
Abstract
Objective
Arthroscopic partial meniscectomy (APM) is one of the most commonly performed surgical procedures. However, the indications for APM are controversial and obese patients may have worse outcomes. This study’s primary purpose was to investigate differences in outcome after APM associated with elevated body mass index (BMI). Secondary objectives included differences in pathophysiology, surgical complications/failures, or osteoarthritis development.
Design
MEDLINE, EMBASE, and OVID databases were systematically searched for eligible studies reporting on APM outcomes at a minimum of 1 year postoperatively. Studies that did not include BMI categorization were excluded. Meta-analysis was conducted with random-effects modeling where data from at least 2 studies was available.
Results
A total of 16 articles were included. Overweight/obese BMI was associated with worse preoperative Lysholm (mean difference, −6.06 [95% CI, −11.70 to −0.42]) and visual analogue scale pain scores (0.43 [0.07 to 0.79]). Worse postoperative normalized knee-specific patient-reported outcome scores were also associated with obese BMI (−4.57 [−5.33 to −3.81]). There were no significant differences in clinical improvement or osteoarthritis progression among BMI groups. Two studies found higher complication/failure rates, 3 articles associated medial meniscus posterior root tears, and 1 article found differences in gene transcript expression with increased BMI.
Conclusions
Obesity is associated with worse knee function after APM, and patients with elevated BMI have worse preoperative knee pain and function. However, there is no difference in amount of improvement between elevated and normal BMI patients. Further prospective research is necessary to determine the comparative effectiveness of APM in patients with elevated BMI.
Introduction
In a 10-year span from 1996 to 2006, the number of arthroscopic knee procedures increased by 49%, and over half were performed for meniscal tears in just 1 year. 1 Arthroscopy for meniscal tears was also the single most commonly-reported procedure to the American Board of Orthopaedic Surgery from 1999 to 2003. 2 The specific surgical treatment of meniscal tears varies depending on multiple clinical and patient factors but when meniscal tears are symptomatic and irreparable, arthroscopic partial meniscectomy (APM) is currently the gold standard. 3 However, obesity may affect surgical outcome and there is no consensus in the current literature on how body mass index (BMI) should factor into the clinical decision-making process for treatment of meniscal tears.
Almost 40% of the US population was obese in 2016, and this number is projected to continue increasing.4-6 Patients with elevated BMI are thought to experience higher load through the knee joint, altered alignment and gait, and often have higher levels of pro-inflammatory cytokines associated with increased adipose tissue.7,8 These characteristics may affect the pathoanatomy and/or pathophysiology of meniscal tears, and could contribute to the development or progression of knee osteoarthritis (OA). Meniscal tears and APM are independently associated with knee OA in previous literature, and obesity may further increase the risk of OA.9-12 Additionally, increased BMI is associated with increased risk of postoperative complications such as venous thromboembolism or surgical site infections.13,14 Therefore, it is critical for orthopedic surgeons to understand how obesity may play a role in treatment of meniscal tears with APM.
The purpose of this study is to investigate any differences in surgical outcomes associated with overweight and/or obese BMI after APM. Secondary goals of this study include assessing differences in postoperative complications or failures and in pathophysiology of meniscal tears among BMI classification groups.
Methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and was registered with PROSPERO.15,16 Studies that reported mechanism of injury, pathoanatomy/pathophysiology, outcomes, and complications of partial meniscectomy in the overweight and obese patient population were eligible. Two authors (T.Z. and J.J.J) independently and systematically searched the MEDLINE, EMBASE, and OVID electronic libraries up to July 2019 for any articles that met the eligibility criteria by using the following Boolean string: menis*[ti] AND (obese OR overweight OR BMI OR “body mass index”). All articles were checked for references to identify any other articles that could potentially meet eligibility criteria.
Articles were then screened based on the following inclusion criteria: (1) primary partial meniscectomy; (2) skeletally mature; (3) containing comparison groups based on BMI category/classification; (4) minimum follow-up of 1-year postoperatively; (5) original article; (6) published in English; and (7) human study population. The exclusion criteria were the following: (1) bilateral or revision partial meniscectomy; (2) previous or concomitant meniscus repair or meniscus transplantation; (3) previous or concomitant ligamentous reconstruction; (4) lack of stratification by BMI; (5) studies that excluded any groups that would be considered overweight or obese by BMI; and (6) any publication that was a case report, review, abstract, or technical notes. The quality of the included studies was assessed based on the Methodological Index for Non-Randomized Studies (MINORS) criteria and any study with a MINORS score less than 16 was excluded. 17 In order to guarantee full inclusion of the adequate studies this process was independently performed by both authors, if any discrepancies appeared, these were resolved by the senior author (R.F.H.).
The initial search returned 239 total articles, and 45 additional records were identified via cross-referencing relevant articles, for a total of 284 articles. Articles were excluded due to the listed exclusion criteria either during initial screening of abstracts or evaluation of full-text articles as seen in Figure 1 . There was a total of 16 studies that met all the criteria and were included in this study ( Table 1 ). Four of those articles used the same or overlapping patient cohorts but each produced different analyses such as tibiofemoral versus patellofemoral or radiographic versus symptomatic OA.18-21
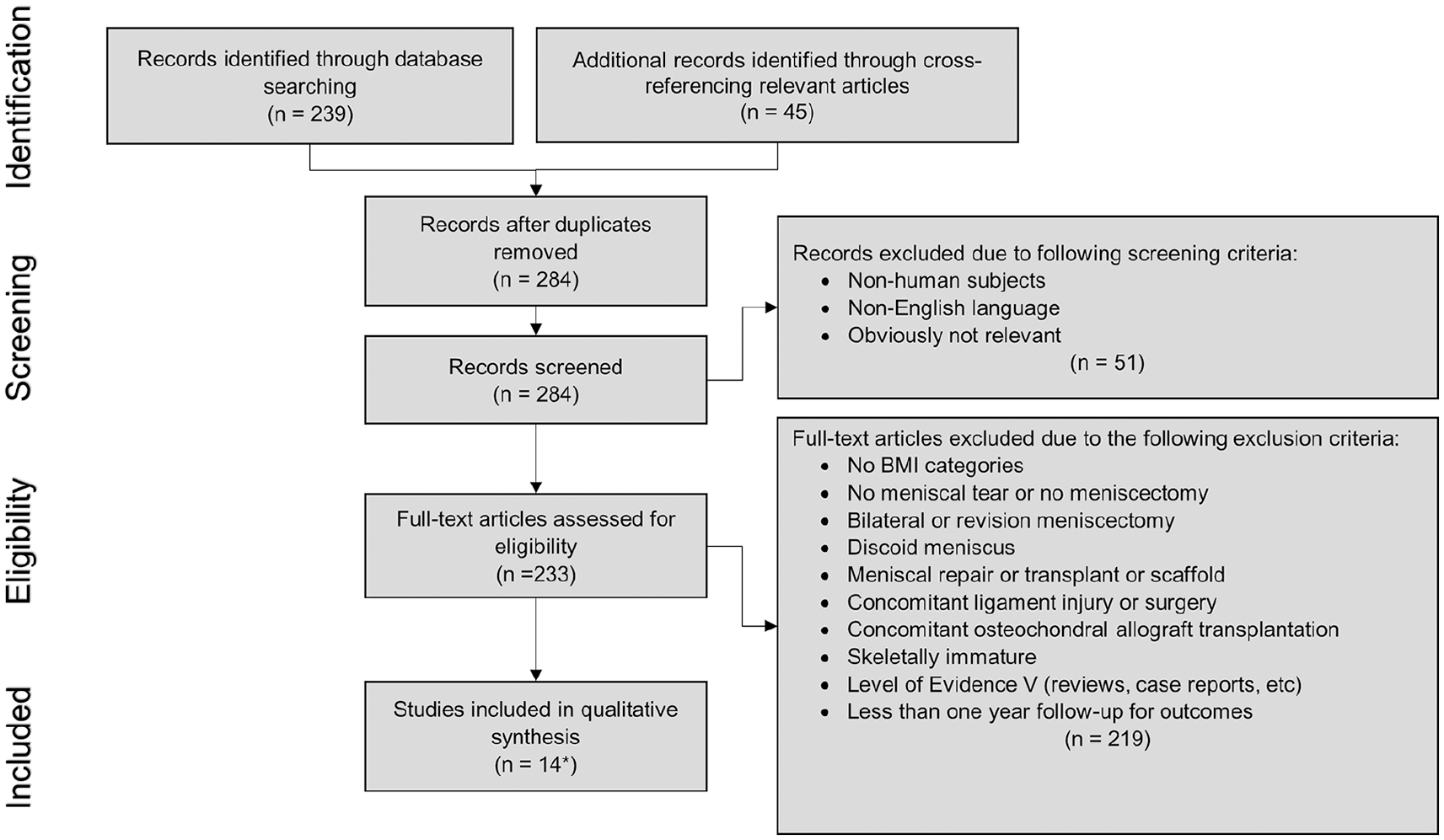
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of systematic literature search.
