
Abstract
Objective
Knee osteochondritis dissecans (OCD) is a still poorly understood pathological condition of the articular subchondral bone and its overlying cartilage. Patellofemoral involvement accounts for less than 1% of cases; tibial plateau and multifocal involvement is an even rarer instance. The purpose of this study is to review what is currently known about patellofemoral OCD (PF-OCD) and to present an unusual case of PF-OCD which progressed to become multifocal in an adult female patient.
Methods
A comprehensive literature search was conducted on PubMed/Medline, Cochrane, Embase, Web of Science, and Scopus databases on September 2021 for all levels of evidence and English language. After duplicate removal, 234 papers pertaining to PF-OCD were retrieved. Thirty-nine studies met inclusion criteria and were included in the review. As an example, a unique case of delamination of patellar cartilage consistent with PF-OCD with progressive involvement of trochlea and both tibial plateau in a 35-year-old woman is also presented.
Results
PF-OCD is a rare localization of knee OCD. Two hundred eighty-eight cases have been reported in the literature to date. Mean age at time of diagnosis was 16 years and the location could also be bilateral and multifocal. The etiology is still debated but traumatic, vascular, and hereditary mechanisms are likely. Management mirrors that of classical OCD.
Conclusions
PF-OCD is an uncommon cause of anterior knee pain but should be considered even when physeal plates are closed. Current available evidence on treatment is of low quality, based on single case reports or small retrospective case series.
Introduction
Osteochondritis dissecans (OCD) is a still poorly understood pathological condition of the joint in which a fragment of the subchondral bone and its overlying cartilage begins to separate from the surrounding area, eventually detaching and becoming a loose body. While this condition may occur in various joints (e.g. elbow, ankle), the knee is by far the most commonly involved. 1 OCD is a common source of knee pain and dysfunction and must be differentiated from other sources of nontraumatic knee pain. Osteochondral lesions are predominantly located on the articular surface of medial and lateral condyles with the patella, trochlea, and tibial plateau being much more rarely involved, particularly in older patients when the physeal plates are already closed. Estimated prevalence ranges from 15 to 29 cases per 100,000 with the greatest incidence of OCD in the young, physically active male, with still open physis (12-19 years old). Incidence dramatically decreases with age and closure of the physis.2-4 Males are 4 times more likely than females to develop the disease. OCD affects mainly the medial femoral condyle (70%) followed by the lateral femoral condyle (24%). Patellofemoral involvement accounts for less than 1% of all cases of knee OCD (although Flynn reports rates as high as 5%, tibial plateau and multifocal involvement is an even rarer instance with only few reports in medical literature). 3 ,5-9 The precise pathogenesis is still unknown although it can be divided into 3 different categories: traumatic, ischemic, and biological/hereditary. Repetitive microtrauma or focal cartilage overload in varus/valgus knee malalignment or the presence of discoid menisci are established mechanisms implicated in the young open physis athlete.10,11 Subchondral ischemia leading to bone edema and subsequent necrosis, coupled with genetic predisposition, might be a more common cause in older, nonathlete patients or in nonweightbearing articular zones. The purpose of this study is to review what is currently known about patellofemoral OCD (PF-OCD) and to present an unusual case of PF-OCD which progressed to become multifocal, involving the femoral trochlea and both tibial plateaus in a 35-year-old female.
Methods
A comprehensive search was conducted on PubMed/Medline, Cochrane, Embase, Web of Science, and Scopus databases on August 2021 using the following terms and Boolean logic operators: “Patellar osteochondritis dissecans” OR “Osteochondritis dissecans of the patella” OR “Patello femoral osteochondritis dissecans” OR “Patellofemoral osteochondritis dissecans.” Articles were screened by title and abstract. Inclusion criteria for relevant articles were English language and focus on patellar or trochlear OCD. Exclusion criteria were studies on knee pathologies other than OCD, no available abstracts, languages other than English, and involvement of joints other than the patellofemoral. The full text of selected papers was reviewed and their reference lists were analyzed to look for potential inclusion of papers omitted from the initial search. Relevant data (type of study, demographics of study population, pathomechanisms proposed, type of treatment, and outcome) were then extracted and a unique database for analysis was created.
