
Abstract
Aim
To demonstrate the immediate and medium-term results of the surgical treatment of patients with first metatarsophalangeal (MTP) joint osteoarthritis (OA) using the autologous matrix-induced chondrogenesis (AMIC) technique and to evaluate the effectiveness.
Materials and Methods
Preoperatively the range of motion (ROM) in the first MTP joint was determined, and the following questionnaires were used: Visual Analogue Scale (VAS) of pain, American Orthopedic Foot & Ankle Society (AOFAS) score, and Functional Foot Index (FFI). All of the patients experienced a significant restriction of the ROM in the first MTP joint. The VAS of pain median was 70, AOFAS 52, and FFI 5.8.
Results
AMIC was performed in 19 patients with first MTP joint OA. All the patients experienced a significant restriction of ROM in the first MTP joint. The VAS of pain median was 70, AOFAS 52, and FFI 5.8. By the third month, VAS of pain decreased to 25, FFI to 2.2; AOFAS median increased to 77, ROM to 60°. Six months after the surgery VAS of pain decreased to 10, FFI to 1.1; AOFAS median increased to 90, ROM to 65°. After a year of observation, VAS of pain decreased to 5, FFI to 1,0; AOFAS median increased to 92.5, ROM to 71.5°.
Conclusion
The results showed that a first MTP joint AMIC procedure can be a fairly effective method of surgical treatment that can relieve pain and significantly improve the quality of life of patients with first MTP joint OA.
Introduction
The first metatarsophalangeal (MTP) joint osteoarthritis (OA) is a disease characterized by pain, which is aggravated by walking, stiffness in joint, and a decreased range of motion (ROM), especially of dorsal flexion. First MTP joint OA is the second most frequent pathological condition of foot after hallux valgus deformity and is found, according to various sources, in 2.5% to 10% of the adult population.1,2 Currently, there are many different methods of surgical treatment of the first MTP joint OA, such as cheilectomy, shortening osteotomy of the first metatarsal bone (MB), hemiarthroplasty, endoprosthetics, and arthrodesis of the first MTP joint. All of them have both advantages and disadvantages.3 -7 For patients with disease stages I and II by X-ray classification with moderate or intermittent pain and stiffness, the recommended method of surgical treatment is cheilectomy. 8 However, cheilectomy does not restore damaged areas of articular cartilage; therefore, the pain syndrome may recur with time. Canseco et al. 9 did not observe any ROM increase in the first MTP joint after cheilectomy in their study. The authors pointed to the need for the development of rehabilitation measures after surgical treatment. In addition, according to Seibert and Kadakia, 10 cheilectomy is contraindicated at the late stages of the disease, when less than 50% of the articular surface of the first MTP joint remains intact.
Shortening osteotomy of the first MB is relevant in case of its excessive relative length1,6 and distal oblique osteotomy—in case of the excessive elevation of the first MB. 11 With normal anatomical size and position of the first MB, the question of the expediency of these operations remains open. Moreover, the occurrence of the overload metatarsalgia is a quite common complication of the shortening osteotomy. 12
Keller arthroplasty is often used in elderly patients. It provides rapid relief of pain and a short recovery period, but this operation can lead to a significant shortening of the first toe and the development of instability in the first MTP joint. 7 According to Pakhomov et al., 13 40% of patients who underwent Keller arthroplasty were not satisfied with its result due to relapse of pain, osteophytes, and the formation of the first MTP joint fibrous ankylosis, observed in 21 of 25 cases in this investigation.
The first MTP joint arthrodesis is considered to be the “gold standard” of surgical treatment of OA at the late stages. This method solves the primary problem of hallux rigidus—to relieve pain during movements.7,14 However, researchers indicate that arthrodesis does not fully restore normal walking biomechanics due to the movements reduction. 15
The first MTP joint hemiarthroplasty and endoprosthetics have been used for more than 60 years. 5 Since 1967, silicone prostheses were used, but postoperative results were unsatisfactory, and their use was discontinued.6,16 Furthermore, with the development of the prostheses manufacturing technology the results of surgical treatment improved. Currently, the results of the first MTP joint endoprosthetics often remain unsatisfactory, and therefore this type of surgical treatment cannot be recommended as the method of choice.1,16
To date, there is no single surgical approach to solve the problem of first MTP joint OA. In turn, it is known that in the presence of bone-cartilaginous defects in the knee,17,18 hip, 19 and ankle 20 joints, autologous matrix-induced chondrogenesis (AMIC) is quite successfully used. In the knee joint AMIC can be performed both arthroscopically or using a minimally invasive open incision. In a number of studies, positive results were obtained—the majority of patients were satisfied with the postoperative outcome, reporting a significant decrease of pain.17,18 As for the hip joint, an arthroscopic technique is used for performing AMIC. Fontana and de Girolamo reported the high effectiveness of AMIC in the treatment of cartilage defects of the acetabulum. 19 As for the ankle joint, arthroscopy is used at the first stage with the aim of identifying the possible instability of the ligaments and to determine the location and size of osteochondral lesions. The second stage is arthrotomy using anteromedial or anterolateral incision, depending on the location of the defect zone. Usuelli et al. estimated the immediate postoperative results as positive—all scores used in this investigation significantly improved (P < 0.05) with respect to preoperative values after 6 months. 20 In this regard, we proposed the use of this technique in the treatment of patients with first MTP joint OA, including the late stages of the disease.
Materials and Methods
This study was approved by the ethics committee of V.A. Nasonova Research Institute of Rheumatology in 2018. From October 2017 to January 2020 in V.A. Nasonova Research Institute of Rheumatology, first MTP joint chondroplasty was performed in 19 patients: 14 women and 5 men. Recruitment of patients for the study was carried out using the following exclusion criteria: patients younger than 18 and older than 74 years, body mass index >40, the presence of systemic inflammatory diseases of medium and high activity, and the presence of infection. The median age of the patients was 52 years (minimum age was 20 years, maximum age was 71 years). To assess the condition of patients before the surgery, the total ROM in the first MTP joint was determined, and the following questionnaires were used:
Visual Analogue Scale (VAS) of pain—from 0 to 100 mm, where 0 = no pain, 100 mm = maximum intensity
The American Orthopedic Foot & Ankle Society (AOFAS) score—from 0 to 100 points, where 0 is the worst condition of the foot, 100 is the best 21
Functional Foot Index (FFI)—from 0 to 10, where 0 is the best score, 10 is the worst 22
Due to the presence of small sample for each of the estimated parameters, median values were calculated instead of average.
The clinical status of patients before surgery is presented in Table 1 . All patients had a significant restriction. The minimum ROM was 0°, the maximum 50°, and the median 20°. The VAS of pain median was 70 (minimum 20, maximum 90), while the AOFAS median was 52 (minimum 39, maximum 62). Before surgery the FFI median was 5.8 (the minimum index was 2.0, the maximum was 8.2; Table 1 ).
Clinical Status before the Surgery.
