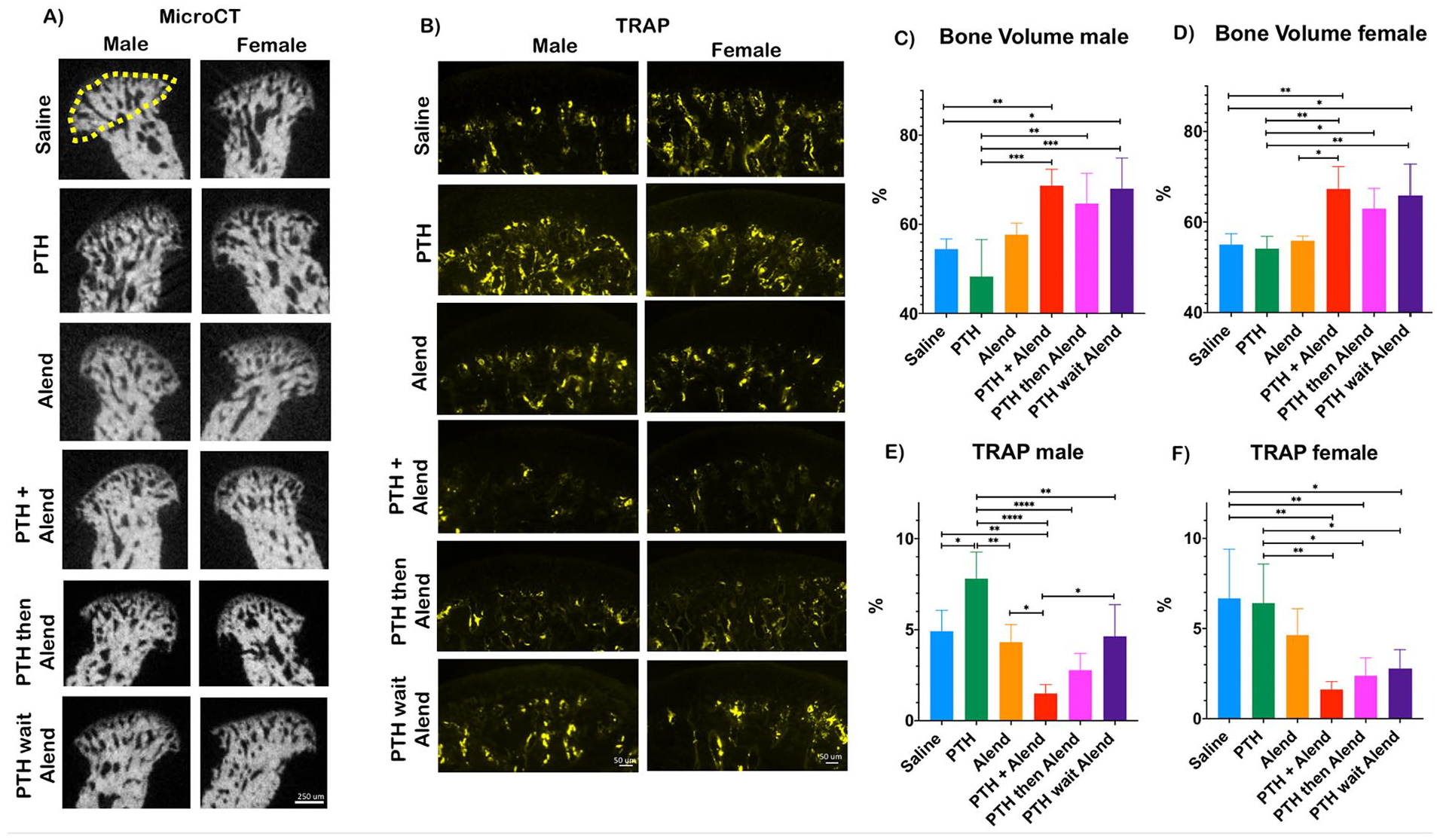
Significant increased bone volume and decreased TRAP of the mandibular condyle after I-PTH + Alendronate administration. (
Bone remodeling was studied by fluorescent TRAP staining. PTH alone led to a significant increase in TRAP activity in relation to saline group in males (PTH vs. Saline: P = 0.01, Fig. 2E). Interestingly, in female mice, the combination uses of Alend and PTH led to a significant reduction in TRAP activity in comparison with the saline group or the PTH group, when the individual use of Alend failed to do so (Saline vs. PTH + Alend: P = 0.001; Saline vs. PTH then Alend: P < 0.01; Saline vs. PTH wait Alend: P < 0.05; PTH vs. PTH + Alend: P = 0.001; PTH vs. PTH then Alend: P = 0.01; PTH vs. PTH wait Alend: P < 0.05; Fig. 2B and
Cartilage Thickness
Mandibular condyle cartilage thickness was evaluated in TB-stained sections. In female mice, PTH or Alend alone caused a substantial increase in cartilage thickness (PTH vs. Saline: P = 0.01; Alend vs. Saline: P < 0.001; Fig. 3A and