Results
Two hundred thirty-one results were retrieved. Articles were screened by title and abstract. Three additional papers were identified through references. After duplicate removal, 75 studies focusing on PF-OCD were identified, with the earliest report published by Rombold in 193612. Thirty-six studies were excluded (20 studies had no abstract available, 3 articles were in German, 4 articles were in French, 1 article was in Italian, 1 article was in Polish, 2 articles were about knee OCD and not PF-OCD, 4 articles dealt with other pathologies than OCD, and 1 article was an historical account), thus leaving 39 full-text papers for analysis. Of these, 2016 were single case reports, 14 retrospective case series, 4 surgical technique notes, and 1 radiological description.
Prevalence and Pathogenesis
Pooling the results of the studies analyzed, 288 patients (249 patellar OCD, 39 trochlear OCD) have been reported to date, but figures are likely to be higher as a significant percentage of published studies have not been included due to exclusion criteria.12-39 Mean age at time of diagnosis of PF-OCD is higher than that of general knee OCD, being around 16 years with the oldest patient reported being 30 years old.12,16,19,20,23,26-36,38,39 Generally only 1 knee is affected but 11 studies reported bilateral involvement.13,16,20,21,23,27,28,34,37,40,41 Men are more commonly affected than women with ratios ranging from 2:1 to 9:1 (mean 4:1),16,18,23,24,26,30,31,33-36, 39 and 2 studies reported only on male patients.18,24 Mechanical pathomechanism such as repetitive shearing stress and overuse is reported by 12 studies, 13 ,15-17,20-22,24,25,29,36,41 while only 3 studies report a possible biological etiology.20,27,29 One study found a significant association between PF-OCD and sports like soccer and basketball 36 and 4 studies reported a history of previous trauma.13,16,25,42 An association with patellar instability/maltracking was hypothesized by 5 studies.13,20,24,25,37
