
Abstract
Objective
To evaluate the effect of intra-articular injection of autologous micronized adipose tissue (MAT) with ankle arthroscopic debridement in patients with advanced-stage posttraumatic osteoarthritis (PTOA) of ankle.
Design
A retrospective cohort study investigating patients treated with arthroscopic debridement and autologous MAT injection for ankle PTOA was performed. Patients with Kellgren-Lawrence (KL) grade 3 to 4 were included. Visual analogue scale (VAS), Foot and Ankle Outcome Scores (FAOS), and patient satisfaction were evaluated.
Results
A total of 19 patients (19 ankles) were included (KL grade 3, 8 patients; grade 4, 11 patients). At a mean follow-up time of 14.3 months (range, 7-23 months), the mean FAOS subscales for pain and quality of life significantly increased from 48.8 and 20.1 preoperatively to 61.1 and 30.1 (P = 0.029 and 0.048, respectively). The mean VAS score significantly improved from 6.1 to 3.8 (P = 0.003) at final follow-up. A total of 10.5% (2/19) of patients were very satisfied, 31.6% (6/19) satisfied, 26.3% (5/19) neutral, 21.1% (4/19) unsatisfied, and 10.5% (2/19) very unsatisfied with their outcomes. The overall FAOS score demonstrated a significant difference in pre- to postoperative change with 14.8 for KL grade 3 and 5.9 for KL grade 4 (P = 0.048).
Conclusions
Autologous MAT injection is a safe and potentially beneficial procedure for advanced-stage ankle PTOA as an adjunct to arthroscopic debridement, although more than one-third of patients were unsatisfied with the procedure. This procedure may be more beneficial for KL grade 3 patients than grade 4 patients. However, future investigations are necessary to define the role of MAT for ankle PTOA.
Keywords
Introduction
Osteoarthritis is one of the leading musculoskeletal disorders in the adult population. Unlike knee and hip joints, up to 90% of osteoarthritis in the ankle joint is posttraumatic in nature. 1 The ankle is the most commonly injured joint during sports activities. 2 Consequently, individuals with a history of ankle sprain comprise 70% to 85% of patients who undergo surgery for end-stage ankle posttraumatic osteoarthritis (PTOA). 3 Patients with ankle PTOA are therefore an average of 14 years younger at the time of diagnosis and progress more rapidly to end-stage disease than patients with hip or knee arthritis. 1 Many nonsurgical treatment paradigms are available for the treatment of PTOA; however, most are temporizing and none have proven to prevent the relentless progression of the disease. 4
Orthobiologic treatments have recently been added as therapeutic modalities to combat osteoarthritis. Among these, adipose-derived stem cells (ADSCs) have attracted attention as a promising treatment due to the propensity for these cells to differentiate into chondrocytes and therefore potentially provide chondrogenic capability as well as a chondroprotective role to arthritic joints. 5 Regulatory constraints, however, hinder the use of ADSCs in the United States. Micronized adipose tissue (MAT) injection was introduced as an innovative isolation method for autologous ADSCs, reducing costs and avoiding the regulatory issues with expanding ADSCs in a laboratory setting. 6 Administration of MAT has been shown to be safe and effective in the treatment of knee osteoarthriti 6 ; however, there exists a paucity of studies reporting the effects of MAT injection for the treatment of ankle osteoarthritis.
The purpose of this study was to evaluate the effect of intra-articular injection of autologous MAT with arthroscopic debridement in patients with advanced-stage ankle PTOA. Our hypothesis was that autologous MAT injection as an adjunct to arthroscopic debridement would reduce the pain and improve the quality of life for patients with ankle PTOA.
Materials and Methods
Patients
This is a retrospective comparative study using chart review for the retrieval of data on individual patients. All patients treated with intra-articular injection of autologous MAT with arthroscopic debridement for ankle PTOA between 2017 and 2019 by the senior author were identified. The inclusion criteria of the current study were the following: age between 18 and 80 years at the time of surgery, Kellgren-Lawrence (KL) grade 3 to 4, and a minimum 6 months of postoperative follow-up visits. Patients were excluded if they had a previous infection of the ankle joint or a history of rheumatoid arthritis, or profound mechanical malalignment of the ankle joint.
