
Abstract
Objective:
To assess the variability of postoperative rehabilitation protocols used by orthopedic surgery residency programs for microfracture of femoral condyle and patellofemoral lesions of the knee.
Design:
Online postoperative microfracture rehabilitation protocols from US orthopedic programs and the scientific literature were reviewed. A custom scoring rubric was developed to analyze each protocol for the presence of discrete rehabilitation modalities and the timing of each intervention.
Results:
A total of 18 programs (11.6%) from 155 US academic orthopedic programs’ published online protocols and a total of 44 protocols were analyzed. Seventeen protocols (56.7%) recommended immediate postoperative bracing for femoral condyle lesions and 17 (89.5%) recommended immediate postoperative bracing for patellofemoral lesions. The average time to permitting weight-bearing as tolerated (WBAT) was 6.1 weeks (range, 0-8) for femoral condyle lesions and 3.7 weeks (range, 0-8 weeks) for patellofemoral lesions. There was considerable variation in the inclusion and timing of strength, proprioception, agility, and pivoting exercises. For femoral condyle lesions, 10 protocols (33.3%) recommended functional testing prior to return to sport at an average of 23.3 weeks postoperatively (range, 12-32 weeks). For patellofemoral lesions, 4 protocols (20.0%) recommended functional testing for return to sport at an average of 21.0 weeks postoperatively (range, 12-32 weeks).
Conclusion:
A minority of US academic orthopedic programs publish microfracture rehabilitation protocols online. Among the protocols currently available, there is significant variability in the inclusion of specific rehabilitation components and timing of many modalities. Evidence-based standardization of elements of postoperative rehabilitation may help improve patient care and subsequent outcomes.
Introduction
Chondral defects of the knee are common sources of pain and loss of function that affect approximately 900,000 Americans each year and result in more than 200,000 surgical procedures.1,2 The exact incidence of cartilage defects is unknown, but several studies note the presence of articular lesions in nearly 60% to 66% of patients undergoing knee arthoscopy.2-4 Although many procedures exist to manage these injuries, microfracture remains one of the most commonly used surgical techniques due to its procedural simplicity, short surgical time, and low cost.5-7
Postoperatively, microfracture has led to favorable outcomes as evidenced by improvements in Lysholm, Tegener, SF-36 (Short Form-36), and WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores across several studies.1,8-12 In addition to the technical aspects of microfracture, postoperative success is predicated on the completion of an appropriate and effective rehabilitation program geared toward restoring range of motion (ROM), strength, and facilitating a return to baseline function. Currently, differences in rehabilitation guidelines for femoral condyle versus patellofemoral defects have not been clearly assessed. The distinction is important given the kinematics of the knee joint as modifications in variables such as weight-bearing, ROM, or exercise progression may be necessary to protect the healing lesion from compressive and shear forces during the recovery process.13-15
Several past studies have examined microfracture rehabilitation guidelines8,12,16-18 with general recommendations provided on the phases of rehabilitation. For example, Reinold et al. propose a rehabilitation progression with 4 phases based on the biological phases of cartilage maturation. 16 Mithoefer et al. propose a similar approach to rehabilitation after cartilage procedures consisting of an initial protection and joint activation phase, a progressive loading phase followed by a functional restoration phase, and ending with an activity restoration phase. 19 However, standardization of the frequency, type of exercises, timing, and inclusion of therapeutic modalities remains limited in the literature. 19 To date, minimal effort has been directed toward developing a standardized postoperative rehabilitation protocol specific to microfracture surgery. As evidenced by the literature seen across other orthopedic subspecialties, standardization of rehabilitation protocols has been correlated with improved patient outcomes as therapeutic approaches and adjunctive therapies would be presumably optimized.20-22 In addition, increased variability can have the unfortunate effects on a patient by increasing confusion. 23 Furthermore, as patients begin to utilize more online resources, the standardization of publicly available online rehabilitation protocols can help positively influence patient understanding and expectations.24,25 However, although there are general guidelines present in the literature on how rehabilitation should proceed following microfracture, distinctions on how therapeutic elements should be instituted, what, and when, modalities should be incorporated or initiated and how they differ between lesion location are yet to be elucidated. Presently, there is a paucity of research on the aforementioned subject that has precluded standardization of practice at this time. 26
The quality and variability of postoperative rehabilitation protocols for anterior cruciate ligament (ACL) reconstruction, 23 medial patellofemoral ligament reconstruction, 27 meniscal repair, 28 proximal hamstring repair, 29 Achilles tendon repair, 30 and ulnar collateral ligament 31 reconstruction have been previously assessed with significant heterogeneity found between recommended rehabilitation protocols. Similarly, the present investigation sought to assess the variability of online postoperative patellofemoral and femoral condyle microfracture rehabilitation protocols published by academic orthopedic surgery programs in the United States. We hypothesized that considerable variability will be present among all published protocols, with several deviations in protocol from what is present in the current literature.
Methods
Using a methodology previously outlined by several studies on variability in rehabilitation protocols,23,27-31 publicly available online rehabilitation protocols from academic orthopedic surgery programs in the United States were reviewed. Programs were identified from the Electronic Residency Application Service (ERAS). ERAS is an online, centralized application service used in the residency application process. Academically focused protocols were specifically selected to minimize potential bias and variability obtained through online search engines. A web-based query was performed (www.Google.com) using the search term “[Program/affiliate hospital/affiliate medical school name] microfracture rehabilitation protocol.”27-29,31 Protocols designed for pediatric patients, those pertaining to concomitant procedures (ACL reconstruction, meniscal repair or debridement, osteochondral autograft and osteochondral allograft transfer system), protocols not associated with academic orthopedic surgery programs and those lacking details about specific elements of the rehabilitation, such as time points for the initiation and progression of protocol elements, were excluded from final review. Protocols that did not provide specifics on the type of articular cartilage restoration procedure performed were also excluded.
A custom rubric ( Table 1 ) was created following review of all collected protocols. The following general categories were noted in the rubric: prehabilitation, postoperative adjunct therapy, ROM and weight-bearing, strengthening, proprioception, and return to basic activities and sports. Each protocol was evaluated for the presence or absence of modalities pertaining to the aforementioned categories contained within the rubric. Timing and range for the initiation of specific modalities contained within each protocol were extracted and averaged across all reviewed protocols containing comparable modalities for the respective articular lesion investigated. The documented time of initiation of each modality was based on the earliest documented start time in the protocol. Each protocol was assessed and reviewed by the primary author (DPT) and confirmed independently by the coauthors (SGC, HWS).
Femoral Condyle and Patellofemoral Microfracture Postoperative Rehabilitation Rubric Categories.