Treatment
Twenty of the 39 articles reviewed contained data on surgical treatment and outcome on a pooled population of 209 patients with a mean age of 16 years (
Outcome of Surgical Treatment of Patellofemoral OCD.

OCD = osteochondritis dissecans; ICRS = international cartilage repair society; IKDC = internationl knee documentation committee.
Case Presentation
A 35-year-old female presented after sustaining a left knee sprain injury while skiing. She underwent knee MRI which showed partial anterior cruciate ligament (ACL) injury and was initially managed with muscle strengthening because of mild post-traumatic instability. Initially, her pain resolved, allowing her to focus on rehabilitation for 2 months. After that point, she experienced an unexpected, progressive, relapse of pain along with new onset knee catching. Her symptoms worsened so much that she was unable to walk unaided, raising the suspicion of post-traumatic complex regional pain syndrome (CRPS). There was no gross instability as might have been expected and her main complaint was anterior knee pain. A repeat MRI showed high-signal-intensity fluid separating the patellar cartilaginous surface almost entirely from the underlying subchondral bone (
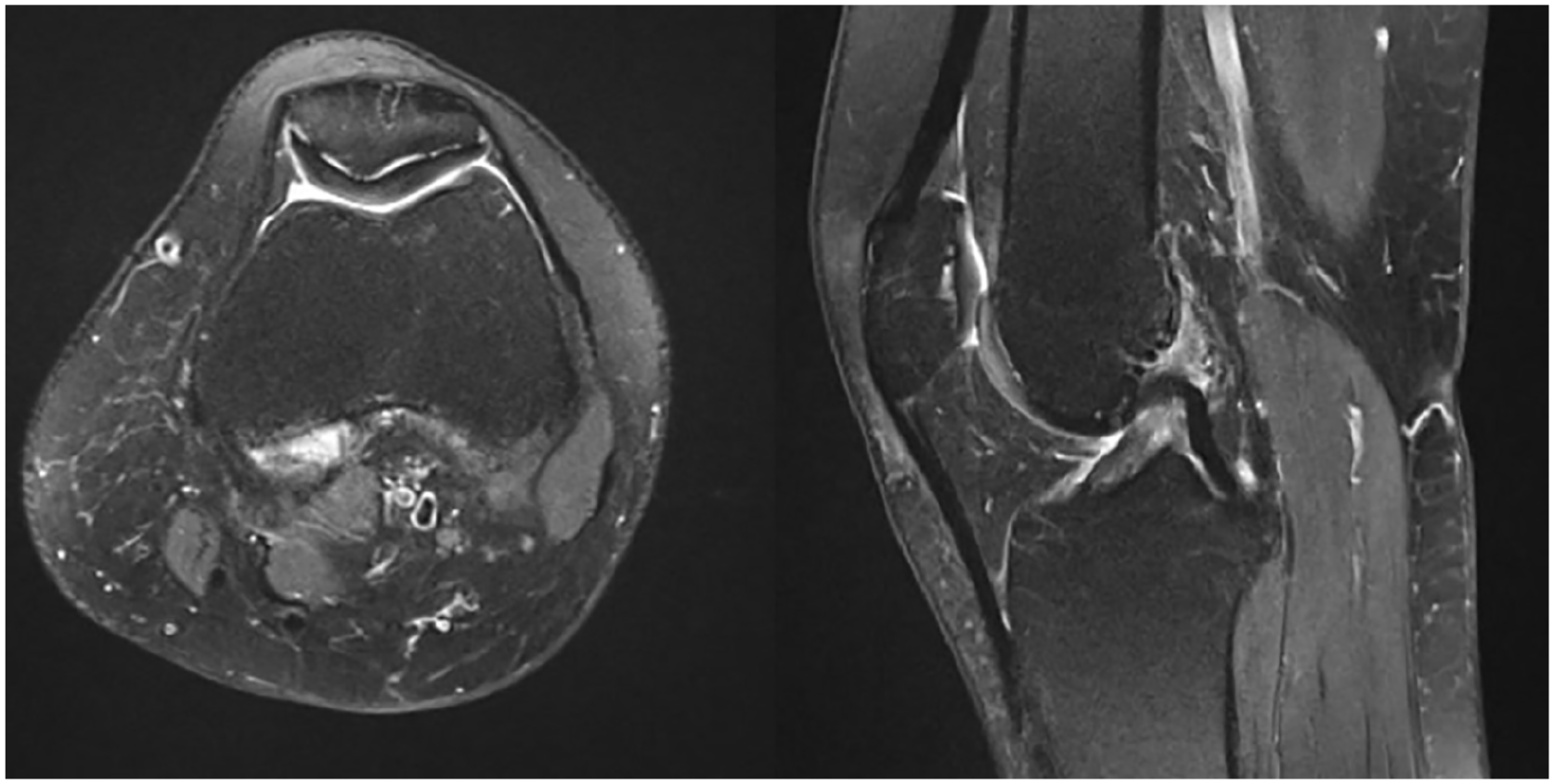
Fat suppressed proton-density turbo-spin-echo (FS-PD-TSE) high-signal-intensity line representing fluid collection separating the patellar cartilage from the underlying subchondral bone. This delamination might represent osteochondritis dissecans of the entire patella. The same finding is visible, although to a much lesser extent, on the femorale trochlea.
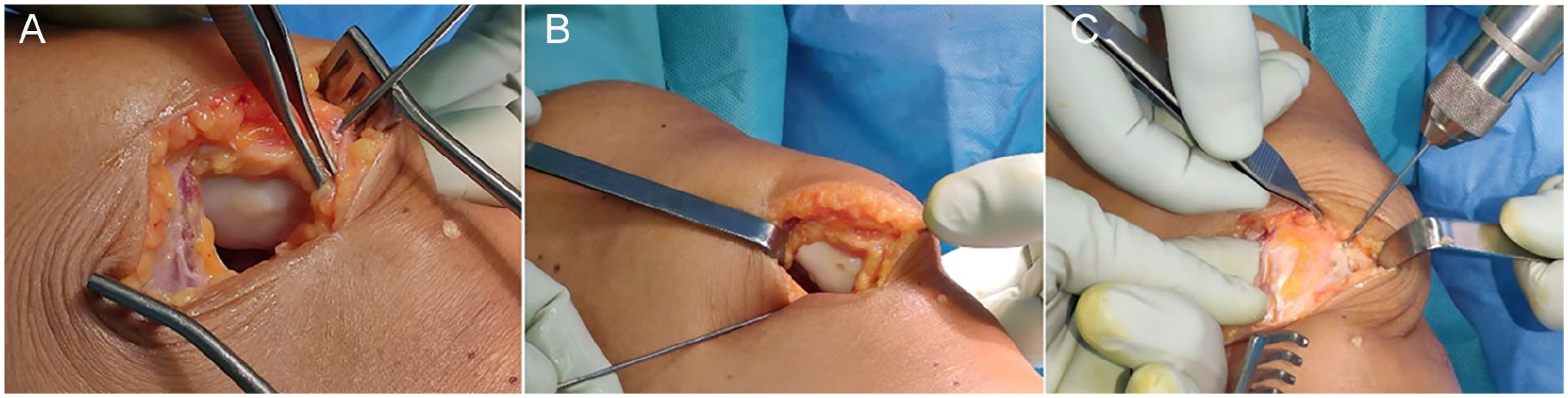
(A) Deceivingly healthy and smooth looking patellar cartilage with a 3-cm blister on the medial facet. Despite the innocent-looking appearance, the cartilage was soft on probing. (B) Pinning and drilling of the separated cartilage. (C) Dorsal drilling of patellar cartilage.
