
Abstract
Objective
Determine if femoral chondral cartilage degeneration on cadaveric knee joints exacerbate differently with aging between the sexes.
Methods
A total of 85 cadaveric femurs were assessed for macroscopic femoral condyle pathology using a scale for gross signs of osteoarthritis. Raters scored specimens and raters’ scores were averaged to provide each specimen a Disease Severity Score (DSS).
Results
The DSS for the 80+-year-old population was greater than the DSS of the 70- to 79-year-old population (*P < 0.05) and the <70-year-old population (**P < 0.01). Specimens that scored a DSS of 2 and higher were assessed for their specific site of most severe degeneration. The most severe degeneration on the articular cartilage was most regularly on the patellar fossa. The second most degenerated region varied by age and biomechanical alterations. There were no significant changes in DSS between the sexes within the age groups.
Conclusions
No difference was shown between the sexes in the severity or location of degeneration indicating that men and women are likely affected by the same biomechanical changes that spur on osteoarthritis in their eighth decade of life (70s) and later. Lateral femoral degeneration predominates in younger populations. When patients approach their 70s, medial degeneration begins to predominate likely based on an increase in shearing at the knee joint.
Introduction
Osteoarthritis (OA) is a degenerative joint condition that affects more than 27 million adults in the United States. 1 OA is considered the most prevalent musculoskeletal disease and the weightbearing joints, including the spine, hip, knee, and ankle, are particularly prone to the pathogenesis. Mechanical influences are placed on these joints and when the biomechanics of these influences become excessive or abnormal OA can develop. Such mechanical forces are highly modifiable based on weight loss, activity, and alignment adjustments. This makes them a primary address in current and future conclusions. 2 A systematic review of the literature stating prevalence data of OA in America determined that approximately 27.3% of women, 21% of men, and 23.9% of the overall population have OA. 3 Given that obesity is reaching epidemic proportions in the United States and is a cause for altered biomechanics at the knee joint, OA prevalence is also estimated to increase.2,4 Particularly considering the increases in life expectancy of the aging population, OA has become a leading cause of disability.2,5
Long thought to be exclusively due to “wear and tear,” it is now understood that the cause of OA is multifactorial. Abnormal inflammatory signaling and joint tissue remodeling are hallmarks of the disease and affect nearly all components of synovial joints. 6 This study is part of an ongoing program that assesses gross morphometric changes to the knee joint with OA. Thinning of the anterior cruciate ligament (ACL), loss of menisci coverage, and degeneration of the articular cartilage on the tibial plateau were quantified from 21 cadaveric knee joints in a preliminary study. 7 This is the first assessment employing cadaveric knee dissections from 5 cohorts of donors utilized in the medical gross anatomy course at the University of Utah’s School of Medicine from 2014 to 2018. Appraisal of this larger population has allowed investigators to more confidently report age-related changes as well as changes within the age groups based on gender, subpopulations of age, clinical history, and occupation.
Previous studies in this program focused on changes to the tibial plateau, ACL, and the menisci of the knee joint. Statistically significant findings related to the pathogenesis of OA in those structures lead investigators to assess the distal articular cartilage of the femur given its direct relationship. The articular cartilage of the tibial plateau was assessed for “percent degeneration” using ImagePro software to trace regions of linear cracks, stellate fractures, fibrillations, erosions, and cortical bone mass exposure. The contours of the tibial plateau were minimal enough that this technique could be used to document surface area losses of cartilage on the tibia as long as the minimal contour of the plateau was addressed in the methods as a limitation of the study. The femoral condyles display substantial convexity, therefore a qualitative grading scale for gross signs of OA was modified and used to assess the degenerative changes seen on the proximal aspect of the cadaveric knee joints.
It was expected that donors that displayed obesity during their life span would have different sites of visible OA degeneration compared to donors that did not display obesity and its comorbidities. It was also hypothesized that donors that displayed substantial muscular atrophy to the muscular compartments reinforcing the knee joint would display more substantial, visible signs and symptoms of OA on their distal femurs. The specific, anatomical compartments include the anterior and posterior compartments of the thigh and the superficial posterior compartment of the leg. These compartments, representing the hamstrings, quadriceps, and calf muscles, neutralize the knee joint on the sagittal, flexion-extension plane. It warrants mentioning that the hamstring muscles and the gastrocnemius muscle of the superficial posterior compartment of the leg aid in frontal plane and rotational movement, and therefore, stabilization of the knee joint on that plane. The quadriceps muscles, specifically the vastus medialis and vastus lateralis components, are crucial for stabilizing the patella in the patellar fossa and intercondylar fossa of the femur during gait and standing. 8 A lack of neutrality between these 2 muscles’ frontal plane, patellar pull can displace the patella outside of its normal tracking sites. This may cause abnormal friction and inflammation and hence, OA, in the patellar fossa and internal, anterior femoral cartilage.
Specimens were not designated as obese or not obese prior to this study and analysis. Determination of obese classification of a single donor was based on the sites of cartilage degeneration on the femoral condyles. Obesity sways tibiofemoral compression forces to the lateral aspect of the knee joint. During single-leg stance of gait, forces in the joint are equivalent to 3-6 times an individual’s body weight. These compression forces can be increased several times over when an individual is partaking in high-impact activities.2,4,9 Based on these proven biomechanical findings, lateral condylar degeneration in this study is thought to be determined by the lateral displacement of tibiofemoral compression forces due to excess body weight per the given skeletal frame. This represents a minor limitation of the assessment given some donors may give rise to lateral degeneration in the knee joint by other, less likely, mechanisms. Future studies will assess thickness of the tela subcutanea and muscle mass in cross-sectional anatomy of the thigh and leg to give rise to quantitative data related to cause of degeneration; this population is currently being harvested to reach a statistically assessable quantity.
Methods
Cadaver Sample and Dissection
A population of 85 cadavers (28 females, 58 males) were analyzed for signs of OA in the knee joint. Some cadavers offered bilateral knee specimens and others, unilateral. There were a total of 2 female knee joints and 20 male knee joints in the <70-year-old age group, 14 female joints and 28 male joints in the 70- to 79-year-old age group as well as 12 female joints and 9 male joints in the ≥80-year-old age group ( Table 1 ). The population was divided into 3 age cohorts: <70 years old (n = 22), 70 to 79 years old (n = 42) and ≥80 years old (n = 21). There were no specimens included in this assessment pool that had documented surgeries performed on the joint at hand. Cadavers were provided to the investigators from the University of Utah Body Donation Program in Salt Lake City, Utah. Physical demographics such as height and weight are provided by the Body Donation Program but represent an approximation that is estimated by the party registering the donor with the program such as a nurse, police officer, or a family member. These data were not incorporated into the study as the heights and weights represent measurements at death. It can be assumed that the weight measurement does not necessarily represent the weight of the donor during the decades where pathogenesis of OA was more noteworthy, especially for donors where the cause of death was a long-standing disease such a cancer.
