
Abstract
Objective
Cartilage health is thought to be dependent on the relationship between mechanics, structure, and metabolism, rather than these individual components in isolation. Due to sex differences in cartilage health, there is need to determine if the relationships between these cartilage components separately for males and females. Therefore, we sought to determine the sex-specific associations between cartilage structure and metabolism at rest and their acute response following walking and drop-landing in healthy individuals.
Design
A cartilage ultrasound assessment and an ante-cubital blood draw were performed before and after walking and drop-landing conditions in 20 males and 20 females. Cartilage structure was assessed via medial and lateral femoral cartilage cross-sectional area. Cartilage metabolism was quantified with serum cartilage oligomeric matrix protein (COMP) concentration. Percent change scores from pre- to postloading were used to calculate acute alterations in cross-sectional area and COMP. Correlational analyses were used to assess the association between cartilage structure and metabolism measures separately for males and females.
Results
In females, greater resting COMP concentration was associated with less cartilage cross-sectional area in the medial(ρ = −0.50, P = 0.03) and lateral (ρ = −0.69, P = 0.001) femur. Resting cartilage measures were not associated among males. Following walking and drop-landing, percent change scores in cartilage structure and metabolism were not associated.
Conclusions
This study highlights that, in females, thinner anterior femoral cartilage is associated with greater resting serum COMP concentrations, a biomarker often linked to cartilage breakdown. Future studies into the relationships between various cartilage components should consider sex-specific analyses as these relationships are sex dependent.
Introduction
A decline in cartilage health is a hallmark sign of knee osteoarthritis (OA); therefore, being able to effectively monitor the underlying cartilage changes throughout the life span is critical for the successful early detection of OA development. 1 Cartilage health is influenced by the complex interplay between its structural (e.g., cartilage thickness), biological (e.g., metabolism), and mechanical (e.g., loading) properties. 2 While there are multiple modalities to assess cartilage structure, 3 ultrasound offers a valid, clinically-accessible, and cost-effective technique capable of assessing femoral cartilage.4,5 Cartilage metabolism is often quantified by assessing serum concentrations of cartilage oligomeric matrix protein (COMP) because it may reflect changes in cartilage breakdown 6 and is a potential indicator of OA. 7 In addition to evaluating the cartilage components in isolation, a multifaceted approach termed an integrated joint system 8 seeks to understand the interaction between this broad range of individual cartilage components to provide new insight to in vivo cartilage function.2,9,10
One approach to determine the interaction between the components of cartilage health is by assessing cartilage thickness (i.e., structure) and serum biomarkers (i.e., metabolism) prior to and following an acute bout of physical activity (i.e., acute loading).2,9,11 Since cartilage composition governs the ability of cartilage to deform in response to acute loading, previous investigations have quantified the change in cartilage thickness following acute loading (e.g., walking, running, landing) as a surrogate measure of cartilage composition.12-15 COMP is also considered mechanosensitive due to its role in binding structural components of cartilage that transduce force throughout the tissue. 16 Acute changes in serum COMP are observed following acute loading (e.g., walking, running, biking, drop-landing) that are attributed to whole-body cartilage turnover in response to mechanical loading.15,17-23 Previous studies have highlighted the importance of assessing the associations between the cartilage components in a young, healthy population before the development of OA, as these “healthy” associations may serve as benchmarks for future studies to identify disruptions in the homeostasis between cartilage components in individuals with OA.8,24 However, there is limited previous research with conflicting results that attempt to establish the “healthy” relationship between cartilage structure and metabolism before or after acute loading,15,20 and these studies do not take into account sex differences in cartilage that may affect the relationships between these cartilage components differently for males and females.
Sex differences have been demonstrated for prevalence, incidence, and severity of knee OA, 25 and may be attributed to sex differences in cartilage components that may be intrinsic and present before the onset of OA. 24 A previous review highlights the presence of extensive sex differences in outcomes assessing cartilage structure and metabolism. 24 Most studies assessing cartilage structure and metabolism include sex as a covariate, but sex-stratified analyses are recommended to better quantify sex differences in these outcomes. 24 Previous studies have identified assessing sex differences in the association between serum COMP and cartilage thickness as a need for future research, 26 and no studies have utilized an integrated joint systems approach to evaluate sex-specific association between cartilage structure and metabolism. Since onset and progression of OA is theorized to start once the “healthy” homeostasis between the cartilage components are disrupted, 8 there is a need to determine the associations between cartilage structure and metabolism outcomes separately for males and females prior to OA diagnosis. However, a recent review indicates that most research assessing the serum COMP response to acute loading have focused on populations that are male, older, and inactive. 11 Therefore, it is important to establish the associations in cartilage structure and metabolism separately for males and females in a young, active population.
This study uses an integrated joint system approach to provide a better understanding of the relationship between cartilage structure and metabolism. Thus, the first purpose of this study was to determine sex-specific associations between cartilage cross-sectional area (i.e., structure) and serum COMP concentration (i.e., metabolism) in young individuals without history of previous knee injury. Additionally, we wanted to determine the association between the acute change in cartilage cross-sectional area (i.e., cartilage deformation) and the acute change in serum COMP concentration following an acute bout of walking and drop-landing.
Methods
Design
The design used within this article is part of a larger study that has previously observed significant acute cartilage deformation and an acute increase in COMP concentration following walking and drop-landing.13,21 A femoral cartilage ultrasound assessment and an ante-cubital blood draw were performed in young, healthy individuals before and after 2 loading conditions (i.e., walking and drop-landing) to determine the resting values and acute cartilage responses (i.e., structural and metabolic) to each condition. We utilized a repeated-measures design in which each participant completed both conditions during independent data collection sessions separated by at least 1 week (12 ± 9 days) at the same time of day (0.3 ± 0.7 hours) to control for diurnal variation in serum COMP and femoral cartilage thickness.27-29 We counterbalanced the order in which participants conducted the walking and drop-landing conditions. Participants were instructed not to engage in any lower extremity strength training or running on both days that data collection occurred.
