
Abstract
Purpose
To evaluate autologous matrix-induced chondrogenesis (AMIC) for isolated focal retropatellar cartilage lesions and the influence of patellofemoral (PF) anatomy on clinical outcomes at a minimum of 2-year follow-up.
Methods
Twenty-nine consecutive patients (31 knees) who underwent retropatellar AMIC with a mean age of 27.9 ± 11.0 years were evaluated at a follow-up averaging 4.1 ± 1.9 years (range, 2-8 years). Patient factors, lesion morphology, and patient-reported outcome measures, including Knee Injury and Osteoarthritis Outcome Score (KOOS), Tegner, Kujula score, and visual analogue scale (VAS) score were collected. PF anatomy was assessed on pre- and postoperative imaging, and subsequently correlated to outcome scores and failure to determine risk factors for poor outcome.
Results
At final follow-up, the AMIC graft failed in 4 cases (12.9%) at a mean follow-up of 21 ± 14.1 months. Patients with failed grafts had a significantly smaller patellar and Laurins’s PF angle than patients whose graft did not fail (P = 0.008 and P = 0.004, respectively). Concomitant corrective surgery for patellar instability was performed in 29 knees (93.5%). Grafts that did not fail presented with an average Kujala score of 71.3 ± 16.9, KOOS Pain of 76.2 ± 16.6 and Tegner scores of 4.2 ± 1.8. The patellar angle was significantly associated with the patient’s satisfaction level (r = 0.615; P < 0.001).
Conclusion
AMIC for retropatellar cartilage lesions in combination with concomitant corrective surgery for patellar instability results in low failure rate with satisfactory clinical outcome and patient satisfaction of almost 80% at mid-term follow-up. As most failures occurred in patients without concurrent tibial tubercle osteotomy and both a smaller patellar and Laurins’s PF angle were associated with less favorable outcome, this study supports the growing evidence for the need of unloading retropatellar cartilage repair, when indicated.
Level of Evidence
Case series; level of evidence, 4.
Keywords
Introduction
Articular cartilage lesions of the knee are commonly found on magnetic resonance imaging (MRI) and reported in up to 2/3 of all knee arthroscopies.1,2 One-third of the lesions are located in the patellofemoral (PF) joint and are associated with pain, disability and can eventually progress to osteoarthritis.3,4 The pathomechanism of PF cartilage lesions is multifactorial, including direct trauma, PF dislocation, instability, and maltracking.5,6
Treating retropatellar chondral defects is particularly challenging due to the complex biomechanical circumstances with high loading stress on its surface. 7 Associated patho-anatomical morphologies are known causes for cartilage lesions and thus have to be addressed during treatment.5,8,9 Consequently, determining lesion etiology is crucial to define and initiate an individual treatment plan.
Various options exist for the treatment of focal cartilage lesions of the knee. 10 Primary treatment consists of nonoperative management with nonsteroidal anti-inflammatory medications, intra-articular corticosteroid injections, hyaluronic acid viscosupplementation, and physiotherapeutic strengthening and stretching of the thigh muscles.7,11 If symptoms persist, surgical therapy may be considered. Hence, various surgical techniques are available, but the optimal treatment remains controversial.12-19
