
Abstract
Objective
The role of vitamin D in the pathogenesis of osteoarthritis (OA) is not well understood. In this study, we aimed to investigate the association of serum vitamin D with the serum cytokine profile in patients with primary knee OA.
Design
In a cross-sectional study, 116 patients with radiologic diagnosis of grade I to III knee OA were included. The study population included 79 (75.9%) females and 25 (24.1%) males with a mean age of 55.1 ± 9.6 years. The serum concentration of IL-6, IL-8, TNF-α, IL-4, IL-10, IL-13, and vitamin D were assessed using an enzyme-linked immunosorbent assay. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was used for the assessment of patient’s reported disability associated with knee OA.
Results
Serum vitamin D status was deficient, insufficient, and sufficient in 18 (15.5%), 63 (54.3%), 35 (30.2%) patients, respectively. Higher levels of serum IL-6 were observed in patients with vitamin D deficiency (P = 0.022). The mean serum vitamin D level was not associated with OA grade (P = 0.88) and WOMAC scores of the patients (P = 0.67). Serum IL-6 level was significantly associated with both OA grade and WOMAC scores of the patients (P < 0.001 and P = 0.001, respectively). The vitamin D status was not significantly associated with the serum levels of other evaluated cytokines.
Conclusion
Vitamin D deficiency in knee OA seems to be associated with a higher release of IL-6. Therefore, vitamin D supplementation could reduce the disease burden by controlling the IL-6 release.
Introduction
Osteoarthritis (OA) is one of the most common chronic disorders among the elderly population and a leading cause of disability.1-3 To date, no definitive treatment has been introduced for OA, and available therapeutic options only aim to decelerate the progression of the symptoms. 4 Further insights into the pathogenesis of OA result in better evaluation of the disease process and the implication of more effective therapeutic interventions.
According to the current state of knowledge, OA is considered an inflammatory disease, and chronic joint inflammation is strongly suggested as an underlying factor in the pathogenesis of OA. 5 Seemingly, this phenomenon is driven by the interaction of a variety of immune mediators, including anti- and proinflammatory cytokines.6,7
Vitamin D has several immunomodulating properties that support its anti-inflammatory role in many inflammatory disorders.8-11 This modulation is mainly centered on promoting the production of anti-inflammatory cytokines and inhibiting the production of proinflammatory cytokines. 12 In addition, a potential role has been suggested for vitamin D in cartilage regeneration. 13
Despite the potential beneficial effects of vitamin D on articular cartilage, the role of vitamin D supplementation in the improvement of OA symptoms is controversial. 14 While some studies found no association between vitamin D supplementation and OA pain/disability,15-17 other studies suggested a link between vitamin D deficiency and OA symptoms.18,19 To make it more complicated, a double-blind, placebo-controlled trial revealed that patients given oral vitamin D supplements had slightly higher pain and functional disability compared with those receiving placebos. 20 Such controversy has been attributed to a number of factors such as different laboratory techniques in determining serum vitamin D level, study populations with different geographical locations and different ethnic backgrounds, lack of universal definition for hypovitaminosis D, stage of OA, and so on. 21
Considering the acknowledged role of cytokines in the development of OA 7 and the regulatory role of vitamin D in cytokine production, 22 an association between the serum vitamin D and cytokine levels is expected. We hypothesized that if a link were found between vitamin D status and serum cytokines, vitamin D supplementation could be suggested to modulate the inflammatory profile of OA, thereby reducing the disease burden.
In this study, we aimed to investigate the association between serum vitamin D status and serum cytokine profile in patients with symptomatic primary knee OA.