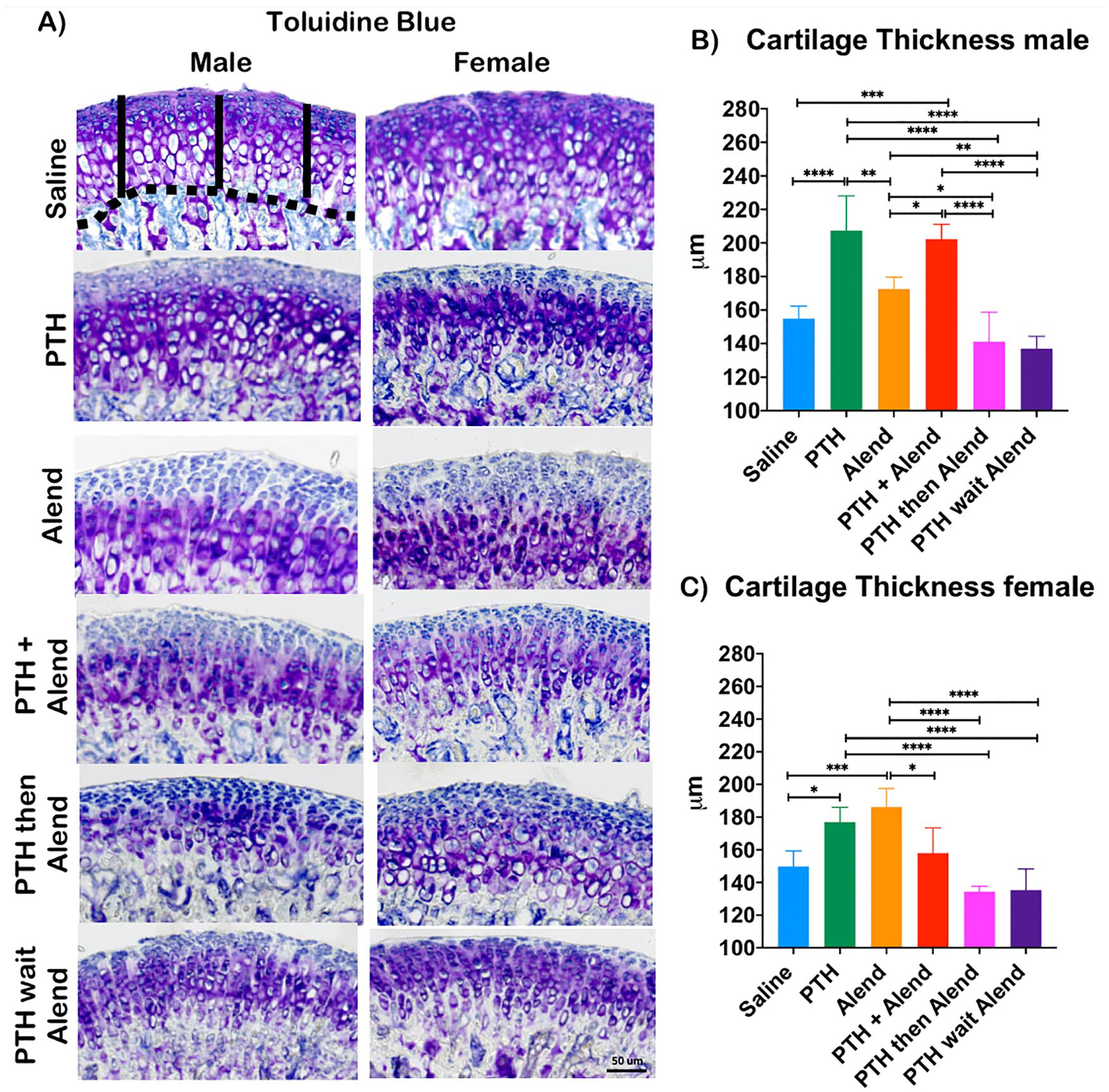
Significant increased cartilage thickness after I-PTH administration in male and female. In addition, in males, the cartilage thickness was significantly increased with concurrent administration of I-PTH + Alendronate, whereas in females, the cartilage thickness was increased with administration of Alendronate. Sagittal sections of mandibular condyles stained with Toluidine blue. (
Chondrocyte Proliferation and Apoptosis
Next, we examined chondrocyte apoptosis by TUNEL staining. In both females and males, PTH or Alend treatment alone reduced chondrocyte apoptosis in comparison with Saline (females: Saline vs. PTH: P = 0.0005; Saline vs. Alend: P < 0.05; males: Saline vs. PTH: P < 0.0001; Saline vs. Alend: P < 0.0001; Fig. 4A,
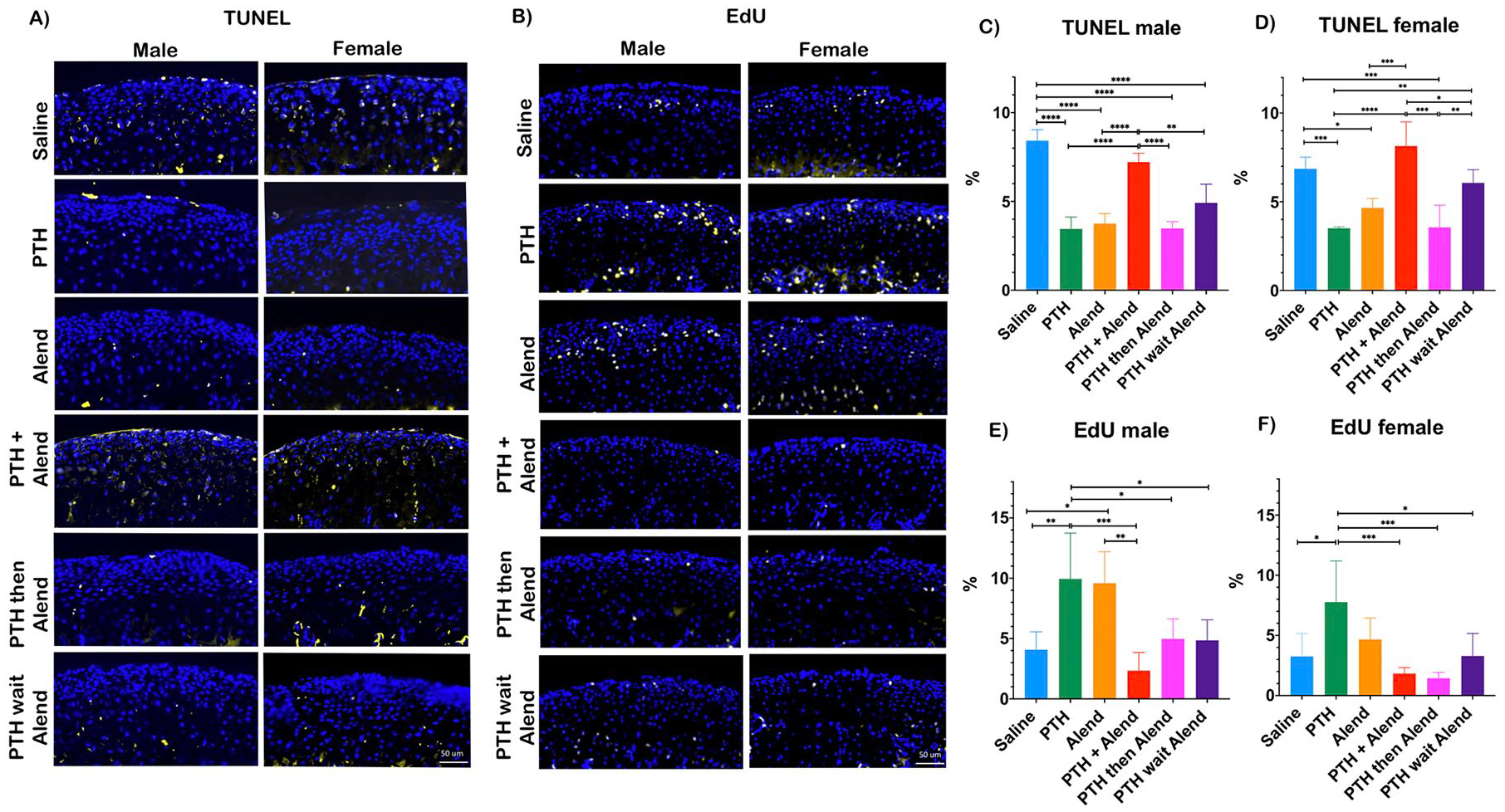
Significant increased TUNEL in saline and concurrent administration of I-PTH and Alendronate. Significantly increased EdU with administration of I-PTH both in males and females. In addition, we saw increased EdU in males with the administration of Alendronate. (