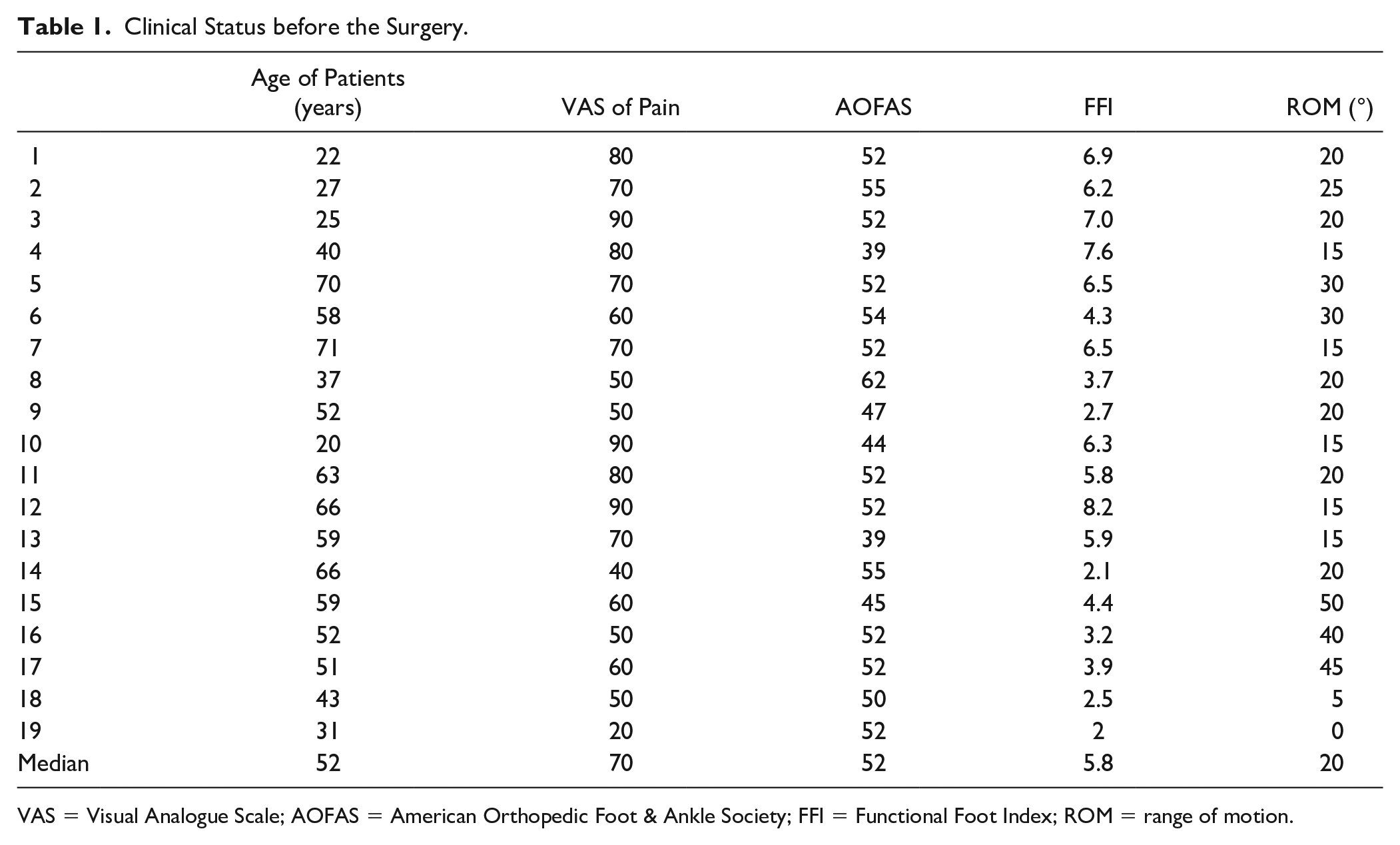
VAS = Visual Analogue Scale; AOFAS = American Orthopedic Foot & Ankle Society; FFI = Functional Foot Index; ROM = range of motion.
To evaluate the clinical and radiological status before the surgery, the Coughlin-Shurnas classification was used ( Table 2 ). 23 In this classification, there are 5 grades of the disease (from 0 to 4). It uses characteristics such as state of the first MTP joint gap, pain syndrome features, and limitation of the ROM.
Coughlin and Shurnas Classification.
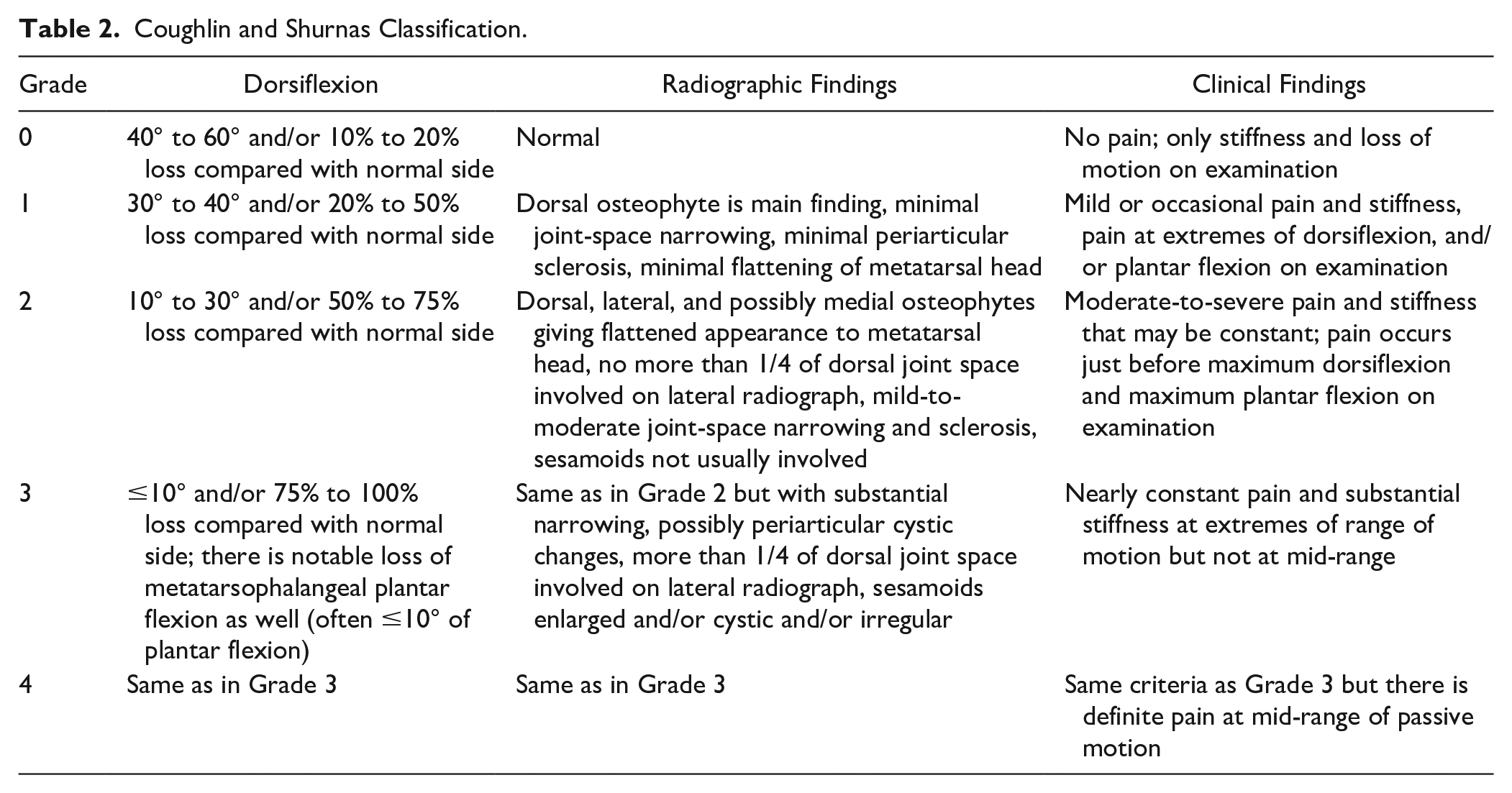
According to Coughlin and Shurnas classification, 3 patients had the first MTP joint OA at the grade 2, 11 patients grade 3, and 5 patients grade 4.