Patients and Methods
This cross-sectional study was conducted according to the Declaration of Helsinki and approved by the ethics committee of the Iran University of Medical Sciences under the code of IR.IUMS.REC.1396-01-196-30631. Written informed consent was obtained from patients before their participation in the study. Patients with primary symptomatic knee OA who were consecutively referred to the OA clinic of our university hospital were evaluated for eligibility criteria. The inclusion criteria were the radiologic diagnosis of grade I to III primary knee OA, according to the Kellgren and Lawrence classification system, and bilateral involvement. 23 Patients with Kellgren and Lawrence grade IV were excluded to minimize a potential confounding variable that influences circulating cytokines. Patients with concomitant disorders affecting the serum cytokines level, including other chronic inflammatory disorders, infection, diabetes mellitus, cardiovascular disorders, renal disorders, and neurodegenerative disorders, were also excluded. In addition, patients who were taking anti-inflammatory drugs and those in whom the grade of OA was not the same in both knees were excluded. From a total of 324 knee OA patients who were evaluated, 116 patients were identified as eligible for this study ( Fig. 1 ). Demographic characteristics of the patients are presented in Table 1 .
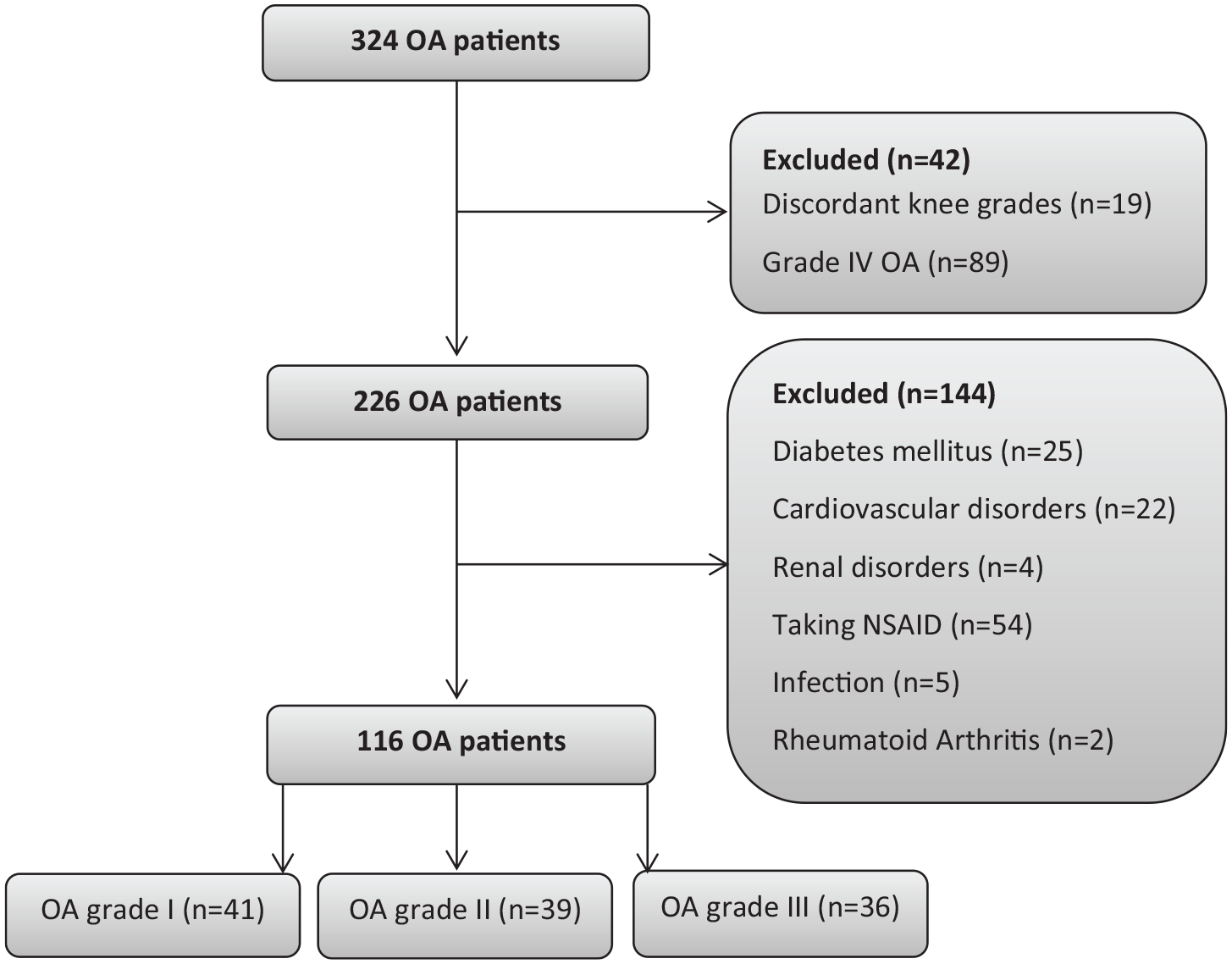
The flow diagram of study inclusion and exclusion.