EdU proliferation assay revealed that PTH administration alone induced an increased chondrocyte proliferation in comparison with saline or when PTH in combined with Alendronate in female mice (PTH vs. Saline: P = 0.PTH vs. PTH + Alend: P < 0.001; PTH vs. PTH then Alend: P < 0.001; PTH vs. PTH wait Alend: P < 0.05; Fig. 4B and
Our transgene expression revealed that PTH administration alone induced an increased Col1a1 cells when compared with other experimental groups both in males and females (PTH vs. saline: P < 0.001; PTH vs. Alend: P = 0.001; PTH then Alend: P < 0.001; PTH wait Alend: P < 0.05; Fig. 5A,
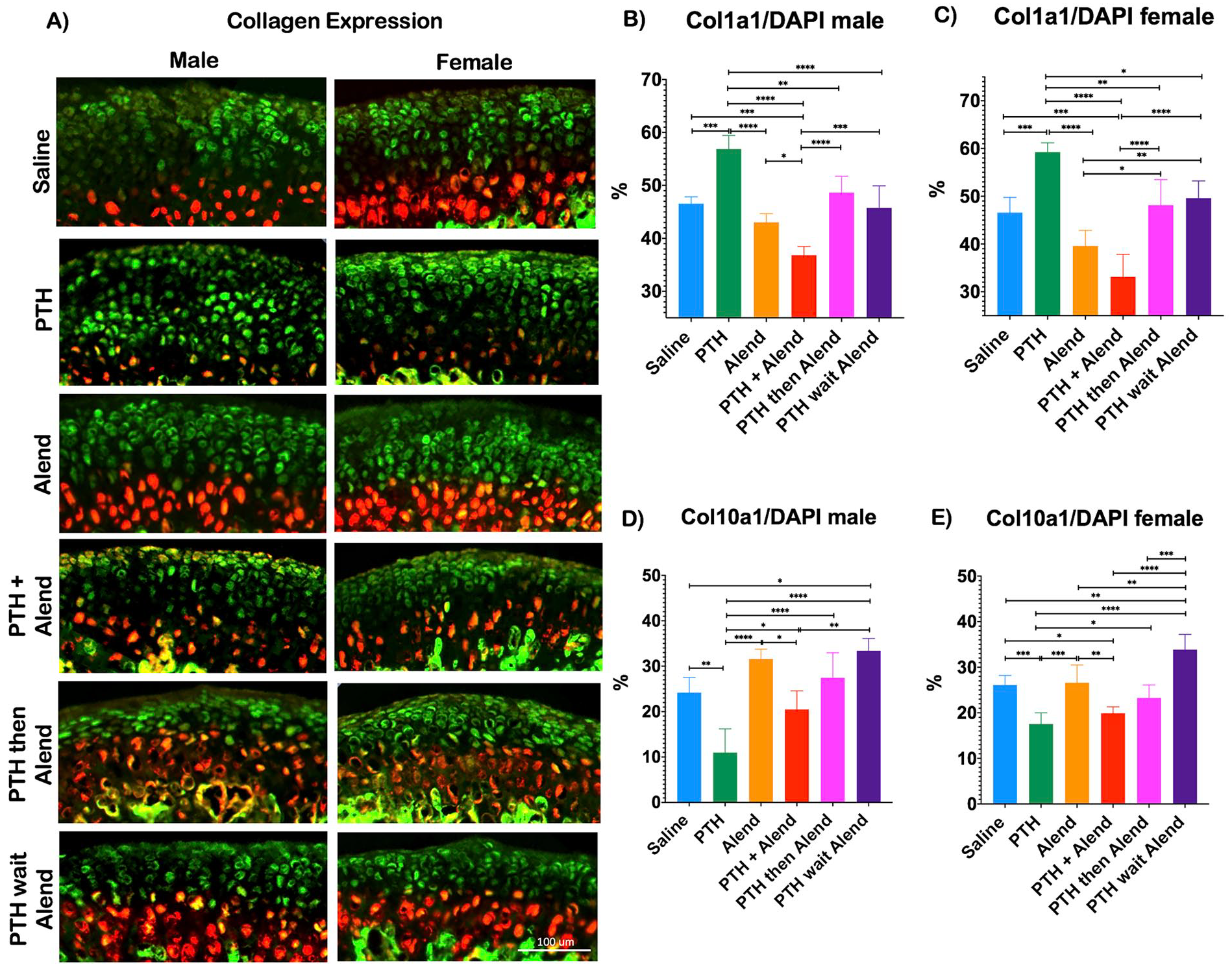
Significant increased Col1a1 green cells with I-PTH administration and increased Col10a1 cells with I-PTH wait and Alendronate administration. In addition, Alendronate alone had significant increase in Col10a1 red cells with all the groups but Saline and PTH wait and Alendornate administration. (