A treatment option for contained retropatellar full-thickness cartilage lesions is autologous matrix-induced chondrogenesis (AMIC). The technique combines bone marrow stimulation of microfracturing and the augmentation of a collagen type I/III bilayer membrane to contain the subchondral bleeding and provide a matrix for repair tissue maturation. It has been shown effective for the treatment of cartilage lesions in the knee joint.20-22 However, results of AMIC for retropatellar cartilage lesions are only reported in small case series or are embedded in studies investigating AMIC for tibio- and patellofemoral lesions missing thorough subanalysis.23-27 Furthermore, evidence of factors influencing the outcome after retropatellar AMIC is lacking, especially the effect of recently determined risk factors for PF cartilage lesions, including trochlear dysplasia, patella alta, and excessive lateral tilt remains unknown. 9
The purpose of this study was therefore to report the clinical outcome of AMIC for isolated focal retropatellar cartilage lesions and to evaluate the influence of PF anatomy. It was hypothesized that AMIC would generally result in favorable mid-term clinical outcomes, yet individual PF anatomy significantly affects patient outcome.
Materials and Methods
Ethical approval (No. 2020-01052) was granted by the local research ethics committee and all included patients gave their written consent.
Patients
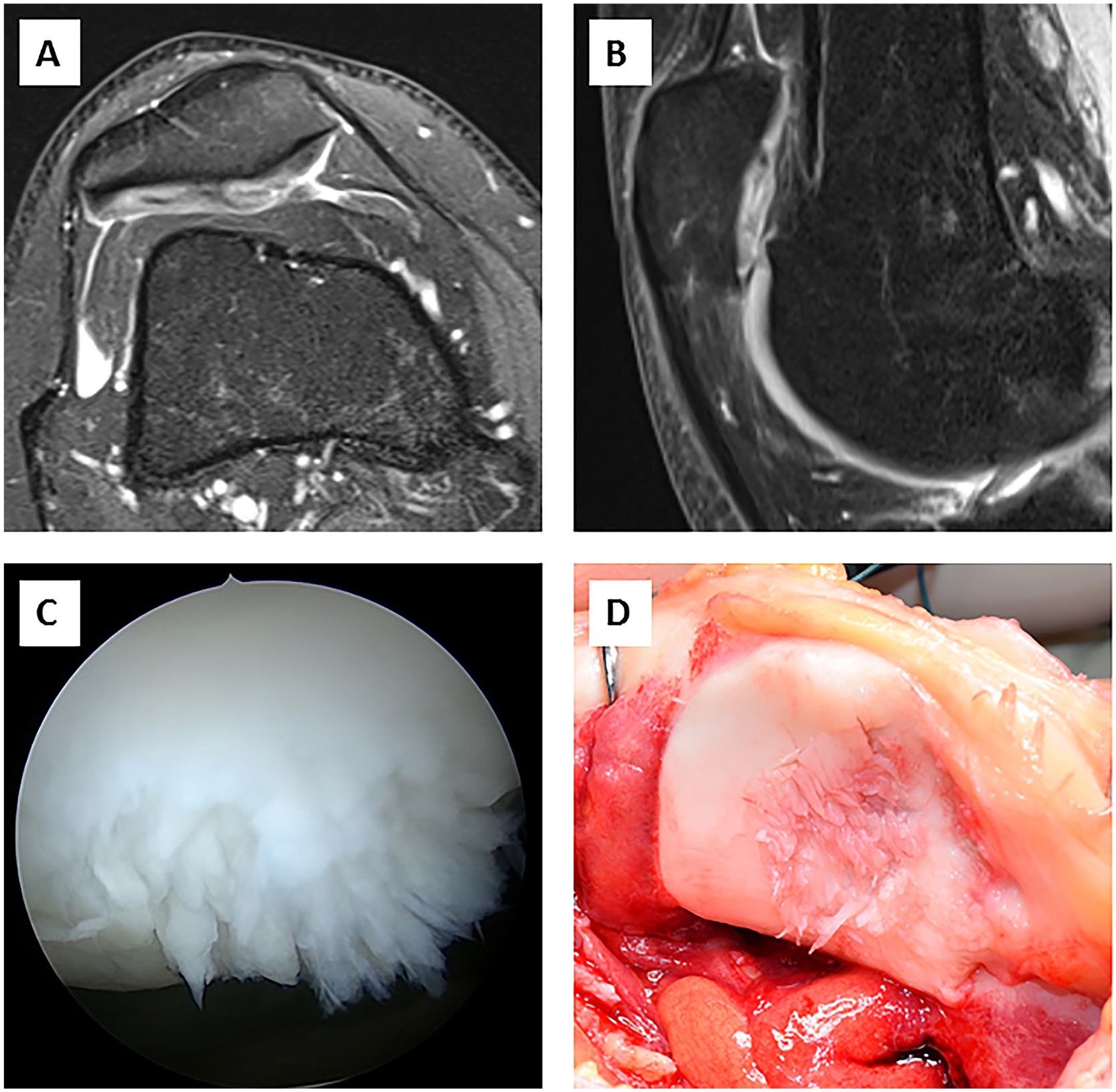
A total of 36 consecutive patients (38 knees) underwent retropatellar cartilage repair with AMIC for isolated focal full-thickness chondral lesions (Outerbridge type III and IV) of the patella at our institution between August 2013 and June 2018. 28 The treatment with AMIC was indicated in patients with (1) symptomatic contained retropatellar cartilage lesion with fissuring to the level of subchondral bone and (2) failed conservative management which was initiated for a minimum of 3 to 6 months ( Fig. 1 ). Exclusion criteria comprised advanced osteoarthritis, inflammatory joint diseases, and infection. To minimize confounding, 2 patients with concomitant high tibial and distal femur osteotomies were excluded from the study. A total of 5 patients (5 knees, 14%) were not available for follow-up; Three refused to participate and 2 could not be traced. According to telephone or chart review, none of the 5 patients had undergone revision surgery. Thus, this study included 29 patients (31 knees) that received retropatellar AMIC with a minimum follow-up of 2 years.
(
Clinical and Radiographic Assessment
Clinical notes and operative reports were reviewed to determine patient’s age at the time of surgery, sex, body mass index (BMI), smoking status, previous surgery, concomitant surgical procedures, defect size, location, lesion location type according to Fulkerson, 29 etiology, complications, and reoperations.
Patients were contacted and asked for any complications or reoperations since the initial procedure. Clinical outcomes were evaluated using patient-reported outcome measures (PROMs), including Tegner activity score, 30 Knee Injury and Osteoarthritis Outcome Score (KOOS) with its subscales, 31 Kujula score, 32 and visual analogue scale (VAS) pain score. 33 Patients rated their overall postoperative outcome as “excellent,” “good,” “fair,” or “unsatisfactory.”
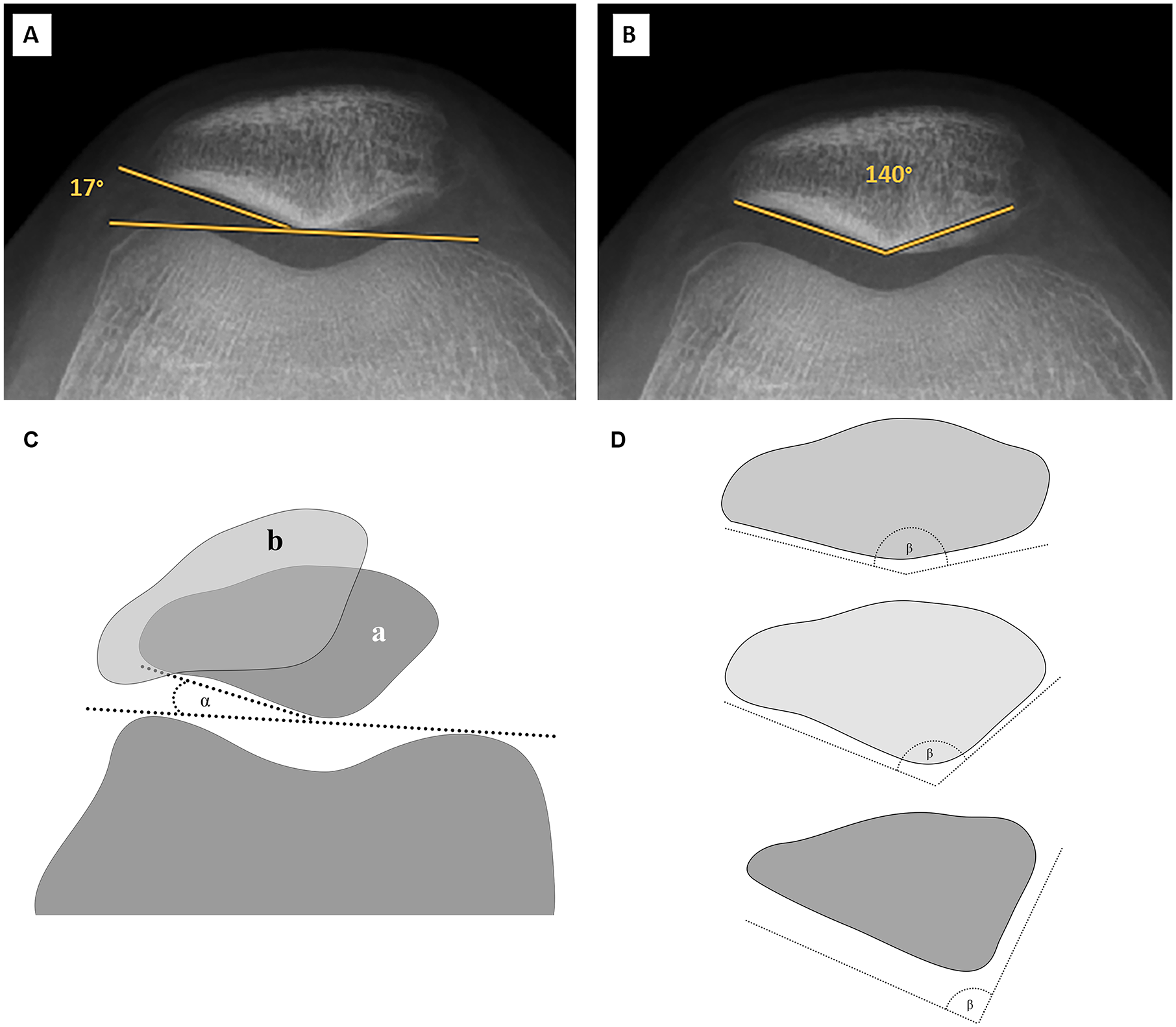
Radiographic analysis on preoperative MRI, radiograph, and orthoradiogram in all patients consisted of assessment of tibial tubercle trochlear groove (TTTG) distance, 34 Caton-Deschamps index (CDI), 35 Laurins’s PF angle, 36 trochlear sulcus angle, 37 Merchants’s congruence angle, 38 sulcus depth, 39 patellar angle, 40 PF index, 41 patella morphology according to Wiberg, 42 and degree of trochlea dysplasia according to Dejour.43,44 Postoperative radiographic analysis was based on standard radiograph of the knee in all patients and MRI if available.