The presence and size of the defect in the cartilaginous coating of the head of the first MB was determined intraoperatively. If the cartilage defect was less than 3 mm, we debrided it, did a microfracture, and inserted the membrane. Single cartilage defects with a diameter of more than 3 mm were subjected to chondroplasty ( Fig. 1 ), as well as multiple defects, regardless of size. If it was larger than 3 mm or had multiple defects, we took the entire cartilage surface off, microfractured it, and then inserted the membrane. In most cases (12 operations), multiple cartilage defects were detected in combination with the presence of osteophytes ( Fig. 2 ), and a total cheilectomy was performed with the entire first MB head area covering by collagen matrix.
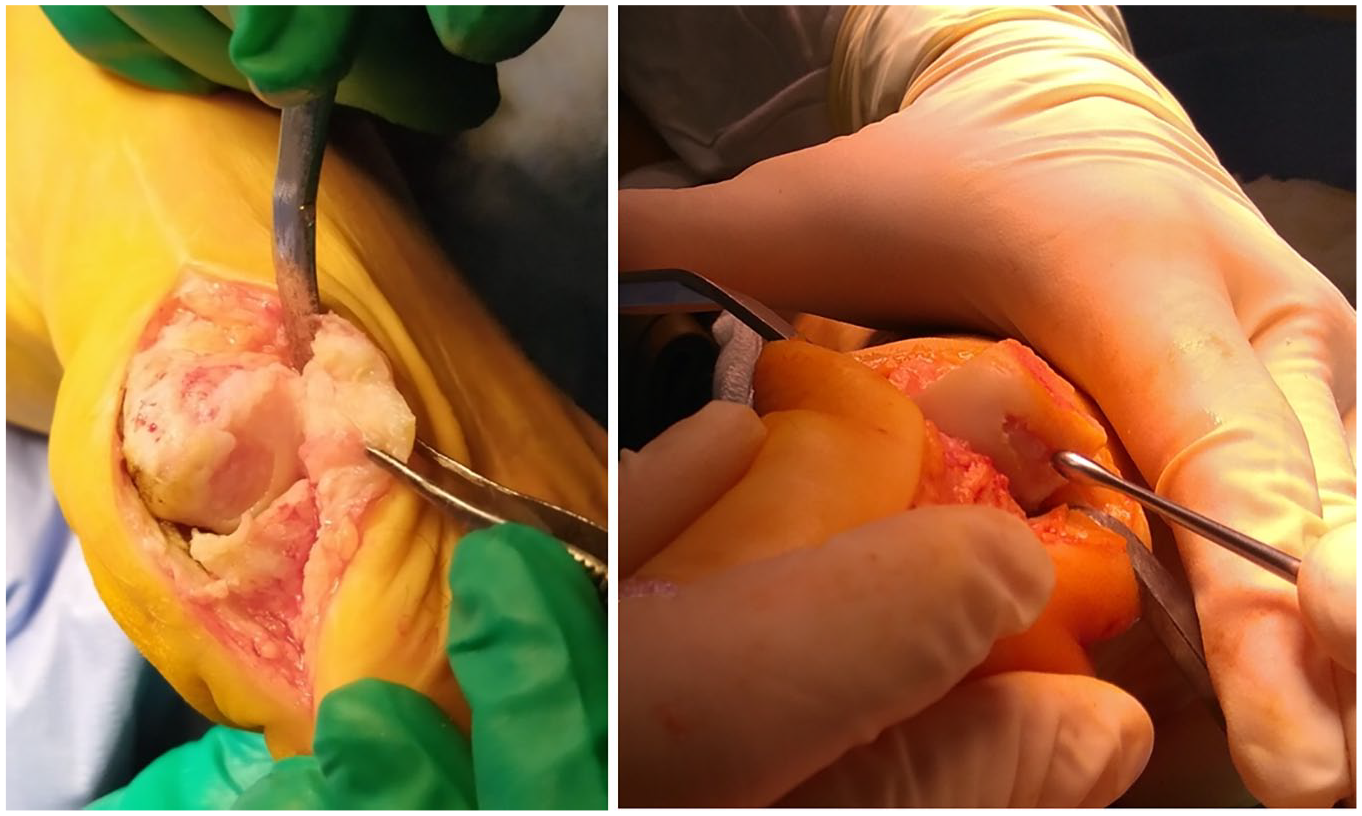
Single cartilage defects with a diameter of more than 3 mm.
Multiple cartilage defects.
The first MTP joint chondroplasty was performed using the AMIC technique with Chondro-Gide or Aesculap Novocart Basic collagen matrices. The matrix consists of types I to III collagen. It has a 2-layer structure with a dense side and a porous side. The dense layer has a smooth surface that is not permeable to cells, preventing the penetration of mesenchymal stem cells into the joint cavity. The porous layer consists of loose collagen fibers that promote cell adsorption. The matrix is made of porcine (Chondro-Gide) or bovine (Aesculap Novocart Basic) collagen, which, sometime after the operation, is naturally resorbed by enzymes to free amino acids. In the manufacturing process, telopeptides, the main determinants of antigenicity, are removed from collagen. Thus, the collagen matrix has minimal immunogenic potential.17,18 The decision to use the Chondro-Gide or Aesculap Novocart Basic collagen matrices was determined by the presence of a particular matrix at our disposal. There were no specific indications for using a particular matrix.