The Col10a1 cells were significantly increased in PTH wait Alend group when compared with Saline, PTH and PTH + Alend groups (PTH wait Alend vs. saline: P < 0.05; PTH wait Alend vs. PTH: P < 0.0001; PTH wait Alend vs. PTH + Alend: P < 0.001; Fig. 5A,
Expression of Cartilage Degeneration Markers
Administration of PTH or Alend alone or in separated combination (PTH then Alend, PTH wait Alend) substantially decreased the expression of MMP13, in both female and male mice in comparison with saline injection (females: Saline vs. PTH: P < 0.0001; Saline vs. Alend: P < 0.0001; Saline vs. PTH the Alend: P < 0.0001; Saline vs. PTH wait Alend: P < 0.001; males: Saline vs. PTH: P < 0.001; Saline vs. Alend: P < 0.001; Saline vs. PTH then Alend: P < 0.0001; Saline vs. PTH wait Alend: P < 0.05. Fig. 6A,
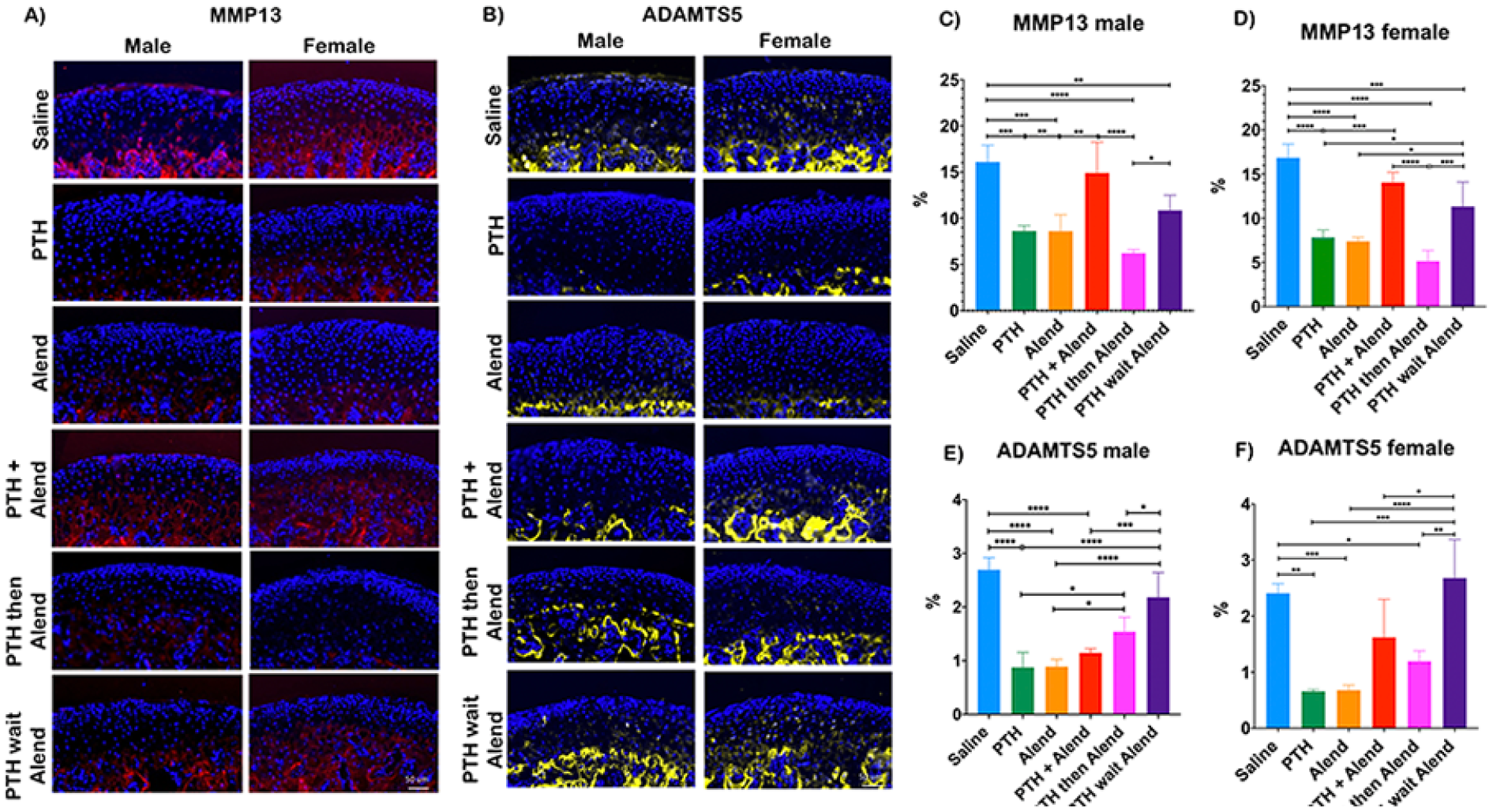
Significant decreased expression of MMP13, and ADAM metallopeptidases with thrombospondin type 1 motif 5 (ADAMTS5) with I-PTH and Alendronate administration. In addition, the MMP13 expression in males and females was significantly decreased with I-PTH administration and then wait and then Alendronate administration, whereas ADAMTS5 expression in males was decreased with concurrent administration of I-PTH + Alendronate, and in females, it was decreased with I-PTH administration and then wait and then Alendronate Immunohistochemistry for MMP13 (
Regarding ADAMTS5, PTH and Alend also significantly decreased the expression of this proteinase associated with aggrecan degradation (females: Saline vs. PTH: P < 0.005; Saline vs. Alend: P < 0.0005; males: Saline vs. PTH: P < 0.0001; Saline vs. Alend: P < 0.0001; Fig. 6B,
Discussion
The current treatment for TMJ-OA is limited and National Institute of Dental and Craniofacial Research (NIDCR) recommends palliative treatment with analgesics (nonsteroidal anti-inflammatory drugs). Partial or total TMJ replacement is the only available alternative treatment for TMJ-OA. Therefore, the development of effective disease modifying treatment for TMJ-OA is needed.