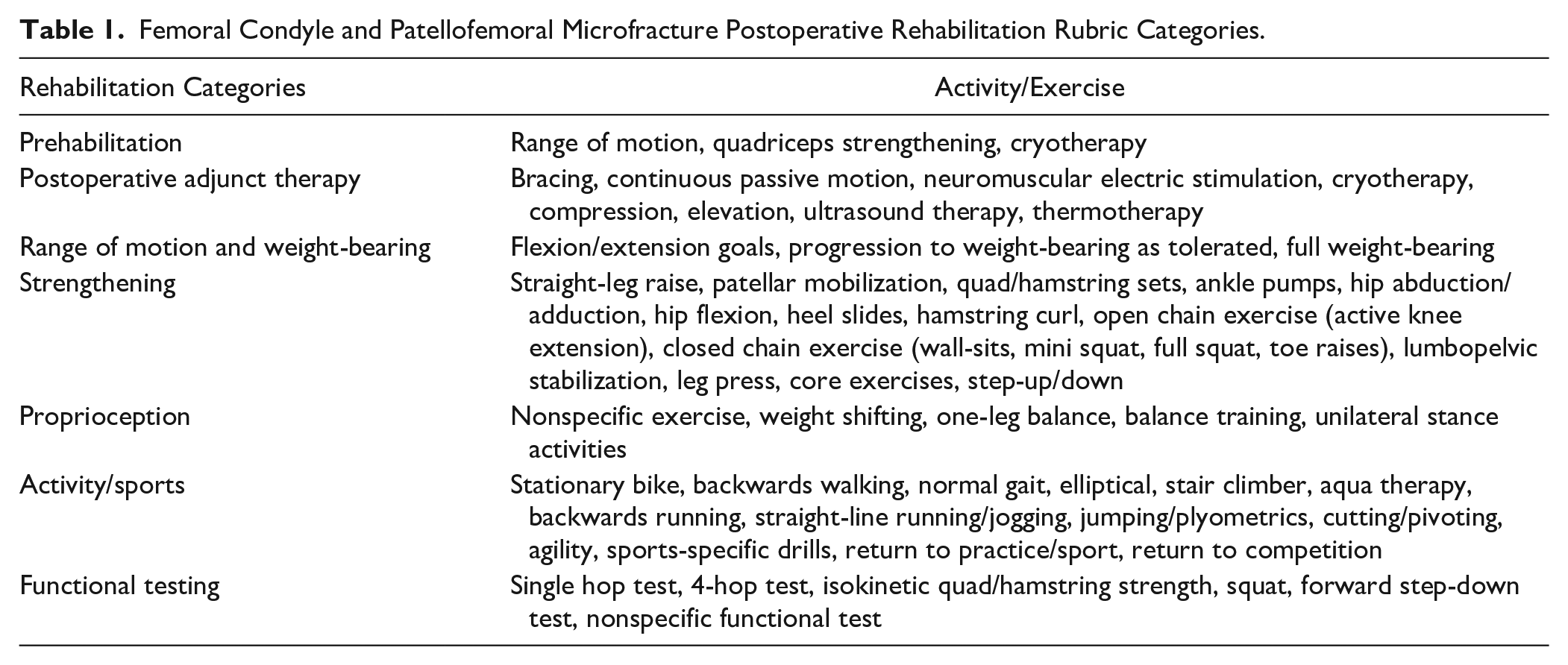
Collected information was recorded and analyzed in Microsoft Excel (Excel v16.42, Microsoft Corporation, Redmond, WA). Descriptive analyses such as the mean and range of reported initiation times for adjunctive therapies, immobilization, ROM, and strengthening were performed. Additionally, percentages of protocols that provided this information were performed.
Results
Of the 155 ERAS institutions reviewed, 18 institutions (11.6%) provided online rehabilitation protocols that met eligibility criteria. Thirteen institutions provided individual, separate protocols for femoral condyle and patellofemoral lesions (26 total protocols), 5 institutions provided protocols for femoral condyle lesions only (5 protocols total), and 5 institutions provided multiple additional, but unique protocols each attributed to different authors (7 protocols for femoral condyle lesions, 1 protocol for patellofemoral lesions, 5 protocols with mixed protocols for both patellofemoral and femoral condyle lesions), producing a total of 44 protocols available for analysis. Of the 44 protocols, 25 pertained explicitly to femoral condyle lesions, 14 pertained explicitly to patellofemoral lesions, and 5 were inclusive of both types of lesions ( Fig. 1 ).
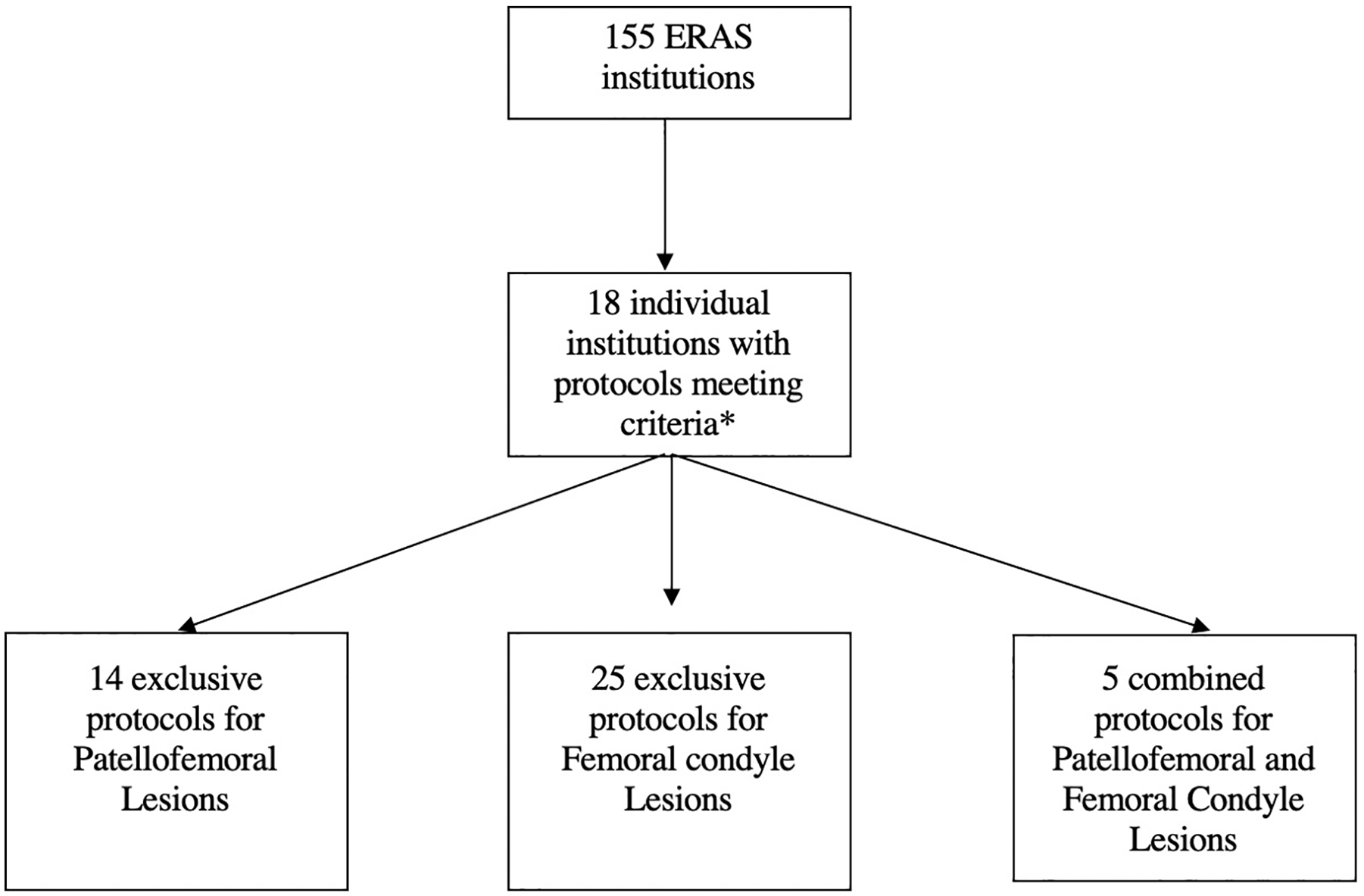
Collection of online postoperative rehabilitation protocols following microfracture of the knee.