Breakdown of Assessment Population by Age Group (<70 Years Old, 70-79 Years Old, and ≥80 Years Old). a
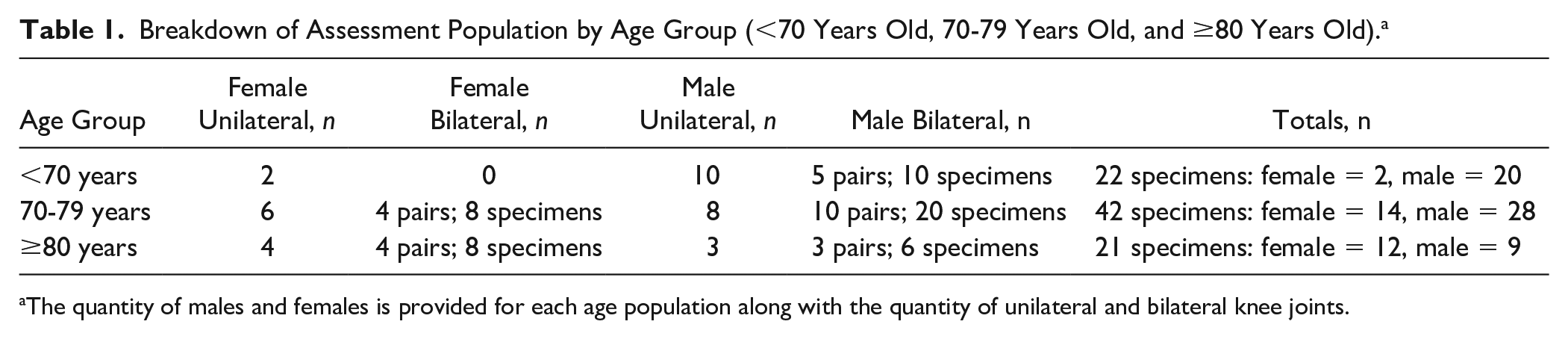
The quantity of males and females is provided for each age population along with the quantity of unilateral and bilateral knee joints.
Knee joints were disarticulated from the cadavers with trans-femoral and trans-tibiofibular cuts. Once knee joints were removed, the quadriceps tendon, patella, and patellar ligament were together reflected inferiorly toward the tibial tuberosity, opening the anterior fibrous capsule. The vastus lateralis muscles and the vastus medialis muscle were bluntly dissected away from the distal femur. Posteriorly, the capsule was dissected away from the intrasynovial anatomy of the knee joint, including the femoral condyles and menisci. This project (Protocol 150430-04) was reviewed and approved by Rocky Mountain University of Health Profession’s Institutional Review Board in Provo, UT. This project was determined to be research not involving human subjects.
Morphometric Analysis of the Femoral Articular Cartilage and Its Degeneration in the Knee Joint
Once the joint was opened anteriorly, all components of the joint capsule and the collateral ligaments were removed leaving the femur and tibia attached solely by cruciate and meniscofemoral ligaments. At this point in the dissection protocol, all ligaments were bisected from their attachments in the intercondylar notch of the femur. Ample photography was taken of the femoral articular cartilage including where the joint capsule had periosteal attachments at the chondral margin. A Nixon Coolpix A900 digital camera was utilized for photography of each specimen. A minimum of 4 photos was taken for each specimen to provide complete views of the patellar fossa, anterior, inferior and posterior aspects of the femoral condyles. Care was taken to ensure the chondral margins were adequately photographed for the assessment of osteophyte growth. All specimens were photographed with a calibrated drafting ruler to provide a visual gauge for size.
Once the photography was collected for all specimens, a blinded individual provided each specimen a new identification number, rearranged the order of specimen dissection and organized the photographs in Microsoft PowerPoint for ease of rater review. Each specimen was assessed and given a Disease Severity Score (DSS), which identified the gross signs of OA and classified the severity of OA on a 0-to-4 qualitative scale (scale modified from Kovler et al. 10 ). Specimens were classified as: Normal Cartilage (0), Questionable if OA is present (1), Mild OA (2), Moderate OA (3) or Severe OA (4). Table 2 describes the specific gross surface features of the cartilages that must be present to be classified at each grade of disease. Figure 1 displays representative images of each grade of disease severity. This scale does not incorporate an assessment of measured surface area damaged; only overall appearance of the cartilage was assessed. This could be viewed as a limitation of the tool given descriptors such as “extensive” and “large areas” are not specifically defined for the raters prior to review of specimens. This concept also likely relates to the need for experience in assessing arthritic joints as determined by statistical assessment of the interrater reliability. This scale has been used in two previous studies which generated statistical significance in similar, blinded assessments of the hip and wrist joints.10,11 No specific statistics for validation were performed; the study at hand is the first study to show statistical reliability of the tool.