All images were analyzed by two independent observers (M.W. ad C.S). In the event of disagreement, a third observer (J.A.) assessed the images to achieve consensus.
Surgical Technique and Postoperative Care
All patients’ cartilage lesions were accessed via arthrotomy through an open approach.
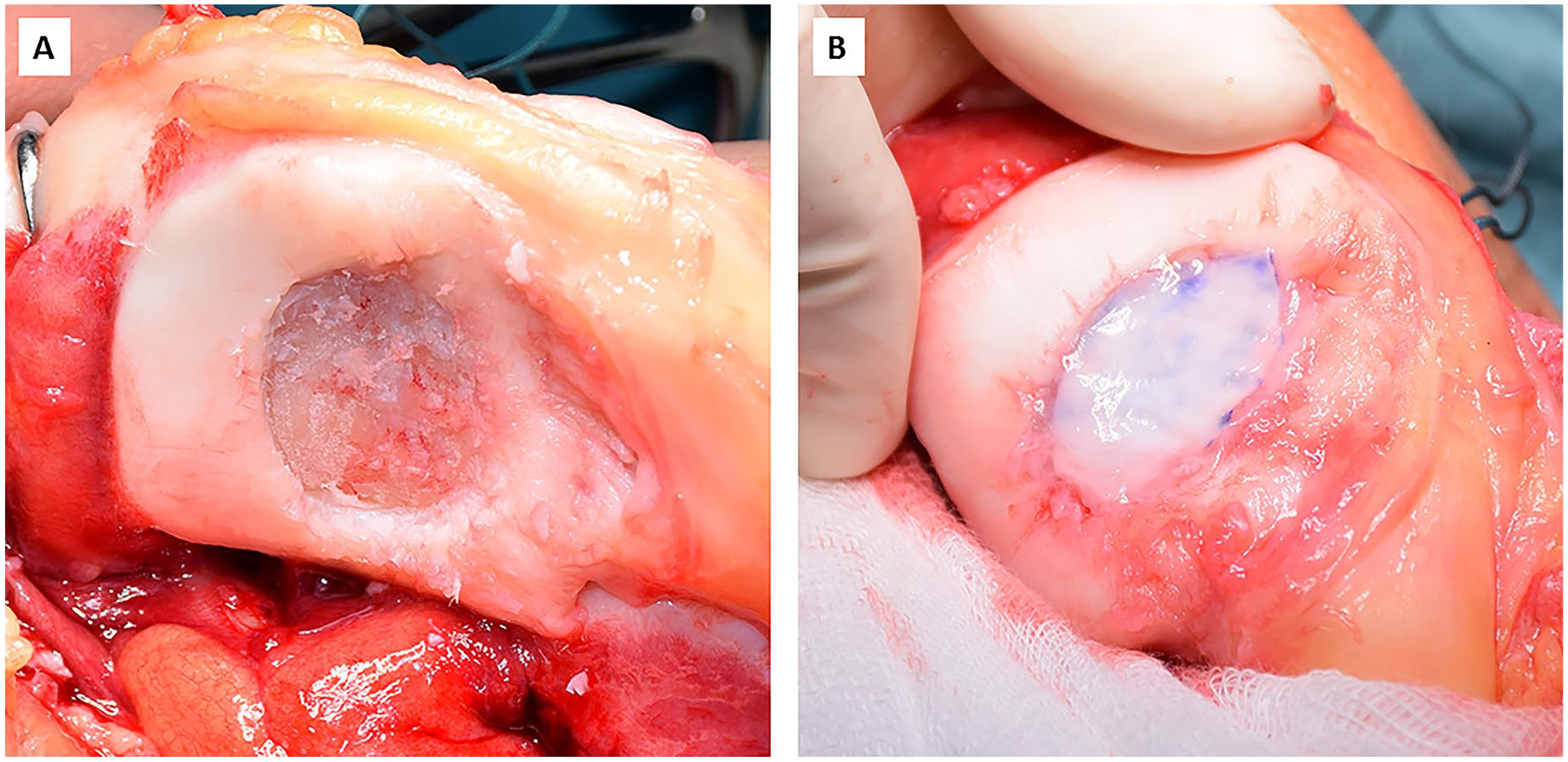
First, the retropatellar cartilage defect was identified and carefully debrided creating a defect with vertical walls. Necrotic/cystic bone was excised until vital bone tissue was visible. Then, microfracturing of the bone was achieved by drilling with an awl or K-wire (Ø 1.2 mm, DePuy Synthes, Oberdorf, Switzerland). In case of a large bony defect, the joint surface of the patella was reconstructed with autologous cancellous bone from the ipsilateral tibia or femur. Thereafter the bilayer type I/III collagen matrix (Chondro-Gide, Geistlich Pharma AG, Wolhusen, Switzerland) was cut to fit the defect and placed on the lesion. After complete coverage of the defect, surgical fibrin glue was applied to secure the membrane to the adjacent cartilage (Tissucol Duo S, Baxter International Inc., Deerfield, IL) ( Fig. 2 ). To ensure stable membrane fixation, the joint was brought through full range of motion. Concomitant corrective surgery for patellar instability was performed as indicated. Arthrotomy was closed using running absorbable sutures followed by standard wound closure.