Surgical Technique
All arthroscopic procedures were performed using a standardized technique by the senior surgeon. Standard anteromedial and anterolateral portals were created with noninvasive distraction for arthroscopy. Bony and soft tissue debridement was performed to address anterior impingement in all patients to obtain adequate dorsiflexion. Any observed scar, inflamed synovium, unstable cartilage, loose bodies, and cicatrization in the ankle joint were removed.
An 11-blade scalpel was used to make a skin incision in the right flank area. Before harvesting the fat, the site was injected with tumescent solution (25 mL of 2% lidocaine and 0.5 mL epinephrine [1:1000] in 250 mL of normal saline) by using a disposable 17-gauge blunt cannula connected to a Luer-lock 60-mL syringe. Gentle agitation of the tissue was completed followed by a 15-minute resting period to allow for adequate emulsification. The adipose tissue was then harvested using the liposuction 13-gauge blunt cannula connected to a Vaclock 20-mL syringe. Liposuction of the abdominal tissue was performed using brisk broad strokes until a total of 80 to 120 mL of aspirate was obtained. The adipose tissue from each of Vaclock syringes was transferred to a single 60-mL syringe using a Luer-lock connector. The harvested fat was immediately processed in the Lipogems processing kit (Lipogems International, Milan, Italy) as described in the manufacturer’s technique guide. Lipogems processing reduces the size of the adipose tissue clusters with a mild mechanical action while eliminating oily substances and blood residues. The resulting MAT was then transferred into several 10-mL syringes to be injected in the patient. After the excess fluid was removed, 5 mL of MAT was obtained and was injected into the ankle after the arthroscopic procedure. Although 10 to 15 mL of MAT was injected into the knee in several studies 6 , the ankle joint has less space than the knee joint and therefore we injected 5 mL of MAT into the ankle joint, which was tolerated by patients without pain from capsular distension.
An abdominal binder was applied for 1 week following surgery to minimize swelling and ecchymosis in all patients. A compression bandage was applied after the procedure and the patient was asked to be nonweightbearing for 1 week. Ankle pumps were allowed the day after surgery for 20 minutes daily. After 1 week, the patient was allowed to begin weightbearing as tolerated with no activity restrictions. Physical therapy was commenced after 1 week following the procedure. Therapy concentrated on strengthening, balance, and proprioception exercises and was encouraged to be twice weekly for 2 months.
Data Collection
Data were collected on patient age, gender, follow-up time, and concomitant procedures. Clinical outcomes were evaluated using the Foot and Ankle Outcome Scores (FAOS). Visual analogue scale (VAS) score was also evaluated preoperatively, at 6 months and at the final follow-up visit. Patients were surveyed via email on a 5-point Likert-type scale regarding satisfaction with their ankle following procedure; 5 = very satisfied, 4 = satisfied, 3 = neutral, 2 = unsatisfied, and 1 = very unsatisfied. As we did not obtain postoperative magnetic resonance imaging (MRI) routinely, the effects of MAT injection on change detectable by MRI were not investigated.
Statistical Analysis
Descriptive statistics were completed consisting of mean and standard deviation for continuous variables and frequency and percentage for categorical variables. Wilcoxon signed-rank test was performed to compare preoperative and postoperative outcome scores. Mann-Whitney U test was performed to compare pre- to postoperative changes in outcomes scores between patients with KL grades 3 and 4 PTOA. A value of P < 0.05 was considered statistically significant. All statistical analysis was performed with SPSS version 22 (IBM Corp. Release 2013. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp, Armonk, NY).
Results
A total of 19 patients (19 ankles) who underwent arthroscopic debridement and autologous MAT injection for ankle arthritis with KL grade 3 to 4 were included in the analysis (KL grade 3, 8 patients; grade 4, 11 patients). Of those, 2 patients underwent concomitant injection of flowable calcium phosphate into large subchondral cysts in the tibial plafond. An additional patient required a concurrent lateral ankle ligament stabilization procedure. The mean age was 49.2 ± 15.0 years (range, 18-73 years). Patients were followed up for a mean of 14.3 ± 6.3 months (range, 7-23 months).
The mean FAOS subscale scores of pain and quality of life significantly improved from 48.8 ± 13.0 and 20.1 ± 9.9 preoperatively to 61.1 ± 15.5 and 30.1 ± 15.5 postoperatively (P = 0.029 and 0.048, respectively). The mean FAOS subscale scores of symptoms and daily activities improved from 43.9 ± 14.0 and 61.2 ± 13.6 preoperatively to 53.9 ± 17.6 and 70.1 ± 13.5 postoperatively, but this change was not statistically significant (P = 0.103 and 0.091, respectively). The overall FAOS scores significantly improved from 43.6 ± 9.8 to 53.8 ± 13.5 postoperatively (P = 0.026) ( Table 1 ).