Prehabilitation
For femoral condyle lesions, 2 protocols (6.7%) recommended a preoperative rehabilitation program including stationary cycling to maintain or improve ROM while 1 protocol (3.3%) provided recommendations on methods to decrease swelling with cryotherapy.
For patellofemoral lesions, 2 protocols (10.5%) recommended a preoperative rehabilitation program involving stationary cycling while 1 protocol (5.3%) included recommendations for cryotherapy use. No information on the timing, progression criteria, or treatment endpoints were indicated in any protocol for the use of stationary cycling or cryotherapy.
Postoperative Adjunct Therapy
The 8 types of postoperative adjunct therapies assessed were bracing, continuous passive motion (CPM), neuromuscular electric stimulation (NMES), cryotherapy, compression, elevation, ultrasound therapy, and thermotherapy. For femoral condyle lesions, 29 protocols recommended CPM (96.7%), 3 recommended electrical stimulation (10.0%), 5 recommended cryotherapy (16.7%), 4 recommended compression (13.3%), and 3 recommended elevation (10.0%), while ultrasound therapy and thermotherapy were recommended in 1 protocol each (3.3%). All aforementioned modalities began in the immediate postoperative period. In terms of bracing, 17 (56.7%) protocols recommended immediate postoperative bracing for an average of 7.5 weeks (range, 2-12; median 8 weeks) of brace use. Fifteen protocols (50.0%) specifically mentioned locking the brace during ambulation. In the protocols that did not recommend bracing, there were no explicit recommendations for or against bracing. Unlocking the brace during ambulation was recommended in 12 protocols (40.0%) at an average of 4.8 weeks (range, 0-8; median 6 weeks), postoperatively.
Six protocols (20.0%) specified when to discontinue brace use. The most common criterion for brace removal was the ability to perform a straight-leg raise (SLR) without extension lag at the knee (10.0%). Other recommended criteria for brace removal included the ability to perform 20 repetitions of an SLR without extensor lag (3.3%), the achievement of “full quadriceps control” (3.3%), and per individual surgeon evaluation (3.3%).
Following microfracture of patellofemoral lesions, 18 protocols recommended CPM (94.7%), 4 recommended immediate cryotherapy (21.1%), 3 recommended compression (15.8%), while electrical stimulation and elevation was recommended in 2 protocols (10.5%) each. In terms of bracing, 17 (89.5%) protocols recommended immediate postoperative bracing with an average of 7.1 weeks (range, 1-12; median 8 weeks) of brace use. Thirteen protocols (68.4%) mentioned locking the brace in full extension during ambulation. Unlocking of the brace during ambulation was suggested in 15 protocols (78.9%), at an average of 4.2 weeks (range, 0-8; median 6 weeks) postoperatively.
Five protocols related to patellofemoral lesions (26.3%) offered criteria for when to discontinue brace wear, with the most common parameter being the ability to perform an SLR without extensor lag (15.8%). Additional protocols cited the ability to perform 20 repetitions of SLR without lag (5.3%), and the presence of “full quadriceps control” (5.3%) as indicators of when brace wear can be discontinued.
Range of Motion and Weight-Bearing
Of the 30 protocols specific to femoral condyle lesions, 21 (70.0%) restricted any flexion of the knee immediately postoperatively, 5 (16.7%) permitted 90° of flexion at an average of 1.6 weeks (range, 0-6; median 1 week) postoperatively, 4 (13.3%) allowed 120° of knee flexion at an average of 4.0 weeks postoperatively (range, 2-6; median 4 weeks), and 25 (83.3%) protocols allowed full knee flexion at a mean of 6.8 weeks (range, 0-8; median 8 weeks). A weight-bearing progression, transitioning from non-weight-bearing, to weight-bearing as tolerated (WBAT) and “full weight bearing” (FWB) was clearly described in 18 out of the 30 protocols (60.0%) specific to femoral condyle lesions. In the analyzed protocols, WBAT was defined as the ability to support at least 50% of their body weight during ambulation, while FWB was defined as a patient’s ability to support 100% of their bodyweight. 32 Immediate weight-bearing was permitted in 11 protocols (36.7%), while 18 (60%) suggested WBAT with full knee ROM at an average of 7.3 weeks (range, 4-12; median 8 weeks) postoperatively. The average time to the initiation of WBAT across all femoral condyle-based protocols was 6.1 weeks (range, 0-8; median 8 weeks). The average time to expected FWB was 9.0 weeks (range, 4-16; median 8 weeks) postoperatively ( Fig. 2 ).