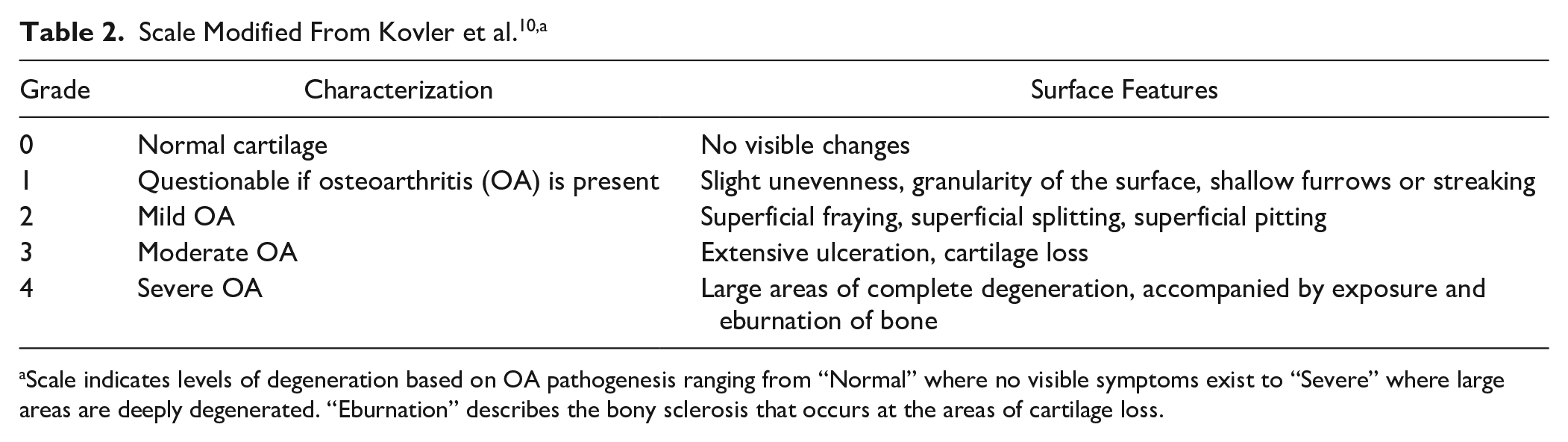
Scale indicates levels of degeneration based on OA pathogenesis ranging from “Normal” where no visible symptoms exist to “Severe” where large areas are deeply degenerated. “Eburnation” describes the bony sclerosis that occurs at the areas of cartilage loss.
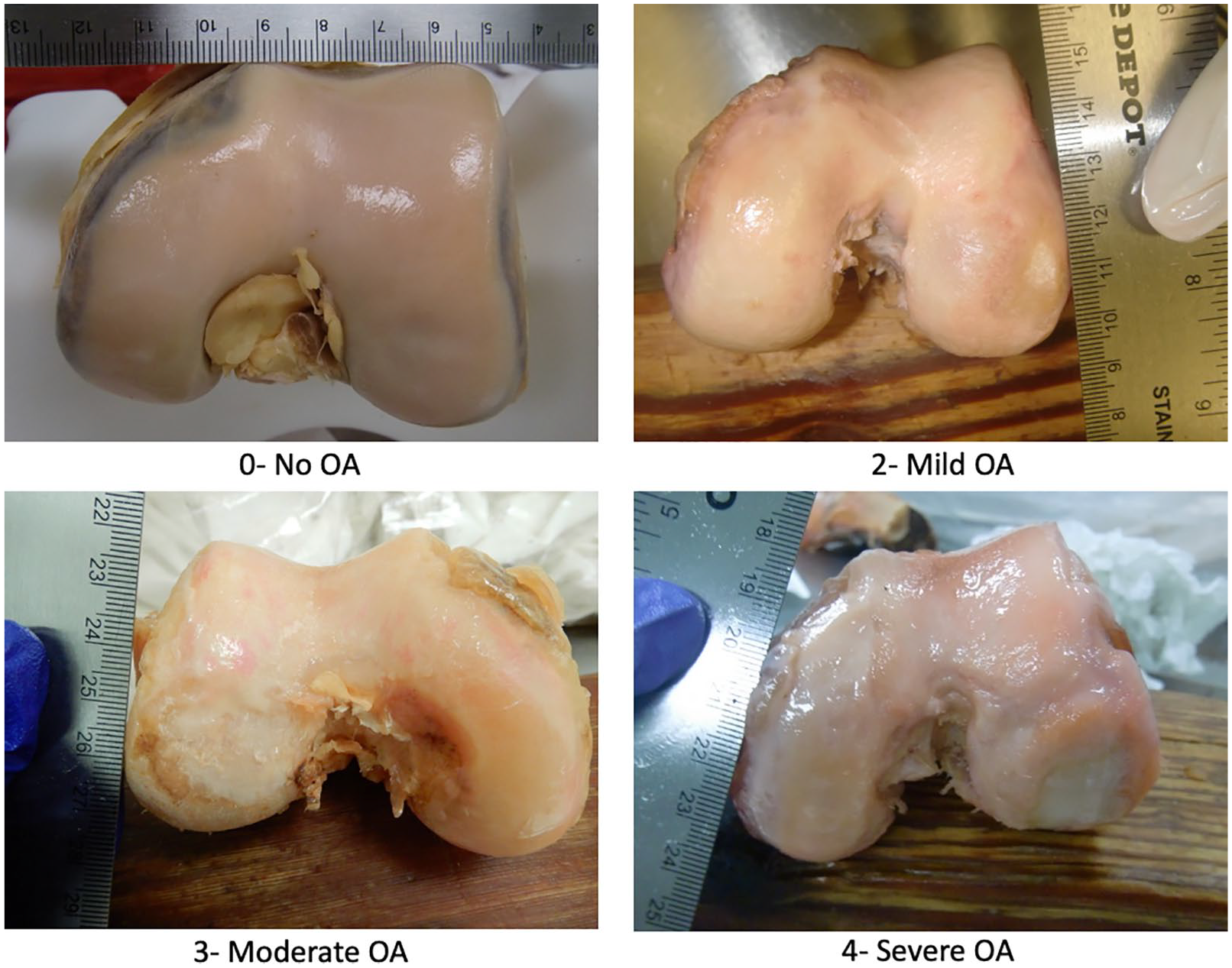
Representative images for the 4 grades of disease severity on the femoral condyles. A score of “0” represents no signs of osteoarthritis (OA). A score of “1” is not represented on this figure as “Questionable OA presentation” was sparingly awarded by raters.
Statistics
All statistical analyses were ran using SPSS statistics software. The interrater reliability for OA rating were evaluated using Krippendorff’s alpha (Kα). Reliability was insufficient when assessing all 4 raters so assessment of interrater reliability was repeated with only 2 of the raters’ DSS ratings. The mean DSS rating of the 2 investigators was used as the dependent variable. The 2 raters included in the final analysis for interrater reliability were the raters with the most experience in assessing arthritic specimens and conducting osteoarthritis research. Normality of the data was evaluated using the Kolmogorov-Smirnov test. Condylar cartilage DSS ratings for the 3 age populations were compared using the Kruskal-Wallis Test with a Dunn’s posttest for multiple comparisons. Condylar cartilage DSS ratings between the sexes overall and within the age populations were compared using the Mann-Whitney U test for nonparametric data. The influence of age and gender on OA rating was evaluated using Kendall’s τb.