Detail of Included Articles.
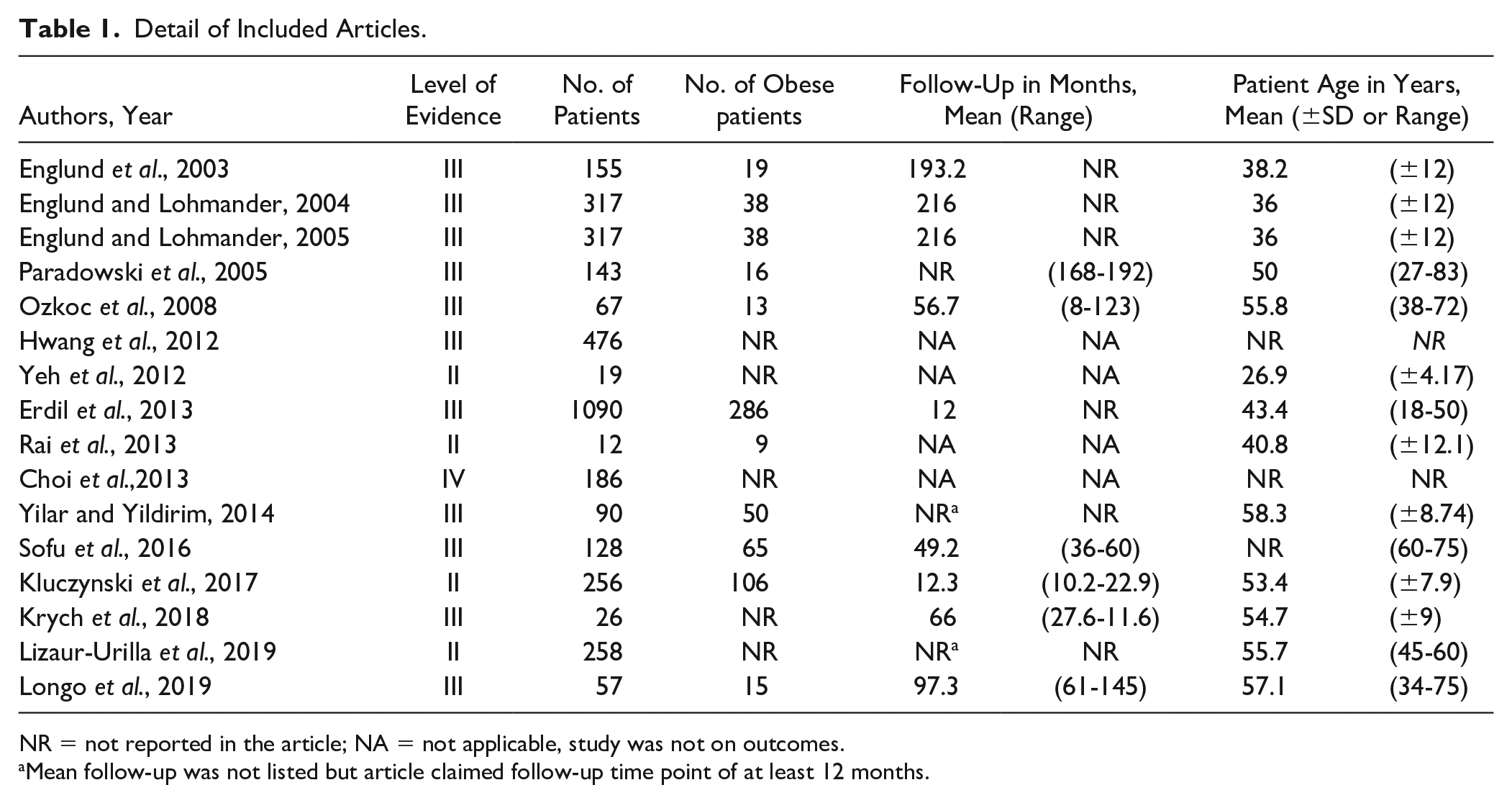
NR = not reported in the article; NA = not applicable, study was not on outcomes.
Mean follow-up was not listed but article claimed follow-up time point of at least 12 months.
The specific data that were extracted from the included articles when available included: study design, level of evidence, sample size, patient age and demographic characteristics, BMI classification, length of follow-up, mechanism of injury, postoperative outcome measures and results, and complication or failure rates. Again, the 2 authors (T.Z. and J.J.J.) independently extracted the data to an electronic spreadsheet (Microsoft Excel; Microsoft Corp., Redmond, WA) and the senior author (R.F.H.) resolved any discrepancies.
Statistical Analysis
All data were initially extracted into an electronic spreadsheet (Microsoft Excel). Descriptive statistics were generated using JMP Pro, Version 13 software (JMP, Version 13. SAS Institute Inc., Cary, NC). The Review Manager (RevMan) software (Version 5.3. Cophenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used to determine proportions or mean differences using either fixed or random effects modeling, depending on the heterogeneity of the data analyzed. A P value of less than 0.05 was interpreted as statistically significant.
As in previous studies, to compare various knee-specific patient-reported outcomes (PROs) used by different studies, the scores were normalized to a scale out of 100 points where 0 is the worst and 100 is the best score. Improvement or change in a PRO score is defined as the postoperative score minus the preoperative score. Six studies reported on knee-specific PROs such as the Lysholm Knee Score (LKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Knee Injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC) score, Oxford Knee Score (OKS), and the Tapper-Hoover score. The most commonly used knee-specific PROs were LKS (3 studies), WOMAC (2 studies), and IKDC (2 studies) while the other PROs were used by 1 study each ( Table 2 ).
All Patient-Reported Outcomes after Meniscectomy for Body Mass Index (BMI) Categories by Article.