Effects of I-PTH and Alendronate on Bone
We found that in both male and female mice, I-PTH and Alendronate had no effect on mandibular condylar subchondral bone volume when administered individually, but when combined, they acted synergistically to promote significant increases on bone volume. Effects on bone volume were comparable regardless of the combination, and it made no difference if I-PTH and Alendronate were co-administered or administered in sequence. I-PTH and Alendronate also acted synergistically to block osteoclast activity (as revealed by TRAP staining) in both males and females. In males, this effect was somewhat less pronounced when Alendronate was administered immediately after I-PTH and significantly less pronounced when Alendronate was administered after 7 days; in females, all combinations were comparably synergistic. Although there was a significant increase in TRAP levels in males, overall, I-PTH and Alendronate had little effect on osteoclast activity by themselves in either males or females. Together, these results demonstrate strong, synergistic, and anabolic effects of PTH and Alend on mandibular condylar subchondral bone when they are administered in combination or in sequence, but not individually. This signifies that concurrent I-PTH + Alendronate administration and Alendronate treatment after I-PTH administration significantly reduced the subchondral bone remodeling and increased mandibular condylar subchondral bone volume both in males and females. Alendronate has been shown to improve the architecture of subchondral bone and periarticular bone following OA in the knee joint. 15 The efficacy of anti-resorptive treatments for preventing OA may depend on several systemic and environmental factors, such as the rate of subchondral bone turnover. The current study used young male and female triple transgenic reporter mice, and they have an accelerated subchondral bone remodeling of the TMJ, which is further accentuated by administration of I-PTH, 10 and Alendronate has been shown to be more effective in a background with high bone turnover. 15 Increased bone volume in response to combined PTH and Alend paralleled decreased osteoclast activity, raising the possibility that reduced matrix turnover might be responsible for the increased bone volume. One of the hallmark of OA is thickened subchondral bone or significant loss of subchondral bone. Loss of subchondral bone usually happens after trauma/injury and based on our observation, alendronate if given after I-PTH can significantly reduce the loss of subchondral bone.15-18
Effects of I-PTH and Alendronate on Cartilage Alone
PTH is an endocrine regulator of mineral homeostasis specifically of calcium and phosphate levels.19,20 It has been shown that continuous PTH exposure results in catabolic effects, while intermittent PTH is associated with anabolic effects.19,20 I-PTH has been used for the treatment of clinical osteoporosis.17,21,22 Effects of individual I-PTH and Alendronate were consistently anabolic for TMJ cartilage, causing significantly increased cartilage thickness and chondrocyte proliferation, and significantly reduced levels of apoptotic cell death, MMP13, and ADAMTS5. It has been shown that I-PTH has an anabolic effect to the osteochondral tissue of TMJ 10 and knee joint.23,24 Anabolic effects of I-PTH and Alendronate were nearly always significantly more dramatic in males; the only exception was cartilage thickness in response to Alendronate—which was increased in both males and females, but the increase did not reach statistical significance in males. These observations lead us to conclude that overall, female TMJ cartilage is less responsive than male TMJ cartilage to anabolic stimulation by I-PTH 25 or Alendronate, and/or that some aspects of female physiology impair the ability of I-PTH or Alendronate to promote anabolic responses.25,26
We also noted significant changes in the domains of expression of Col1a1 and Col10a1 in response to I-PTH treatment. Specifically, in response to PTH, the domain of Col1a1 expression in the MCC was significantly increased, and that of Col10a1 significantly decreased. Increased Col1a1 expression in MCC is associated with anabolic stimuli such as treatment with BMP2 27 or mechanical loading. 28 Thus, the increased Col1a1 expression in mice treated with I-PTH can be unambiguously categorized as an anabolic response, which aligns well with the other anabolic effect that I-PTH exerted on TMJ cartilage, including increased proliferation and cartilage thickness and suppression of apoptotic cell death and MMP13/ADAMTS5 levels. That the reduced Col10a1 expression domain is also an anabolic response to I-PTH is supported by other studies demonstrating reduced Col10a1/collagen type X levels in TMJ cartilage in response to other anabolic stimuli, such as genetic FGFR1 deletion, in which decreased collagen type X accompanied increased cartilage thickness and chondrocyte proliferation, and reduced matrix protease production. 29