(
Postoperative Rehabilitation
After surgery, patients were immobilized in a knee brace for the immediate postoperative period. After 2 days, protected partial weightbearing was allowed with the knee in a dynamic brace for the first 6 weeks. Stepwise increase of active and passive range of motion was emphasized during that time to avoid arthrofibrosis. After 6 weeks, the brace was removed and full weightbearing was allowed. Return to sport was permitted by 6 to 9 months postoperatively, depending on the sport (running vs. cutting sports).
Definition of Failure
Patients who presented with persistent pain and therefore underwent revision procedures such as autologous chondrocyte implantation, osteochondral grafting, microfracture, arthroplasty, or failure of more than 25% of the graft, were considered a failure. This definition was previously utilized for autologous chondrocyte implantation grafts and served to provide standardization and improve comparability.6,45-47
Statistical Analysis
Sociodemographic and clinical characteristics of patients were determined using descriptive statistics. All data were assessed for normality utilizing the Shapiro-Wilk test. Subsequently, continuous variables were analyzed with the independent t test or Mann-Whitney U test. Categorical variables were assessed with the chi-square or Fisher’s exact test. The Friedman test was utilized to analyze the course of patient activity (Tegner score) from preinjury to pre- and postoperatively. Clinical improvement measured by the Kujala score was analyzed with the paired t test. Pearson correlation was used to assess the relationship of anatomical parameters and clinical scores. Interobserver reliability was assessed with the Cohen’s kappa coefficient (κ) for patellar and trochlear dysplasia, and with the intraclass correlation coefficient (ICC) for TTTG, Laurins’s PF angle, CDI, patellar angle, PF index and congruence angle, trochlear sulcus depth and angle. All statistical analyses were performed in SPSS for Mac (Version 23.0, SPSS Inc., IBM Corp, Armonk, NY). Significance was set at P < 0.05. A post hoc power analysis showed that with a sample size of 31 knees, the study had a power of 0.84 to detect a large effect size (r = 0.5) in the relationship between anatomical parameters and clinical outcome on a level of significance of 0.05. Power calculation was performed with G-power version 3.1.
Results
The reviewed cohort included 31 knees of 29 patients with a mean age at the time of surgery of 27.9 ± 11.0 years and a BMI averaging 25.4 ± 5.5 kg/m2. Of these, 29 knees (93.5%) underwent concomitant corrective surgery for patellar instability ( Table 1 ). The mean postoperative clinical follow-up was 4.1 ± 1.9 years. While 9 knees (29%) had prior knee surgery, of which 7 (22.6%) had cartilage surgery (4 debridement, 2 mosaicplasty, and 1 chondral flake refixation), the remaining 21 knees (67.7%) received primary retropatellar AMIC. A history of patellar dislocation was present in 20 knees (64.5%) with recurrent dislocations in 16 knees (51.6%). Traumatic injury without patellar dislocation was reported in 4 knees (12.9%) ( Table 2 ).
Demographics and Treatment of the Patient Cohort.
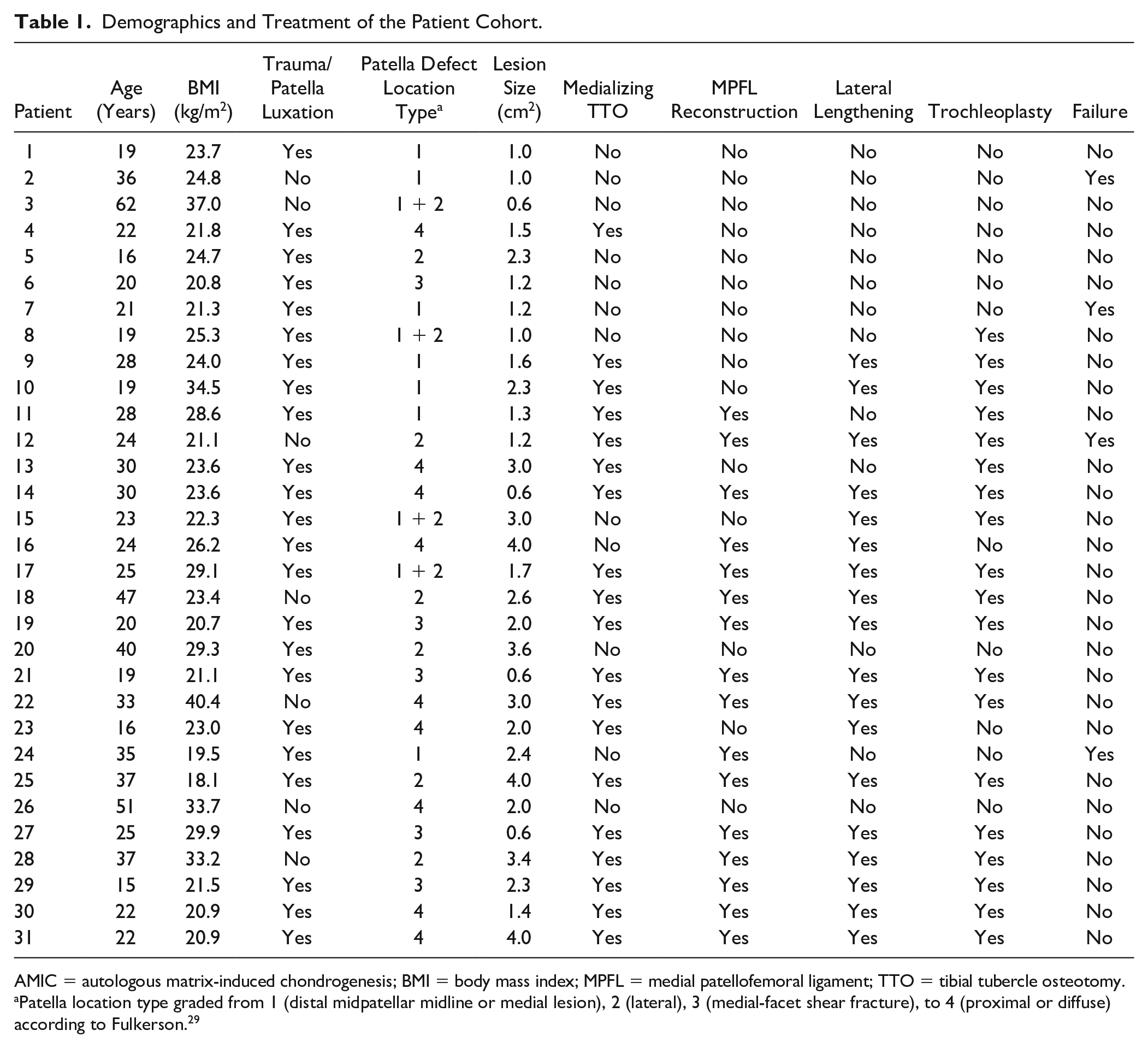
AMIC = autologous matrix-induced chondrogenesis; BMI = body mass index; MPFL = medial patellofemoral ligament; TTO = tibial tubercle osteotomy.