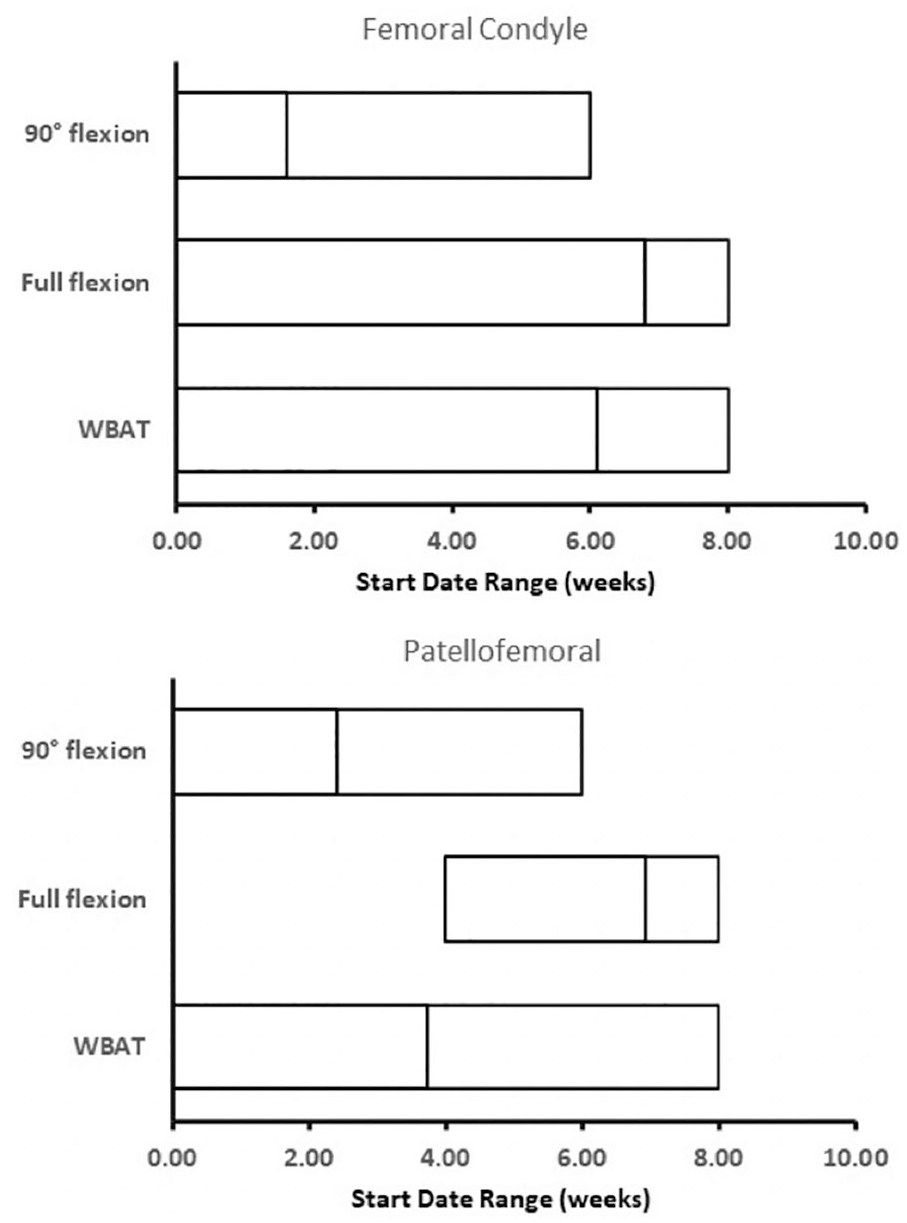
Range of motion and weight-bearing. The numbered line within each range represents the mean of the data set. WBAT = weight-bearing as tolerated; FWB = full weight-bearing.
Of the 19 protocols for patellofemoral lesions, 17 (89.5%) restricted any flexion of the knee in the immediate postoperative period, 5 (26.3%) permitted 90° of flexion at a mean of 2.4 weeks (range, 0-6; median 1 week), 2 (10.5%) allowed 120° of flexion at a mean of 5.0 weeks (range, 4-6; median 5 weeks), and 15 (78.9%) recommended full flexion at an average of 6.9 weeks (range, 4-8; median 8 weeks) postoperatively. A weight-bearing progression was clearly outlined in 9 (47.4%) protocols. Immediate weight-bearing was permitted in 10 protocols (52.6%), while WBAT with full knee ROM was recommended in 18 protocols (94.7%) at an average of 7.2 weeks (range, 4-12; median 8 weeks) postoperatively. The average time to WBAT was 3.7 weeks (range, 0-8; median 8 weeks) postoperatively while the average time to FWB was 7.7 weeks (range, 0-12; median 8 weeks; Fig. 2 ).
Strengthening
Eighteen different strengthening exercises were included in our custom rubric. Closed chain exercises, quadriceps and hamstring sets, and SLRs were recommended in more than 50% of all femoral condyle protocols. Time to initiation of strengthening exercises varied over a range of 12 weeks. The timing of hip abduction exercises occurred at an average of 4.8 weeks postoperatively (median 6 weeks), hip adduction at an average of 6.3 weeks (median 6 weeks), hamstring curls at an average 4.8 weeks (median 8 weeks), and open chain exercises at 7.4 weeks over the 12-week range (median 6 weeks; Fig. 3 ).
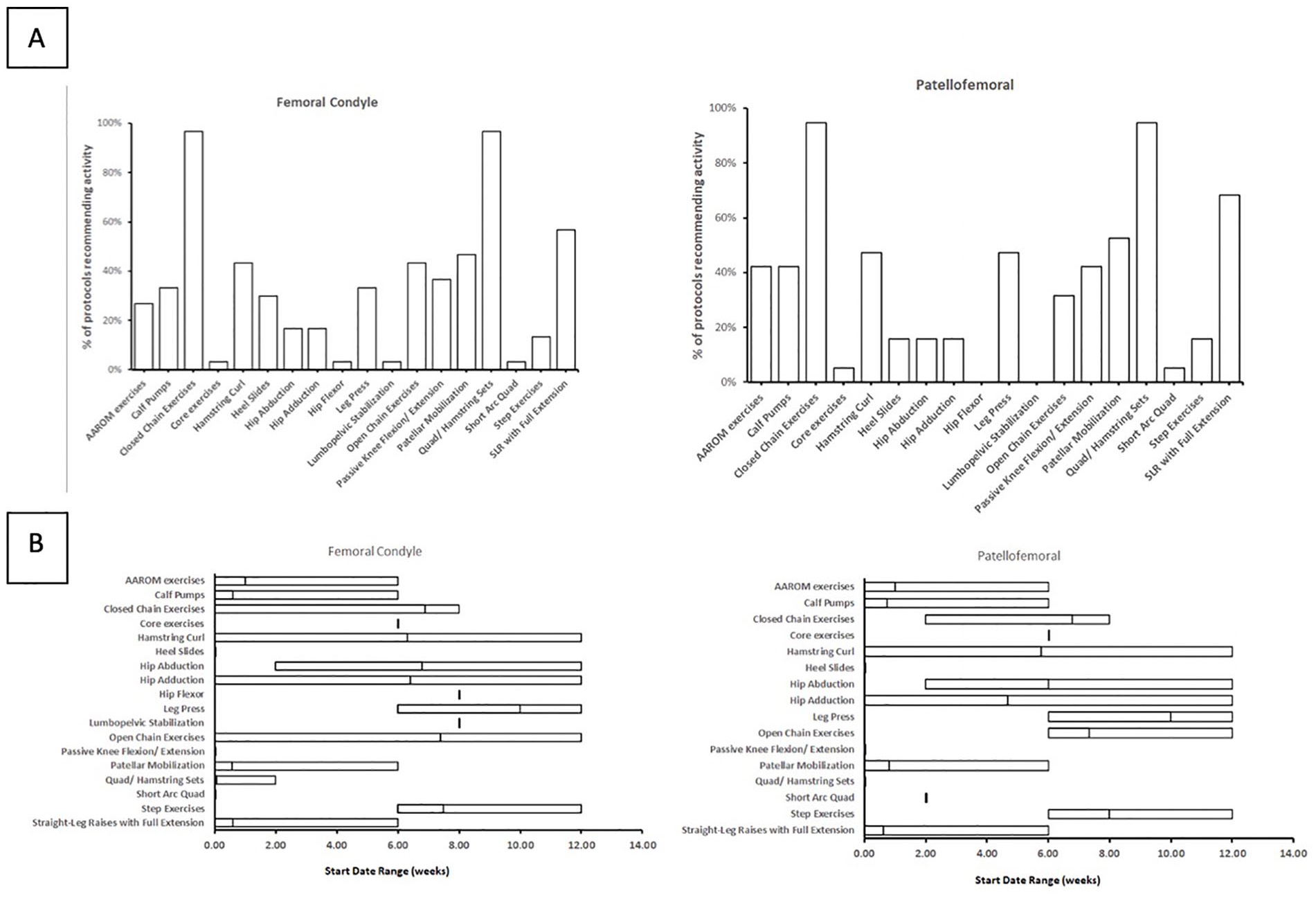
Strengthening exercises. (
Quadriceps and hamstring sets, closed chain exercises, SLRs, and patellar mobilization exercises were recommended in more than 50% of patellofemoral specific protocols. Similar to femoral condyle lesions, there was variation in the time to initiation of strengthening exercises over a 12-week range. The largest ranges were found in the timing of hip adduction (average 4.7 weeks; median 6 weeks) and hamstring curl (average 5.8 weeks; median 8 weeks) over a 12-week time range. On average, hip abduction exercises occurred at 4.0 weeks (median 6 weeks) postoperatively and started over a 10-week time range ( Fig. 3 ).