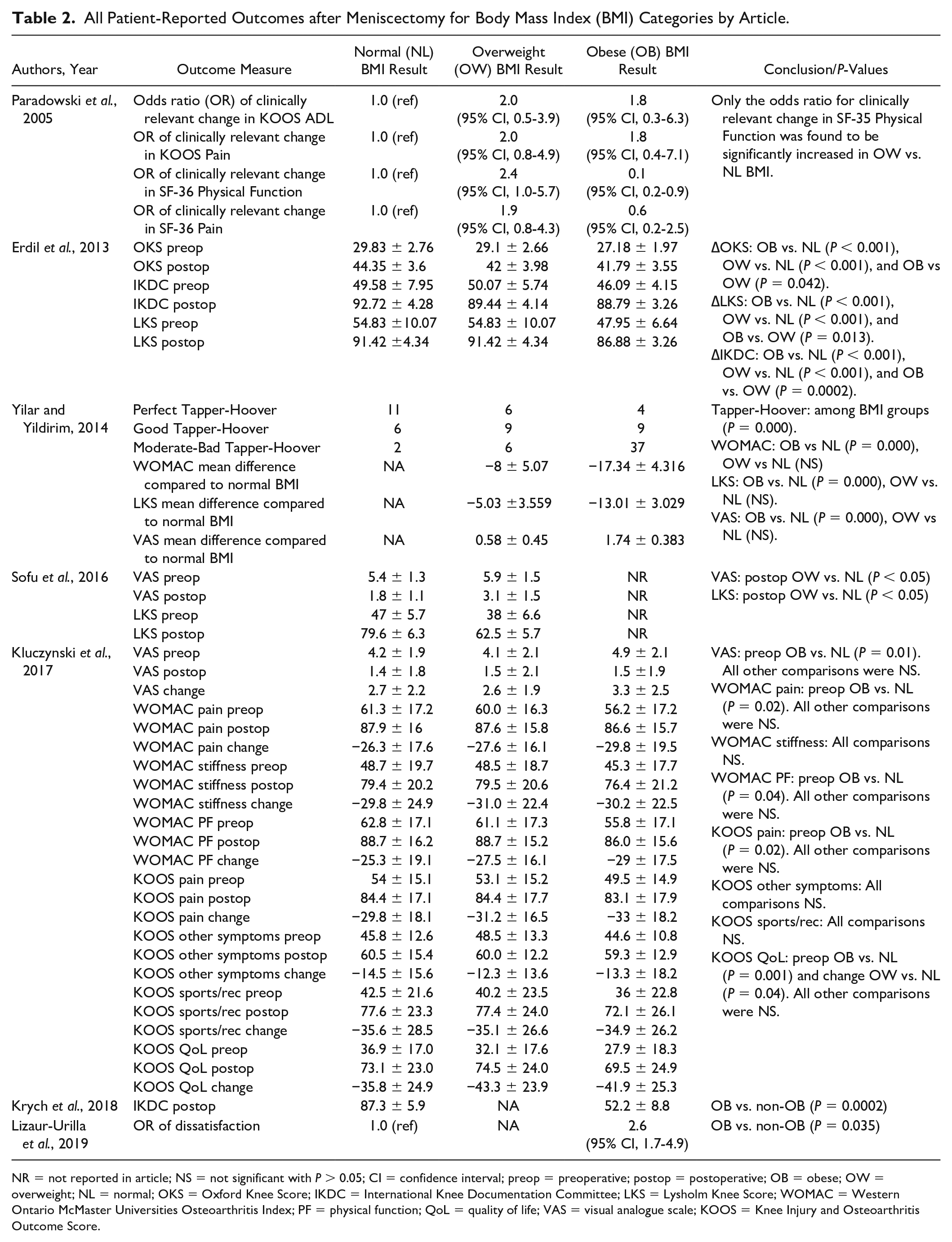
NR = not reported in article; NS = not significant with P > 0.05; CI = confidence interval; preop = preoperative; postop = postoperative; OB = obese; OW = overweight; NL = normal; OKS = Oxford Knee Score; IKDC = International Knee Documentation Committee; LKS = Lysholm Knee Score; WOMAC = Western Ontario McMaster Universities Osteoarthritis Index; PF = physical function; QoL = quality of life; VAS = visual analogue scale; KOOS = Knee Injury and Osteoarthritis Outcome Score.
Results
The final cohort, after excluding duplicate patient cohorts, consisted of 3,091 patients. Of these patients, 59.0% (n = 1,823) were male and 41.0% (n = 1,268) were female. A total of 618 patients were categorized as obese and 636 patients were categorized overweight. However, there were various definitions or thresholds for BMI categorization (Supplemental Appendix A). Most studies included 3 groups for normal BMI, overweight BMI, and obese BMI. However, a few studies used only 2 BMI groups such as nonobese versus obese or normal versus overweight,22-24 and 2 studies had additional groups such as morbidly obese at BMI ≥40 kg/m2 or underweight at BMI <18.5 kg/m2.25,26 The range of mean follow-up in the included studies was 12 to 216 months.
Erdil et al.
27
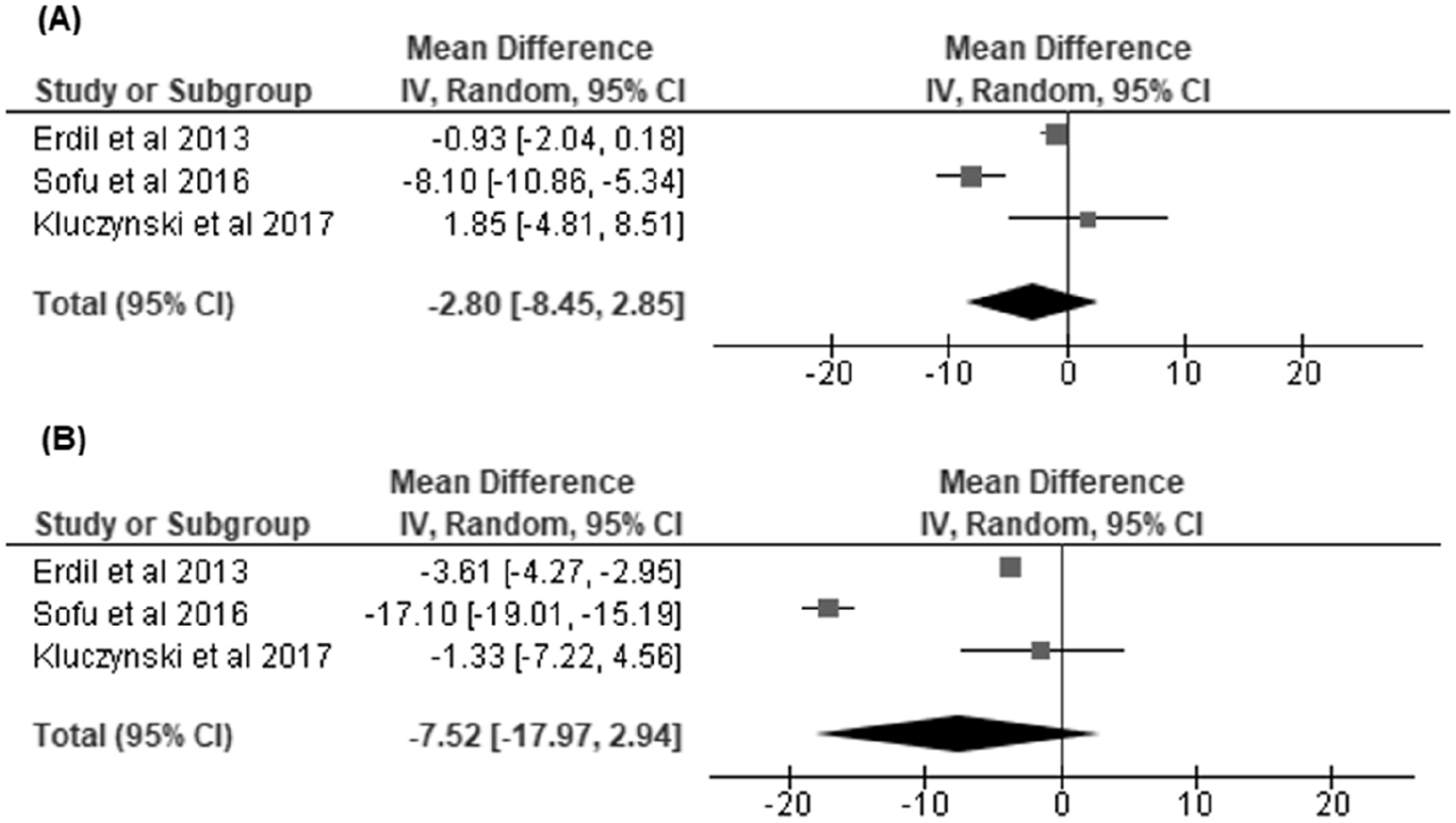
and Sofu et al.