Figure 1 illustrates the flow of each data collection session. Participants were seated on a padded plinth with their back against a wall in a long-sit position with their knees in full extension for 1 hour to unload the femoral articular cartilage and minimize effects of any preceding activity.13,30 Next, the ultrasound cartilage assessment occurred immediately prior to the blood sample collection. To limit acute loading between the cartilage assessments and the loading conditions, the participants were transferred across the laboratory in a wheelchair to begin the loading condition. Immediately following cessation of each loading condition, the participants were transferred back to the padded plinth with a wheelchair to begin the posttest ultrasound assessment and blood sample collection. Posttest outcomes were obtained within 5 minutes following each condition. 13
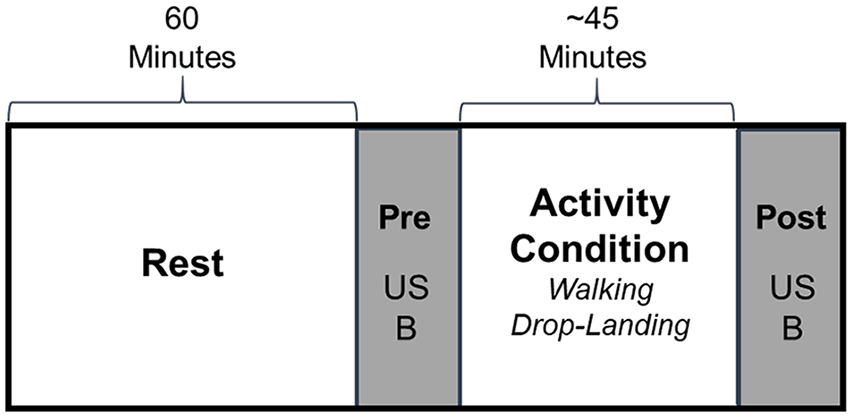
Description of the study design flow for each data collection session. Following a 60-minute rest, a femoral cartilage ultrasound assessment (US) and blood draw (B) occurring before and after a ~45-minute activity condition (i.e., walking or drop-landing). Participants completed both activity conditions during separate data collection sessions separated by at least 1 week.
Participants
We recruited a convenience sample of young, healthy individuals between the ages of 18 and 35 years who self-reported participating in at least 30 minutes of physical activity at least 3 times per week. We excluded individuals with a history of ligamentous or cartilage injury to the knee or hip, cartilage injury to the ankle, congenital or degenerative joint condition, orthopedic implant, lower extremity fracture, or upper extremity fracture. Additionally, those with current joint pain (quantified as greater than 2 on a 10-cm visual analog scale) were excluded from participation. We conducted an a priori power analysis that estimated we would need 17 participants within each sex to identify a significant moderate association (r = 0.60) between acute COMP change and acute medial femoral cartilage cross-sectional area deformation with an alpha level of 0.05 and power (1 − β) of 0.80. Due to the time commitment of multiple 3-hour data collection sessions, we over-sampled each sex by 18% (n = 3) to increase the likelihood that we would achieve adequate statistical power in our final analyses (i.e., total n = 40, male n = 20, female n = 20) in case of participant dropout. The study was approved by the university’s biomedical institutional review board, and all subjects provided written informed consent prior to participation.
Structural Assessment of the Femoral Cartilage
Femoral Ultrasound Image Acquisition
Ultrasound images were obtained from the participants’ dominant limb, which was defined as the self-reported limb used for kicking a ball. Participants were positioned with their back against a wall and their knee positioned to 140° of flexion using a manual goniometer ( Fig. 2A ). 12 A single unblinded investigator (MSH) with more than 4 years of experience performed all imaging using a LOGIQe ultrasound system (General Electric Co., Fairfield, CT, USA) with a 12-MHz linear probe. All ultrasound system settings were consistent between each time-point, condition, and participant. The probe was placed transversely in line with the medial and lateral femoral condyles above the superior edge of the patella and rotated until the probe was perpendicular to the femoral cartilage surface to maximize the reflection of the cartilage ( Fig. 2A ).4,31,32 Three images were recorded, with the ultrasound probe being removed and repositioned on the knee between each recorded image, prior to (i.e., resting) and immediately after the walking and drop-landing conditions. A more detailed account of our methods for ultrasound image acquisition has been described in earlier studies.12,13,33
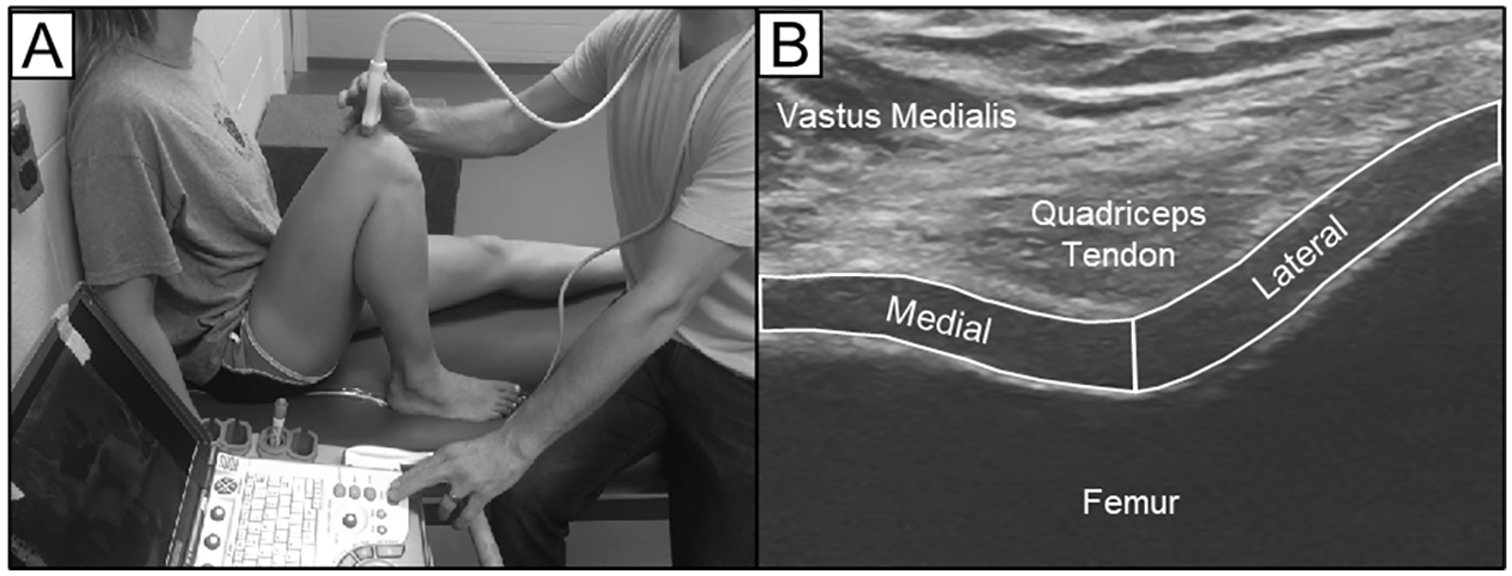
Ultrasound acquisition and processing of femoral cartilage. (A) Patient and ultrasound probe positioning and (B) cross-sectional area technique.