The Demographic, Clinical, and Laboratory Characteristics of the Patients with Knee Osteoarthritis (OA), n = 116.

Presence of disease in the patient’s first-degree relatives.
Laboratory Investigations
A single venous blood sample was taken from the patients in the early morning after fasting for 12 hours and collected in tubes containing a clot activator. The blood serum was withdrawn and transferred to a −80° C freezer for later examinations. After the completion of the sample collection step, serum levels of proinflammatory cytokines, including interleukin (IL)-6, IL-8, and tumor necrosis factor-α (TNF-α), serum levels of anti-inflammatory cytokines, including IL-4, IL-10, and IL-13, and serum vitamin D level were measured using the manufactured enzyme-linked immunosorbent assay kits (BE53061, BE53081, BE55001, BE58041, BE53101, BE53131, and RE53041, respectively, IBL-Immuno-Biological Laboratories Co, Ltd., San Diego, CA, USA). Vitamin D measurement included both D2 and D3 variants (25-OH-vitamin D total). Serum vitamin D levels was categorized as deficient (<20 ng/mL), insufficient (20-30 ng/mL), and sufficient (30-100 ng/mL). 24
Clinical Assessment of Disability
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire in Persian 25 was used for the assessment of patient’s reported disability associated with knee OA. The questionnaire contains 24 items divided into 3 subscales, including pain (5 items), stiffness (2 items), and physical function (17 items). The WOMAC scores were presented as a percentage so that a higher score was indicative of more disability.
Statistical Analysis
The prevalence of vitamin D deficiency is reported to be 69.5% in the Iranian knee OA. 26 According to this prevalence, power of 80%, and type I error (alpha) of 0.1, a sample size of at least 82 patients was found to be enough to access the difference of serum cytokines using the 1-way analysis of variance (ANOVA) test.
GraphPadPrism 6 (GraphPad Software Inc., La Jolla, San Jose, CA, USA) was used for the statistical analysis of data. Descriptive data were provided as mean ± standard deviation, or number and percentage. A comparison of mean values between groups was made using 1-way ANOVA for parametric variables and the Kruskal-Wallis H test for nonparametric variables. A multivariate analysis was done using a binary logistic regression model to remove the effect of confounders (age, sex, body mass index, and OA grade) on the association of serum vitamin D and serum cytokine levels. A chi-square test was used for the analysis of the associations between categorical variables. Pearson’s correlation coefficient test was used for the evaluation of potential correlations. A P value less than 0.05 was considered significant.
Results
Vitamin D
The mean serum vitamin D level was 33.5 ± 18.1 ng/mL (range 14-78 ng/mL) in OA patients of the current series. Accordingly, serum vitamin D status was identified as deficient, insufficient, and sufficient in 18 (15.5%), 63 (54.3%), 35 (30.2%) patients, respectively. Serum vitamin D status was not associated with OA grade (P = 0.88).
WOMAC Score
The mean WOMAC score of the patients was 50.7 ± 15.6 (range 6.8-100). The mean WOMAC scores were significantly higher in higher stages of OA (P < 0.001). The mean WOMAC score was not significantly associated with the vitamin D status of the patients (P = 0.67). No significant correlation was also found between the serum vitamin D levels and the WOMAC score of the patients (r = −0.026, P = 0.77).