22
reported on pre- and postoperative LKS scores, and our random model effects demonstrated worse preoperative scores in overweight/obese versus normal BMI patients with a mean difference of -6.06 [95% CI, −11.70 to −0.42]. However, there were no significant differences in final postoperative or improvement of scores with a mean difference of −9.57 [95% CI, −24.23 to 5.09] and −0.47 [95% CI, −4.99 to 4.05], respectively (
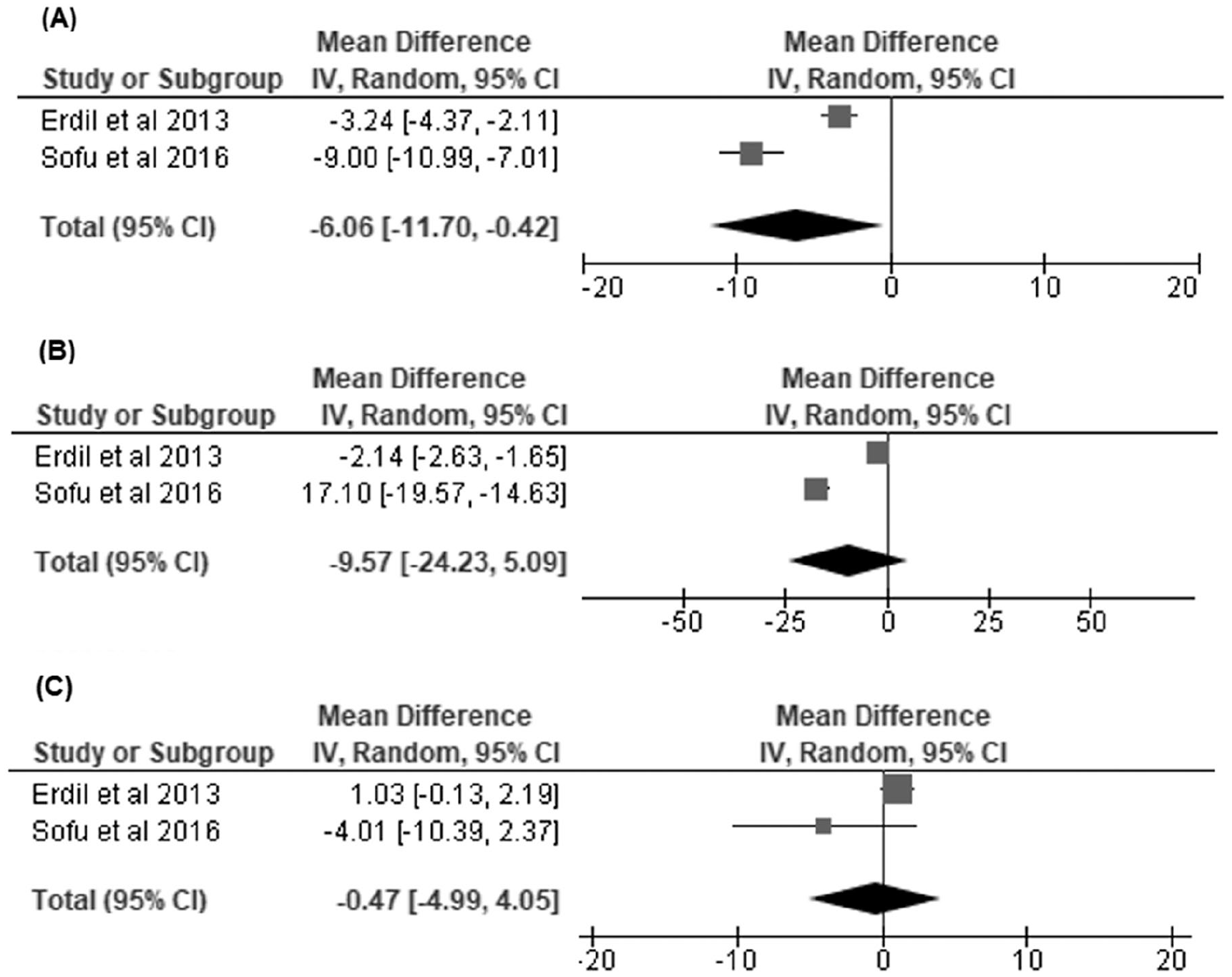
Overweight/obese versus normal body mass index (BMI) groups: (
Overweight/obese versus normal body mass index (BMI) groups: (
Obese versus normal body mass index (BMI) groups: (
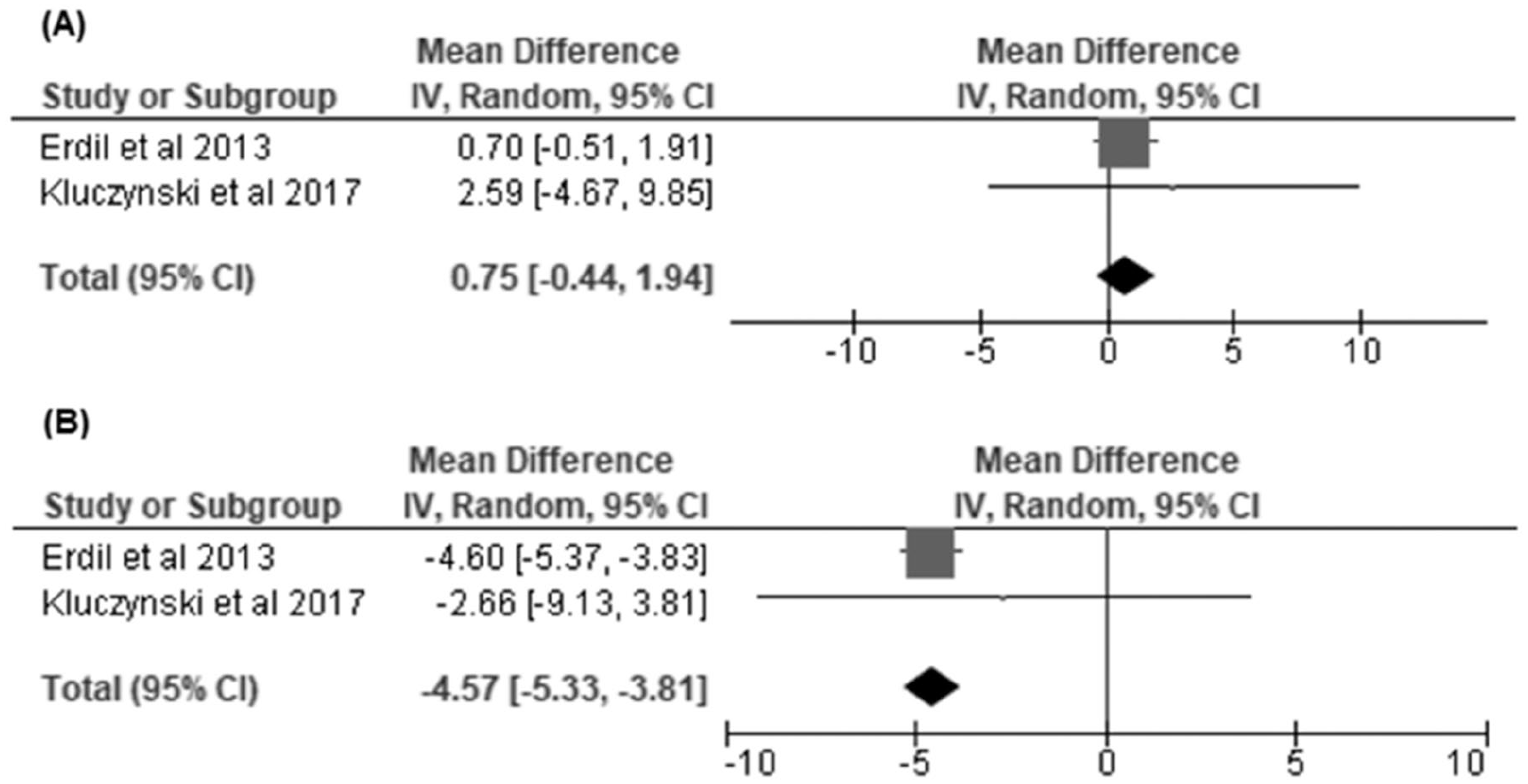
There were a few significant differences in other knee-specific PROs reported by singular studies that could not be included in our analyses ( Table 2 ). Kluczynski et al. 28 found that worse preoperative KOOS pain, KOOS QOL, WOMAC pain, and WOMAC physical function scores was associated with obese BMI. Similarly, Yilar and Yildirim 29 noted that patients with BMI >29 kg/m2 were more likely to have a worse postoperative WOMAC scores compared with patients with BMI < 25 kg/m2. They also reported increased frequency of moderate or bad Tapper-Hoover scores in higher BMI groups. Both Erdil et al. 27 and Krych et al. 23 observed that increased improvement in IKDC scores was associated with obese BMI. Finally, Erdil et al. 27 also showed better improvement in OKS in obese and overweight patients when compared with the normal BMI group.