Femoral Ultrasound Cross-Sectional Area
The femoral cartilage was manually segmented using ImageJ software (National Institutes of Health, Bethesda, MD, USA) by individually outlining the cartilage of the medial and lateral femoral condyles to obtain the cartilage cross-sectional area (mm2). 13 The medial and lateral areas were separated by a line drawn perpendicular to the lowest point of the cartilage surface of the intercondylar notch ( Fig. 2B ). We have established strong intra- and intersession reliability for cartilage cross-sectional area in the medial (intrasession intraclass correlation coefficient [ICC]2,k = 0.99, standard error of the measurement (SEM) = 0.68 mm2; intersession ICC2,k = 0.98, SEM = 1.16 mm2) and lateral (intrasession ICC2,k = 0.99, SEM = 0.91 mm2; intersession ICC2,k = 0.98, SEM = 1.09 mm2) condyles. 13
For data analysis, all ultrasound images from each time point were processed and averaged. For the resting baseline analysis, we utilized resting cartilage cross-sectional area prior to the walking condition. For the change analysis, we calculated the cartilage deformation (i.e., percent change from pre- to posttest) following the walking and drop-landing conditions. A negative percent change of cross-sectional area indicates cartilage deformation.
Quantifying Cartilage Metabolism
Blood Sample Collection
For both the pre- and posttest time points, the participants were positioned supine on the padded plinth, and 5 mL of blood were collected from the antecubital vein in a serum separator tube vacutainer. Blood samples were placed on ice until the completion of each data collection session (~1.5 hours). The samples were then centrifuged at 4°C for 15 minutes at 4,000 rpm, serum was pipetted equally into 2 cryovials, and stored at −80°C until a batch analysis that occurred at the completion of the study.
Analysis of Serum COMP
We quantified cartilage metabolism with serum COMP using commercially available enzyme-linked immunosorbent assays (Human COMP PicoKine ELISA; Boster Biological Technology; Pleasanton, CA, USA). Blood samples were analyzed in triplicate. The COMP assay detection sensitivity was <10 pg/mL, and the intra-assay coefficient of variability was 2.35%. Serum samples for each participant were analyzed on a single plate to control for differences caused by inter-assay variation. For the resting analysis, we utilized resting serum COMP concentration prior to the walking session. For the change analysis, we calculated the acute COMP response (i.e., percent change from pre- to posttest) following the walking and drop-landing conditions. Serum concentrations of COMP provide a global measure of cartilage metabolism throughout the entire body. 34
Walking and Drop-Landing Activity Conditions
Familiarization Session Used to Determine Duration of the Walking and Drop-Landing Conditions
Prior to testing, participants performed an initial familiarization session to determine their habitual walking speed and corresponding comfortable step frequency. Habitual over-ground walking speed was initially determined by utilizing 2 sets of infrared timing gates (TF100, TracTronix, Lenexa, KS, USA). Participants were instructed to walk at a self-selected speed described as “comfortably walking on the sidewalk” through the 6-m area.35-37 After completing 5 familiarization trials, we recorded the time of the next 5 walking trials to determine their average habitual walking speed. Next, participants completed 60 seconds of walking on a treadmill (4Front, WOODWAY, Waukesha, WI, USA) at their determined habitual walking speed for familiarization. After treadmill familiarization, participants continued walking on the treadmill at their habitual walking speed while study personnel manually counted the number of steps they took for an additional minute. Using their steps per minutes, we calculated the time each participant would need to reach 5,000 steps (46.2 ± 4.3 minutes). 38 The calculated time for each participant was used for the duration of both the walking and drop-landing conditions. The participants wore the same pair of their personal athletic footwear for the walking and drop-landing conditions.
Walking Condition
Participants walked on a treadmill at their predetermined habitual walking speed. This speed was maintained for the duration calculated during the screening session to reach 5,000 steps (46.2 ± 4.3 minutes). Based on the results of a subset of our participants wearing a pedometer, we are confident that our walking protocol is an effective way of estimating the time needed to reach 5,000 steps (n = 23; mean ± standard deviation = 5,004 ± 258 steps).