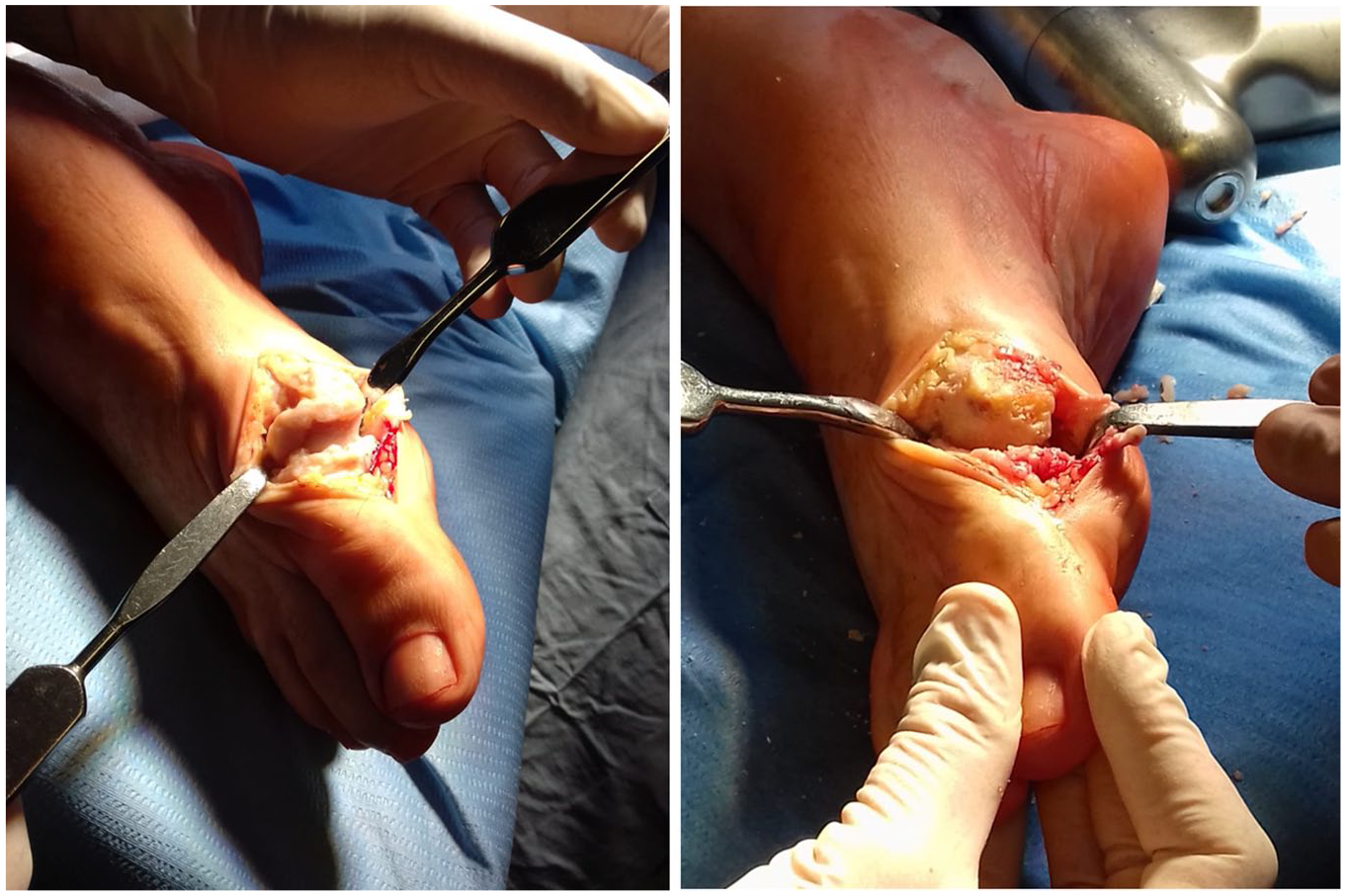
The operation was performed as follows: a direct medial skin incision was performed in the first MTP joint projection with a length of 4 cm, followed by mobilization of the skin with subcutaneous fat, exposing the joint capsule and arthrotomy ( Fig. 3 ). The osteophytes were removed from the head of the first MB and the base of the proximal phalanx of the first toe—cheilectomy; the area of the cartilage defect on the head of the MB to the subchondral bone was processed ( Fig. 4 ), microfracturing ( Fig. 5 ) of this area was performed using a thin needle (the distance between microperforations was 2-3 mm), and the defect was covered with a prepared bilayer collagen matrix ( Fig. 6 ), which was fixed along the edges to the intact cartilage and/or periosteum using a thin absorbable threads—PDS, Vicryl, or Monosyn 6-0 ( Fig. 7 ). It is important to pay attention to the fact that the matrix should cover the defect with a porous layer to the bone surface.

Osteophytes on the first MB head.

Cheilectomy, removing of damaged cartilage.

Microfracturing.

Placing of the collagen matrix.

Fixation of the matrix with absorbable suture.
Before inserting the collagen matrix, it was kept in a 0.9% NaCl solution for 7 minutes, after that the matrix was trimmed along the edge of the defect ( Fig. 8 ).
Preparation of the collagen matrix.
According to the AMIC technique, the axial load on the operated joint should be prevented for a month after the operation17,20; therefore, a mandatory condition for postoperative rehabilitation for our patients was to wear Barouk shoes immediately after surgery for unloading the forefoot for 6 weeks ( Fig. 9 ). The patients were bandaged in a compression dressing for 1 month after surgery. As for the development of movements, after chondroplasty of large joints using the AMIC technique, it was recommended to exclude movements in the operated joint within 2 weeks after the operation, and then begin the gradual rehabilitation.17,20 On the other hand, after the cheilectomy, a number of authors, particularly, Seibert and Kadakia, pointed to the need for early aggressive development of movements in the first MTP joint. 10 Based on this, we recommended that our patients begin the gradual development of passive movements in the painless range a week after surgery. Three weeks after the operation, it was recommended to begin the development of active movements. After the transfer to wearing the regular shoes, patients were advised to use the individual insoles. The patients maintained their range of motion exercises for the first year after surgery. We did not have patients undergo physical therapy postoperatively.

Barouk shoe.
The results of surgical treatment were evaluated according to the previously mentioned questionnaires 3, 6, and 12 months after surgery.
Statistical Analysis
The Wilcoxon criterion (
Statistical calculations of the Wilcoxon criterion, as well as reliability by the P criterion, were carried out using the BioStat program. The difference was considered significant when the P criterion was less than 0.05.
Results
The VAS of pain data dynamics is shown in Table 3 (median values). As we can see from this table, a significant decrease in pain was observed by the third month—from 70 to 25 (min 10, max 50; P < 0.024, W = 36.0). Positive dynamics was observed after 6 months—the median VAS of pain was 10 (min 0, max 40; P < 0.024, W = 36.0). By the end of the first year of observation, the median VAS of pain decreased to 5 (min 0, max 30; P < 0.024, W = 36.0). The difference in all cases was statistically significant. Minimum and maximum values before the surgery were 90 and 20, 3 months after the surgery 50 and 10, 6 months after the surgery 0 and 40, and 12 months after the surgery 0 and 30, respectively. Also we can see that in one case the pain level increased by the sixth month (from 10 to 40), but then decreased again (from 40 to 10), and in 2 cases VAS of pain level increased by the 12th month of observation (from 10 to 30 and 20, respectively).
VAS of Pain Dynamics.
