
Abstract
Objective
To bring forward an arthroscopic classification of the popliteomeniscal fascicles of the lateral meniscus (PFLM) tears.
Design
Six fresh frozen knee joint samples of adult males were chosen, and the lateral meniscus at the popliteal hiatus region were measured to analyze their anatomic relationship. Patients who had received magnetic resonance imaging scan at knee joint before the surgery and diagnosed as PFLM tears by arthroscopy from April 2014 to October 2017 were selected. Data regarding the integrity of PFLM were prospectively recorded in a data registry. Tear morphology and treatment received were subsequently extracted by 2 independent reviewers from operative notes and arthroscopic surgical photos.
Results
The average length and thickness of the popliteal hiatus of the lateral meniscus were 2.09 ± 0.21 cm and 0.43 ± 0.08 cm, respectively. The average length of anterosuperior popliteomeniscal fascicle (APF) was 0.87 ± 0.18 cm, and the posterosuperior popliteomeniscal fascicle (PPF) was 0.72 ± 0.15 cm. A total of 36 PFLM tears in 36 patients were divided as type I (APF tear; n = 5, 13.9%), type II (PPF tear; n = 20, 55.6%), and type III (both APF and PPF tears; n = 11, 30.6%). All patients were treated with arthroscopic all-inside repair using a suture hook for the PFLM tears and follow-up for 21.1 months. All patients have done well with significantly improved Lysholm and International Knee Documentation Committee scores at the last follow-up relative to preoperative scores (P < 0.01).
Conclusion
This study suggests to possibly classify the PFLM tears for clinical practice.
Introduction
Because of the popliteus tendon, the lateral meniscus is separated by popliteus tendon in the middle and posterior segments, and it is not connected with joint capsule, forming a free “lateral meniscus-popliteal hiatus” with clear boundaries. 1 The relations between the popliteal hiatus and the popliteus tendon are the dynamical structures. Therefore, the lateral meniscus at the popliteal hiatus has high vulnerability to injuries due to the high activity. The lateral meniscus at the popliteal hiatus tears are often accompanied with anterior cruciate ligament (ACL) and posterolateral corner (PLC) injuries, and have various injury patterns.2-4 Many studies have investigated the lateral meniscus tears at the popliteal hiatus region based on their uniqueness.1,5,6 However, the classification of injuries in this area is not uniform. Also, no detailed classification for lateral meniscal tears at the popliteal hiatus has been reported.7-9 Thus, the aim of this study was to bring forward an arthroscopic classification of the traumatic popliteomeniscal fascicles of the lateral meniscus (PFLM) tears and assess the effects of arthroscopic all-inside repair using a suture hook in management of such injuries.
Methods
This study was carried out in accordance with the guidelines of the Declaration of Helsinki. All experimental protocols were approved by our institutional review board, and written informed consent was obtained from all study patients.
Specimens
A total of 6 fresh frozen knee joint samples were collected from healthy young males that between 19 and 37 years of age (mean 26.5 years), including 2 left knees and 4 right knees. A separate anatomic specimen of the lateral meniscus and popliteus tendon with intact the anterosuperior popliteomeniscal fascicle (APF) and the posterosuperior popliteomeniscal fascicle (PPF) was measured to analyze their anatomic relationship.
Patients
Patients who had underwent a magnetic resonance imaging (MRI) scan of the knee joint before surgery and were diagnosed as a traumatic PFLM tears by arthroscopy from April 2014 to October 2017 were selected. The knee joint symptoms, signs, Lysholm scores, and International Knee Documentation Committee (IKDC) scores were recorded. Data regarding the integrity of PFLM were prospectively recorded in a data registry. Tear morphology and treatment received were subsequently extracted by 2 independent reviewers from operative notes and arthroscopic surgical photos. Exclusion criteria were the symptomatic discoid lateral meniscus, severe synovitis or osteoarthritis, and the patients with medical history of ipsilateral knee joint surgery.
Surgical Technique
All patients underwent surgery under spinal anesthesia. A standard supine position was applied for the knee arthroscopy. Standard anterolateral and anteromedial portals were used to inspect the joint. In the suture process, the knee joint was kept at the figure-of-four position, and pressurized to increase the lateral joint space completely. The arthroscope inserted through the anterolateral portal and the repair processes were performed through the anteromedial and posterolateral portals. Generally, the lateral 2/3 width of the meniscus were reserved. A PFLM tear was identified by probing, and the margins of the meniscus tear were refreshed with a rasp. A right curved hook (Smith & Nephew, Andover, MA) is used for a right knee and vice versa for a left knee. The 25° suture hook loaded with lasso was placed into the tear area through a posterolateral portal. If the sutures need to be positioned more peripherally, the suture hook may be maneuvered past the lateral meniscus.10,11 The No. 2-0 nonabsorbable suture was then passed up through the tear area from below, after which a suture retriever could be used to retrieve the upper leg of the suture through easy repair.