Results
Reliability of the Assessment Tool and the Disease Severity Scores
Interrater reliability, as assessed by Krippendorff’s alpha (Kα), was inadequate (α = 0.5975) when assessing scores from all 4 raters. Assessment of interrater reliability was repeated with only 2 of the raters’ DSS ratings to achieve a strong score indicating reliability of the assessment scale in this setting (α = 0.8361). For the remaining analyses, nonparametric statistics were used as the distribution of the ≥80-year-old age group was negatively skewed, greater than 2 times the standard error of skewness (−1.41, SEskew = 0.49) and violated normality (P < 0.01). The ≥80-year-old age group (n = 22) had an average DSS of 3.19 ± 0.69 compared with a DSS of 2.7 ± 0.85 and a DSS of 2.52 ± 0.95 for specimens 70-79 years old (n = 42) and specimens <70 years old (n = 22), respectively. The DSS for the ≥80-year-old population was significantly greater than the DSS of the <70-year-old population (**P < 0.01) and the DSS of the 70- to 79-year-old population (*P < 0.05; Fig. 2 ). Within the entire sample, the average DSS for females was significantly greater than the average DSS for males (**P < 0.01; Fig. 3 ). The average male DSS was 2.75 and the average female DSS was significantly more severe, with a value of 3.34. Gender (τb = 0.24, P < 0.01) was a slightly larger correlate to DSS ratings in comparison with age (τb = 0.21, P < 0.05). In the 70- to 79-year-old age group and the ≥80-year-old age group, the males and females did not significantly differ in their DSS ratings (70- to 79-year-old males DSS rating = 2.71, n = 28, females DSS rating = 3.21, n = 14; ≥80-year-old males DSS rating = 3.17, n = 9, females DSS rating = 3.54, n = 12). There were too few female specimens in the <70-year-old age group to make a statistical comparison (females n = 2; males n = 20).
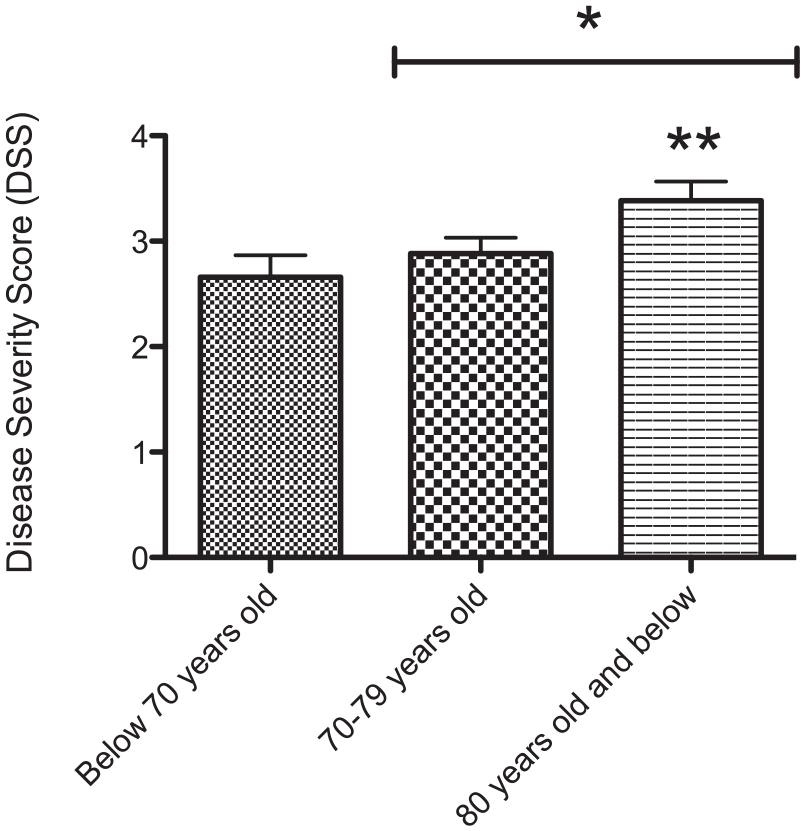
Histogram represents statistical comparison of Disease Severity Scores (DSS) between the 3 age groups. Condylar cartilage DSS ratings for the 3 age populations were compared using the Kruskal-Wallis test and Dunn posttest for multiple comparisons. The DSS for the ≥80-year-old population was significantly greater than the DSS of the <70-year-old population (**P < 0.01) and the DSS of the 70- to 79-year-old population (*P < 0.05).
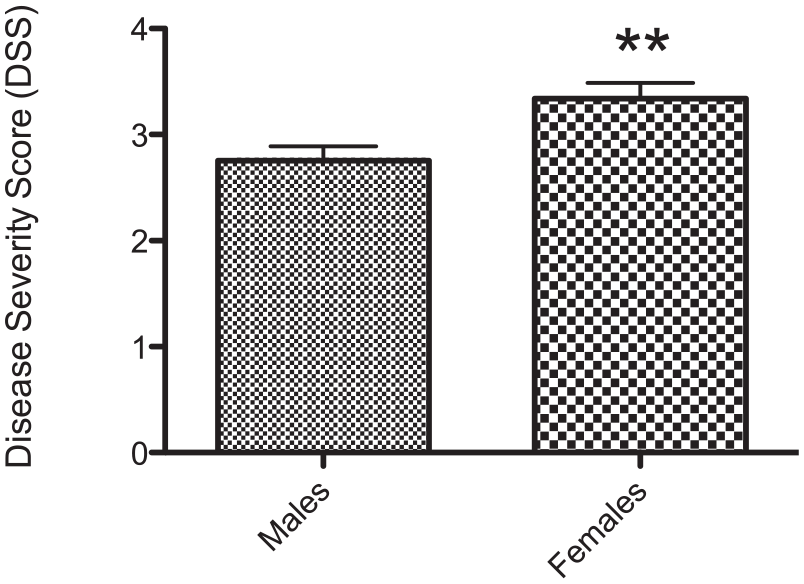
Histogram represents a statistical comparison of Disease Severity Scores (DSS) between the males and females in the overall sample. Condylar cartilage DSS ratings were compared using the Mann-Whitney U test for nonparametric data. In the overall sample, the average DSS for females was significantly greater than the average DSS for males (**P < 0.01).