Preoperative and Postoperative FAOS Scores.
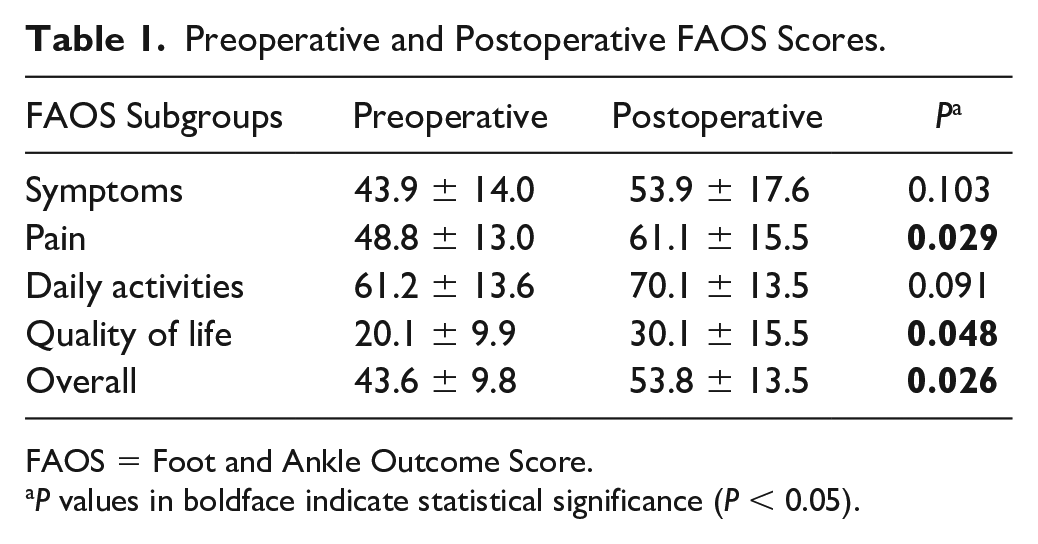
FAOS = Foot and Ankle Outcome Score.
P values in boldface indicate statistical significance (P < 0.05).
The mean VAS score significantly improved from 6.1 ± 1.4 to 3.8 ± 2.5 (P = 0.003) at final follow-up. Of the 14 patients who had a greater than 1 year of follow-up time, 11 patients reported VAS scores at 2 time points, including 6 months and final follow-up (mean of 16.1 months). Of these 11 patients, the mean VAS scores significantly decreased from 6.6 ± 1.5 preoperatively to 3.9 ± 1.9 at 6 months (P = 0.003), and then increased to 4.7 ± 2.7 at final follow-up, which was not statistically significant (P = 0.448) ( Fig. 1 ). On a 5-point Likert-type scale, the mean satisfaction rating was 3.4 ± 1.1 at 6 months and then decreased to 2.9 ± 1.3 at final follow-up, which was not statistically significant (P = 0.390).