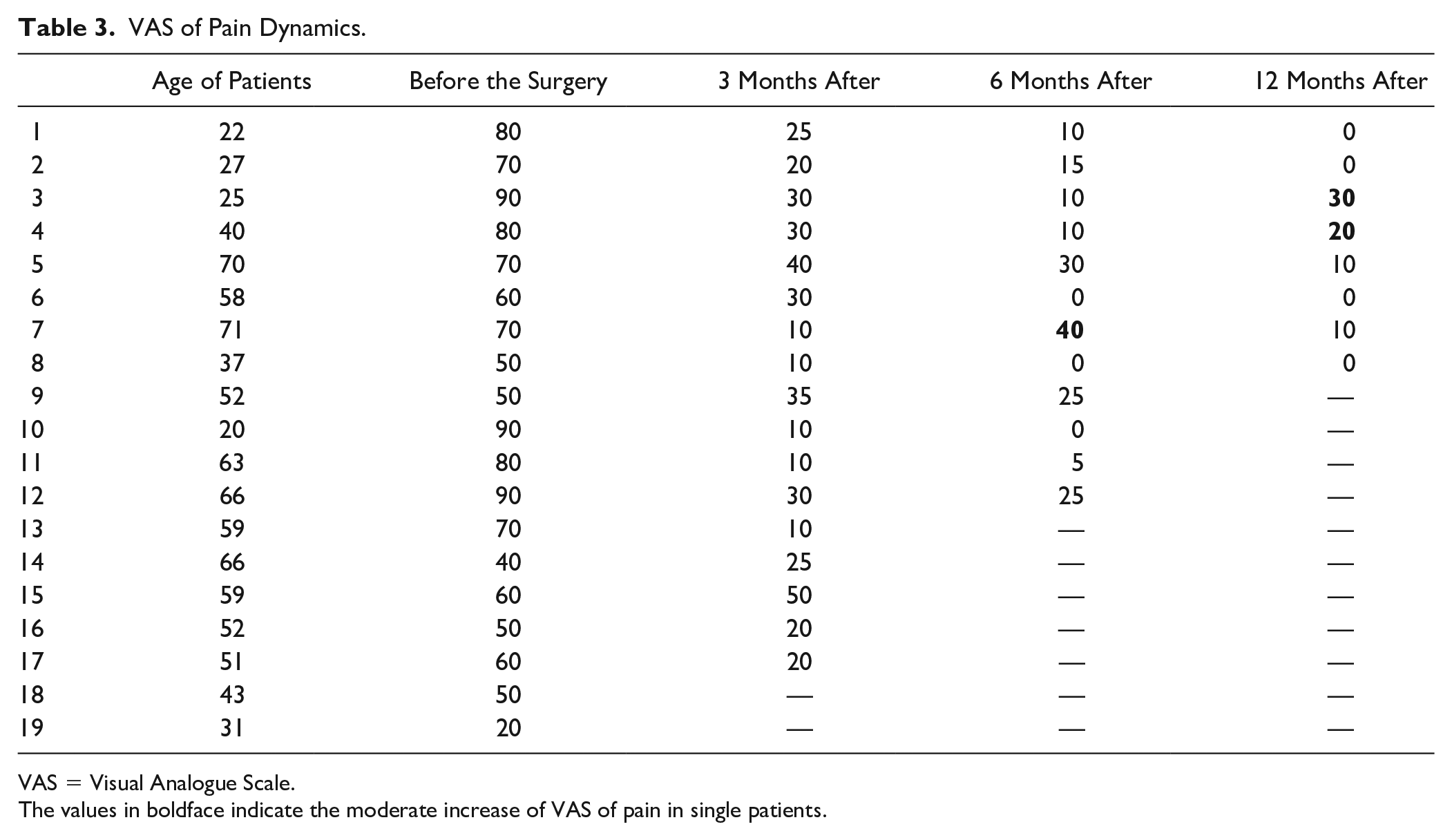
VAS = Visual Analogue Scale.
The values in boldface indicate the moderate increase of VAS of pain in single patients.
Table 4 demonstrates the AOFAS score data dynamics (median values). As we can see, a notable increase in AOFAS score was observed by the third month—from 52 to 77 (min 50, max 85; P < 0.024, W = −36.0). Positive dynamics continued to be observed after 6 months—the median AOFAS score increased to 90 (min 67, max 95; P < 0.024, W = −36.0). By the 12th month of observation, the median AOFAS score increased to 92.5 (min 80, max 95; P < 0.024, W = −36.0). The difference in all cases was statistically significant. Minimum and maximum values before the surgery were 39 and 62, 3 months after the surgery 50 and 85, 6 months after the surgery 67 and 95, and 12 months after the surgery 80 and 95, respectively. Also we can see that in one case the AOFAS score decreased by the sixth month (from 80 to 67), but then increased again (from 67 to 85), and in another case the AOFAS score fractionally decreased by the 12th month of observation (from 85 to 80).
AOFAS Dynamics.
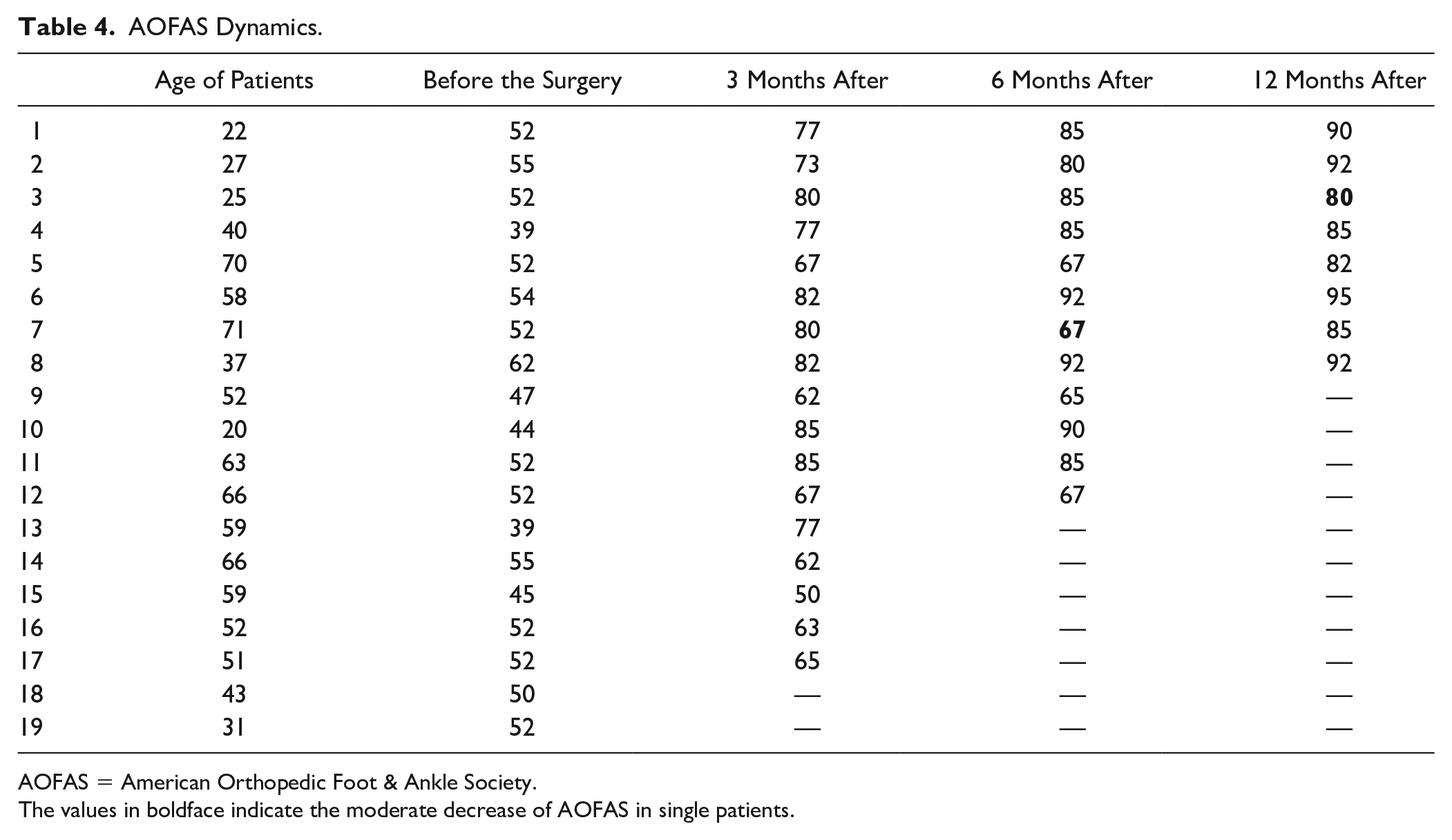
AOFAS = American Orthopedic Foot & Ankle Society.
The values in boldface indicate the moderate decrease of AOFAS in single patients.