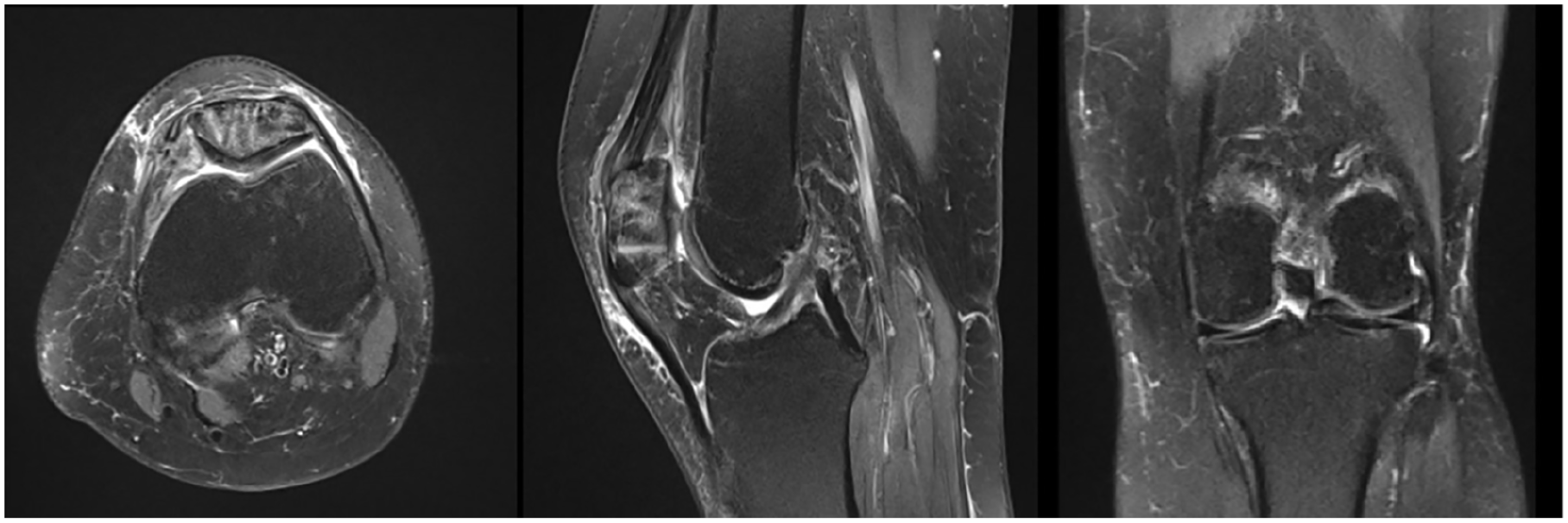
Fat suppressed proton-density turbo-spin-echo (FS-PD-TSE) MRI sequences 2 months after surgery. Patellar cartilage has now healed and cartilage delamination has progressed to entire trochlea and to a lesser extent to both tibial plateau. Note the continuous thin high-intensity-signal line separating cartilage from underlying subchondral bone.