Drop-Landing Condition
The participants performed 120 drop-landings from a 62-cm platform. We selected 120 drop-landings in order to match the magnitude of loading in a previous study utilizing a similar drop-landing protocol. 15 For each drop-landing, the participants ascended a set of 2 steps to position themselves on the platform and were instructed to drop down from the platform and perform a comfortable landing. 13 No specific instructions were provided regarding how to land. After each drop-landing, participants would ascend the steps to prepare for the next drop-landing trial. The 120 drop-landing trials were evenly distributed over the same time period utilized in the walking condition (46.2 ± 4.3 minutes).
Statistical Analysis
Group Demographics
Age, body mass index (BMI), and Tegner Activity Level Scale (0-10; 10 = highest level of activity) were compared between males and females with independent-samples t tests. Additionally, we compared walking speed and distance from the walking condition between males and females with independent-samples t tests.
Association between Resting and Acute Changes in Cartilage Cross-Sectional Area and COMP
Shapiro-Wilk tests were used to determine the normality of our resting values and acute changes in cartilage cross-sectional area and COMP for the overall group and separately for males and females. If the data were normally distributed, separate Pearson product moment correlations were used. If the data were nonnormally distributed, Spearman rank-order correlations were used. We defined outliers as data points greater than three standard deviations away from the mean for all outcomes for the overall group and separately for males and females. For the resting analysis, we determined the association between resting cartilage cross-sectional area and resting COMP concentration in the walking condition. For the change analysis, we determined the separate associations between acute cartilage deformation and the acute COMP response following the walking and drop-landing conditions (i.e., %Δ scores). Association magnitudes (i.e., Pearson r or Spearman ρ) were classified as negligible (0.0-0.30), weak (0.31-0.50), moderate (0.51-0.70), strong (0.71-0.90), and very strong (0.90-1.00). 39 We performed the same association analyses separated for males and females to specifically determine the sex-specific association between resting and acute change in cartilage structure and metabolism. All statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA) with an a priori α level of P < 0.05.
Results
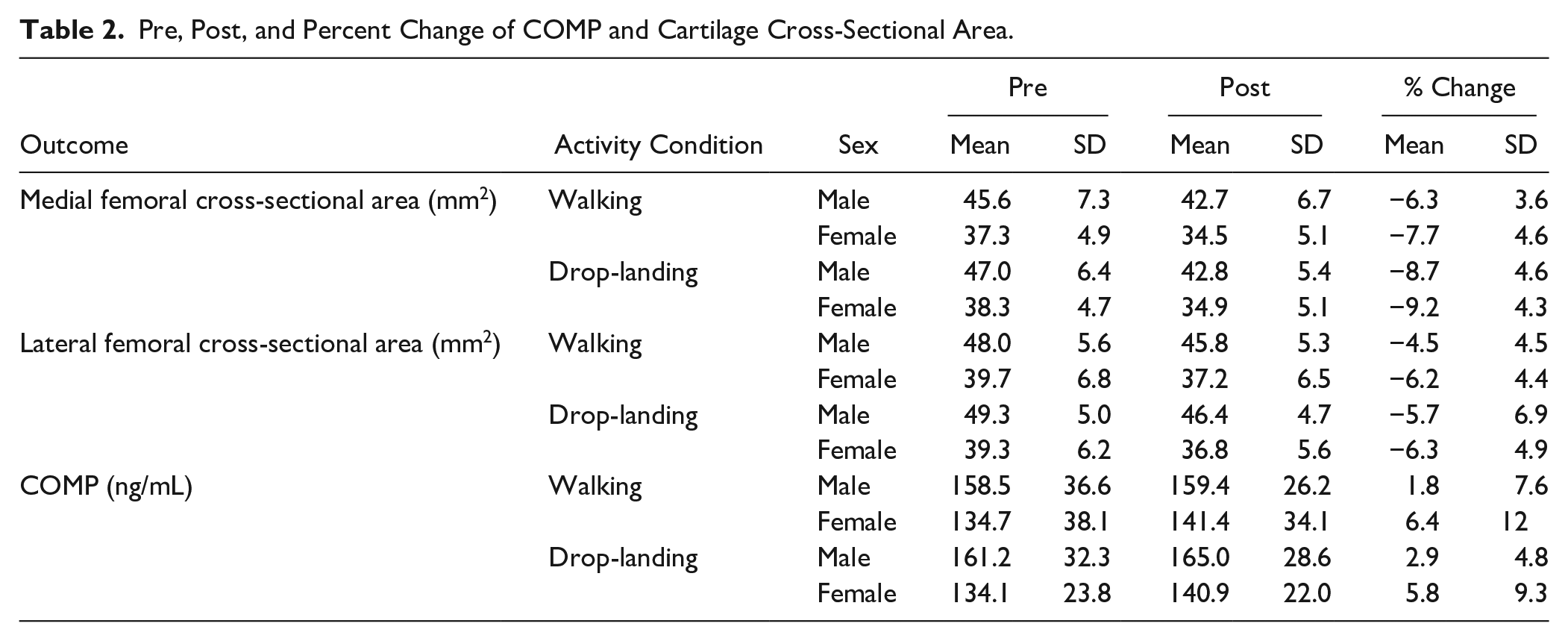
A total of 40 participants were included in this study ( Table 1 ). However, due to participant dropout between data collection sessions, 39 participants completed each data collection session. The drop-out in the walking condition was due to an unrelated injury in a female participant between the 2 sessions, and the drop-out in the drop-landing condition was due to a male participant being unwilling to complete the drop-landing protocol. There were no sex differences in age, physical activity, BMI, or walking speed/distance (Table 1). Sex-specific descriptive statistics for the pretest, posttest, and percent change of cartilage cross-sectional area and COMP following walking and drop-landing can be found in Table 2 .