The increased Col1a1—and decreased Col10a1—domains in response to I-PTH are not the result of altered collagen turnover, because the fluorescent reporters in our study reflect mRNA expression, and not protein distribution. Rather, the changes in Col1a1 and Col10a1 expression domains in I-PTH-treated TMJ cartilage reflect a shift toward a greater proportion of chondrocytes expressing Col1a1 relative to Col10a1. This pattern is characteristic of TMJ cartilage from young animals as opposed to aged animals, 30 suggesting I-PTH treatment not only stimulates growth of the MCC, but may also rejuvenate it; this idea is supported by recent studies by us and others showing delay of age-related TMJ degeneration in response to I-PTH.10,31
Effects of I-PTH and Alendronate on Cartilage Together
Co-administration of I-PTH and Alendornate (PTH + Alend) significantly blocked or blunted their individual anabolic effects on chondrocyte proliferation and suppression of apoptosis and MMP13 levels, in both male and female TMJ cartilage.
Notably, and only in females, co-administration also blocked the individual anabolic effects of I-PTH and Alendronate on TMJ cartilage thickening. This result is consistent with our suggestion that some aspects of female physiology impair the anabolic effects of PTH and Alendronate on TMJ cartilage, 25 and further, raises the possibility that this catabolic influence is part of a feedback response to I-PTH7,32,33 and/or Alendronate stimulation.
Our observation that TMJ cartilage thickness was increased only in male mice in response to co-administered I-PTH and Alendronate (PTH + Alend) is at first puzzling, as most of the accompanying physiologic measures were catabolic, not anabolic—for example, proliferation and Col1a1 levels were reduced, and MMP13, TUNEL, and Col10a1 levels were no longer suppressed. Moreover, similar changes occurred in female mice, indicating that changes in these measures were not influenced by the sex of the animal. However, we noticed that in males, ADAMTS5 levels continued to be very strongly suppressed in response to co-administered I-PTH and Alendronate—to the same extent as they were in response to I-PTH or Alendronate alone—but this was not the case in females, in which ADAMTS5 levels returned to baseline when I-PTH and Alendronate were co-administered. These results indicate that ADAMTS5 suppression is completely blocked by co-administered I-PTH and Alendornate in female TMJ cartilage only. We propose that the increased cartilage thickness in male mice in response to co-administered I-PTH and Alendronate is due to impaired ADAMTS5-mediated matrix turnover—presumably of aggrecan and/or other matrix components normally targeted by ADAMTS5, such as hyaluronan or versican.34-36 In the future, it will be of interest to examine the relative abundance of aggrecan, hyaluronan, and versican in male versus female TMJ cartilage in the presence of PTH and Alend alone and in combination.
Administering I-PTH and Alendronate in sequence (first PTH, then Alendronate), restored some, but not all, of their individual anabolic effects on MCC, which were otherwise blocked by combined delivery. For example, the ability of I-PTH or Alendronate to suppress TUNEL and MMP13 levels, and of I-PTH to increase Col1a1 expression—anabolic effects that were completely blocked when I-PTH and Alendornate were given together—were partially restored when PTH and Alendronate were given in immediate sequence. This is surprising as the difference between administering I-PTH and Alendronate together, versus administering them in immediate sequence, is only a matter of moments. Our interpretation is that the physiology of MCC is exquisitely sensitive to even subtle shifts in the relative amounts of I-PTH and Alendronate in the body. In contrast, the physiology of mandibular condylar bone was relatively insensitive to these shifts, at least as assayed by the measures we examined in this study (bone volume as revealed by uCT and osteoclast number as revealed by TRAP staining), which were virtually the same regardless of I-PTH and Alendronate co-administration, immediate sequential delivery, or sequential delivery with a 7-day wait in between.
Notably, sequential delivery was unable to restore the anabolic effects of individual or combined I-PTH and Alendronate on chondrocyte proliferation or cartilage thickness. Chondrocyte proliferation and cartilage thickness are key indicators of anabolic response and suggests the potential clinical benefit of individual or co-administered I-PTH and Alendronate supplementation for cartilage homeostasis.