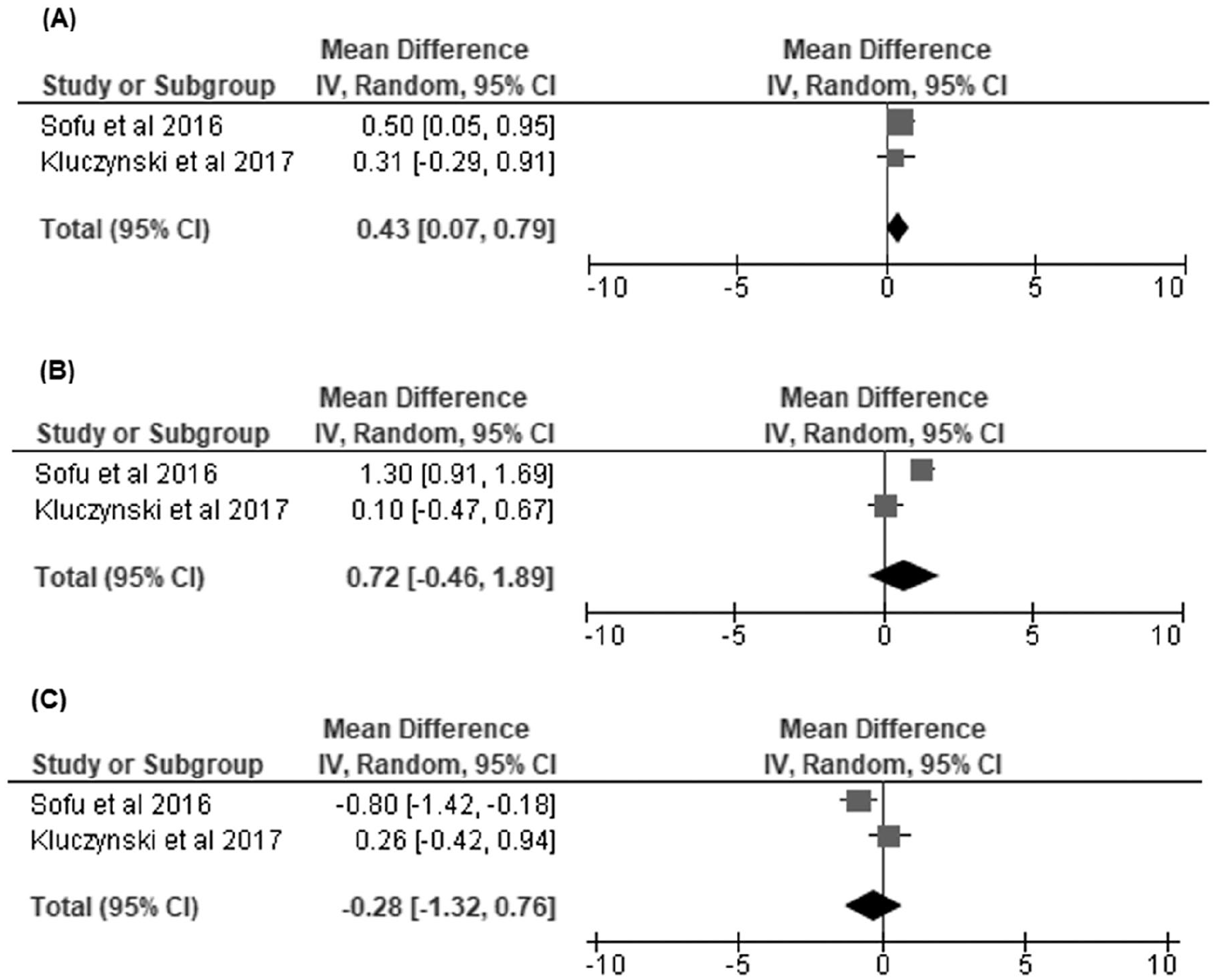
With regard to pain, Sofu et al.
22
and Kluczynski et al.
28
reported on pre- and postoperative visual analogue scale (VAS) for knee pain, and our random-effects model demonstrated that overweight/obese BMI was associated with worse preoperative VAS scores at a mean difference of 0.43 [95% CI, 0.07 to 0.79] (
Overweight/obese versus normal body mass index (BMI) groups: (
Regarding other outcome metrics, Paradowski et al. 20 looked at the odds ratio of clinically relevant change in Short Form 36 (SF-36) Physical Function and Pain scores, reporting no significant differences among BMI groups except for increased change in SF-36 physical function scores for overweight BMI. Lizaur-Urilla et al. 24 found that patients with BMI >30 kg/m2 were more likely to be dissatisfied based on a Likert-type scale survey ( Table 2 ).
For objective outcomes, Kluczynski et al. 28 was the only study to evaluate pre- and postoperative extension deficit, flexion, and presence of knee effusion ( Table 3 ). The authors did not find any significant differences regarding neutral extension deficit but did observe that obese BMI patients were more likely to have decreased flexion both pre- and postoperatively. However, no significant difference was found when comparing change in flexion. Additionally, they found that both obese and overweight patients were more likely to have knee effusion preoperatively.
Objective Outcome Measures of Meniscectomy for Body Mass Index (BMI) Categories by Article.