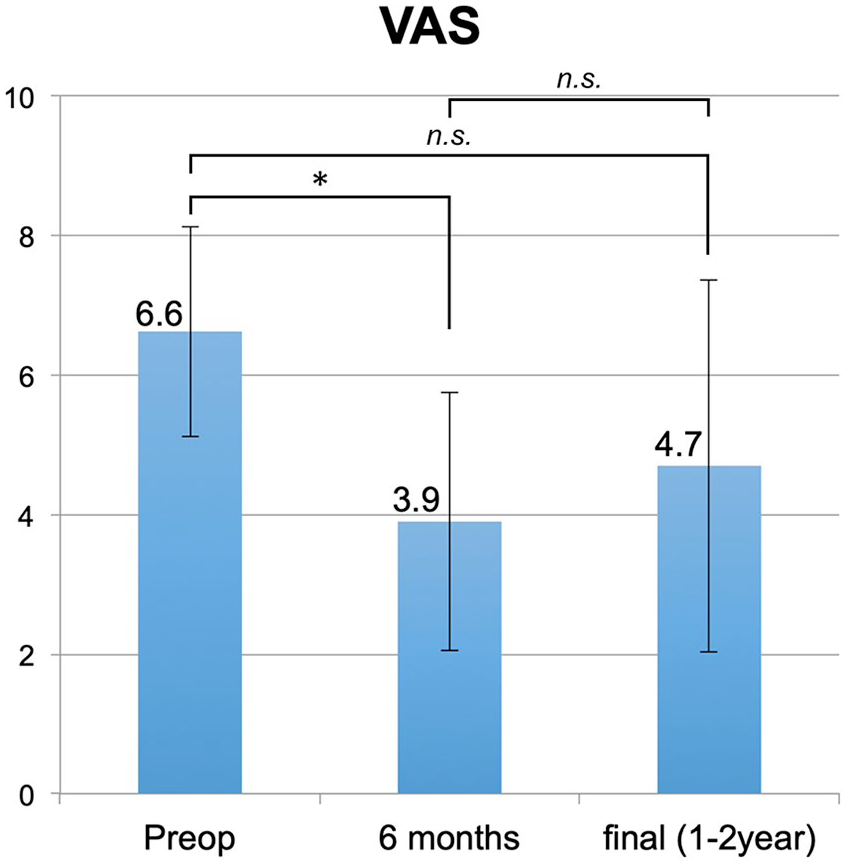
Trend of visual analogue scale (VAS) scores preoperatively, at 6 months, and at final follow-up (*P = 0.003; n.s., not significant).
On a 5-point Likert-type scale in 19 patients, the mean satisfaction rating was 3.1 ± 1.2 (range, 1-5) at final follow-up. Two patients (10.5%) were very satisfied, 6 patients (31.6%) satisfied, 5 patients (26.3%) neutral, 4 patients (21.1%) unsatisfied, and 2 patients (10.5%) were very unsatisfied with their outcomes. There were no complications related to procedure. Three patients did not have any improvements postprocedure (KL grade 3, 1 patient; grade 4, 2 patients), all of whom were “unsatisfied” with the procedure. One patient who had KL grade 4 arthritis required total ankle replacement at 10 months following the procedure. A second patient who also had KL grade 4 arthritis was considering undergoing total ankle replacement due to persistent ankle pain, although this patient was “neutral” on the procedure.
Comparison of Outcomes Based on Kellgren-Lawrence Grade
Both KL grade 3 and 4 groups had significant improvement in VAS scores with mean scores improving from 5.0 ± 0.6 to 2.5 ± 1.4 for the grade 3 group (P = 0.008), and from 6.6 ± 1.4 to 4.5 ± 2.5 for the grade 4 group (P = 0.033) ( Table 2 ). The mean FAOS subscales scores improved in all subscales in both KL grade 3 and 4 groups, but only the subscales for pain and quality of life in KL grade 3 were statistically significant (P = 0.047 and P = 0.019). The overall FAOS scores in KL grade 3 significantly improved from 50.0 ± 5.5 preoperatively to 64.3 ± 5.3 at final follow-up (P = 0.004); however, there was no significant improvement in the overall FAOS scores in KL grade 4, with 40.3 ± 8.9 preoperatively and 47.5 ± 12.2 at final follow-up (P = 0.180).
Comparison of Pre- and Postoperative Overall Functional Outcome Scores between KL Grade 3 and 4 Patients.