Proprioception and Functional Testing
Four different proprioceptive exercises were found within the reviewed protocols: unilateral stance activities, balance training, “weight shifting” exercises, and unspecified proprioceptive drills. For femoral condyle lesions, at least one proprioceptive exercise was recommended in 24 protocols (80%), and the average number of proprioceptive drills recommended was 1.4 per protocol. Balance training was recommended in 21 protocols (70.0%), unspecified proprioceptive drills were recommended in 15 protocols (50.0%), unilateral stance activities were recommended in 7 protocols (23.3%), and “weight shifting exercises” was recommended in 3 protocols (10.0%; Fig. 4 ).
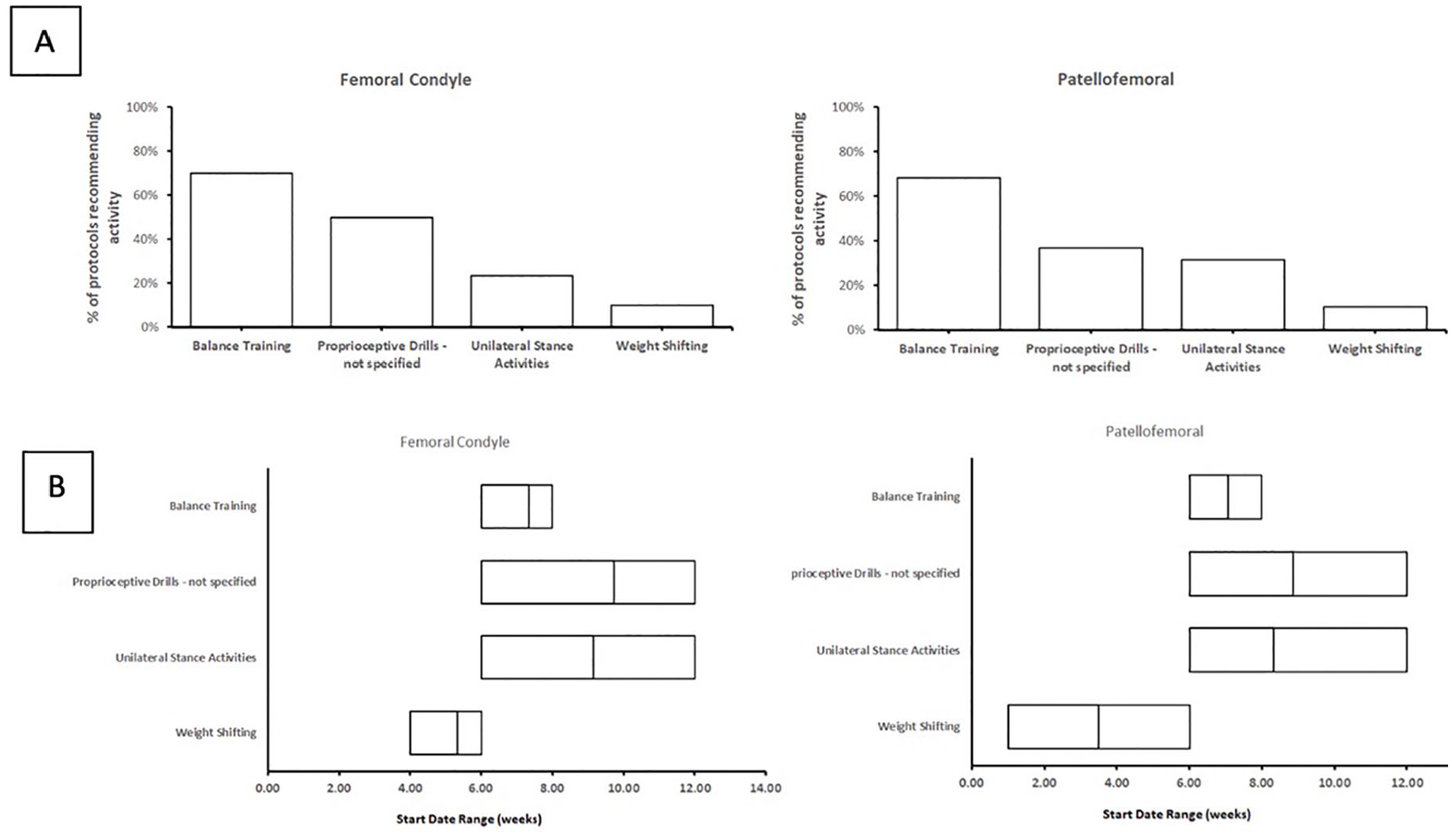
Proprioception exercises. (
For patellofemoral lesions, at least one proprioceptive exercise was recommended by 15 protocols (78.9%), and the average number of proprioceptive drills recommended was 1.5 per protocol. Balance training was recommended in 13 protocols (68.4%), unspecified proprioceptive drills were recommended in 7 protocols (36.8%), unilateral stance activities were recommended in 6 protocols (31.6%), and “weight shifting” exercises were recommended in 2 protocols (10.5%; Fig. 4 ).
“Weight shifting” exercises were recommended at an earlier time postoperatively for patellofemoral lesions (range, 1-6; median 6 weeks) compared to femoral condyle lesions (range, 4-6; median 3.5 weeks). However, there was a similar start time for the remaining proprioceptive exercises (i.e., unilateral stance training, balance training, and unspecified proprioceptive drills) for both femoral condyle and patellofemoral lesions at 6 weeks.