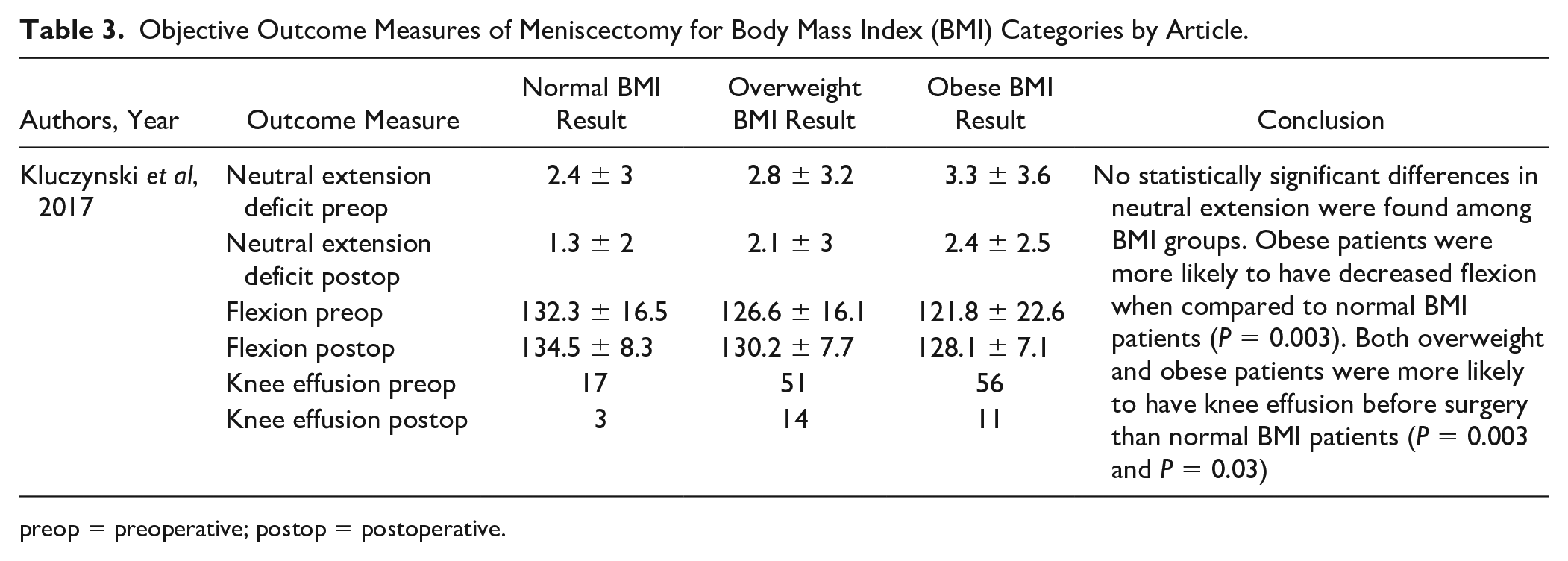
preop = preoperative; postop = postoperative.
Several studies evaluated the incidence of degenerative joint disease following APM ( Table 4 ) at a mean or minimum follow-up of 5 years postoperatively. Two articles18,30 reported odd ratios for radiographic tibiofemoral OA at latest follow-up; however, our random model effects did not demonstrate a significantly increased odds ratio (OR) for obese when compared to normal BMI (OR, 5.34 [95% CI, 0.75 to 38.11]) or overweight/obese versus normal BMI (OR, 1.52 [95% CI, 0.99 to 2.32]) as seen in Figure 6 . Regarding other measures of OA that could not be included in our analysis, Englund and Lohmander 18 also evaluated patellofemoral OA as well as symptomatic tibiofemoral OA, finding increased ORs associated with obese BMI ( Table 4 ). Lizaur-Utrilla et al 24 also observed increased OR for progression of OA in obese patients, as measured by change in Kellgren-Lawrence (K-L) grade pre- and postoperatively.
Osteoarthritis Outcomes of Meniscectomy for Body Mass Index (BMI) Categories by Article.
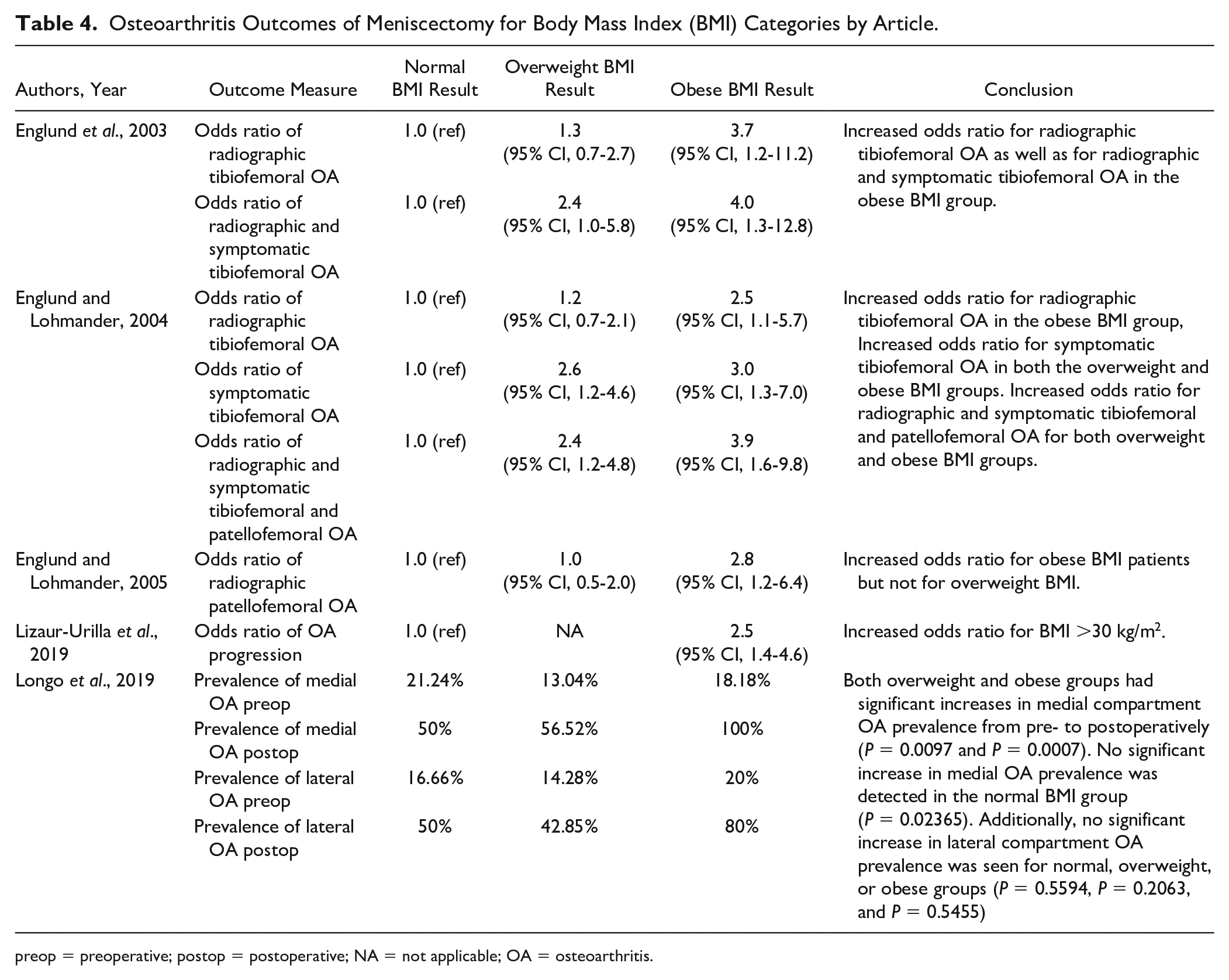
preop = preoperative; postop = postoperative; NA = not applicable; OA = osteoarthritis.