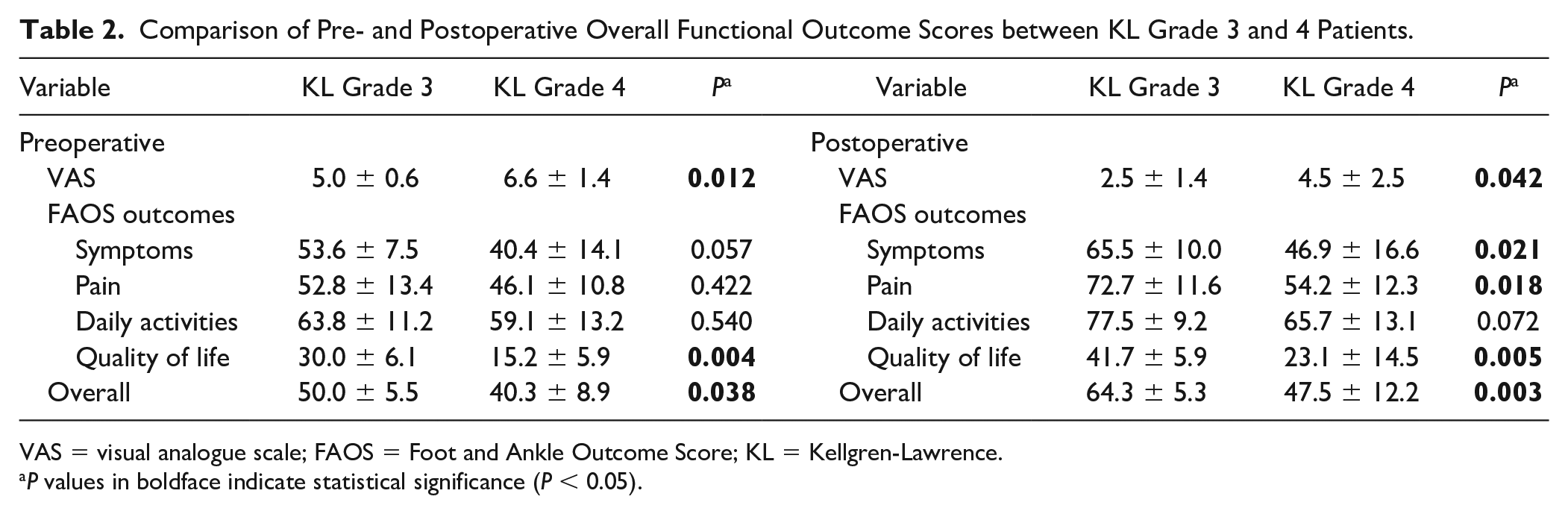
VAS = visual analogue scale; FAOS = Foot and Ankle Outcome Score; KL = Kellgren-Lawrence.
P values in boldface indicate statistical significance (P < 0.05).
The outcomes scores between KL grade 3 and 4 groups were compared next ( Table 2 ). The mean postoperative VAS scores, FAOS subscales for symptoms, pain and quality of life, and overall FAOS score in KL grade 3 group were significantly better than those in KL grade 4 group at final follow-up. However, significant differences between groups were already observed in preoperative VAS scores, FOAS subscale for quality of life, and overall FAOS score. Therefore, the pre- to postoperative change in scores were compared between groups ( Table 3 ). There were no statistically significant differences between groups in the change in FAOS subscales and VAS scores pre- to postoperatively, although KL grade 3 patients had a higher observed change in all scores. Only the overall FAOS score demonstrated a significant difference in pre- to postoperative change between groups, with 14.8 ± 6.2 in KL grade 3 group and 5.9 ± 6.4 in KL grade 4 group (P = 0.048).
Comparison of Pre- to Postoperative Change in Outcome Scores Between KL Grade 3 and 4 Patients.
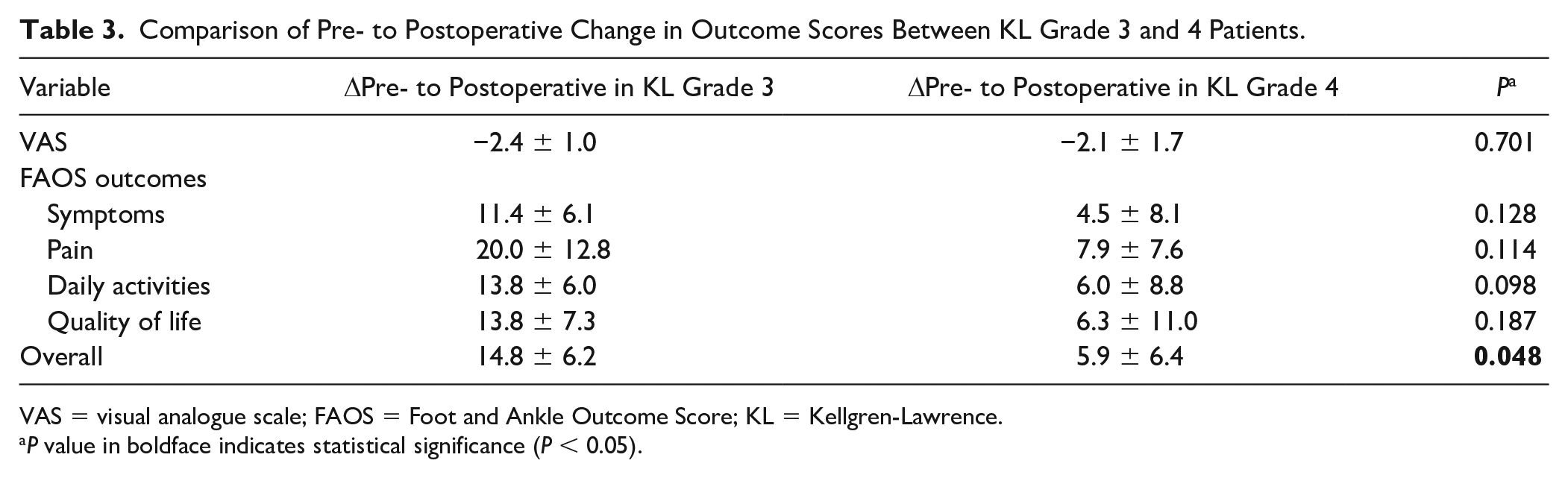
VAS = visual analogue scale; FAOS = Foot and Ankle Outcome Score; KL = Kellgren-Lawrence.