Patella location type graded from 1 (distal midpatellar midline or medial lesion), 2 (lateral), 3 (medial-facet shear fracture), to 4 (proximal or diffuse) according to Fulkerson. 29
Patient and Lesion Characteristics.
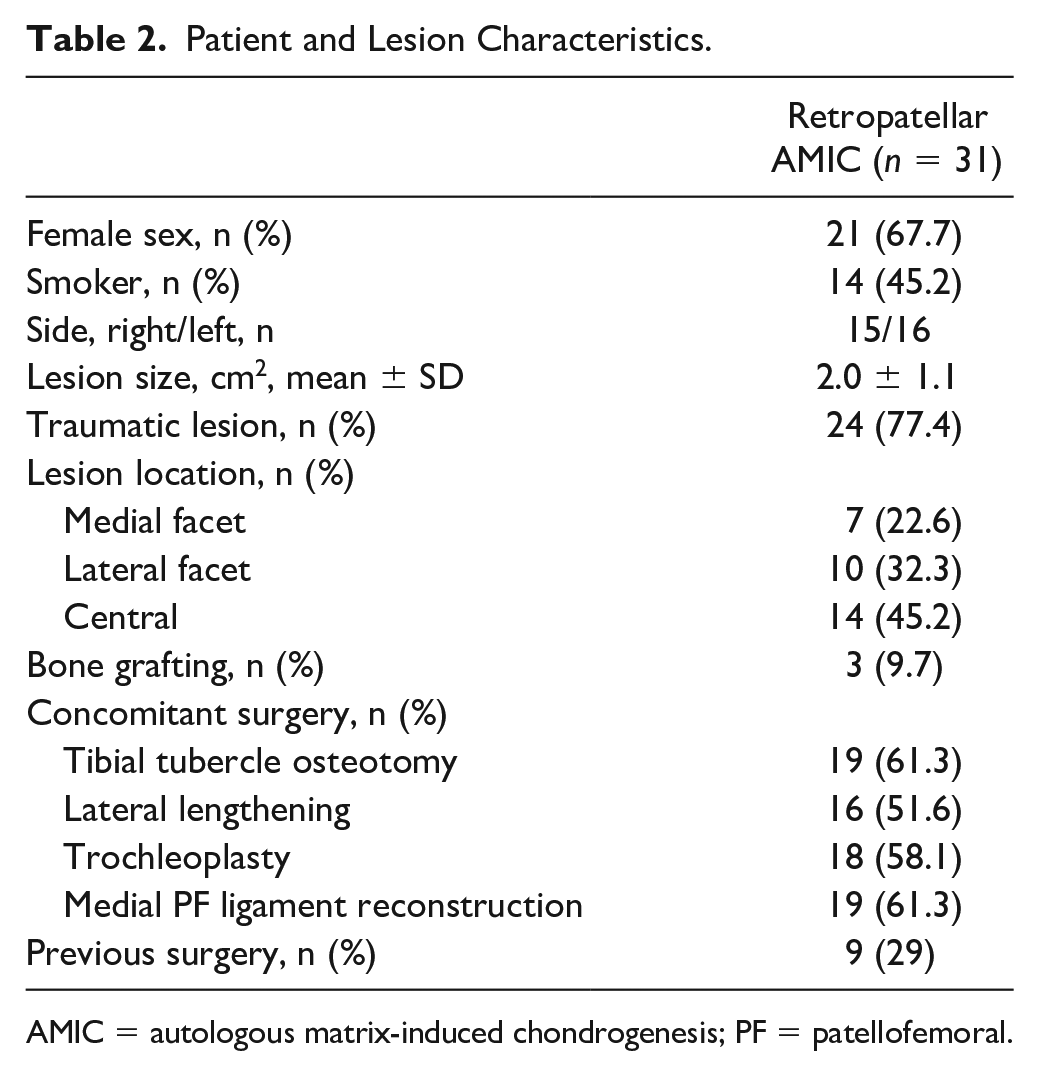
AMIC = autologous matrix-induced chondrogenesis; PF = patellofemoral.
Agreement for trochlear (Dejour) and patellar dysplasia (Wiberg) assessed with Cohen’s kappa were substantial (κ = 0.71) and excellent (κ = 0.94), respectively. ICCs assessed for all other postoperative PF parameters but TTTG (ICC = 0.82) resulted in excellent agreement (ICC > 0.9) between the readers (all, P < 0.001).