Management of Associated Injuries
For patients associated with ACL injuries, the ipsilateral autograft hamstring tendons use as the reconstruction graft. Single bundle ACL reconstructions were performed. The graft was secured to the femur with an Endo-button (Smith & Nephew, Andover Massachusetts, United States) and the tibia was fixed by the absorbable extrusion screw (Smith & Nephew, Andover, MA). For patients associated with PLC injuries, the repair was optimal only if the sufficient tissue was present for re-approximation by suturing, or the reconstruction is recommended. 12 After surgery, the knee was immobilized in extension.
Postoperative Rehabilitation
The index leg was kept with a long knee brace with the knee at 0° flexion, and non-weight-bearing range of motion (ROM) exercises were started on postoperative day 1 with a flexion limit of 90° for 3 weeks after surgery. The affected knee could flex past 90° through joint function exercises from the fourth week after surgery and perform progressive quadriceps strength exercises from sixth week. Running was allowed at 3 months postoperatively.
Statistical Analysis
The SPSS 19.0 statistical software was applied for statistical analysis of data. Lysholm and IKDC scores of joint functions before and after surgery were compared and verified by a paired t-test. P < 0.05 indicates the statistically significant difference.
Results
The average length and thickness of popliteal hiatus of the lateral meniscus were 2.09 ± 0.21 cm (range = 1.84-2.67 cm) and 0.43 ± 0.08 cm (range = 0.34-0.52 cm), respectively. The average length of the APF was 0.87 ± 0.18 cm (range = 0.68-1.07 cm), and the PPF was 0.72 ± 0.15 cm (range = 0.56-0.89 cm; Fig. 1 and Table 1 ).
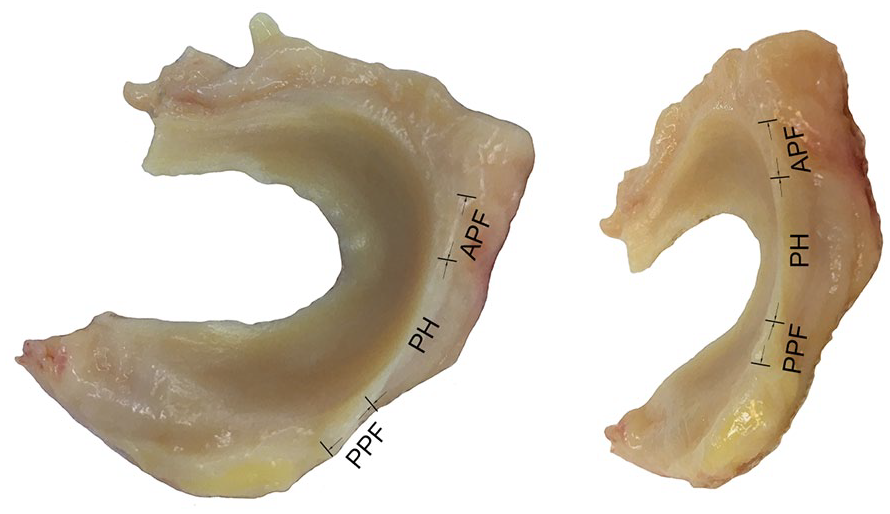
The anatomic attachment to the lateral meniscus. APF = anterosuperior popliteomeniscal fascicle; PH = popliteal hiatus; PPF = posterosuperior popliteomeniscal fascicle.
Average Dimensions of the Popliteal Hiatus of the Lateral Meniscus (n = 6).