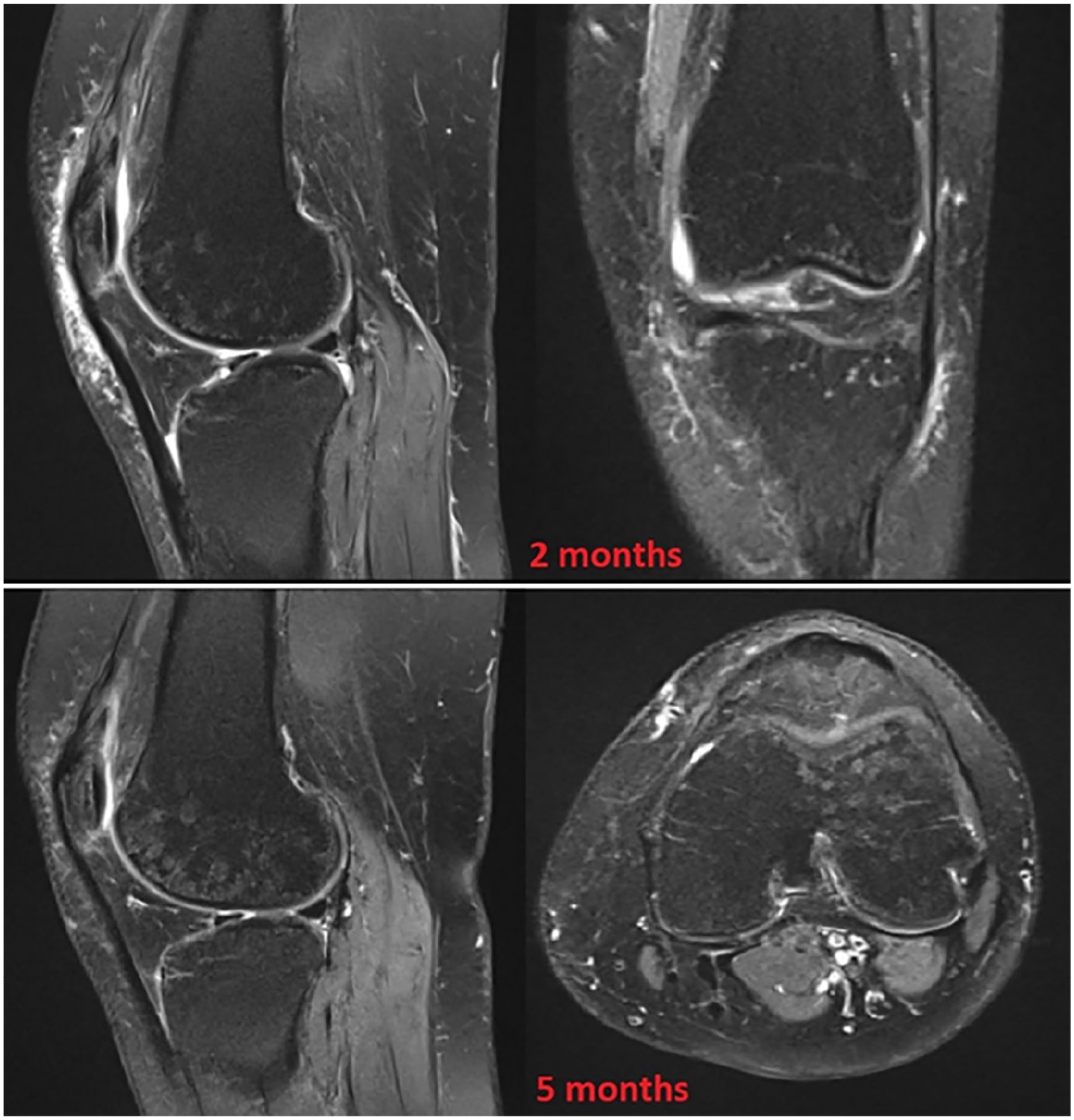
Grainy appearance with hyperintense fat suppressed proton-density turbo-spin-echo (FS-PD-TSE) ovalar foci “salt & pepper” of the bone of the lateral femoral condyle at 5 months after surgery. Compared with the MRI taken at 2 months, the finding had become more evident.