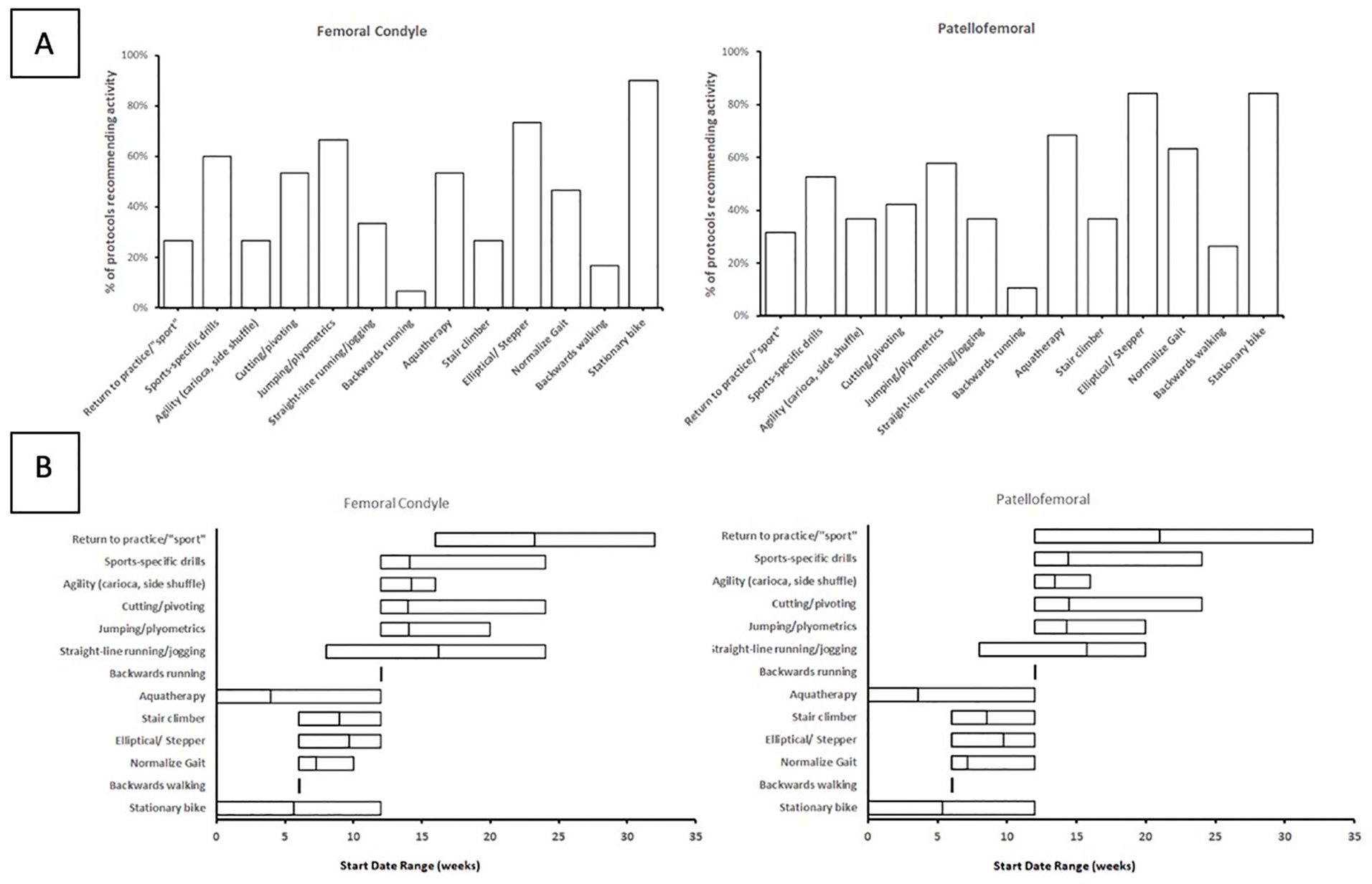
Return to Basic Activities and Sports
For femoral condyle lesions, higher level exercises were implemented as patients approached a return to baseline activities. Exercises included stationary bike use (90% of protocols) at an average of 5.6 weeks (range, 0-12; median 6 weeks), use of an elliptical or stair machine (73% of protocols) at an average of 9.7 weeks (range, 6-12; median 9 weeks), hydrotherapy (53% of protocols) at an average of 3.9 weeks (range, 0-12; median 3 weeks), and gait training (47% of protocols) at an average of 7.3 weeks (range, 6-10; median 6 weeks). Plyometrics were suggested in 67% of protocols starting at a mean of 14.3 (range, 12-20; median 12 weeks) weeks postoperatively. Agility and cutting exercises were started at a mean of 14.2 (range, 12-16; median 15 weeks) and 14.0 (range, 12-24; median 15) weeks, respectively. Sports-specific drills were recommended in 18 protocols (60.0%) and started at an average of 14.1 (range, 12-24; median 12) weeks postoperatively. Information on return to practice or sport was presented in 8 protocols (26.7%) with projected average dates for return to sport at 23.3 (range, 12-32; median 24) weeks postoperatively. Criteria for return to sport was based on individual physician decision in 9 protocols (30.0%) and functional performance testing in 10 protocols (33.3%). No protocols explicitly discussed timing for return to competition ( Fig. 5 ). Analyzed protocols did not provide clear instructions for limitations of athletic activities or criteria-based progressions for a return to training.
(
Of the postoperative functional assessments pertaining to rehabilitation progression for microfracture of femoral condyle lesions, 6 protocols (20%) included the single hop test, 5 protocols (16.7%) included isokinetic quadriceps strength testing, 3 protocols (10%) included balance testing, and 1 protocol (3.3%) each included isokinetic hamstring strength testing, squat testing, and “forward step-down testing.” Four protocols (13.3%) mentioned the use of functional assessments; however, they did not include explicit information on the testing measures included. All testing was recommended between 12 and 18 (median 14) weeks postoperatively, except for balance testing, which was recommended at an average of 6 weeks (range, 6; median 6 weeks).
For patellofemoral lesions, recommended exercises included the stationary bike (84% of protocols) at an average of 5.4 (range, 0-12; median 6) weeks postoperatively, elliptical or stair machine use (84% of protocols) at an average of 9.8 (range, 6-12; median 10) weeks, hydrotherapy (68% of protocols) at a mean of 3.6 (range 0-12; median 3) weeks, and gait training (63% of protocols) at an average of 7.2 (range, 6-12; median 6) weeks. Plyometrics were recommended in 58% of protocols, starting at an average of 14.3 (range, 12-20; median 12) weeks. Agility and cutting exercises were started at an average of 13.4 (range, 12-16; median 12) and 14.5 (range, 12-24; median 12) weeks, respectively. Ten protocols (52.6%) recommended sports-specific drills starting at a mean of 14.4 (range, 12-24; median 12) weeks. Six protocols (31.6%) explicitly mentioned an expected return to practice or sport at an average of 21.0 (range, 12-32; median 21) weeks. Criteria for return to sport was based on physician decision in 5 protocols (25.0%) and successful completion of a functional performance assessment in 4 protocols (20.0%). No protocols explicitly discussed timing for a return to competition ( Fig. 5 ). Of the analyzed protocols, none provided clear instructions for athletic activities or establish criteria-based progression for return to training.