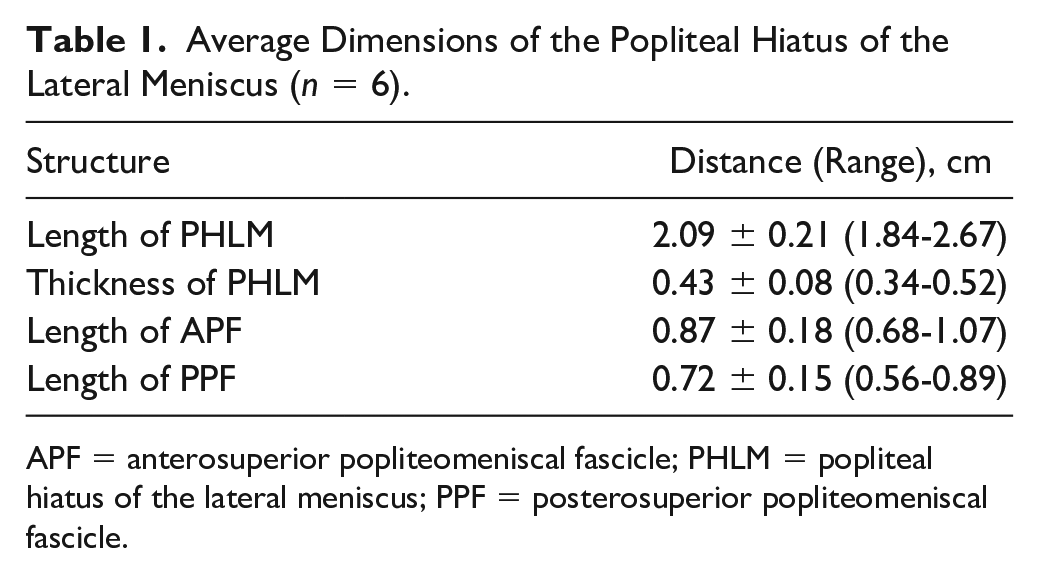
APF = anterosuperior popliteomeniscal fascicle; PHLM = popliteal hiatus of the lateral meniscus; PPF = posterosuperior popliteomeniscal fascicle.
Between April 2014 and October 2017, a total of 1566 knee arthroscopies were performed in our institution. In total, 36 traumatic PFLM tears in 36 patients were enrolled in our cohort, including 25 males and 11 females. The average age of these patients was 27.8 years (range = 19-42 years). Among the included patients, 21 patients had right knee injuries and 15 patients had left knee injuries. Overall, there were 27 (75%) patients with ACL injuries, and 7 (19.4%) patients with posterolateral corner (PLC) injuries ( Table 2 ).
Patient Demographic Information for Each Type of the PFLM Tears.
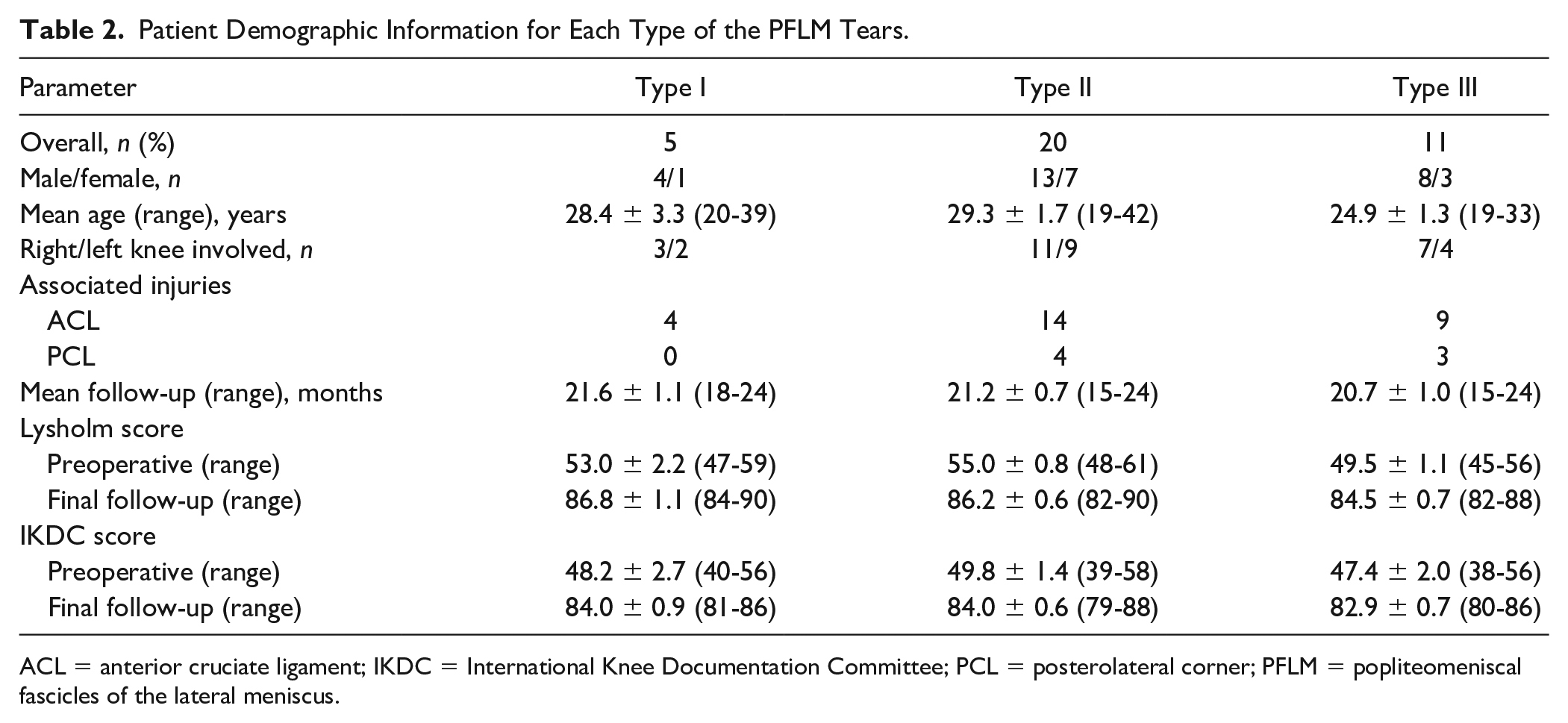
ACL = anterior cruciate ligament; IKDC = International Knee Documentation Committee; PCL = posterolateral corner; PFLM = popliteomeniscal fascicles of the lateral meniscus.