Demographics.
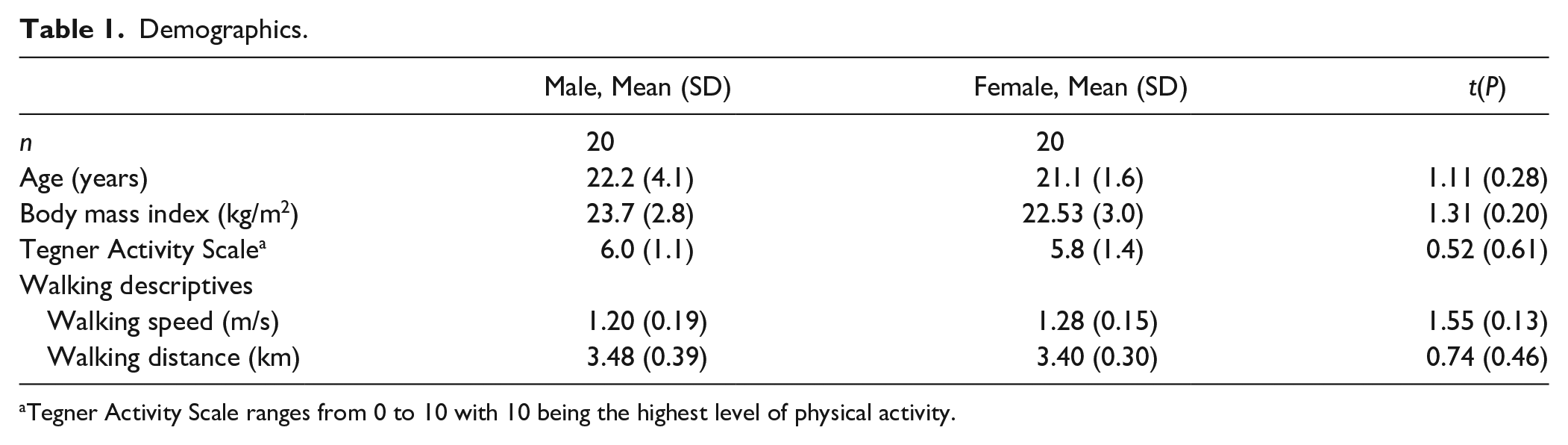
Tegner Activity Scale ranges from 0 to 10 with 10 being the highest level of physical activity.
Pre, Post, and Percent Change of COMP and Cartilage Cross-Sectional Area.
Association between Resting Cartilage Cross-Sectional Area and COMP Concentration
As resting COMP concentration was non-normally distributed in the overall group, as well as separately for males and females. For the overall group, one outlier (i.e., male participant) was removed from the analysis due to an extremely high resting COMP concentration. There were no outliers for any outcome when separated by sex. Resting COMP concentration was not significantly associated with either the medial or lateral cartilage cross-sectional area for the overall group and in the male participants ( Table 3 ). In females, greater resting COMP concentration was significantly associated with smaller medial (ρ = −0.50, P = 0.03) and lateral (ρ = −0.69, P = 0.001) cartilage cross-sectional area ( Table 3 ; Fig. 3 ).
Sex-Specific Associations between Resting COMP and Resting Cartilage Cross-Sectional Area.
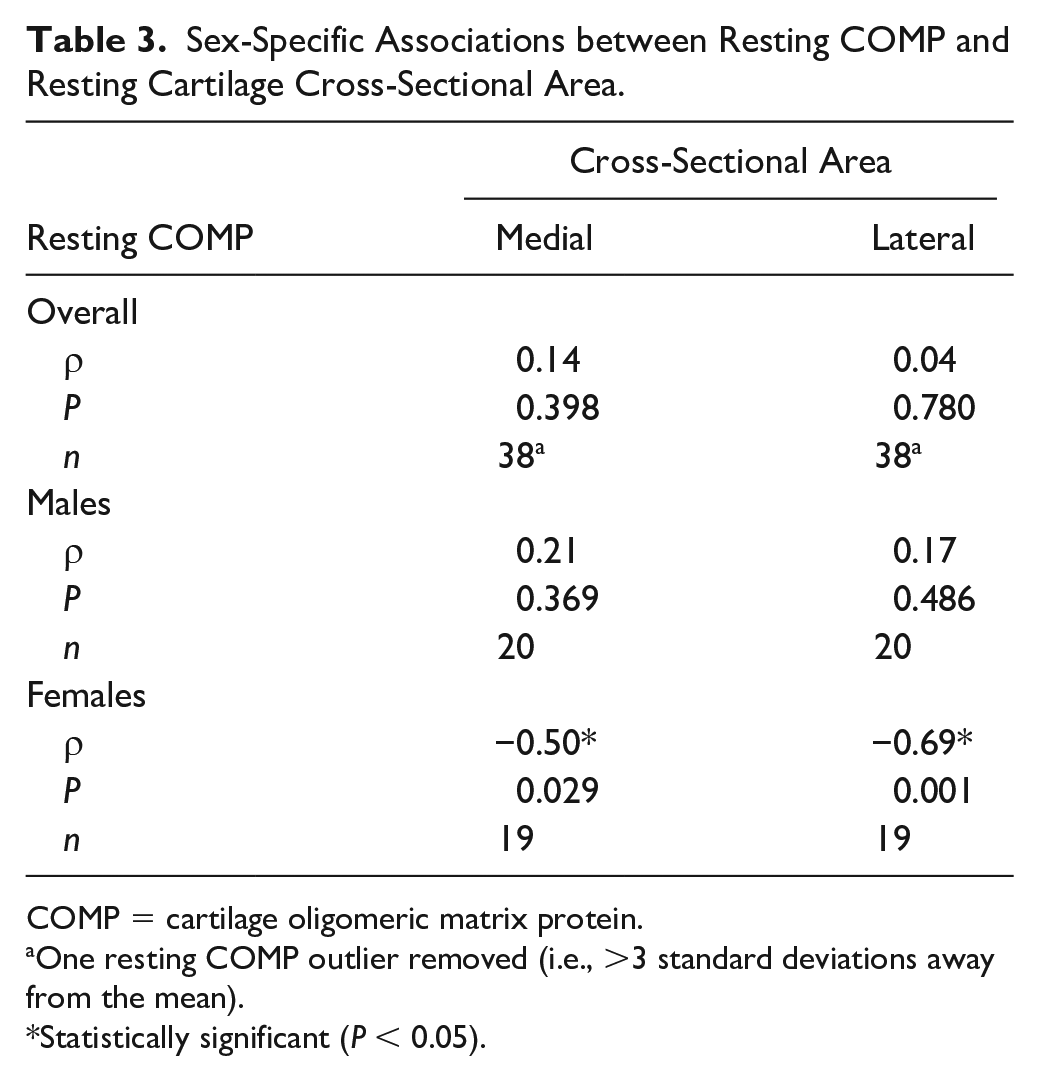
COMP = cartilage oligomeric matrix protein.