P value in boldface indicates statistical significance (P < 0.05).
Discussion
ADSCs have demonstrated early promise in managing the pain associated with OA. 5 However, because both culture-expanded ADSCs and enzymatic derived stromal vascular fraction have faced difficult-to-navigate regulatory policies in the United States, MAT therapy was developed as an alternative method for utilizing autologous adipose stem cells to treat an osteoarthritic joint. Although several studies have evaluated MAT injection for the management of knee OA, 5 limited data exist describing the effect of MAT on ankle PTOA.
The current study is one of the first to evaluate the use of MAT for the management of ankle PTOA. Although our patients reported a statistically significant improvement in FAOS subscales of pain and quality of life, no significant change was noted for the other subscales of daily activities and symptoms. One explanation for this difference may be that although MAT can improve patients’ pain, the improvement is not enough to allow them to return to their daily activities. An interesting aspect of this study was that MAT injection was capable of improving the VAS at 6 months, however this then increased at a final follow-up visit. Initial symptomatic improvement with gradual worsening over a longer timeframe may suggest that MAT therapy provides a significant, but gradually diminishing benefit for improving the pain associated with ankle osteoarthritis. Alternatively, the large standard deviation may reflect that some patients have long-term pain improvement from MAT whereas others’ relief is short-lived. Additional work is necessary to better define the longevity of any benefit from MAT injection for PTOA.
When comparing the outcome scores between KL grade 3 and 4 patients, no significant differences between groups were found in pre- to postoperative change in VAS score and all FAOS subscale scores, although KL grade 3 patients had a higher change in all scores. Only for the overall FAOS score did KL grade 3 patients have a significantly better change pre- to postoperatively, which may suggest that MAT injection may be more beneficial for KL grade 3 than grade 4 in the treatment of ankle PTOA. Patient selection may be critical for MAT injection in the treatment of ankle PTOA; however, future studies with larger cohorts would be necessary to confirm this finding.
ADSC therapy likely reduces pain through regulation of the inflammatory response. Ragni et al. 7 cultured adipose-derived mesenchymal stem cells in media mimicking osteoarthritic synovial fluid and evaluated secreted cytokines, chemokines, and growth factors. 7 The authors found that the levels of factors involved in regulating extracellular matrix remodeling and inhibition of matrix metalloproteinases were elevated in the media, suggesting that these cells may function in a protective role for cartilage. Zhou et al. 8 injected human adipose-derived mesenchymal stem cells into mice prophylactically and therapeutically for collagen-induced OA and evaluated inflammatory mediators. The authors found that levels of pro-inflammatory cytokines were decreased in both scenarios and levels of the anti-inflammatory cytokine IL-10 were increased after adipose-derived mesenchymal stem cell injection. This works supports adipose-derived mesenchymal stems cells as a modulator of the inflammatory response. One possible mechanism by which MAT and enzymatic derived stromal vascular fraction exert an anti-inflammatory effect is through pericytes. Pericytes are structural cells in the external wall of adipose tissue microvessels and capillaries. When exposed to inflammatory cytokines, these cells detach from capillaries and convert into active mesenchymal stem cells which, in turn, modulate the inflammatory response. 9 Mashiko et al. 10 found that MAT included a significantly higher percentage of pericytes than enzymatically generated stromal vascular fraction. Our patients’ improved pain after MAT injection may be in part due to a decrease in inflammation mediated through pericyte activation in the fat tissue.