Common Sites of Degeneration
Specimens that scored a DSS of 2 and higher, representing mild OA to severe OA, were assessed for their specific site of most severe degeneration. The anteroinferior aspects of the medial and lateral femoral condyles and the patellar fossa were assessed when determining the site of most severe degeneration per specimen. The most severe degeneration on the distal femoral articular cartilage was regularly on the patellar fossa. The most severe site of degeneration was seen on the patellar fossa in 45% of specimens <70 years old, 60% of specimens 70 to 79 years old, and 50% of specimens ≥80 years old. The lateral condyle was the second most degenerated region in the <70-year-old specimens (27%). The medial condyle became the second most degenerated region in the 70- to 79-year-old specimens (38%) and the ≥80-year-old specimens (68%).
The males and females in the <70-year-old population displayed a 6:4 and a 1:0 ratio for “lateral femoral condyle” versus “medial femoral condyle” as a site of most severe deterioration, respectively. The female and male specimens typically showed more substantial degeneration on one condyle or the other. There were 6 exceptions (6/16 specimens with a DSS >2) for the male population where equivalent disease presented on both condyles. These specimens were left out of the disease presentation ratios. Excluding 5 male specimens, all knee joints in the <70-year-old population had notable degeneration on the patellar fossa along with degeneration on the condylar cartilage ( Tables 3 and 4 ).
Sites of Degeneration in Females of the <70-Year-Old Population. a
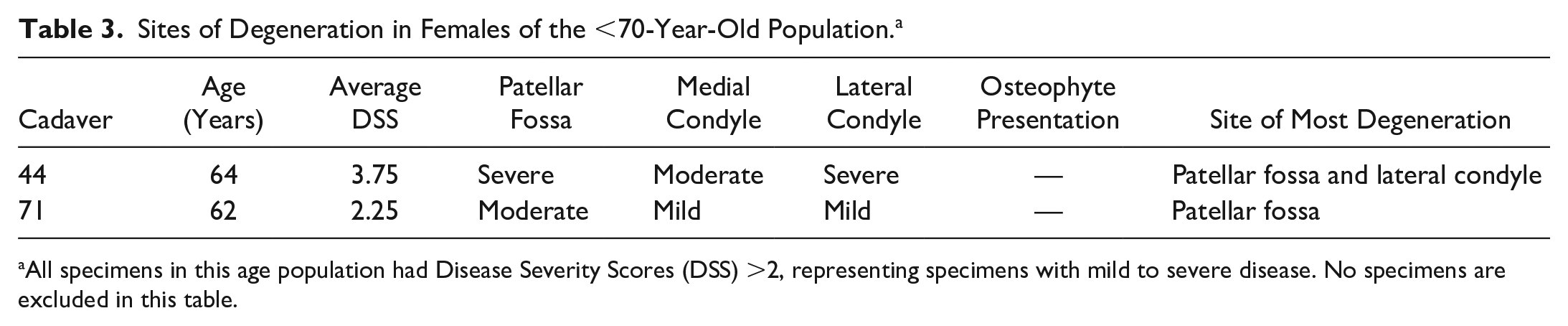
All specimens in this age population had Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. No specimens are excluded in this table.
Sites of Degeneration in Males of the <70-Year-Old Population. a
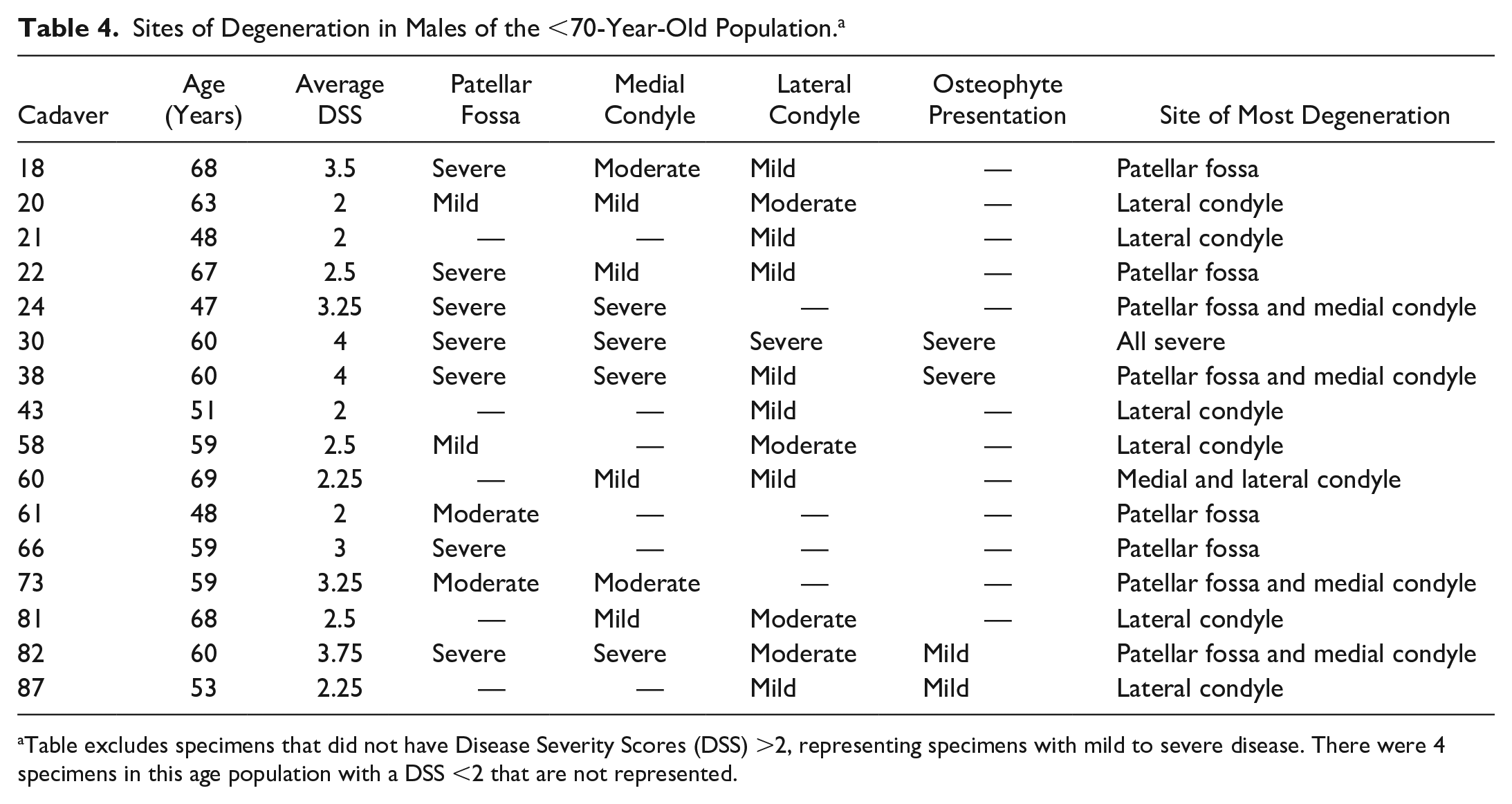
Table excludes specimens that did not have Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. There were 4 specimens in this age population with a DSS <2 that are not represented.