The FFI data dynamics is presented in Table 5 (median values). Three months after the performed chondroplasty, the index median decreased from 5.8 to 2.2 (min 0.6, max 6.0; P < 0.024, W = 36.0). Positive dynamics was observed after 6 months—FFI continued decreasing to 1.1 (min 0, max 3.9; P < 0.024, W = 36.0). Twelve months after the surgery FFI stabilized at 1.0 (min 0, max 2.5; P < 0.024, W = 36.0). Also we can see that in one case FFI increased by the sixth month (from 1.2 to 3.9), but then decreased again (from 3.9 to 1.1), and in 2 cases FFI increased by the 12th month of observation (from 1.1 to 2.5 and from 0.7 to 1.2).
FFI Dynamics.
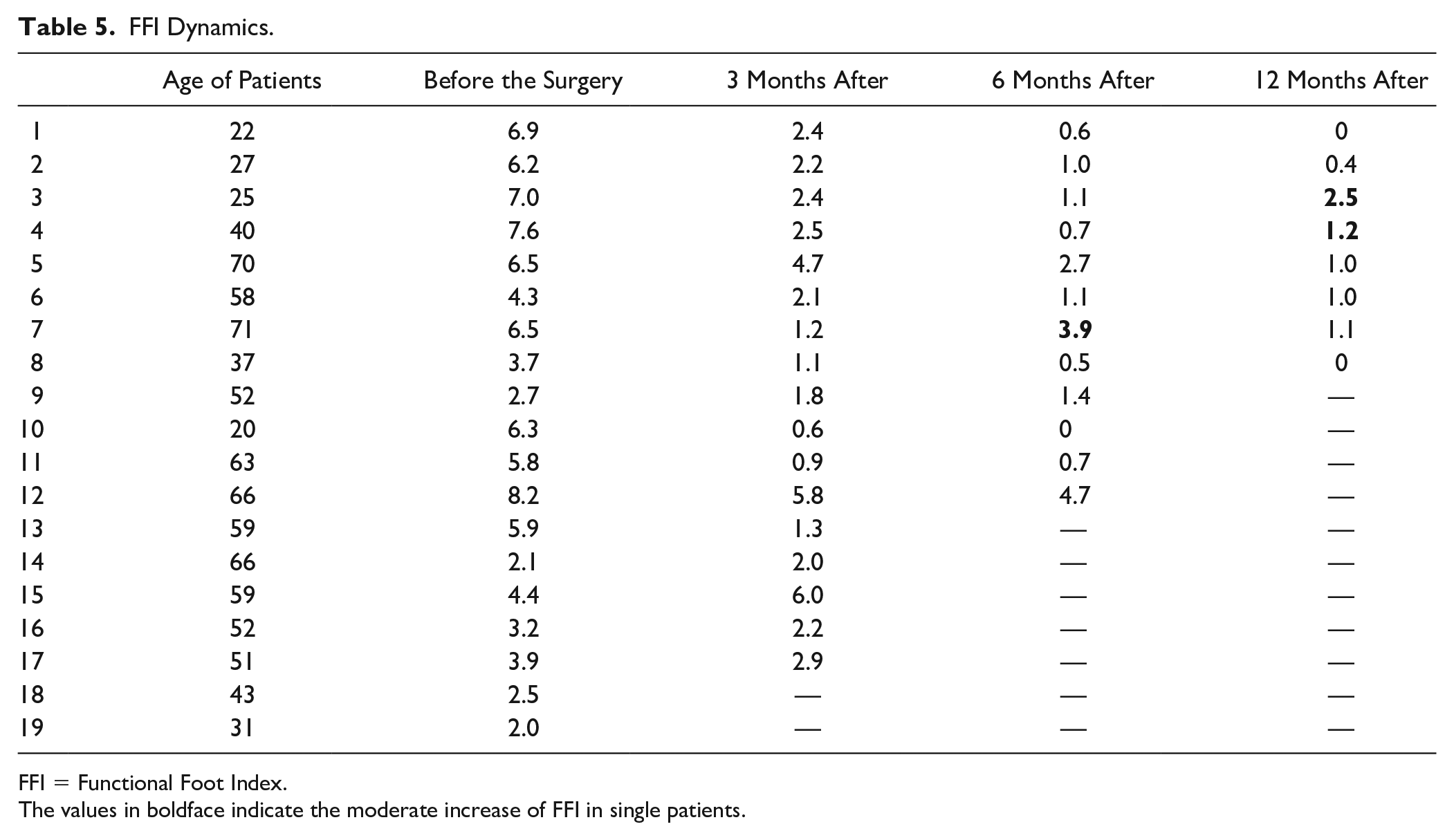
FFI = Functional Foot Index.
The values in boldface indicate the moderate increase of FFI in single patients.
As for the ROM in the first MTP joint ( Table 6 , median values), 3 months after the surgery, its significant increase was also observed—ROM increased from 20° to 60° (min 25°, max 85°, P < 0.024, W = −36.0). Six months after the performed chondroplasty the positive dynamics continued to be observed—ROM was 65° (min 30°, max 80°, P < 0.024, W = −36.0). By the end of a year of observation ROM increased to 71.5° (min 50°, max 90°, P < 0.024, W = −36.0). It also can be seen that in one case ROM decreased by the sixth month (from 65° to 40°), but then the previous level was regained (from 40° to 65°), and in another case ROM fractionally decreased by the 12th month of observation (from 60° to 50°).
ROM Dynamics.
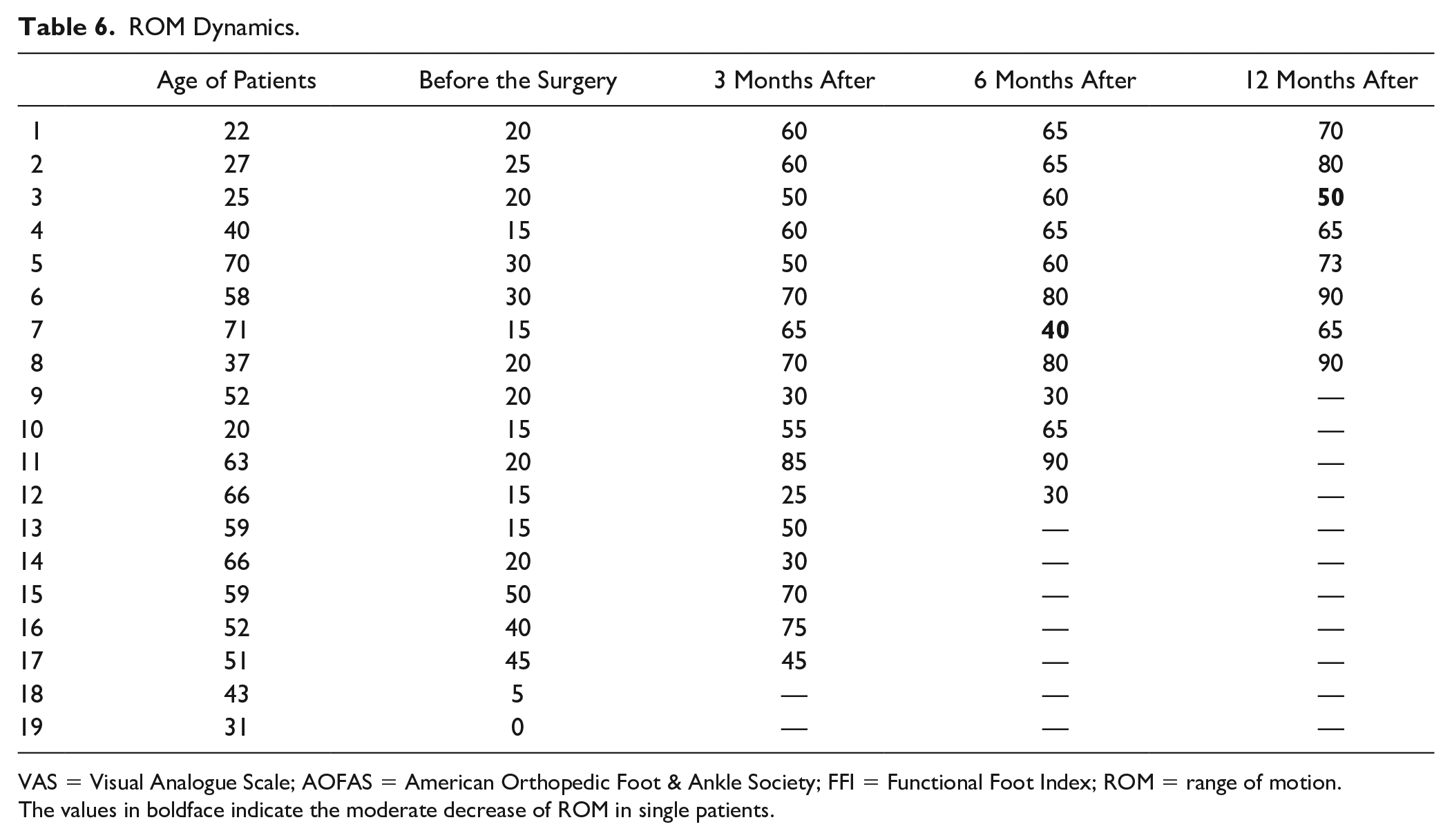
VAS = Visual Analogue Scale; AOFAS = American Orthopedic Foot & Ankle Society; FFI = Functional Foot Index; ROM = range of motion.