Complications and Reoperations
In the study period, the AMIC graft failed in 4 patients (12.9%) at a mean follow-up of 21 ± 14.1 months. Of these, 3 patients (75%) presented with an initial patellar lesion type I and 1 patient with a lesion type II (25%). None of the lesion type I patients underwent concomitant TTO. A total of 11 knees (35.5%) underwent reoperations, of which 8 (25.8%) had screw removal after tibial tubercle osteotomy (TTO), 1 patient (3.2%) had revision with microfracturing because of a partial AMIC-membrane dissection and proximalization TTO, 1 patient (3.2%) was revised to PF arthroplasty (PFA) because of symptomatic PF osteoarthritis, and 1 patient (3.2%) had medial patellofemoral ligament (MPFL) reconstruction due to persistent PF instability. One patient (3.2%) presented with persistent anterior knee pain (VAS = 80) and postoperative MRI showed failure of the entire AMIC graft, yet revision surgery was refused.
Clinical Outcome
At the final follow-up, patients who underwent retropatellar AMIC that did not fail (n = 25; 80.7%) presented with an average Kujala score of 71.3 ± 16.9, KOOS Pain of 76.2 ± 16.6, KOOS Symptoms of 70.8 ± 15.1, KOOS Activities of Daily Living (ADL) of 84.1 ± 12.1, KOOS Sport of 57.9 ± 28.7 and KOOS Quality of Life (QOL) of 54.4 ± 20.3. Preoperative Kujala score was available in 21 knees, showing a significant improvement from 63.5 ± 11.6 to 72.2 ± 17.4 at final follow-up (P = 0.029). Tegner scores declined from 5.1 ± 2.0 preinjury to 4.2 ± 1.9 preoperatively and 4.2 ± 1.8 postoperatively (P = 0.041), respectively ( Fig. 3 ).
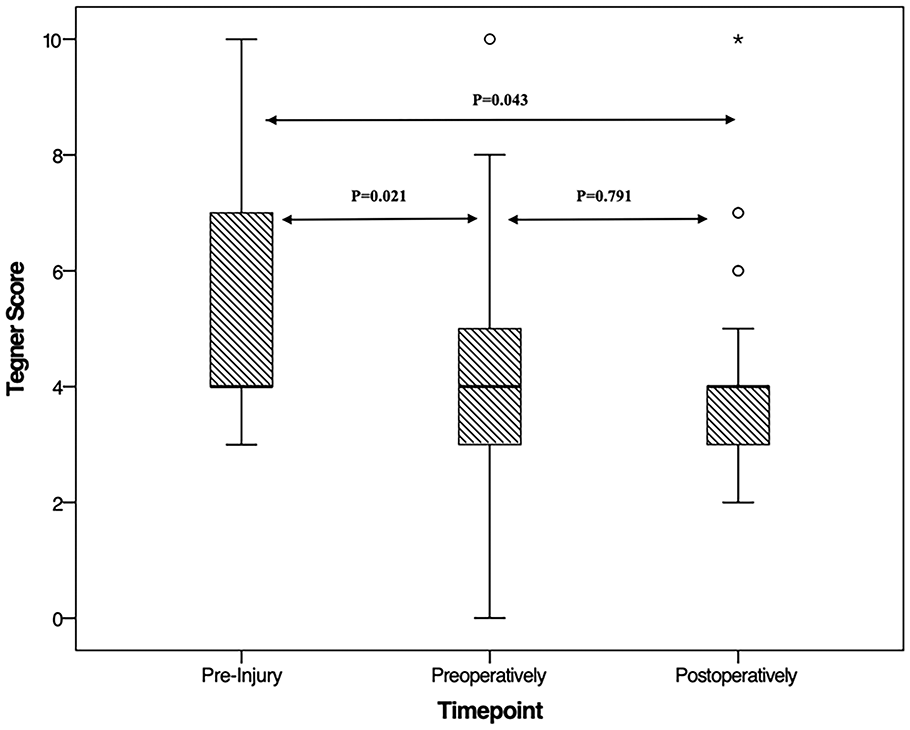
Comparison of Tegner scores between preinjury, preoperatively, and postoperatively.
When correlating postoperative clinical scores and patient-/lesion-specific characteristics, female sex was negatively associated with KOOS QOL (r = −0.434; P = 0.024) and CDI was significantly correlated with KOOS Sport (r = 0.392; P = 0.048). No other statistically significant associations were found.
Patients with failed grafts within the study period had a significantly smaller patellar and Laurins’s PF angle than patients whose graft did not fail (P = 0.008 and P = 0.004, respectively), yet no difference was seen in patient or lesion demographics ( Table 3 ).
Comparison of Patient-/Lesion-Specific Characteristics and Postoperative PF Parameters between Failures and Nonfailures.
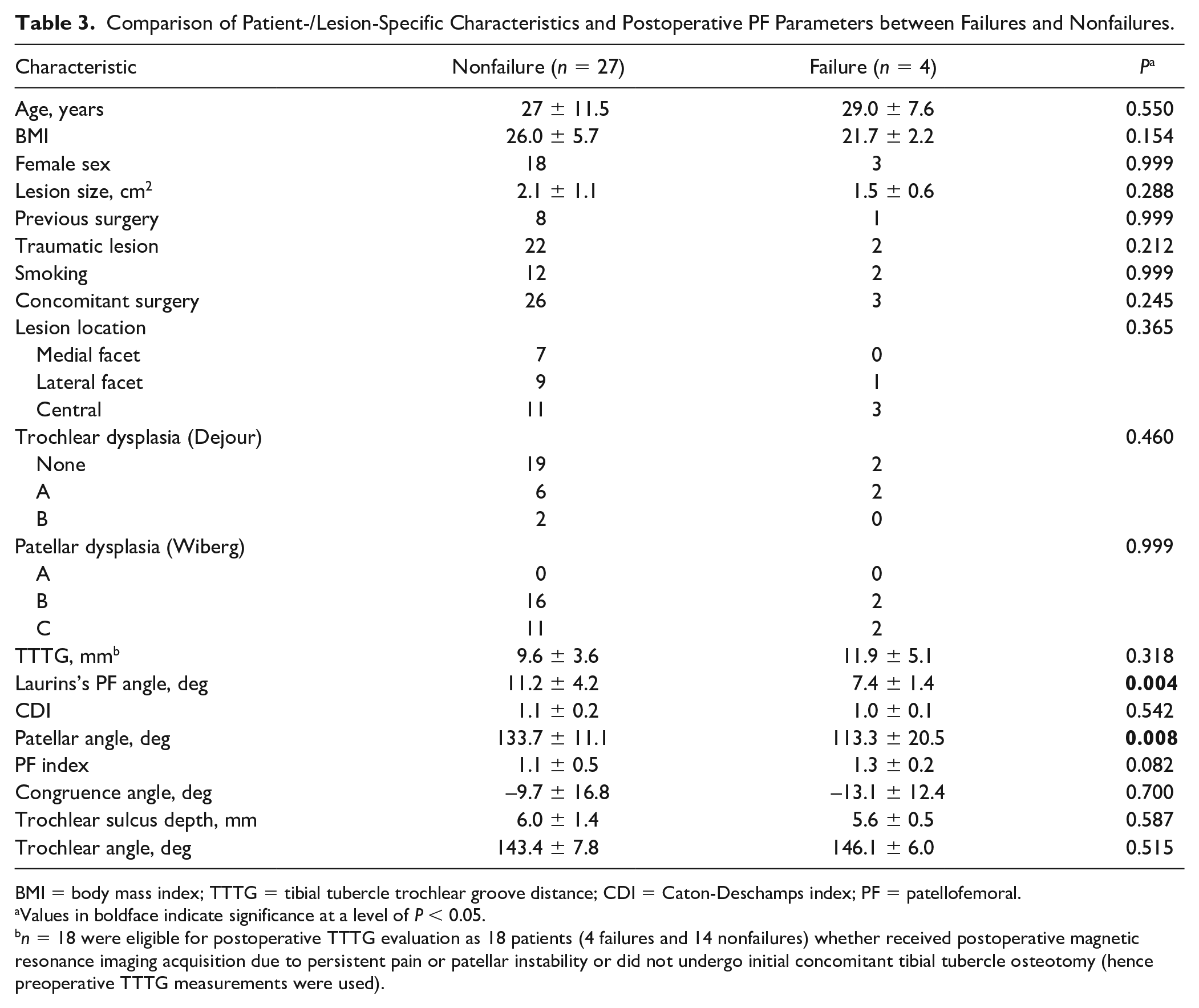
BMI = body mass index; TTTG = tibial tubercle trochlear groove distance; CDI = Caton-Deschamps index; PF = patellofemoral.
Values in boldface indicate significance at a level of P < 0.05.
n = 18 were eligible for postoperative TTTG evaluation as 18 patients (4 failures and 14 nonfailures) whether received postoperative magnetic resonance imaging acquisition due to persistent pain or patellar instability or did not undergo initial concomitant tibial tubercle osteotomy (hence preoperative TTTG measurements were used).
At final follow-up, 19 patients (61.3%) complained about anterior knee pain with a mean VAS of 21.7 ± 26.5 points during daily life and 45.7 ± 28.4 points during sports. Generally, 25.8% of patients reported that they were very satisfied with the result of the surgery, 51.6% were satisfied, 9.7% were rather unsatisfied and 12.9% were very unsatisfied at final follow-up. Of all determined patient- and lesion-specific factors, the patellar angle was the only parameter that was significantly associated with the patient’s satisfaction level (r = 0.615; P < 0.001) ( Fig. 4 ).