A total of 36 traumatic PFLM tears in 36 patients were divided as type I (APF tear; n = 5, 13.9%), type II (PPF tear; n = 20, 55.6%), and type III (both APF and PPF tears; n = 11, 30.6%; Fig. 2 ). All patients sustained all-inside arthroscopic repair using a suture hook for the traumatic PFLM tears and follow-up with averaged 21.1 months (range = 15-24 months). All patients evolved toward full ROM more than 135°, with no knee joint locking and snapping. Clinical examination illustrated the figure-of-four test, Lachman test, anterior drawer test, pivot shift test, and McMurray were negative.13,14 Lysholm and IKDC scores were improved significantly to the final follow-up 85.7 ± 0.4 (range = 82-90) and 83.7 ± 0.4 (range = 79-88) from the 53.1 ± 0.8 (range = 45-61) and 49.1 ± 1.1 (range = 38-58) before surgery (P < 0.01; Table 2 ). For MRI examination at final follow-up, all 36 patients presented healing changes after the suture at index location. In addition, no extrusion of the meniscus toward peripheral regions was observed. All patients returned to normal work after 4.8 ± 0.9 months in average (range = 3-6 months).
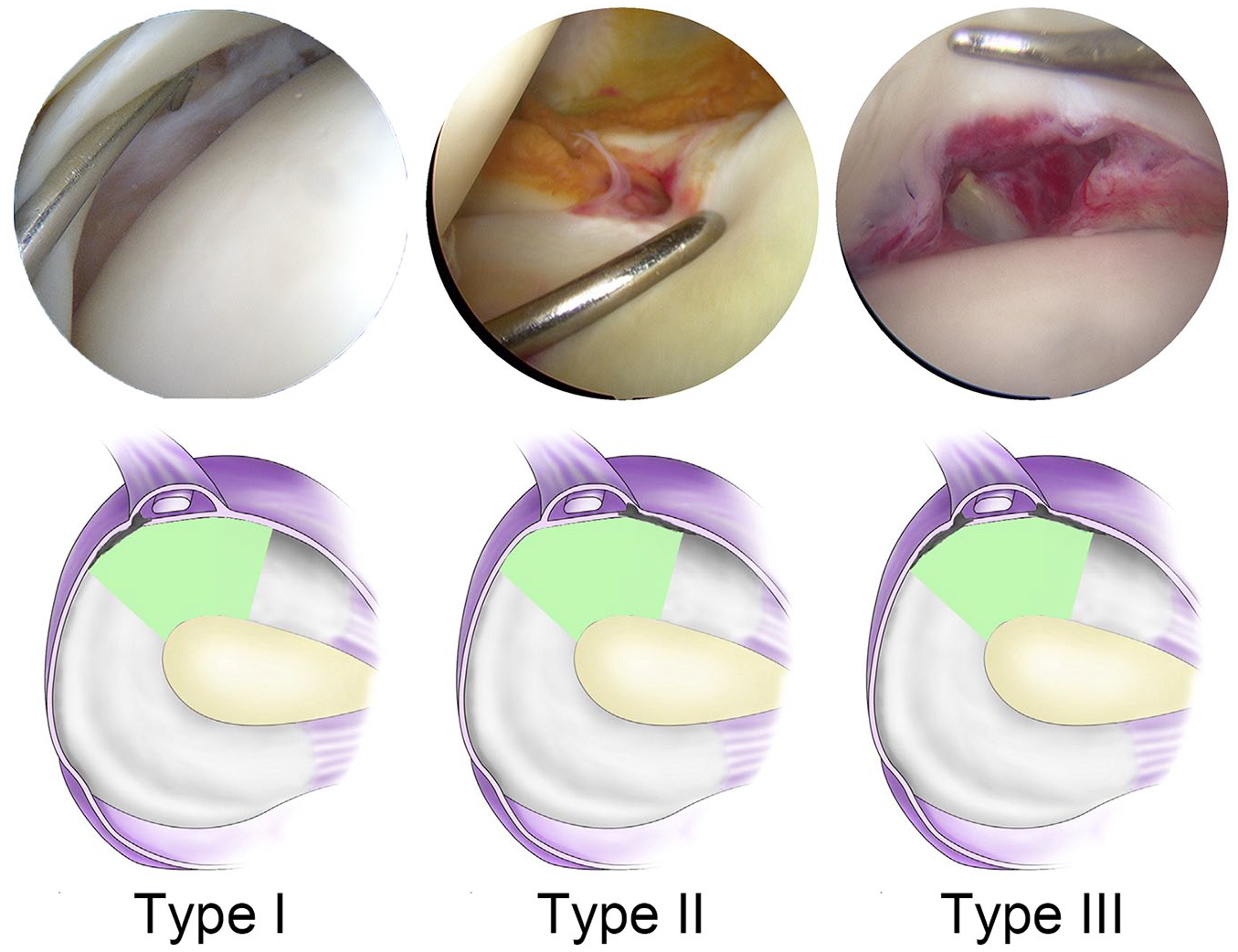
Illustrations of the arthroscopic classification system for popliteomeniscal fascicles of the lateral meniscus.
Discussion