One resting COMP outlier removed (i.e., >3 standard deviations away from the mean).
Statistically significant (P < 0.05).
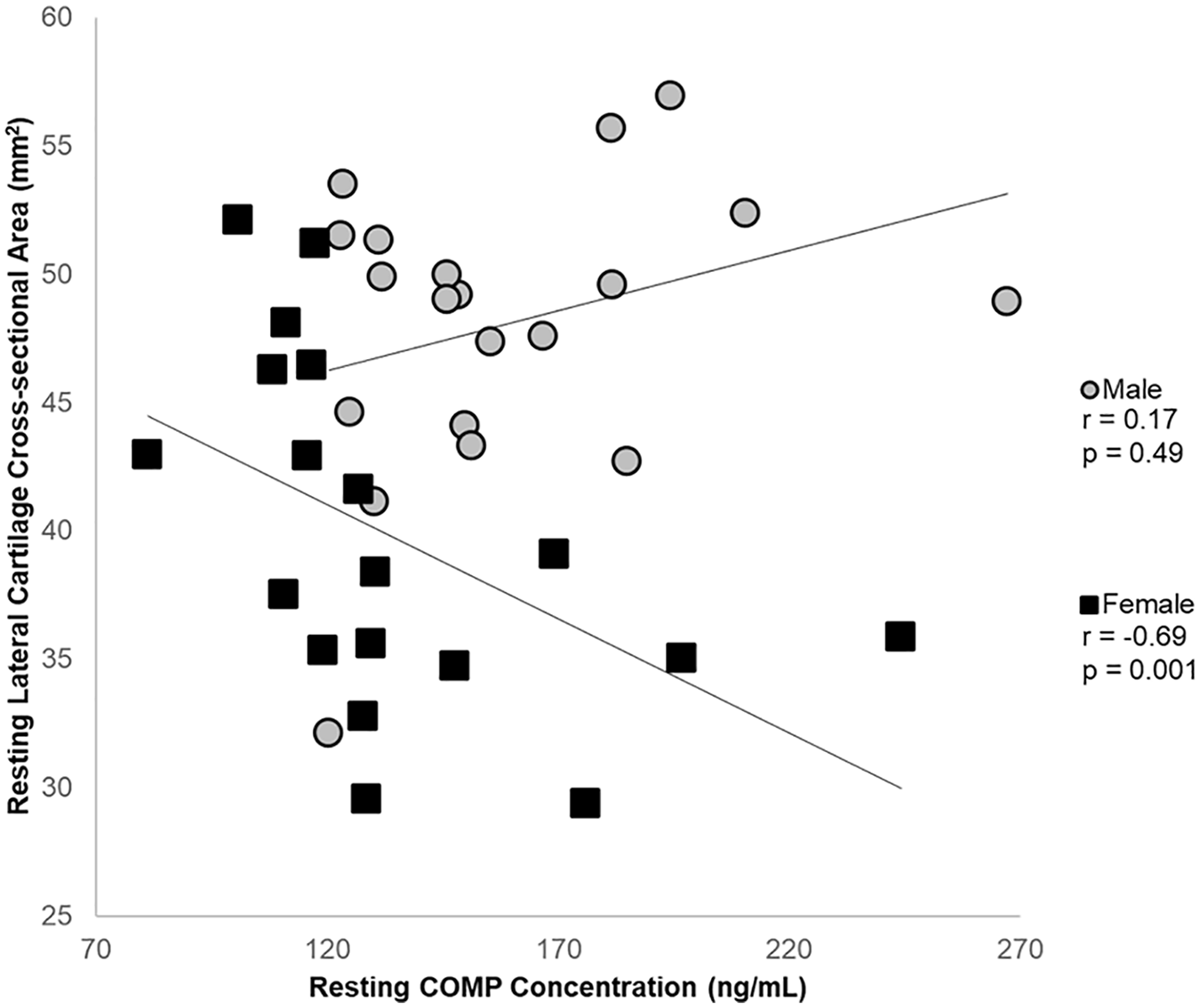
Sex-specific association between resting lateral cartilage cross-sectional area and resting cartilage oligomeric matrix protein (COMP) concentration.
Association between Acute Cartilage Deformation and Acute COMP Response
For walking, acute COMP response and medial/lateral acute cartilage deformation were normally distributed for the overall group, as well as separately for males and females. There were no outliers for any outcome for the overall group or when separated by sex. Following walking, there were no significant associations between acute COMP response and acute cartilage deformation for the overall cohort or specifically in males and females ( Table 4 ).