The values in boldface indicate the moderate decrease of ROM in single patients.
Radiography of the feet 3 months after the surgery showed a significant increase in the joint space of the first MTP joint. However, during the control examination after 6 and 12 months, the joint space narrowing was observed ( Figs. 10 and 11 ). Nevertheless, clinically this phenomenon did not correlate with the assessment by questionnaires and was not manifested by the decrease in ROM. More than that, patients from the 3rd to the 12th month after the operation, in general, noted an increase in ROM.

X-ray of the foot before the surgery; first day after the surgery.

X-ray of the foot 12 months after the surgery.
The picture of the foot MRI (magnetic resonance imaging) after the surgery is particularly interesting. In the area of the operated head of the first MB, cluster-shaped formations—“artifacts” ( Figs. 12 and 13 )—are determined. Most likely, the collagen matrix, as well as the resulting hyaline-like tissue, looks like this on MRI.
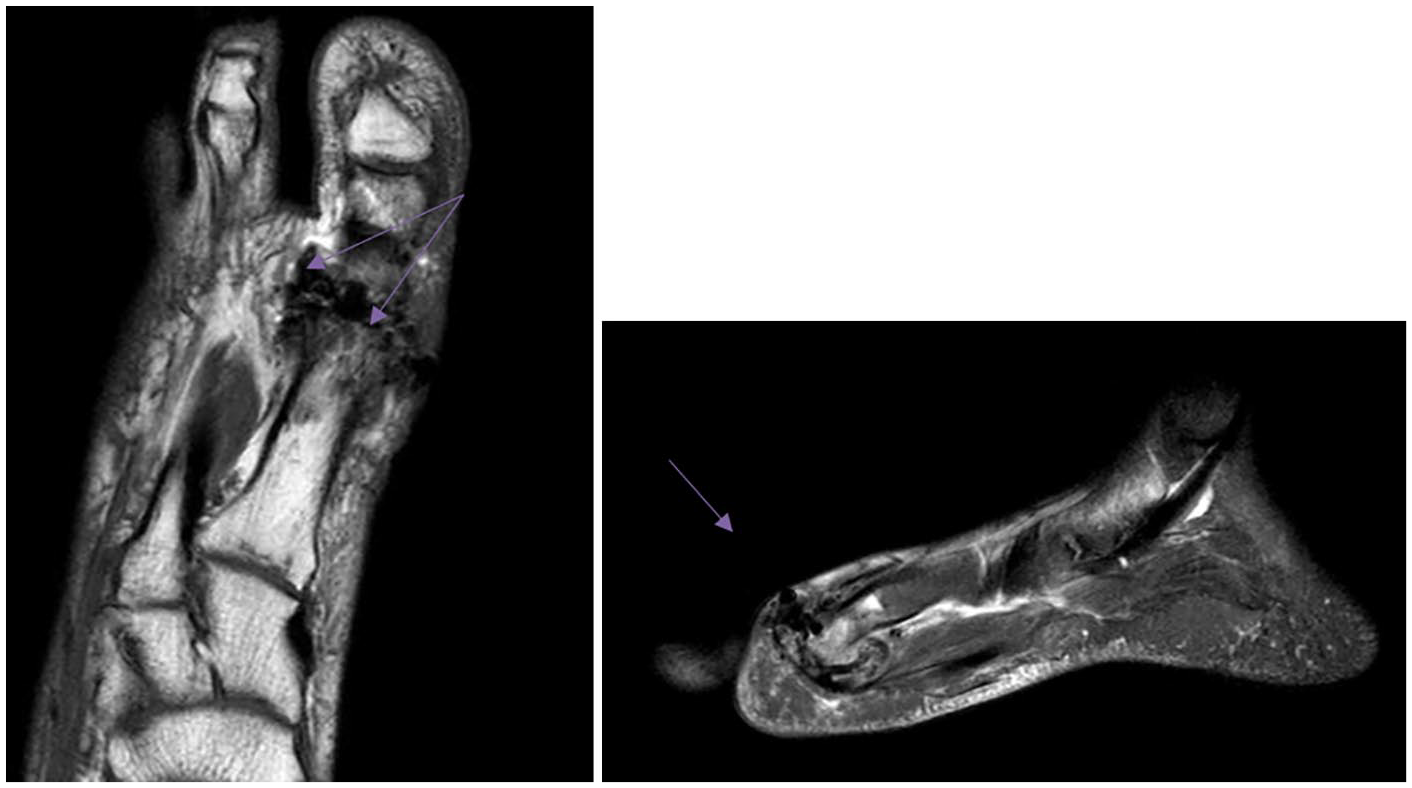
Foot MRI 1.5 months after the surgery (female patient I, 43 years).