Serum IL-6
The mean serum IL-6 level was 6.5 ± 2.5 pg/mL (range 1.7-12.5 pg/mL). The mean serum IL-6 level was significantly more in higher grades of OA (P < 0.001). The mean serum IL-6 level was significantly more in patients with vitamin D deficiency (P = 0.022). A significant positive correlation was observed between the serum IL-6 level and WOMAC scores of the patients (r = 0.305, P = 0.001). A significant negative correlation was found between the serum IL-6 and vitamin D levels (r = −0.220, P = 0.018).
Serum IL-8
The mean serum IL-8 level was 34.7 ± 13.1 pg/mL (range 12-69 pg/mL). The mean serum IL-8 level was not significantly associated with OA grade (P = 0.64) and vitamin D status (P = 0.49). In addition, serum IL-8 was not significantly correlated with WOMAC scores (r = −0.020, P = 0.82) and serum vitamin D levels (r = 0.040, P = 0.88) of the patients.
Serum TNF-α
The mean serum TNF-α level was 40.2 ± 14.7 pg/mL (range 12-82 pg/mL). The mean serum TNF-α level was not significantly associated with OA grade (P = 0.93) and vitamin D status (P = 0.36). In addition, serum TNF-α was not significantly correlated with WOMAC scores (r = 0.013, P = 0.89) and serum vitamin D levels (r = 0.015, P = 0.87) of the patients.
Serum IL-4
The mean serum IL-4 level was 4.8 ± 1.8 pg/mL (range 12-69 pg/mL). The mean serum IL-4 level was not significantly associated with OA grade (P = 0.69) and vitamin D status (P = 0.93). In addition, serum IL-4 was not significantly correlated with WOMAC scores (r = −0.059, p=0.51) and serum vitamin D levels (r = −0.066, P = 0.47) of the patients.
Serum IL-10
The mean serum IL-10 level was 7.8 ± 2.9 pg/mL (range 2-13.4 pg/mL). The mean serum IL-10 level was significantly more in higher grades of OA (P = 0.003). The mean serum IL-10 level was not significantly associated with the vitamin D status of the patients (P = 0.71). Serum IL-10 level was negatively correlated with the WOMAC score (r = −0.267, P = 0.004), but not with serum vitamin D level (r = 0.075, P = 0.42).
Serum IL-13
The mean serum IL-13 level was 21.1 ± 9.4 pg/mL (range 6.8-45 pg/mL). The mean serum IL-13 level was not significantly associated with OA grade (P = 0.44) and vitamin D status (P = 0.38). In addition, serum IL-13 was not significantly correlated with WOMAC scores (r = 0.005, P = 0.92) and serum vitamin D levels (r = −0.063, P = 0.5) of the patients.
The distribution of serum cytokines, vitamin D, and WOMAC scores according to the grade of knee OA is presented in Table 2 in detail. The association of serum cytokines with vitamin D status is demonstrated in Figure 2 .
Distribution of Serum Cytokines, Vitamin D, and WOMAC Scores According to the Grade of Knee OA (Univariate Analysis). a

OA = osteoarthritis; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index.
Data are presented as Mean ± SD or number (%).
P < 0.05 is considered significant.

Distribution of serum cytokines in knee osteoarthritis patients with different vitamin D status (univariate analysis).
Multivariate Analysis
After removing the effect of potential confounding factors (age, sex, body mass index, and OA grade) on the association of serum vitamin D and serum cytokine levels in a binary logistic regression model, vitamin D was still significantly associated with serum IL-6 level (odds ratio = 0.310, P = 0.046, 95% CI = 0.081 to 0.001). No other significant association was observed in the multivariate model.
Discussion
The role of cytokines in the pathogenesis of OA has been demonstrated in many investigations. 27 Also, the effect of vitamin D deficiency on the pathogenesis of pain has been shown in several chronic disorders, including OA. 28 Even so, the cytokine-modulating capacity of vitamin D in knee OA is not well understood.