Sex-Specific Associations between COMP Change and Acute Cartilage Deformation.
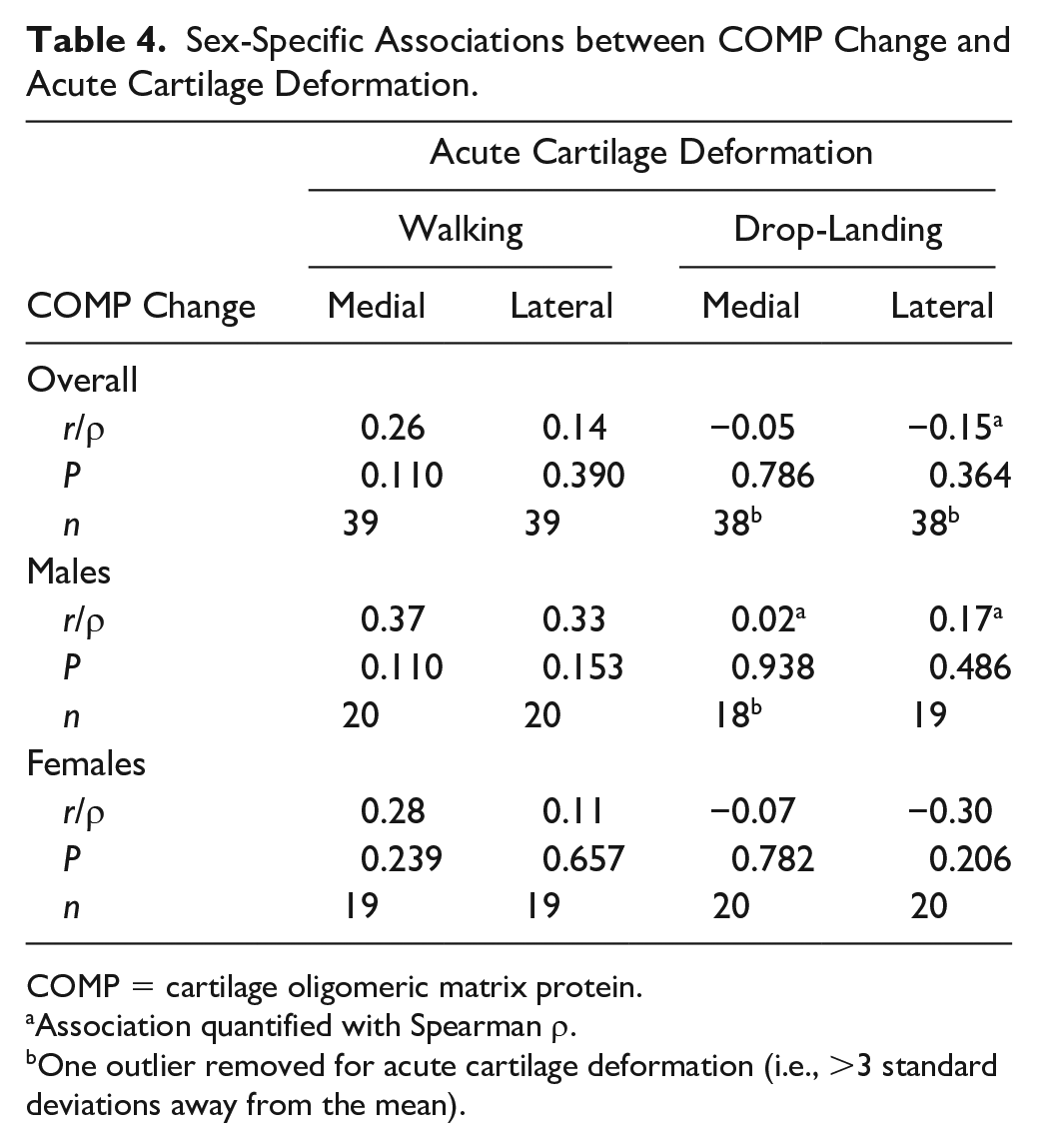
COMP = cartilage oligomeric matrix protein.
Association quantified with Spearman ρ.
One outlier removed for acute cartilage deformation (i.e., >3 standard deviations away from the mean).
For drop-landing, lateral acute cartilage deformation was nonnormally distributed for the overall group, while medial and lateral acute cartilage deformation were nonnormally distributed for the males. For the overall group, there was an outlier for both medial and the lateral cartilage deformation analyses, as well as an outlier in the male analysis for medial cartilage deformation. Following drop-landing, there were no significant associations between acute COMP response and acute cartilage deformation for the overall cohort or specifically in males and females ( Table 4 ).
Discussion
This study highlights sex-specific associations between resting femoral cartilage structure and cartilage metabolism in young, healthy individuals, as well as the lack of significant associations between acute cartilage deformation and acute COMP response following walking and drop-landing. Although there were no statistically significant associations between cartilage structure and metabolism when combined males and females into a single cohort, the sex-specific analyses indicate that sex may influence the association between resting cartilage structure and metabolism. Specifically, females presented with a positive association between cartilage structure and metabolism that indicated that greater resting COMP concentration was significantly associated with thinner cartilage in both the medial and lateral femur. This finding helps to highlight the general lack of associations between cartilage structure and metabolism at rest and following acute loading, but provides compelling evidence that futures studies need to consider sex-specific analyses to more accurately investigate the associations between various cartilage components. Due to the lack of association between cartilage structure and metabolism following an acute bout of walking and drop-landing, this indicates that the localized anterior femoral cartilage ultrasound assessment and the global measure of serum COMP quantify different aspects of the cartilage response to common loading conditions.