The males and females in the 70- to 79-year-old age group displayed a split distribution of “lateral femoral condyle” or “medial femoral condyle” as the site for the second most severe degeneration after the patellar fossa. There was a 3:5 ratio of lateral versus medial degeneration for females and a 4:9 ratio for males; this excludes specimens that had the most severe degeneration solely on the patellar fossa or equivalent severity on all sites. The female and male specimens typically showed more substantial degeneration on one condyle or the other. There were 3 exceptions (3/13 specimens with a DSS >2) for the female population and 7 (7/23 specimens with a DSS >2) exceptions for the male population where equivalent disease presented on both condyles. These specimens were left out of the disease presentation ratios. With the exception of 3 female specimens and 2 male specimens, all knee joints in the 70- to 79-year-old population had notable degeneration on the patellar fossa along with degeneration on the condylar cartilage ( Tables 5 and 6 ).
Sites of Degeneration in Females of the 70- to 79-Year-Old Population. a
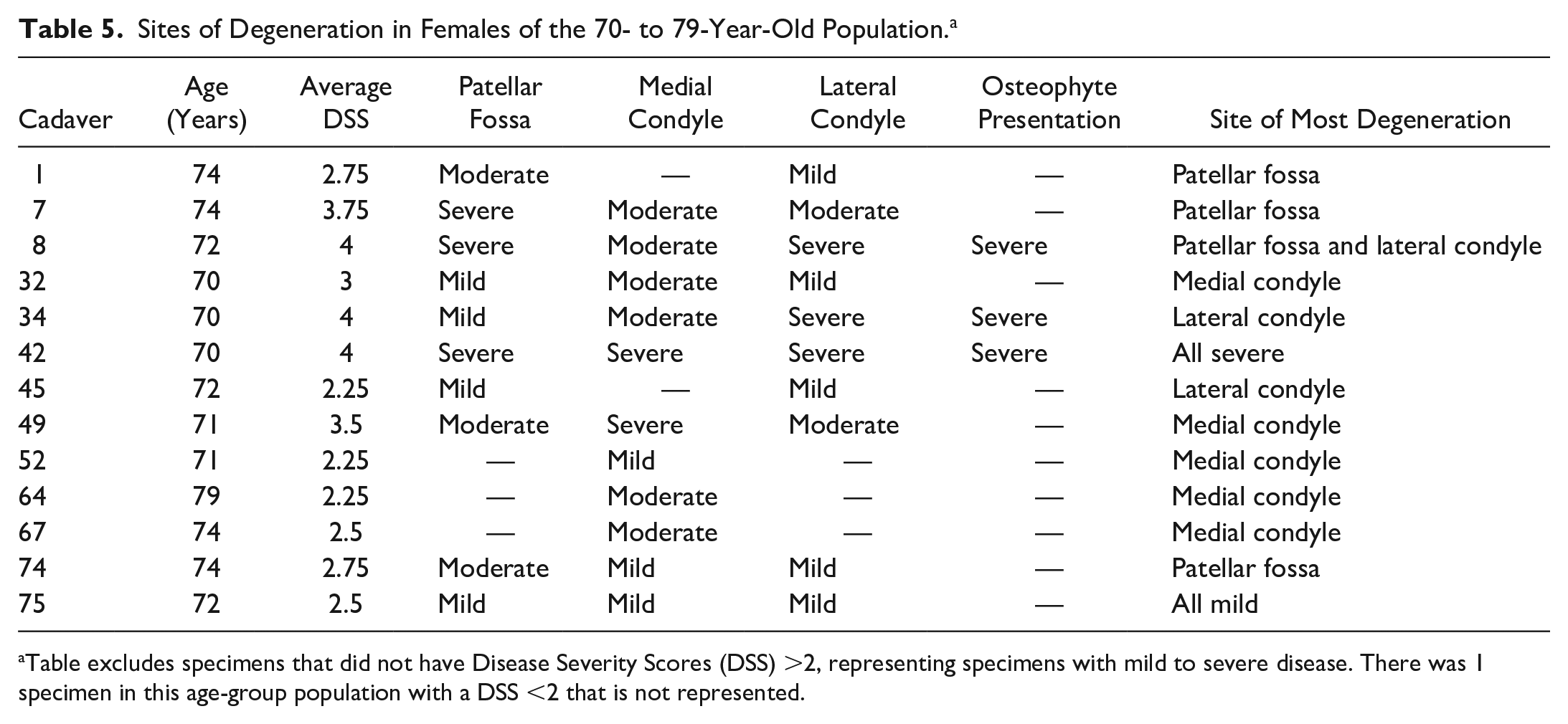
Table excludes specimens that did not have Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. There was 1 specimen in this age-group population with a DSS <2 that is not represented.
Sites of Degeneration in Males of the 70- to 79-Year Old Population.