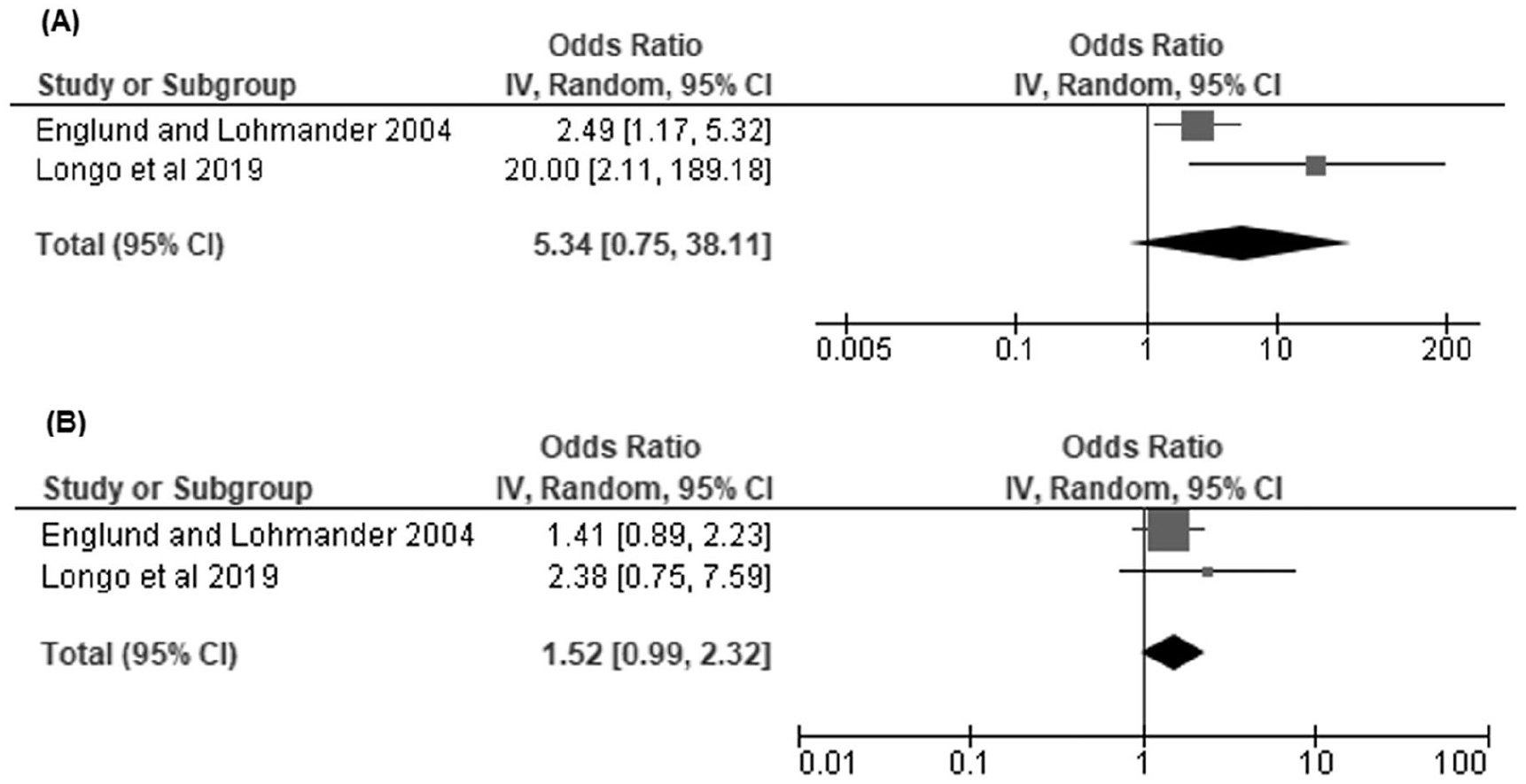
Radiographic osteoarthritis (OA): (
Complication or failure rates after APM stratified by BMI were studied by Erdil et al. 27 and Krych et al. 23 ( Table 5 ). Erdil et al. 27 reported that the obese BMI group had a significantly higher percentage of patients who experienced early unspecified complications after meniscectomy at 36.7% (P = 0.037). Similarly, Krych et al. 23 described that the obese BMI group also had significantly higher failure rate compared with the nonobese BMI group (94.4% vs. 44.4%, P = 0.004). They defined failure as progression to total knee arthroplasty (TKA) or an IKDC score less than 75.4 points. 23
Failures and Complications for Body Mass Index (BMI) Categories by Article.
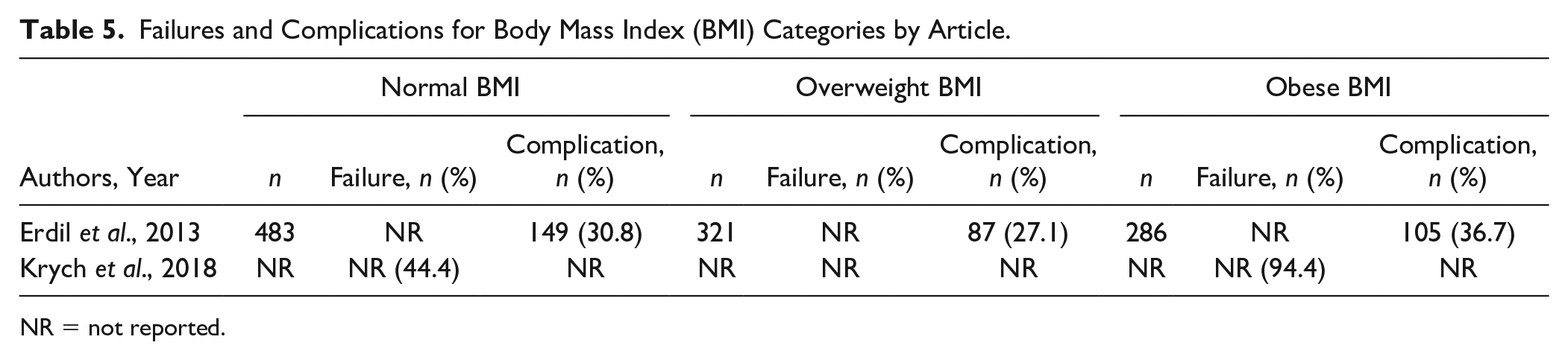
NR = not reported.
Of the studies investigating differences in pathoanatomy or pathophysiology associated with increased BMI, 3 studies looked at presence of medial meniscus posterior root tears and suggested that there may be an association with obese BMI ( Table 6 ).25,26,31 Additionally, Yeh et al. 32 observed that professional basketball athletes with a BMI >25 kg/m2 had increased risk of lateral versus medial meniscus tears in addition to an overall increased risk of meniscal injury. Last, Rai et al. 33 observed differences in meniscal gene expression among BMI categories in patients undergoing meniscectomy.
Pathophysiology of Meniscal Injury for Body Mass Index (BMI) Categories by Article.