Multiple studies have demonstrated positive results when using MAT for the treatment of knee OA. Russo et al. reported a 3-year follow-up on 30 patients with knee OA who were treated with MAT as an adjuvant to anterior cruciate ligament/lateral collateral ligament reconstruction, high tibial osteotomy, meniscectomy, or arthroscopy alone. 11 Of the 22 patients who did not undergo an additional treatment, the clinical improvements achieved at the 12-month follow-up visit were all maintained at the 36-month follow-up visit. Cattaneo et al. 12 conducted a retrospective study where 38 patients with ICRS (International Cartilage Repair SOciety) grade >2 knee OA underwent an arthroscopic procedure with injection of MAT. At 12 months, 92% of patients clinically improved and all of them were satisfied with the treatment. These early results demonstrated that MAT may be useful in the conservative management of knee OA.
Patients in our study had less satisfaction with the MAT injection for ankle PTOA compared to previous work evaluating the therapy for management of knee OA. On a 5-point Likert-type scale, we observed an overall “neutral” level of satisfaction with 32% of patients reporting feeling “unsatisfied” with the procedure. Knee OA and ankle PTOA may respond differently to MAT injection for several reasons. First, the contact surface area of an ankle joint is approximately one-third that of the knee joint. 13 The ankle joint derives its stability from increased bony congruity compared with the knee joint, which is more reliant on supporting soft tissues. This anatomical difference results in higher compressive loading forces in the ankle joint. Additionally, the articular cartilage in the ankle is approximately half the thickness of knee cartilage, and the extracellular matrix of ankle cartilage is denser with a higher dynamic stiffness.14,15 Second, although PTOA is the predominant form of OA in the ankle, knee OA is largely idiopathic. Previous work has demonstrated that synovial inflammation levels are markedly higher in PTOA than the levels observed in idiopathic OA. 16 Several studies also found that mechanical impact injury to cartilage leads to increased levels of matrix metalloproteinase (MMP)-1, MMP-3, MMP-8, MMP-9, MMP-13, and ADAM-TS5, although MMP-8 expression is undetectable in normal ankle cartilage.17 -19 Another study revealed that intra-articular MMP-3 levels remain elevated for years after a traumatic injury. 20 These findings suggest that PTOA may have an increased inflammatory milieu compared with idiopathic OA. In addition, PTOA is associated with decreased joint fluid viscosity, increased production of reactive oxidant species, and reduced antioxidant defenses when compared with idiopathic OA. 21 Additional work aimed at further understanding the pathophysiology of PTOA is necessary to explain the observed outcomes differences after injection of MAT for knee OA and ankle PTOA.
This retrospective study had several limitations that must be considered in lieu of the reported benefits from MAT injection for ankle PTOA. One is the small cohort size. Our patients had a varied response to the treatment, as reflected by the standard deviations, and increasing the cohort size would likely assist with revealing the true effect of MAT injection as an adjuvant to ankle arthroscopy and debridement. A second limitation is the short follow-up. We began to observe a decrease in the initially observed pain improvement by 1 to 2 years, which may represent the start of a diminishing benefit from the treatment. It is unclear whether these patients’ pain symptoms would continue to worsen to preinjection levels or remain at this improved, but less than maximal, level. Third, our work lacks a control group which prevents us from making any definitive conclusion about the effects from MAT injection. Finally, our MAT injections were included with an ankle arthroscopy and debridement and any observed benefit is unable to be attributable solely to the MAT injection. A prospective head-to-head comparative trial with a larger cohort and follow-up period would help clarify the role of MAT in managing ankle PTOA.
Conclusion
The current study demonstrates that autologous MAT injection is a safe and potentially beneficial procedure for ankle PTOA as an adjunct to arthroscopic debridement to reduce pain. However, more than one-third of patients were unsatisfied with the procedure. This procedure may be more beneficial for KL grade 3 patients than grade 4 patients. Further studies investigating longer-term effects and prognostic factors for outcomes in a larger cohort are warranted given the results of this preliminary study.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John G. Kennedy is a consultant for Arteriocyte, Inc.; received research support from the Ohnell Family Foundation, Mr. and Mrs. Michael J. Levitt.
Ethical Approval
The ethical committee at our institution reviewed and approved of the study.
Informed Consent
Not applicable.
Trial Registration
Not applicable.