(
Discussion
The key findings of this study are that retropatellar AMIC with concomitant corrective surgery for patellar instability resulted in satisfactory clinical outcome with a low failure rate (12.9%) at a mean follow-up of 4.1 ± 1.9 years. Both, a smaller patellar and Laurins’s PF angle were the only PF parameters that were significantly associated with failure of retropatellar AMIC. Generally, 77.4% of patients reported a satisfactory result after retropatellar AMIC, yet only 35.4% returned to the previous level of sport.
In 2003, Behrens et al. 49 proposed AMIC as a treatment option for cartilage lesions of the knee by improving the concept of microfracturing. Since then, AMIC proofed itself to be a viable treatment option for chondral lesions across the knee joint.20-22 Due to the unique anatomy and complex biomechanical environment, however, the treatment of cartilage lesions particularly in the PF joint remains a challenge for orthopedic surgeons. So far, clinical results of AMIC for retropatellar cartilage lesions have only been reported in small case series, studies with short-term follow-up or as a part of studies investigating AMIC for the entire knee joint without thorough subanalysis.23-27,50
D’Hollander et al. 25 reported a case-series of 10 patients after AMIC for PF cartilage lesions with a follow-up of 24 months showing significant clinical improvement. Functional outcomes, however, were lower compared with the current study with a reported mean postoperative Kujula score of 59.8 versus 71.3 and total KOOS of 243.9 versus 343.4. Interestingly, only 3 patients (30%) underwent associated procedures for PF instability with 2 anteromedializing TTOs and 1 MPFL reconstruction compared with over 90% in the presented study. This fact might contribute to the difference seen in clinical outcomes between both studied patient cohorts.
In a subanalysis of retropatellar AMIC in 20 patients, Kusano et al. 22 reported a high patient satisfaction and significant improvement of all PROMs at a mean follow-up of 29.3 months. Similar to the current study, concomitant patellar stabilization was performed in the majority of cases (90%) with tibial tubercle realignment.
In another small case series, Sadlik et al. 26 analyzed 12 patients that received all-arthroscopic retropatellar AMIC at mean follow-up of 38 months. The authors reported an excellent clinical outcome with a mean postoperative KOOS and International Knee Documentation Committee (IKDC) score of 90.1 and 79.4, respectively. Additional procedures addressing PF instability were performed in 33% of patients.
A more recent study by Tradadi el al. 27 analyzing 14 patients reported very good results throughout the follow-up period with a mean of 68.1 months. While the mean Kujula score at final follow-up was relatively high with a mean score of 87.7 (vs. 71.3 in the current study), this study excluded patients with uncorrected lower limb malalignment, uncorrected patellar instability, previous cartilage surgery, trochlear dysplasia, and diffuse patellar bone edema. This resulted in the exclusion of 10 (41.7%) of the total 24 patients, thus analyzing a very selected patient cohort, which rarely presents to an orthopedic surgery office. Only 2 cases (14.3%) underwent concomitant corrective surgery with 1 open lateral release and 1 MPFL reconstruction, yet the authors did not specify the anatomy or clinical finding of the patellar instability.