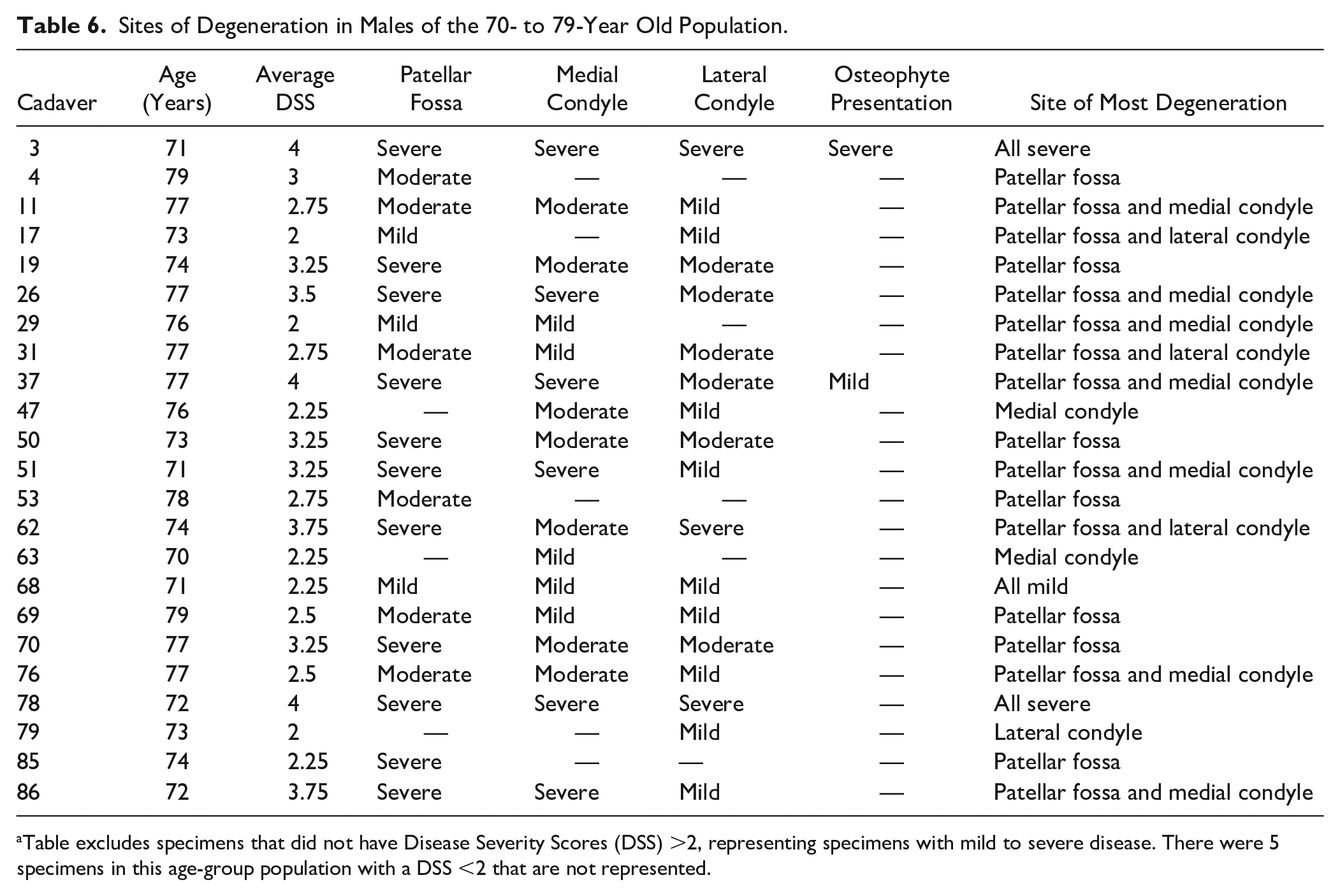
Table excludes specimens that did not have Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. There were 5 specimens in this age-group population with a DSS <2 that are not represented.
The males and females in the ≥80-year-old population displayed a 0:5 and a 2:7 ratio for “lateral femoral condyle” versus “medial femoral condyle” as a site of most severe deterioration, respectively. The female and male specimens showed more substantial degeneration on one condyle or the other. There was one exception of equivalent disease presenting on both condyles for the female population and 2 exceptions for the male population. These specimens were left out of the disease presentation ratios. All male and female knee joints in the ≥80-year-old population had notable degeneration on the patellar fossa along with the condylar cartilage. Two male specimens in the ≥80year-old population did not have a DSS >2 so there were no regions documented to have severe OA ( Tables 7 and 8 ).
Sites of Degeneration in Females of the ≥80-Year-Old Population. a
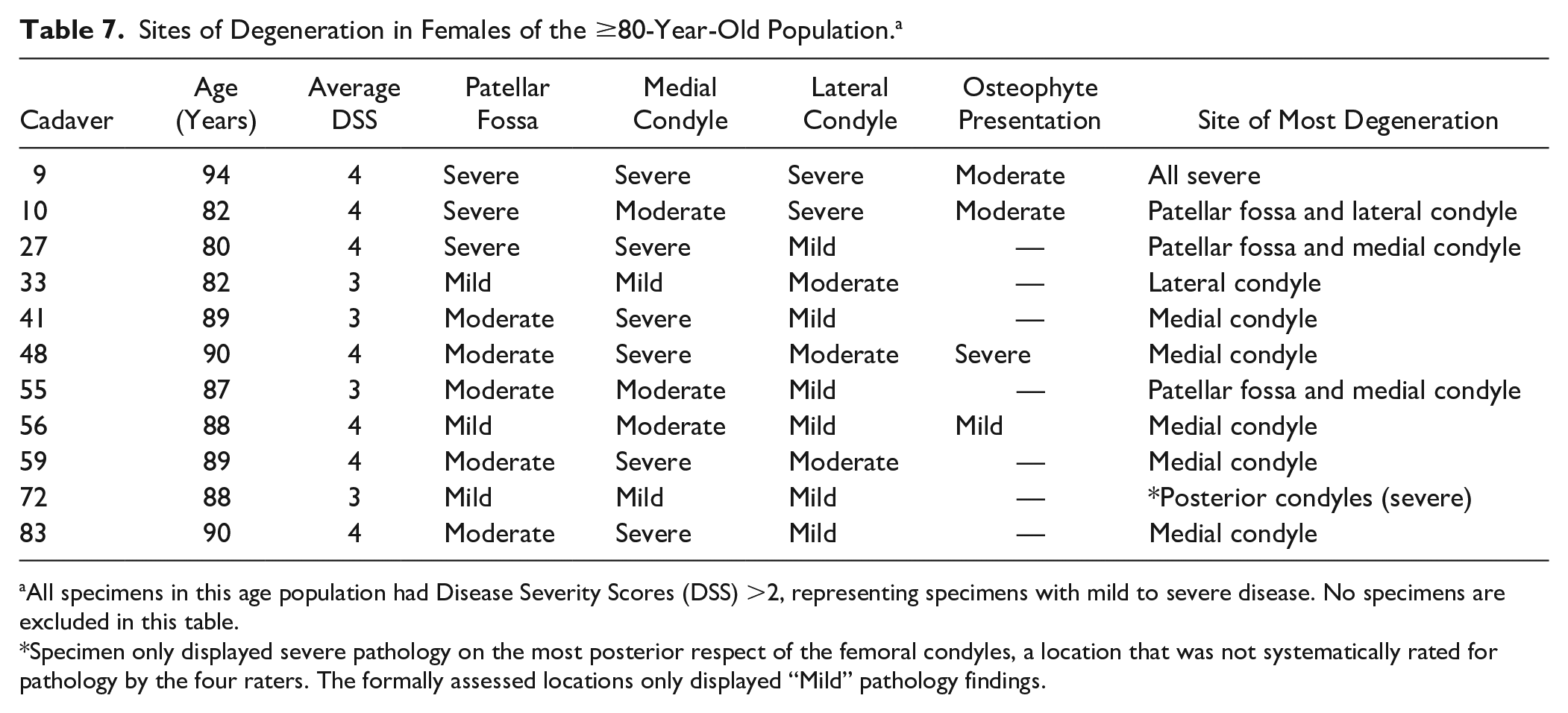
All specimens in this age population had Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. No specimens are excluded in this table.