Of the 4 patellofemoral protocols utilizing functional testing to assess rehabilitation progression, 4 (21.1%) included single hop testing, 2 (10.5%) utilized balance testing, and 1 (3.3%) protocol each recommended isokinetic quadriceps strength testing, squat testing, and forward step-down testing. Four protocols (21.1%) mentioned the inclusion of functional performance testing but did not explicitly discuss the individual testing measures. Similar to femoral condyle lesions, all functional performance testing was recommended between weeks 12 and 18 (median 14), postoperatively, except for balance testing which was recommended at an average of 6 weeks (range, 6 weeks; median 6).
Discussion
The results of this study show that a minority of academic orthopedic programs publish microfracture rehabilitation protocols online. Of the protocols available, there is variation within the modalities recommended and the timing of their initiation. These findings further suggest that a standardized protocol does not exist. The most consistent modalities included in the reviewed protocols were the usage of CPM following microfracture of both patellofemoral (94.7%) and condylar (96.7%) lesions, restriction of knee flexion (70.0% for condylar lesions, 89.5% for patellofemoral lesions), and brace use (56.7% for condylar lesions, 89.5% for patellofemoral lesions). While most protocols included recommendations on strength training or the inclusion of proprioceptive training, there was disagreement on the timing and inclusion of specific exercises during the rehabilitation process. Additionally, disagreement was found on postoperative weight-bearing restrictions, length of brace use, and a minority of protocols provided information on weight-bearing progressions, timing for return to sport, or functional assessments for return to sport, independent of the location of the chondral injury.
Range of Motion
Following knee surgery, flexion contractures and stiffness are common complications. 27 After microfracture surgery, adhesions may develop around the anterior, medial, and lateral aspects of the knee and restrict ROM. 17 However, allowing ROM to prevent stiffness must be balanced with preventing excessive motion and disruption of healing. Although passive knee ROM was allowed postoperatively, immediate restrictions in active knee flexion was recommended across most postoperative protocols following microfracture of both patellofemoral and condylar lesions. To date, most investigations on early active ROM following cartilaginous procedures have been centered on mixed results of animal studies33-35 with only minimal clinical investigations available to support early active motion.36,37
Pervasive use of CPM postoperatively was a consistent modality found in most rehabilitation protocols as an aid to regain motion. The use of CPM has been favorably supported following articular cartilage repair in animal-based studies as it has been shown to increase synovial fluid movement and joint surface articulation during a time when patients may suffer negative effects from prolonged periods of restricted postoperative weight-bearing.38-41 Although outcomes have been studied with CPM use following ACL reconstruction, similar to the literature done on active ROM postoperatively, relatively few clinical studies have evaluated CPM following articular cartilage repair.42,43 Following microfracture, Rodrigo et al. noted significant improvements in cartilage lesion scores across patients who used CPM postoperatively. 44 However, the retrospective design of this study, poor matching between comparative groups, and the lack of patient-reported outcomes limit the clinical utility of this investigation. Marder et al. later found no significant differences in retrospectively collected Lysholm knee rating scores, Tegner activity scores, radiographic data, or clinical exam data such as ROM, pain, or a return to activity with CPM use. 37 Furthermore, variation in studies on the CPM dosing and total length of usage remains unclear.39,45 As such, the proposed benefits of CPM usage, and potentially the rationale for their inclusion in academic rehabilitation protocols, appear to be largely based on significantly favorable data from basic science investigations although little clinical evidence has been found to support their usage clinically. In fact, CPM use following arthroscopic knee surgery was recently questioned in Gatewood et al.’s systematic review as no differences in postoperative ROM or pain relief were found postoperatively in their investigation. 46
Weight-Bearing
Postoperative weight-bearing restrictions are implemented in order to protect the fibrocartilaginous clot created by microfracture surgery. For condylar lesions, avoiding compressive forces on the weight-bearing surface of the knee is paramount, while the avoidance of shearing forces is integral for the healing of patellofemoral lesions. 17 However, overly cautious limitations in weight-bearing and prolonged immobilization have been linked to reduced proteoglycan synthesis and thinning of the articular cartilage in several studies.39,47-50 Among the publicly available rehabilitation protocols analyzed, patients were expected to achieve full-weight-bearing status at an average of 9.0 weeks postoperatively with condylar lesions; however, the suggested timing of full weight-bearing across studied protocols ranged from 4 to 16 weeks. Similarly, for patellofemoral lesions, full weight-bearing status was expected at an average of 7.7 weeks postoperatively, but timing across all patellofemoral protocols ranged from 0 to 12 weeks. Current literature suggests partial, or touch-down, weight-bearing for femoral condyle lesions for 6 to 8 weeks postoperatively, with advancement to full weight-bearing between 9 and 16 weeks.8,12,28 For patellofemoral lesions, present literature supports partial, or touch-down, weight-bearing immediately postoperatively, weight-bearing as tolerated at 0 to 2 weeks postoperatively, and promotion to full weight-bearing between 9 and 16 weeks.8,12,28 As it stands, the online protocols analyzed in our investigation report timelines slightly differ from those present in literature. Schmitt et al.’s systematic review on outcomes following articular cartilage surgery proposed that rather than using time as a factor for weight-bearing progression, clinical signs indicating joint overload, such as effusion or muscle strength/deficits, may serve as more reliable criteria for decision making. 51 Despite their recommendation, the authors note that optimal loads to facilitate cartilaginous healing and subsequent favorable outcomes remain unknown. 51 Ultimately, decisions on the optimal timing of postoperative weight-bearing still merit further investigation. However, until these data are available, academic programs should aim to provide clearly synthesized, evidence-based protocols so providers can better guide patients on when and how to progress weight-bearing in order to minimize undue stress to the healing cartilage.
Prehabilitation
Prehabilitation has been proposed in the literature as an intervention geared toward improving muscle function, muscle strength, mentally preparing patients for the postoperative follow-up period, and to decrease pain preoperatively. 52 Our investigation found a minority of protocols prescribing a course of prehabilitation before microfracture surgery with minimal inclusion of stationary biking or recommendations for the use of cryotherapy. Although prior studies in the arthroplasty and ACL literature propose limited improvements in clinical outcomes and a faster completion of the rehabilitation process following the institution of a prehabilitation protocol, the outcomes of prehabilitation protocols prior to surgical management of articular cartilage lesions remain scarce.52,53 Hirschmüller et al. suggest a prehabilitation protocol, based on available literature, that is geared toward improving neuromuscular control, general fitness, reducing joint effusion, and considerations toward each patient’s pain level. Yet the clinical efficacy of their proposed program remains unknown and highlights the need for further investigation. 52
Postoperative Adjunct Therapy
Brace use was found to be one of the most common postoperative adjuncts following both femoral condyle and patellofemoral microfracture. However, variations exist in terms of how bracing should be managed postoperatively as half of the protocols related to the femoral condyle offered no recommendations on bracing while the majority of protocols for patellofemoral lesions recommended brace use postoperatively. Furthermore, for both lesions, a minority of protocols provided criterion for when to discontinue brace use.