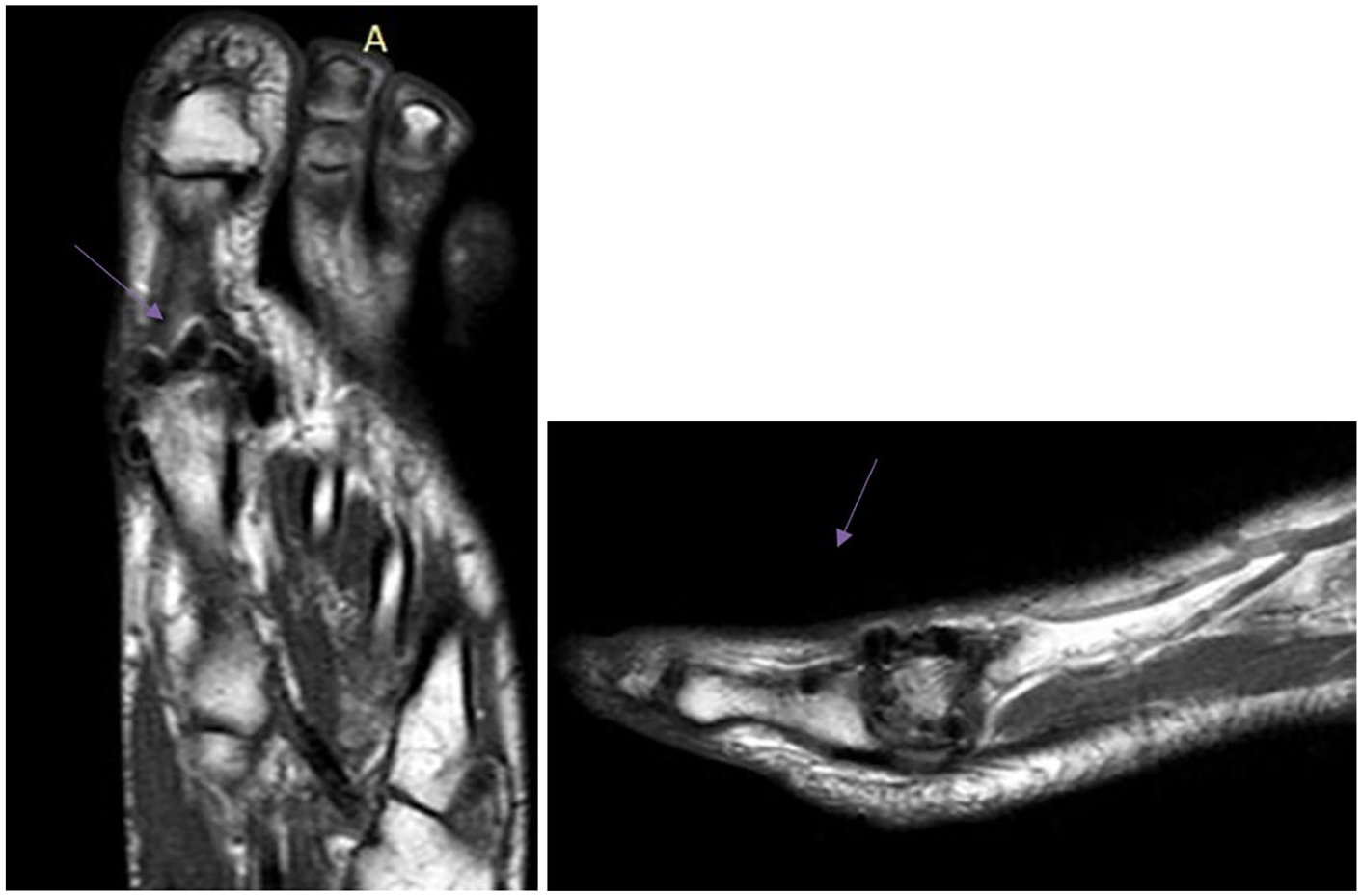
Foot MRI 12 months after the surgery (female patient D, 40 years).
Discussion
The world literature describes only one study conducted in 2016, in which the author proposes a method of surgical treatment of first MTP joint OA, similar to that used in our study—a modified version of AMIC—MAST (matrix-associated stem cell transplantation). 25 Richter and coauthors monitored patients (n = 20) for 2 years after the performed first MTP joint chondroplasty, and they noted a significant improvement in clinical status (including an increase in ROM in the first MTP joint) both in the early postoperative period and after the 2-year observation period: the ROM in the first MTP joint increased from 29.1° to 60°.
Erdil et al. compared the effectiveness of total joint replacement (group A), hemiarthroplasty (group B), and arthrodesis (group C) of the first MTP joint. 5 They monitored patients (n = 38) for 24 to 66 months after surgery. In group A, VAS of pain decreased from 76.7 to 15.8, AOFAS score increased from 45.4 to 92.7, and ROM increased from 15.1° to 40°. In group B, VAS of pain decreased from 78.6 to 13.6, AOFAS score increased from 38.4 to 86.1, and ROM increased from 20.5° to 47.9°. In group C, VAS of pain decreased from 80 to 5, AOFAS score increased from 33.6 to 76.1, but ROM reduced from 13.3° to 0°.
Coughlin and Shurnas et al. analyzed the long-term results after first MTP joint cheilectomy (the mean duration of follow-up was 9.6 years): VAS of pain level decreased from 80 to 15, AOFAS improved from 45 to 90, and ROM increased from 39.2° to 63.7°. 23
In our study, by the 12th month ROM in the first MTP joint increased from 20° to 71.5°; VAS of pain level decreased from 70 to 5, AOFAS score increased from 52 to 92.5. In comparison with abovementioned studies our results seem to be better, but we do not have enough long-term results to confirm it.
We observed positive dynamic in our patients after the performed first MTP joint chondroplasty using the AMIC technique. A particularly significant difference in status before and after the surgery is observed in the early period—after 3 months: the VAS of pain level decreases on average by 45, AOFAS score increases by 25, and FFI by 3.6. And it is important that the difference in parameters was statistically significant (P < 0.024).
A significant improvement in the patients’ condition in the early postoperative period can be associated with the wearing of postoperative Barouk shoes that provide unloading of the forefoot. Although patients use this shoe only for 6 weeks after the surgery and, nevertheless, the positive dynamics also persists 6 months after the operation, there is a further decrease in the VAS of pain level by 15 mm, an increase of the AOFAS score by 13, and FFI by 1.1. The difference in parameters was also statistically significant (P < 0.024).
Subsequently, after 12 months of observation, the condition of the patients, in general, stabilizes to a positive level.
It is notable that one patient showed some deterioration 6 months after the operation: the VAS of pain level increased by 30, FFI by 2.7, AOFAS score decreased by 13, and ROM by 15°. However, by the 12th month the condition had improved again, even compared to the 3rd month after the surgery. Perhaps the possible reason is that the patient began to load the operated foot more by the 6th month, as well as the fact that in older people, regenerative processes are slower. Therefore, by the 12th month, the patient’s condition improved again. As for the slight deterioration in the condition of 2 patients by the 12th month of observation, this is most likely due to the fact that these patients stopped developing motion in first MTP joint 6 months after the surgery.
The phenomenon of the joint space narrowing described above did not correlate with assessment parameters and ROM. The reason is probably that within 3 months after the operation, some swelling in the operated foot persists. Therefore, with a greater joint gap, in that period of observation ROM is less than by the sixth month after the surgery.
It is also notable that the artifacts in the first MTP joint that we found on MRI were not previously described in the literature; therefore, it is impossible to give an accurate interpretation of this phenomenon, but we can assume that these artifacts are essentially the newly formed hyaline-like tissue.
Conclusion
The immediate and medium-term results of the operations showed that the first MTP joint chondroplasty using a collagen matrix can be a fairly effective method of surgical treatment that can relieve pain and significantly improve the quality of life of patients suffering from first MTP joint OA. Within 3 months after the surgery, patients had significant positive dynamics, and within a year the conditioned stabilized at a quite good level. A more complete assessment of the effectiveness of first MTP joint chondroplasty using the AMIC technique will be revealed by longer term follow-up.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of V.A. Nasonova Research Institute of Rheumatology in 2018.
Informed Consent
Written informed consent was obtained from all subjects before the study.