Discussion
PF-OCD is a rare localization of the more common medial and lateral femoral condyle ostechondritis dissecans of the knee. Historically, the first account of this disease dates back as far as the 17th century, when a bony lesion consistent with PF-OCD has been found on the patellar bone of a Florentine kickball player. 43 The exact prevalence has never been reported but it is estimated to be 1% or less than that of general knee OCD (15-29 cases per 100,000 population). 6 ,44-46 Pooling the results of the studies analyzed, 283 patients (244 patellar OCD, 39 trochlear OCD) have been reported to date, but figures are likely to be higher as a significant percentage of published studies have not been included due to exclusion criteria.12-39 Mean age at time of diagnosis of PF-OCD is higher than that of general knee OCD, being it around 16 years with the oldest patient reported being 30 years old.12,16,19,20,23,26-36,38,39 Normally, only 1 knee is involved, but 11 studies reported bilateral involvement.13,16,20,21,23,27,28,34,37,40,41 Backes and 3 other authors have reported >1 lesion occurring in the same knee, as occurred to our patient, coining the term “Multifocal juvenile OCD of the knee,” whose prevalence is currently unkown.29,32,33,47 As for classic knee OCD, etiology of PF-OCD is unclear and still debated: 129 studies reported a previous history of sporting activities and 4 previous history of trauma thus emphasizing the “traumatic hypothesis” in which chronic or repetitive shearing forces, minor injuries to articular surfaces, repetitive loading, microtrauma, and recurrent patellar subluxation are believed to cause the cartilage delamination. Schwarz et al. 16 and Bruns et al. 25 reported a history of trauma in up to 38% and 53% of patients, respectively.16,25 Price et al. 36 found a significant association between pediatric athletes who played basketball and soccer and the development of trochlear juvenile OCD, lending further support to the traumatic pathogenesis stressing the concept of concentration of high loads and shear forces on the patella. 36 There is, however, a subset of patients who do not play any sports nor sustained any knee injury and yet develops the disease: 8 studies report on multifocal knee OCD, involving simultaneously more joints and an entire family suffering from the PF-OCD.20,27,29,32,33,47-49 Livesley and Milligan 20 hypothesized an inherited predisposing factor which they identified in an abnormality of the mechanics of the knee (recurrent subluxation). 20 Irrespectively of anamnestic trauma, Bruns et al. 25 observed that most of the patients with PF-OCD exhibited a flat articular surface of the patella (Hertel type I and V), a greater lateral than medial patellar facet (Wiberg type II and III), and a hypoplasia of the medial and hyperplasia of the lateral part of the trochlea (Hepp type III) postulating that patellar maltracking (due to excessively flat patellar articular surface or anatomic deformities of the trochlea) led to increased localized load transmission, thus initiating the subchondral osteonecrosis. 25 The same mechanism has been advocated by Ravier et al. 37 to explain bilateral lesions in an adolescent skier. In 1967, Scapinelli 50 gave a precise description of the 2 main arterial systems nourishing the patella: the mid-patellar (dorsal) system entering anteriorly and the infrapatellar entering inferiorly through Hoffa’s fat pad. 50 As a result of this vascular anatomy, the inferior half receives dual blood supply as confirmed by a subsequent gadolinium-enhanced MRI cadaveric study by Lazaro et al. 51 PF-OCD lesions are mainly found in the central-inferior part of patella, thereby making the “ischemic hypothesis” unlikely to be the only cause. 28 When multiple joints are involved, a biological factor is likely to play a role.27,48 Andriolo et al., 11 in a recent systematic review on knee OCD, cites several authors who found a familial occurrence and some also identified specific gene alterations. 11 For PF-OCD, choice between nonoperative and operative management and type of operative treatment essentially mirrors that of classical OCD. 1 Surgical treatment is indicated in failure of nonoperative management of stable lesions, symptomatic unstable lesion in skeletally immature patients, and any kind of symptomatic lesions in the adult. Juvenile PF-OCD responds better to conservative treatment, when feasible, compared with adult PF-OCD, where operative treatment is generally the rule since nonoperative management has also been shown to do poorly when physis are already closed. 52 When treating adults with closed physis or unstable lesions, surgical options are essentially: removal of loose bodies, debridement, transarticular drilling, microfractures, fixation with small screws or pins (metallic and bioabsorbable), lateral retinacular release, and chondroplasty or mosaicoplasty for later stages (ICRS III-IV). In 1988, Schwarz et al. 16 published the first case series on 25 patients surgically treated with curettage and loose bodies removal reporting only 38% of good results with 6-year follow-up. 16 In 1990 and 1994, better results by drilling, internal fixation with screws, loose bodies removal, and curettage were reported18,23 and up to 5 of the 6 patients had resumed previous activities pain free.18,23 In 2000, Peters and McLean 26 published the largest case series reporting operative results on 37 patients; using variable techniques treatment generally improved symptoms although individuals with cartilage loss were likely to have persistent patellofemoral pain. Wall et al. 33 in 2014 reported on 67% of patients that were healed and had returned to full activity. 