The most important finding of the study was that we quantified the dimensions of the PFLM, and brought forward a concise arthroscopic classification system for the PFLM tears. The popliteal hiatus of the lateral meniscus is a free segment that the length is 2.09 ± 0.21 cm, with 0.87 ± 0.18 cm length of APF and 0.72 ± 0.15 cm length of PPF. According to cadaver findings, the PFLM tears were defined as the range area of 1 cm to the front or rear edge of the popliteal hiatus ( Fig. 3 ). Most notably, this study classified the PFLM tears into 3 types according to tear area: APF tear is type I, PPF tear is type II, and both APF and PPF tears are type III. These findings of this study provide the anatomic foundation and concise classification system for an improved understanding of the role of the PFLM tears. In addition, we also used the arthroscopic all-inside repair using a suture hook for the PFLM tears, and reported the excellent short-term follow-up results.
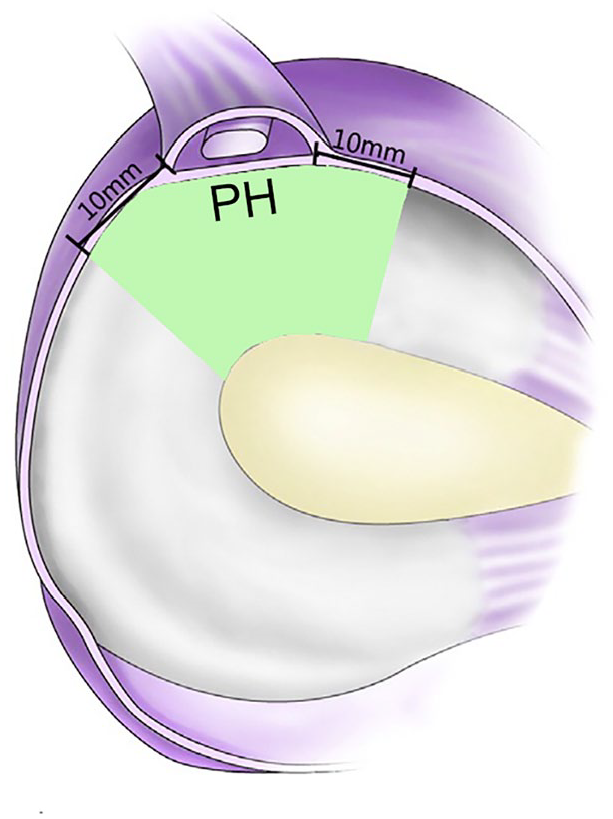
Tears of the popliteomeniscal fascicles of the lateral meniscus are defined as the range area of 1 cm to the front or rear edge of the popliteal hiatus. PH = popliteal hiatus.