In this study, we assessed how the serum vitamin D level affects the serum cytokine profile (IL-6, IL-8, TNF-α, IL-4, IL-10, IL-13) in patients with knee OA. According to our study, the serum IL-6 level was significantly associated with the patients’ vitamin D status as significantly higher levels of serum IL-6 were detected in patients with vitamin D deficiency. Serum IL-6 level was also associated with the grade of OA and the patients’ level of disability. Serum IL-10 level was associated with the severity of OA but not with serum vitamin D level. No other significant association was found.
Barker et al, 29 in a pilot randomized controlled trial study, aimed to identify whether raising serum vitamin D supplementation modulates circulating cytokine concentrations in patients with knee OA. Patients were assigned to either placebo (n = 15) or treatment (n = 14) group. Supplements were administered for 84 days. The primary outcomes of this study were serum concentrations of cytokines, including granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (IFN-γ), IL-1β, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-13, and TNF-α. Prior to the vitamin D supplementation, serum IL-10 and IL-12 concentrations were significantly higher in subjects with more vitamin D levels. After vitamin D supplementation, no alteration occurred in the circulation level of serum cytokine levels. 29 We found a significant association between the serum vitamin D level and serum IL-6 level. This difference could be triggered by several confounding factors, such as the study design. While Barker et al 29 evaluated the causative effect of vitamin D on serum cytokine levels of OA patients in an interventional study, we only observed such an association in a cross-sectional study. The inclusion criteria of the patients could be regarded as the other factor of this inconsistency, as Barker et al 29 only included unilateral knee OA, while only bilateral knee OA was included in the present study.
In their subsequent cross-sectional study, Barker et al 30 examined the hypothesis that vitamin D deficiency associates with quadriceps weakness and increased serum cytokines in subjects with knee OA. Based on the serum vitamin D levels, subjects were divided into vitamin D deficient (n = 17), vitamin D insufficient (n = 21), and vitamin D sufficient (n = 18) groups. Evaluated cytokines included GM-CSF, IFN-γ, IL-5, IL-6, IL-7, IL-8, TNF-α, IL-12, IL-13, IL-1β, IL-2, and IL-4. The average power of the quadriceps was significantly impaired with vitamin D deficiency. Serum vitamin D level significantly correlated with the WOMAC pain score and WOMAC physical pain score of the patients. However, serum vitamin D status was not associated with serum concentration of any evaluated cytokines. 30 Serum vitamin D level was not associated with the WOMAC scores of the patients in the present study. This inconsistency could be attributed to the inclusion of patients with different grades of OA. Patients with OA grade I were excluded in the study of Barker et al, 30 while we excluded patients with OA grade IV.
Zheng et al 31 aimed to determine whether vitamin D supplementation is associated with alterations in inflammatory biomarkers in patients with symptomatic knee OA and vitamin D deficiency. In a randomised, placebo-controlled trial, patients either received 1.25 mg vitamin D3 (n = 106) or placebo (n = 94) monthly for 24 months. Serum levels of inflammatory biomarkers were assessed at baseline and 24 months using immunoassays. Compared with placebo, vitamin D supplementation had no significant effect on serum IL-6, IL-8, and IL-10 concentrations. They suggested that vitamin D deficiency may not affect systemic inflammation in patients with knee OA. 31 While serum vitamin D level was not associated with serum IL-8 and IL-10 levels in the present study, it was significantly associated with serum IL-6 levels. Zheng et al 31 excluded patients with severe radiographic changes and severe knee pain on standing (>80 mm on a 100-mm visual analogue scale). We excluded patients with severe radiologic changes (grade IV) but not patients with and severe knee pain.