33 On the contrary, the last 2 case series published in 2015 and 2018 with a follow-up of, respectively, 3.8 years and 21 months reported higher percentage of return to play ranging from 75% to 100%, although the percentage of patients improved but experiencing persistent pain was as high as 48%.34,36 It seems that choice of treatment depends on lesions size, stability, and stage of chondral damage. Cell-based therapy (autologous chondrocytes, bone marrow stem cell, and more recently, injection of adipose-derived mesenchymal stem cells) has been proposed.31,38 If the chondral damage is too severe (IRCS III-IV), mosaicoplasty with autologous trochlear cartilaginous pegs has been described with satisfying results. 30 Sixteen of the 33 articles reviewed contained data on surgical choice and outcome ( Table 1 ). Over time, there has been a progressive improvement in outcome, ranging from less than 40% of patients achieving satisfying results after surgery to over 85% at present, possibly reflecting refinement of surgical techniques. Female sex and prolonged duration of symptoms have been reported as predictive of residual pain regardless of management. 34 Patellar maltracking has been considered by many authors to be a contributing factor in the development of PF-OCD20,25,37 and as such, correction of the imbalance by release of the lateral retinaculum has been advocated to produce good results.24,26 Smith 18 went further arguing that mild residual symptoms probably represent incongruity of the patellofemoral joint. 18 It is felt that simple drilling and microfracture techniques are less effective, while internal fixation with bioabsorbable pins or metal headless screws are better alternatives, although they carry the risk of hardware prominence and need of second surgery.22,36,52,53 It is in the authors’ practice to use bioabsorbable pins or transarticular drilling depending on the lesion stage. Current available evidence on treatment is of low quality, based on single case report or small retrospective case series. Due to the rarity of the condition, no prospective studies or trials have been so far published, leaving a gap that is much needed to be filled with these important investigations.
Considerations on the Case Story
The occurrence of delamination of patellar cartilage in our patient was an unexpected finding, especially in light of a previous negative MRI taken a few days after the initial trauma and the early pain-free period. Our case has some exceptional features worthy discussion. First, our patient was old enough to virtually rule out OCD in the differential diagnosis, yet this is the first report of patellar OCD affecting a 35-year-old patient to our knowledge. Second, further progression of the process, sequentially affecting other compartments of the knee, months after the initial injury, followed by self-healing, is something quite unique. No clear correlation could be established between the mechanism of injury and the late occurrence of progressive delamination of knee cartilage, leaving the question open as if mechanical factors or genetic factors had played a role. Finally, this finding was not consistent with an osteochondral fracture as it was not present on initial knee MRI and appeared only a few months later, after a pain-free period. The patellar and trochlear cartilage detached from subchondral bone in the same fashion as classical OCD with typical fluid collection between the 2 interfaces. Interestingly, there was no bone edema surrounding the lesion, usually present in classical OCD, indicating that the subchondral bone was spared, at least at an initial stage, and cartilage delaminated in its inferior layers. Instead, a grainy appearance (salt and pepper pattern) of the subchondral bone of the trochlea became evident at a later stage. We speculate that this could represent islets of reactive bone marrow changes (reconversion to red marrow) secondary to ischemia, due to preexistent silent disturbances of the vascular architecture which, in turn, may have been triggered by the trauma.54-56 Nevertheless, standard surgical treatment with drilling and internal fixation with bioabsorbable pins allowed for complete healing.
Conclusion
PF-OCD is an uncommon cause of anterior knee pain but should be considered even when physeal plates are closed. Knee trauma in such patients may result in OCD characteristics similar to the case story included in this review. The development of an osteochondral lesion like a PF-OCD may support the traumatic origin and may be prone to develop in relation to genetic predispositions. Current available evidence on PF-OCD treatment is of low quality, based on single case report or small retrospective case series.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study did not require institutional review board (IRB) approval; however, written consent was obtained by the participant.