The PFLM is composed of 3 distinct fasciculi, the anteroinferior, posterosuperior, and posteroinferior fasciculi, which are attached to the lateral meniscus at the popliteal hiatus. 1 The fibrous structures of the PFLM form a stable ligamentous complex around the popliteus tendon, and play an important role for the stability of lateral meniscus,15-17 with serving as 2 piers of an arch bridge. The PFLM tears will lead to loss of normal peripheral hoop stresses and make the lateral meniscus subluxation.18,19 An experimental biomechanical study reported that the lateral meniscal motion doubled when the PFLM was resected in human cadaveric knee joint. 20 The PFLM tears are often seen in young sports enthusiasts and a common finding in subjects with ACL and PLC injuries. 4 In the clinical practices, the open surgical repair of the PFLM tears was found to improve patient knee joint function and resolve lateral compartment knee joint pain.13,21 Arthroscopic lateral meniscectomy in stable knees without initial cartilage lesions might yield good to excellent results in young patients in the long term. 22 Remarkably, arthroscopic or arthroscopically assisted PFLM repair that restores the integrity of the PFLM and the capsular attachment to the lateral meniscus would also be successful. 13 However, 2 special considerations have to be considered in the suture process. First, out-inside suture, in-outside suture, and all-inside suture might make the torn meniscus and joint capsule closed up. These suture techniques may be able to stitch the tissue of meniscus in the popliteal tendon, or narrow the popliteal hiatus.18,19,23,24 Although Ouanezar et al. 6 reported the satisfying clinical effect of the suture technique that the lateral meniscus of the popliteal hiatus is stitched with the popliteal tendon tissues, without evident complications. Many scholars pointed out that the popliteal tendon make dynamic sliding in the popliteal hiatus. If it is stitched with lateral meniscus that has different activity mode, it will surely cause sutural cutting that will affect not only healing of the lateral meniscus but also functions of the popliteal tendon. If the suture avoids popliteal tendon, but narrowing the front or rear positions of the popliteal hiatus, it still may cause the popliteal tendon adhesion or weakening or loss of sliding effect, thus affecting the relevant functions.18,19,23,24 Second, the traditional in-outside or out-inside suture techniques have to make knots out of the joint capsule. This might cause potential injuring the common peroneal nerve. Even the all-inside sutures have to be careful as well.25-29 Snyder et al. 5 reported the applications of hook all-inside mattress suture which was operated in the joint completely, without influences to the popliteal tendon and the popliteal hiatus, and injuring the common peroneal nerve. In this study, we also used the arthroscopic all-inside repair using a suture hook for the PFLM tears, and this suture technique has achieved good clinical effect in all 36 patients.
We acknowledge some limitations to this study. First, it was a single-site study at an academic medical center. Future prospective randomized studies with appropriate sample size need to detect the tear patterns of the PFLM. Second, because of the complexity of the meniscal tear patterns, we believe that our classification system may be difficult to include all the extensive and complex meniscus tears. However, this classification should be improved in further clinical application. Last, all patients have the excellent short-term follow-up results that these might be attributed to ACL and PLC surgery by restoring stability and reducing the subsequent risk of cartilage lesions.22,30 Therefore, these patients also need to evaluate and treat the clinical outcome at a prospective population-based comparative study.
Conclusion
This study suggests to possibly classify the PFLM tears for clinical practice. An arthroscopic all-inside repair using a suture hook for the traumatic PFLM tears can avoid stitching to popliteal tendon or narrowing the popliteal hiatus.
Footnotes
Authors’ Note
The study was performed at the Orthopaedic Center of People’s Liberation Army, Xiamen University Affiliated Southeast Hospital, Zhangzhou, China.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (81600696) and the Natural Science Foundation of Fujian Province of China (2019J01144).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Xiamen University Ethical Review Committee (ID: EC-11-012).
Informed Consent
Written informed consent was obtained from all subjects before the study.