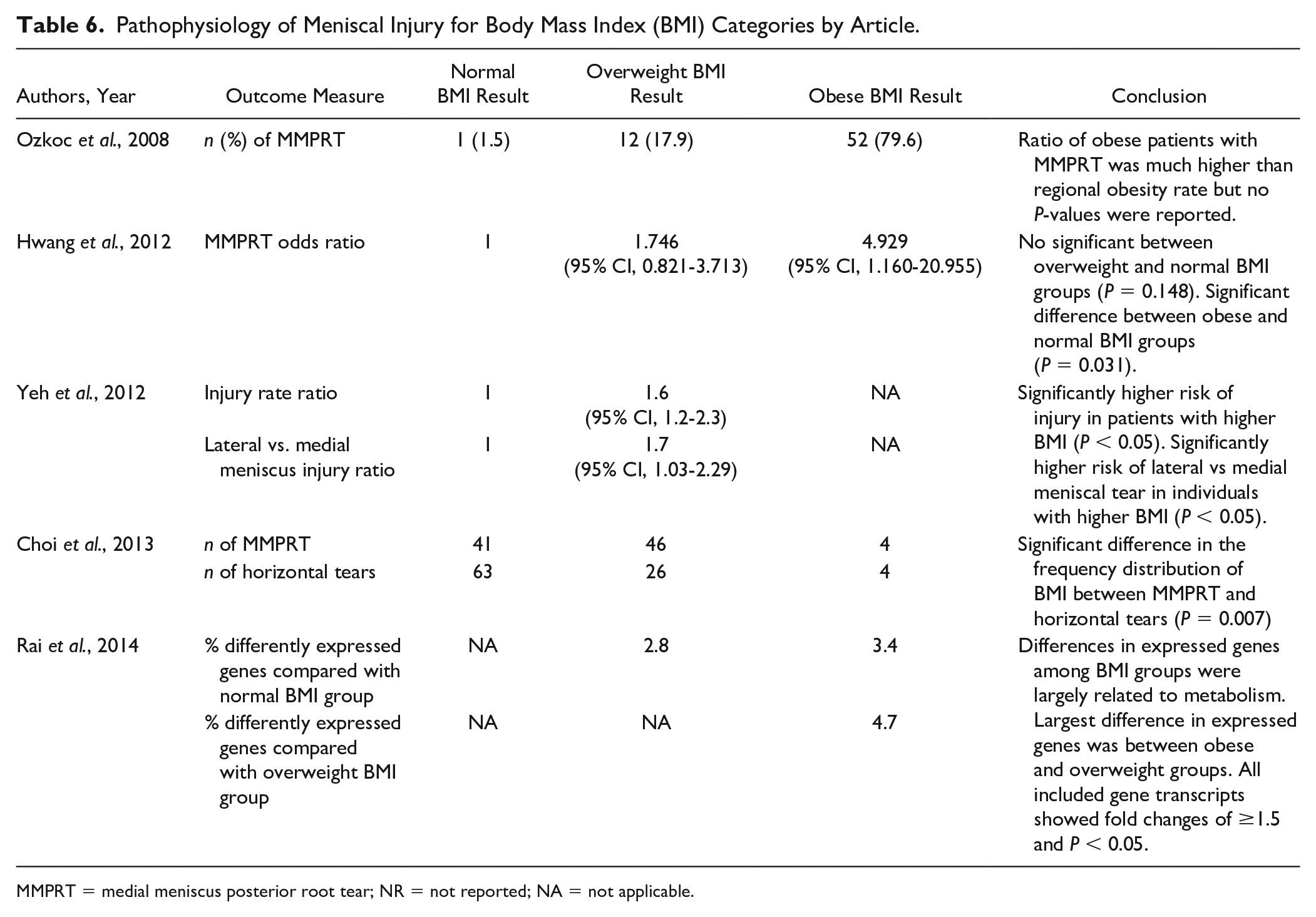
MMPRT = medial meniscus posterior root tear; NR = not reported; NA = not applicable.
Discussion
As the prevalence of obesity continues to rise, it is important for orthopedic surgeons to understand how obesity may affect evaluation, treatment, and surgical outcomes of injuries such as meniscal tears. To the authors’ knowledge, this study is the first meta-analysis on the surgical outcomes associated with obese BMI categorization in patients undergoing APM.
Regarding knee-specific PROs, this study suggests that although obesity may be associated with worse pre- and postoperative scores, there is no strong evidence for any differences in score improvement compared with nonobese patients. Thus, these findings suggest that at short- to mid-term follow-up, obese patients may have similar improvement of symptoms and/or function after meniscectomy as patients with normal BMI. If meniscectomy successfully removes a meniscal tear as the culprit for causing pain and mechanical symptoms, it is plausible that BMI may not significantly affect how much relief a patient experiences in the short-term follow-up period.
In our analysis of the development of radiographic OA as a long-term outcome/complication of APM, there were no significantly higher ORs associated with obese and/or overweight BMI. However, the results were close to statistical significance, and a few studies noted differences individually therefore, these studies may be underpowered. Also, it was variable whether studies categorized OA as being clinically symptomatic in addition to radiographically evident, and these studies did not consistently indicate if OA was present preoperatively as well as at follow-up. Thus, future studies should aim to delineate symptomatic vs non-symptomatic OA both pre- and postoperatively.
Overall, there is a lack of studies that report on surgical complication or failure rates after APM by BMI category. Articles in this review indicated higher rates of complications and failure in obese patients but did not include a statistical analysis. Based on studies of BMI as a risk factor in other types of surgeries, there could be a theoretical increased risk of poor wound healing and infection.13,34 However, in general knee arthroscopy is considered to have an overall low complication rate; therefore, individual studies are likely to be underpowered to detect differences by BMI categories. In the context of meniscectomy, failure can encompass revision/further meniscal surgery, high tibial osteotomy, conversion to TKA, or little to no relief of symptoms.18,21,22,24 Thus, more failures might be expected in the obese population due to increased joint loading forces or altered biomechanics that contribute to either meniscal retear or the development of OA.35,36
Regarding possible differences in pathoanatomy of meniscal tears, there is some evidence obesity may be associated with a higher risk of medial meniscal root tears. This could be due to differences in biomechanics and/or mechanism of injury as elevated BMI is likely to chronically expose the meniscus to higher forces that could act with a greater degree on the medial meniscus posterior horn due to its lack of mobility and close attachment to the tibia. 37 While the studies examining this did not report the treatment of these tears, we felt it was important to include these findings in this article as part of our secondary goals. APM in the setting of a root tear has questionable utility, and meniscal root tears are best treated with root repair in most patients. In another study, an association between lateral versus medial meniscal tears in National Basketball Association athletes with a BMI >25 kg/m2 was reported. 32 However, BMI is a poor measurement of body fat content in professional athletes due to increased muscle mass and therefore, this study is unlikely to be generalizable to a normal population. 38 Last, 1 study provided evidence that obesity may be associated with changes in gene expression related to meniscal tissue degeneration. 33 However, the tissue specimen samples were taken at time meniscectomy so it is unknown if these genetic differences are baseline or in response to injury.
As with any meta-analysis, this study has several inherent limitations such as being limited to the strength of existing literature. The included studies used different definitions for BMI categories, osteoarthritis progression, or surgical failure. Additionally, PROs were not reported in a uniform manner. Another limitation is that many articles were excluded for using BMI as a continuous variable. However, the results from these types of analyses were inconsistent in indicating whether BMI was an independent predictor of PROs after meniscectomy. Possible reasons for this include a nonlinear relationship between BMI and PROs, underpowered studies, or the use of only postoperative versus change in PRO scores. Finally, the inclusion criterion of 1-year follow-up may be short for assessment of certain metrics. However, a minimum or mean follow-up time of 5 years was utilized in the studies investigating the development or progression of OA.
In conclusion, obesity is associated with worse knee function after APM, and patients with elevated BMI have worse preoperative knee pain and function. However, there is no difference in amount of pre- to postoperative improvement in symptoms, suggesting that APM can be as beneficial to overweight and obese patients as to patients with normal BMI. Further prospective research with longer follow-up is necessary to determine the comparative effectiveness of APM in patients with elevated BMI.
Supplemental Material
Appendix_A_BMI_definitions – Supplemental material for Outcomes of Partial Meniscectomy in Obese Patients: A Systematic Review and Meta-Analysis
Supplemental material, Appendix_A_BMI_definitions for Outcomes of Partial Meniscectomy in Obese Patients: A Systematic Review and Meta-Analysis by Tina Zhang, Julio J. Jauregui, Michael Foster, Jonathan D. Packer, Sean J. Meredith, Natalie L. Leong and R. Frank Henn in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.J.M. and J.P. are board or committee members of the American Orthopaedic Society for Sports Medicine. R.F.H. has previously received research support from Arthrex, Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.