Locked bracing after articular cartilage surgery is theoretically intended to prevent abnormal joint arthokinematics and which can have downstream effects on patellofemoral and tibiofemoral joint contact pressures. 54 For patellofemoral lesions, Mithoefer et al. proposed a course of brace wear with the knee locked in full extension for 4 to 6 weeks; however, the authors note that there is currently no evidence-based consensus supporting this recommendation. 55 This proposed time course for bracing appears consistent with time course seen in our investigation as unlocking of the brace was allowed at an average of 4.2 weeks postoperatively, although overall, protocols recommended unlocking of the brace anywhere between 0 and 8 weeks. At this time, literature is lacking on supporting time lengths for bracing, time points for when motion is allowed with the brace for femoral condyle lesions, or outcome data suggesting optimal timing for discontinuation of bracing.
Strength, Proprioception, and Functional Testing
The inclusion of quadriceps, hamstring, and closed chain exercises was fairly consistent across most analyzed protocols following microfracture of both femoral condyle and patellofemoral lesions. Current literature has recommended the institution of strengthening exercises between 4 and 12 weeks postoperatively, which is comparable to what was found across the online protocols studied. 16 Although no consensus exists on the inclusion of specific exercises for postoperative strengthening, general themes in the literature provide support toward an emphasis on correcting quadriceps-to-hamstring strength deficits as well as hip strength asymmetry. In addition to the lack of agreement on which exercises utilized in the rehabilitation process, the exact order in which these exercises should commence also remains unclear.16,19
Balance and proprioceptive exercises were common modalities included in both protocols for both femoral and patellofemoral lesions yet specifics regarding which exercises to include and timing have not been completely elucidated in the literature. A progression from activities performed using a bilateral stance to a unilateral stance has been proposed; however, criteria for this progression varies in the literature. For now it appears that these exercise are initiated once full ROM, improved gait, and adequate quadriceps strength relative to the contralateral side has been obtained, rather than strictly based on time from surgery, which was seen in most protocols included in our analysis.16,19
Return to Sport and Activity
Stationary bike or elliptical bike use was a very common exercises found across online rehabilitation protocols. Although protocols mention institution of such modalities at an average of 5.6 weeks, much of the variability contributing to their incorporation from 0 to 12 weeks postoperatively may have to do with the goals expected from their usage. For example, in the early postoperative period, biking and elliptical use may help improve ROM. 56 In other settings, biking and elliptical use could be considered low to moderate-impact activities geared toward improving cardiovascular health and function as patients near a return to full activity. 16 For those aiming for a return to high-level sport or activity, plyometrics can be instituted; however, its efficacy following articular cartilage surgery remains largely unknown. 26 Despite this, plyometrics were found in a majority of protocols after microfracture and patellofemoral lesions.
Only a minority of academic orthopedic programs included functional assessments for return to play in their postoperative rehabilitation protocols. Specifically, 13.5% of protocols following microfracture of condylar lesions and 20.0% of protocols following microfracture of patellofemoral lesions. Regardless, no protocols explicitly discussed timing for return to competition for either cartilage lesion. The lack of discrete timelines for return to play may be reflective of the variability seen in current literature as reported return to play rates range from 58% to 83% over periods ranging from 8 to 9.2 months.57-60 At the final stages of rehabilitation, patients should demonstrate readiness to return to practice/sports through functional and athletic activities, and more recent studies have supported the use of functional performance testing. Specifically, within the ACL literature, functional assessments for return to sport have largely replaced time-based decisions for return to play.61-64 However, there is presently a paucity of data on the effectiveness of functional testing assessments in assessing readiness to return to play following microfracture of the knee.
As more attention within the orthopedic literature becomes directed at standardizing care and treatment methodologies to improve outcomes, the results of our study highlight an opportunity to improve upon patient care following a relatively common procedure for the treatment of articular cartilage injury.60,65-68 Factors such as when to progress weight-bearing, which strength and proprioceptive exercises to implement postoperatively, and at what stages, as well as information guiding patients on return to play are necessary variables that can help patients monitor their postoperative progress while ensuring adequate recovery leading to favorable postoperative outcomes. Although elements of these variables exist in the rehabilitation protocols presented by reputable academic institutions today, there is minimal standardization and thus a need for further investigation to assess and to appropriately optimize recovery after microfracture surgery to chondral defects of the knee to ensure consistent and favorable clinical outcomes.
Limitations
This study has several limitations to note. First, only 44 protocols met qualification criteria and were included, despite all 155 academic programs being considered. This is only a microcosm of the postoperative microfracture rehabilitation protocols available online as private practice groups and individual physicians likely have personal websites where their own protocols can be found. However, our methodology followed previous investigations and specifically included protocols from academic institution as the authors suspect the information provided by these centers would be most likely evidence-based modalities and treatment approaches.23,27-29,31 Furthermore, many orthopedic surgeons design individualized protocols for patients, based on their preoperative condition and intraoperative decisions, which are then given directly to patients or physical therapists. As such, these individualized recommendations would not be captured by our review of the data currently online. Last, many of the rehabilitation protocols differed in the level of detail included. For example, many protocols explicitly indicated a timeframe for when patients should become weight-bearing as tolerated, yet some did not use this exact phrasing and instead indicated weight-bearing as percent of body weight. It can be inferred that discrepancies arising between the patient and the provider as a result of the lack of specific information were remedied on an individualized basis; however, as more patients begin to rely on multimedia and internet-based resources to monitor and guide their postoperative progress, it further highlights a fundamental need to improve the quality of the information made available online.
Conclusion
A minority of US academic orthopedic programs publish microfracture rehabilitation protocols online. Among the protocols currently available, there is significant variability in the inclusion of specific rehabilitation components and timing of many modalities. Evidence-based standardization of elements of postoperative rehabilitation may help improve patient care and subsequent outcomes.
Footnotes
Acknowledgments and Funding
We thank Cherry Aung, BBA, for her help with data analysis. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bryan M. Saltzman reports publishing royalties, financial or material support from Nova Science Publishers. Christopher S. Ahmad reports IP royalties, paid consultant and research support from Arthrex, Inc; paid consultant, research support, stock or stock options from At Peak; publishing royalties, financial or material support from Lead Player; research support from Major League Baseball; editorial or governing board at Orthopedics Today; and research support from Stryker. Charles A. Popkin reports financial or material support and research support from Arthrex, Inc.; financial or material support from Smith & Nephew; and is a Board or Committee member for USA Hockey Safety and Protective Equipment Committee. The remaining authors, Stephen G. Crowley, Hasani W. Swindell, and David P. Trofa, declare there is no conflict of interest to the prepared work.