Several studies have reported an association between serum vitamin D level and WOMAC scores of patients with knee OA. Alsubiaee et al 32 conducted a clinical trial to evaluate the effect of vitamin D supplementation on WOMAC scores of 58 vitamin D deficient knee OA patients. According to their results, the posttreatment WOMAC scores did not change significantly, despite the significant improvement of vitamin D levels. 32 The same results were observed in the study of Arden et al 33 as well as in the systematic review and meta-analysis of randomized clinical trials performed by Diao et al. 34 By contrast, Gao et al, 35 in a meta-analysis of randomized controlled trials, concluded that vitamin D supplementation is effective in improving the WOMAC pain and function in patients with knee OA. In accordance with the study of Gao et al, 35 we did not find an association between serum vitamin D levels and the WOMAC scores of the patients. However, this result does not preclude the role of vitamin D deficiency in the pathogenesis of knee OA, as vitamin D level was significantly associated with serum IL-6 levels, which is an important cytokine in OA development.
In the present study, serum IL-6 level was directly associated with the level of disability, while an inverse association was found between the serum IL-10 and the patients’ disability. The study of Imamura et al 7 revealed elevated levels of IL-6 and IL-10 in knee OA patients. Both serum IL-6 and IL-10 were directly correlated with the level of pain and disability in knee OA patients. IL-6 and IL-10 were not correlated with pressure pain threshold. 7 Ren et al 36 compared the serum and synovial cytokine profiles between the knee and hip OA. The serum IL6 level was elevated in both hip and knee OA. Serum IL-6 was correlated with pain score, whereas serum IL-10 was not. 36 In the study of Babaei et al, 37 serum IL-10 level negatively correlated with the level of synovial inflammation in knee OA patients. Reviewing the literature reveals more consensus on the association of serum IL-6 and OA severity.38-40 However, the association of serum IL-10 with OA severity is controversial. While some studies have reported a direct association between serum IL-10 and OA severity, 7 other studies, including ours, have found a reverse association 37 or no association. 36 This difference could be attributed to the different grades of knee OA in the studies. While we excluded patients with OA grade IV, it was included in the majority of other studies.7,36 It is acknowledged that the anti-inflammatory effect of IL-10 is more pronounced at the early stages of OA. 41 Therefore, a more inverse association could be expected between the serum IL-10 and OA severity in the early stages. Nevertheless, the association of serum IL-10 and OA severity needs to be further investigated in future studies.
Although the results of the present study suggest a cytokine-modulation role for vitamin D in knee OA patients, most of the earlier investigations found no association between serum vitamin D levels and serum cytokine concentrations in knee OA patients. This difference could be mainly attributed to the different designs of the studies and potential sources of heterogeneity. While the present study was observational, the studies of Zheng et al 31 and Barker et al 29 were interventional. Patients’ inclusion criteria were also a significant source of heterogeneity in several aspects, including the grade of OA and laterality of involvement (unilateral vs. bilateral). Therefore, future standardized studies with fewer heterogeneities are required to further evaluate the cytokine-modulation role of vitamin D in knee OA.
The present study was not without limitations. First, this was an observational study that impairs the potential inference on causality. Second, we assessed serum markers rather than intra-articular markers, which would be more specific and relevant for OA. Third, we did not control for day-to-day variation of cytokines, which could be regarded as the other limitation of the study. Fourth, the study was limited to a specific patient population, and therefore the results may not be applicable to other study populations.
Conclusion
Serum vitamin D was significantly associated with serum IL-6 level but not with the grade of OA or the level of disability. These findings suggest that the role of vitamin D deficiency in the pathogenesis of knee OA could be rather indirectly through its reduced immunomodulating effect and therefore a higher release of IL-6. Hence, vitamin D supplementation could subside the disease burden by controlling the IL-6 release.
Footnotes
Acknowledgments and Funding
This study was funded by the Iran University of Medical Sciences under the code of 30631.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This cross-sectional study was conducted according to the Declaration of Helsinki and approved by the ethics committee of the Iran University of Medical Sciences under the code of IR.IUMS.REC.1396-01-196-30631.
Informed Consent
Written informed consent was obtained from patients before their participation in the study.
Trial Registration
Not applicable.