Kaiser et al. 50 reported stable long-term clinical improvement with a mean Lysholm score of 85 and VAS of 2.3 among the retropatellar subcohort (n = 12) with 1 failure (revision total knee arthroplasty) at a mean follow-up of 9.3 years after AMIC. In this study, all patients with retropatellar AMIC had concomitant corrective surgery for patellar instability with transfer of the tibial tubercle, lateral release and reinforcement of the vastus medialis muscle.
Certain anatomical factors such as dysplasia and patellar maltracking can lead to premature cartilage degeneration. In a study by Ambra et al. 9 trochlear dysplasia, patella alta, and excessive lateral patellar tilt were the most common correlated factors with PF cartilage defects, especially in retropatellar lesions. However, these factors can be surgically corrected by trochleoplasty, MPFL reconstruction (as it lowers patella height) 51 and lateral release, as performed in the current study cohort. The goal in correcting these pathologies is to stabilize the patella and consequently to decrease joint contact pressure and reduce shearing forces on the retropatellar cartilage repair. Trinh et al. systematically reviewed 11 studies and found significant better outcome in patients treated with additional TTO to cartilage repair when compared with isolated cartilage repair of the PF joint. 52 Biomechanical studies demonstrated that TTO reduces shearing forces on the PF compartment, 53 which is important to protect the fresh cartilage graft and promote tissue healing.
In the current study, only a smaller Laurins’s PF and patella angle were significantly associated with retropatellar cartilage repair failure, suggesting an appropriate correction of PF morphology. However, as a smaller Laurins’s PF angle is an indirect indicator of increased patellar tilt, this finding underlines the results reported by Ambra et al. 9 and adequate correction of patellar tilt is warranted in retropatellar cartilage repair with AMIC. Therefore, preoperative evaluation of patellar tilt may help determine the necessity for a corrective TTO in the treatment of cartilage lesions of the PF joint. Furthermore, it can be theorized that a decreased patellar angle also contributes to pathological loading of the PF joint, as it concentrates shear forces on a smaller surface thus increasing contact stresses, which have been shown to be detrimental to cartilage repair. 54 Despite this, correction of patellar morphology is not routinely performed in patients with PF instabilities. Yet, there are techniques described in the literature to alter patellar morphology, but the biomechanical effect and clinical importance remains unknown.55-57 Alternatively, a decrease of PF contact pressure in these patients could be achieved by adding anteriorization during the medialization of the tibial tubercle, which is achieved by an anteromedializing TTO, known as a Fulkerson osteotomy.58,59 Especially isolated lateral and distal retropatellar cartilage lesions (Fulkerson type I and II) can result in good clinical outcome even without cartilage restoration, particularly smaller defects. However, the effect of isolated TTO on central or medial patellar lesions (Fulkerson type III and IV) is less favorable. 29 In fact, all failures in the current study were patellar type I or II lesions, of which none of the type I lesions had concomitant TTO. Interestingly, only half of type II lesions underwent concomitant TTO, yet this did not affect failure rate or clinical outcome, as the one patient who failed in this subgroup received TTO. Furthermore, patients with lesion types III and IV benefited similarly, regardless of concomitant TTO, suggesting a significant effect of retropatellar AMIC.
To assess return to sporting level after retropatellar AMIC, preinjury to postoperative Tegner activity scores were reported. Despite generally good patient satisfaction, the level of sport activity decreased significantly. Similar to a previous report of AMIC for osteochondral lesions of the talus, especially high preinjury sporting level activity patients tend to not return to their previous level. 60
The following limitations have to be acknowledged. First, preoperative KOOS were unavailable and only 67.7% of preoperative Kujala scores were available as the study was retrospective in its design. Tegner preinjury and presurgery scores collected retrospectively at the postoperative follow-up assessment, potentially introducing recall bias. However, selection bias was minimized by reviewing all patients with retropatellar AMIC since the introduction of this technique at our institution and achieving a follow-up rate of 86%. Second, postoperative MRI was not available in all patients, which would have enabled this study to assess repair tissue quality and postoperative patellar tilt. Moreover, due to the limited clinical value of postoperative MRI or arthro computed tomography in cartilage repair, 61 this study did not assess or report postoperative MR imaging outcome. Contrarily, postoperative MRI would have been useful in evaluating postoperative patellar tilt, thus assessing the effect of concomitant corrective surgery. As MRI was not available in all patients, this study utilized the Laurins’s PF angle, which is an accepted indirect measurement for patellar tilt. 41 Third, the high rate of concomitant procedures makes it difficult to evaluate the isolated clinical effect of retropatellar AMIC. Yet, this cohort represents the real-world scenario of patients that receive retropatellar cartilage repair, who often present with complex PF anatomical pathologies and therefore require extensive surgical intervention. Considering the high failure rate in type I lesions without concomitant TTO and the negative overall effect of a small patellar and Laurins’s PF angle, this study supports the growing evidence for the need of unloading retropatellar cartilage repair, when indicated.
By assessing postoperative anatomical parameters and analyzing their influence on the outcome of retropatellar AMIC, the current study is an important contribution to the knowledge about the outcome of AMIC for isolated focal cartilage lesions of the patella.
Conclusion
AMIC for retropatellar cartilage lesions in combination with concomitant corrective surgery for patellar instability results in low failure rate with satisfactory clinical outcome and patient satisfaction of almost 80% at mid-term follow-up. As most failures occurred in patients without concurrent TTO and both a smaller patellar and Laurins’ PF angle were associated with less favorable outcome, this study supports the growing evidence for the need of unloading retropatellar cartilage repair, when indicated.
Supplemental Material
sj-pdf-1-car-10.1177_19476035211021908 – Supplemental material for Autologous Matrix-Induced Chondrogenesis (AMIC) for Isolated Retropatellar Cartilage Lesions: Outcome after a Follow-Up of Minimum 2 Years
Supplemental material, sj-pdf-1-car-10.1177_19476035211021908 for Autologous Matrix-Induced Chondrogenesis (AMIC) for Isolated Retropatellar Cartilage Lesions: Outcome after a Follow-Up of Minimum 2 Years by Manuel Waltenspül, Cyrill Suter, Jakob Ackermann, Nathalie Kühne and Sandro F. Fucentese in CARTILAGE
Footnotes
Authors’ Note
Investigation performed at the Balgrist University Hospital, Switzerland.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval (No. 2020-01052) was granted by the local research ethics committee.
Informed Consent
All included patients gave their written informed consent.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.