Interestingly, the anabolic effect of immediate sequential delivery on restoring the ability of I-PTH and Alendronate to suppress TUNEL and MMP13 levels was reversed by waiting 7 days between I-PTH and Alendronate administration, and the resultant increases in TUNEL and MMP13 levels were significantly more dramatic in females than in males. Similarly, levels of ADAMTS5 and Col10a1 were also significantly increased by the I-PTH-wait-7-day-Alendronate regimen, and these increases were also more dramatic in females than in males. The physiological role of I-PTH as a factor modulating the proliferation and differentiation of chondrocytes has been long identified through parathyroid hormone-related protein (PTHrP)–Indian hedgehog (Ihh) feedback loop,7,32,33 whereas the role of alendronate on chondrocyte turnover is unclear.
MMP13 37 and ADAMTS5 38 , 39 are established cartilage degeneration markers, 40 and increase in MMP13, ADAMTS5, and TUNEL positive cells plays an important role in degradation of the cartilage. 37 ,39-43 In particular, MMP13 plays a central role in degrading collagenase matrix,44,45 whereas ADAMTS5 is known to degrade aggrecan.46,47 In our study, we observed significant reduction in MMP13 with the administration of I-PTH, Alendronate, and I-PTH and then alendronate. Elevation of MMP13 usually signifies the breakdown of the extracellular matrix and which usually precedes cartilage degeneration.10,37,40,48 Our findings of reduction in MMP13 with I-PTH and alendronate treatment have been reported previously in knee cartilage.37,40,49 In addition, our immunostaining of ADAMTS5 (preoteoglycan degrading enzyme) showed that both I-PTH and alendronate administration alone leads to decreased expression of ADAMTS5. 38 The results of our immunostaining are also consistent with increased cartilage thickness and chondrocyte proliferation, and decreased degradation of collagen and aggrecan. Collagen and aggrecan are basic structural components of the TMJ cartilage, and their breakdown correlates with the progression of TMJ-OA. Furthermore, we observed significant decrease in TUNEL (apoptosis) positive cells with the administration of I-PTH, alendronate, and I-PTH and then alendronate. Our findings of immunostaining and TUNEL positive cells are in synchrony.
Our study had several strengths including the triple transgenic reporter male and female mice and in-depth histological and micro-CT examination. To our knowledge, this is the first study looking at the effects of alendronate alone and in combination with I-PTH on the TMJ. Several other studies have investigated the role of PTH23,41 and alendronate on knee joint 15 ; however, knee joint and TMJ have distinct developmental origins 35 and are made up of different types of cartilage, comprised of unique chondroprogenitor and chondrocyte population and with matrices that differ in molecular composition, structure, and mineral content.3,50 In addition, TMJ cartilage is a secondary cartilage (develops after bone formation), whereas knee cartilage is a primary cartilage (precedes bone formation).16,50 Our study focused on younger mice to understand the role of I-PTH and alendronate in different permutations and combinations to harness the distinct role of individual and synergistic/antagonistic effects of PTH and alendronate on the osteochondral tissue of TMJ.
Our future studies will focus on studying the effects of I-PTH and alendronate in a acute (artificially induced) and chronic (age-related) TMJ degeneration model and to study the possible mechanistic pathways by which I-PTH and alendronate act synergistically or antagonictically to modify the disease.
Footnotes
Author Contributions
Conceptualization and Methodology: Mara O’Brien, Eliane Dutra, Po-Jung Chen, Ke Wang, Sumit Yadav. Data Collection: Mara O’Brien, Po-Jung Chen, Shivam Mehta, Sumit Yadav. Data Interpretation: Mara O’Brien, Eliane Dutra, Po-Jung Chen, Caroline Dealy, Ke Wang, Shivam Mehta, Sumit Yadav. Manuscript Preparation: Mara O’Brien, Eliane Dutra, Po-Jung Chen, Shivam Mehta, Ke Wang, Caroline Dealy, Sumit Yadav. Manuscript Approval: Mara O’Brien, Eliane Dutra, Po-Jung Chen, Shivam Mehta, Ke Wang, Caroline Dealy, Sumit Yadav. Funding: Sumit Yadav. Project Administration: Sumit Yadav.
Acknowledgments and Funding
We would like to thank David Rowe for providing the triple transgenic reporter mice for breeding. We would also like to thank Li Chen for assisting with imaging of histological slides. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Dental and Craniofacial Research of the National Institute of Health under Award Numbers KO8DE025914, RO3DE030526, and RO3DE030226 to SY and by the American Association of Orthodontic Foundation provided to SY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the current study as the study was performed on mice.