To our knowledge, this is the first study to determine the association between ultrasound measures of resting cartilage structure and serum COMP concentrations in young, healthy individuals. A previous cross-sectional investigation in individuals with OA, however, observed that greater resting COMP concentration was associated with smaller medial femoral cartilage volume assessed with magnetic resonance imaging (MRI). 40 Those authors suggested that greater resting COMP concentrations are indicative of greater femoral cartilage degradation, and that the association with smaller cartilage volume is due to long term alterations in cartilage metabolism leading to cartilage thinning. 40 We observed a similar cross-sectional association in our female participants as greater resting COMP concentrations were associated with smaller medial and lateral cartilage cross-sectional area, but there was no significant association observed in the male cohort ( Fig. 3 ). We cannot definitively state why there is this discrepancy between males and females, but there are intrinsic cartilage differences between males and females that may help to understand this sex-specific association. Females present with smaller knee cartilage compared with males, even after normalizing cartilage size to height and weight, over a continuum of age ranges spanning from early in life to older individuals at risk of OA development.41,42 Additionally, healthy knee cartilage structure is theorized to be conditioned to the mechanics applied to the joint during walking gait. 43 Since females present with different gait biomechanics, greater tibiofemoral cartilage contact area, and less bony congruency between the tibia and femur compared to males, this may result in the cartilage being loaded differently between the sexes.44-46 Moreover, hormonal imbalances (e.g., estrogen) appear to be involved in maintaining cartilage health, which may play a role in the relationship between cartilage structure and metabolism.47,48 While the interaction between cartilage loading, structure, and metabolism is very complex, these intrinsic differences in cartilage mechanics and hormonal imbalances between males and females may explain the sex-specific association between resting cartilage structure and metabolism. Further longitudinal data are needed to determine if this significant association between cartilage structure and metabolism in females persists, and to determine if sustained higher levels of COMP lead to progressive decline in cartilage structure.
In our overall and sex-specific analyses, we did not observe a significant association between acute cartilage deformation and acute COMP response following walking or drop-landing. Previous studies have speculated that greater acute cartilage deformation would lead to a greater increase in COMP concentration.19,20 However, a previous study observed the opposite following a drop-landing condition, greater overall MRI-assessed tibiofemoral cartilage deformation was associated with lesser increase in COMP concentration. 15 Within this same study, 15 there was not an association between cartilage deformation and COMP response following 30 minutes of running, despite a prior study observing that a running bout of 1 hour produced an acute COMP response associated with cartilage deformation. 20 One reason for the conflicting results between our study and the previous studies may be due to differences in the location and timing of the cartilage assessments. The ultrasound assessment used within our study provides a localized assessment of the anterior femoral cartilage, while the previous MRI study averaged the cartilage deformation throughout the entire articulating surface of the femur. 15 Since the volumetric MRI assessment averages deformation throughout a large region that may be experiencing different magnitudes of deformation, the MRI assessment may not be sensitive to detecting local changes in cartilage morphology.14,49 Also, due to the accessibility of the ultrasound assessment, we captured postloading images within 2 minutes following the end of loading, while the prior MRI study did not obtain images until ~20 minutes following loading. 15 Additionally, in contrast to the localized ultrasound cartilage assessment, the serum COMP concentrations provide a global measure of cartilage metabolism throughout the entire body. 34 Thus, the lack of association between our acute cartilage deformation and the acute COMP response may be due to the COMP response providing a whole-body cumulative measure of acute cartilage turnover that is not representative of the localized cartilage deformation in the anterior femur assessed via ultrasound. Since there was no association between the cartilage structure and metabolic response to loading, this may indicate that these 2 outcomes quantify different aspects of how loading acutely affects cartilage health.
While this study provides information regarding the relative lack of an association between cartilage structure and metabolism, there are some limitations that will inform future research. A reader conducted the ultrasound image acquisition and processing unblinded to the order of time as this has been used previous to maximize the sensitivity to change.50,51 However, this could have introduced bias in the ultrasound results. Therefore, future studies may consider utilizing blinded readers who are unaware of time to minimize bias introduced into the analysis of cartilage deformation. Within our study design, we always conducted our ultrasound analysis prior to the blood sample collection. There is a small likelihood that this discrepancy in timing between the measures could affect their associations. However, due to the accessibility of the ultrasound assessment we were able to collect all post measurements within 5 minutes and believe that our ultrasound and COMP measures represent the same time course following loading. The ultrasound protocol provides a localized assessment of the anterior femoral cartilage, but due to bony alignment this technique is unable to provide an assessment of cartilage in the tibia or posterior femur. However, cartilage thickness using this protocol is associated with walking biomechanics and thus highlights the relevant location of the cartilage assessed with ultrasound. 52
Conclusions
Females with greater resting serum concentrations of COMP present with smaller ultrasound-assessed medial and lateral femoral cartilage cross-sectional area, but this significant association is not observed in male participants. Due to the lack of association between cartilage structure and metabolism following the same bout of joint loading, this indicates that the localized anterior femoral cartilage ultrasound assessment and the global measure of serum COMP quantify different aspects of the cartilage response to common loading conditions. Future studies that continue to investigate the association between cartilage structure and cartilage metabolism should consider performing sex-specific analyses, as combining the sexes may confound the results.
Footnotes
Acknowledgments and Funding
We would like to thank Arianna Douglas, Ryan Fockler, Daniel Farrell, Samantha Hammock, Leslie Sierra-Arévalo, Gabrielle Smith, Nicole Thomas, and Kyle Wolfe for their help with data collection and data processing. MSH was supported by the Royster Society of Fellows within the Graduate School at the University of North Carolina at Chapel Hill (Ross and Charlotte Johnson Family Dissertation Fellowship) and the National Institutes of Health (Grant No. 5TL1TR001454).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the university’s biomedical institutional review board (IRB# 16-0231).
Informed Consent
All subjects provided written informed consent prior to participation.
Trial Registration
Not applicable