Specimen only displayed severe pathology on the most posterior respect of the femoral condyles, a location that was not systematically rated for pathology by the four raters. The formally assessed locations only displayed “Mild” pathology findings.
Sites of Degeneration in Males of the ≥80-Year-Old Population. a
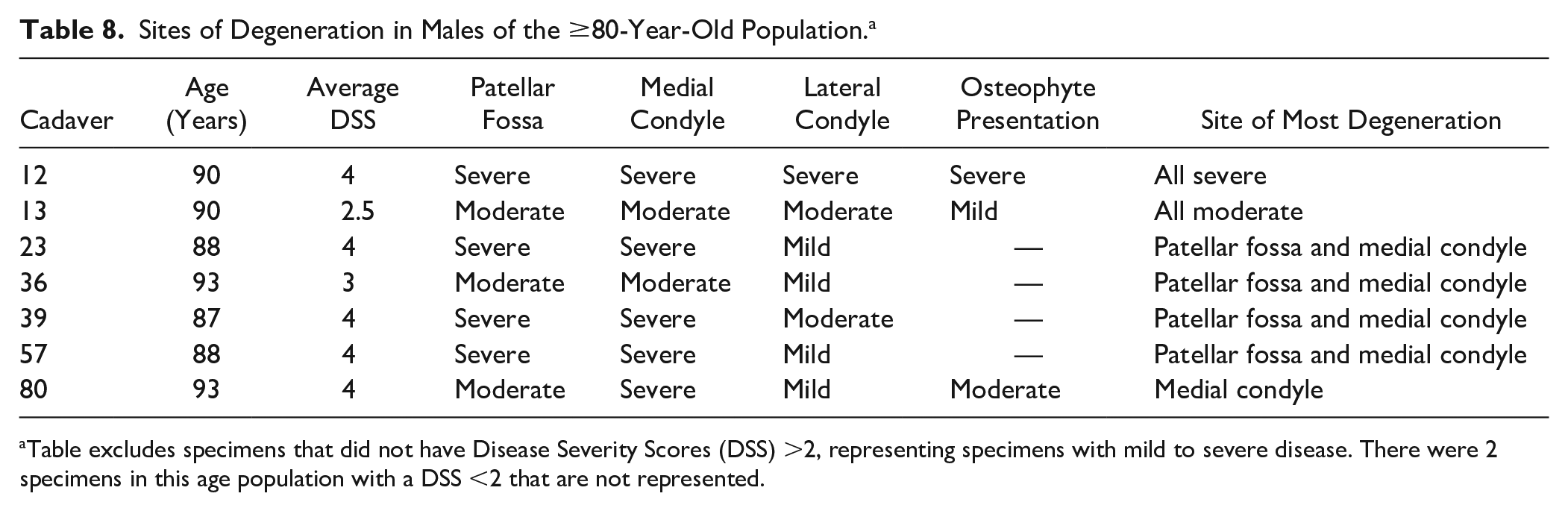
Table excludes specimens that did not have Disease Severity Scores (DSS) >2, representing specimens with mild to severe disease. There were 2 specimens in this age population with a DSS <2 that are not represented.
Discussion
Adding to previously documented data related to OA and its gross symptoms seen in cadaveric knee joints, investigators aimed to assess the femoral condyles for degeneration. 7 Degeneration of the articular cartilage and the pathogenesis of OA is stimulated by factors creating abnormal joint alignment along with previous patient trauma to the joint such as ACL reconstruction or meniscal tears. 12 Given the causes of OA, donors with previous knee joint surgeries were exempt from the study. The extent of degeneration of the articular cartilage is of interest to investigators as this degeneration represents the predominant cause for total knee arthroplasty and knee joint pain. Total knee arthroplasty is the international standard of care for the treatment of degenerative joint diseases as well as certain knee joint fractures.13-15
Currently, the leading treatment for knee OA includes exercise, weight loss and nonsteroidal anti-inflammatory drugs. When these interventions are insufficient, other therapies are implemented such as corticosteroid injections, platelet-rich plasma injections, osteotomy, or total knee arthroplasty. Fairly recently, pluripotent stem cells have materialized as a potential, alternative modality for knee OA. A systematic review on stem cell injections in knee OA patients shows that 5 randomized, controlled trials were conducted and all 5 of the documented trials reported “superior efficacy for patient-reported outcomes” compared with controls at the final follow-up visit. Superior radiological, histological and arthroscopic healing rate outcomes were reported in select trials; no adverse effects were consistently reported. 16 The study at hand represents the first assessment of the severity of cartilage degeneration on the femoral condyles with aging. As the practice of stem cell injections into arthritic joints becomes more commonplace these findings will be of interest and may aid in clinicians’ ability to inject stem cell therapy in a very localized manner for a specific demographic.
This study validated the use of an assessment scale for severity of OA in the knee joint. A scale used for assessing OA in the first carpometacarpal joints and the hip joint, 2 of the most prevalent sites for the development of OA, was modified and implemented in this cadaveric knee joint model.10,11 Investigators demonstrated interrater reliability for this scale in the knee joint model. Initially, fours raters assessed the state of disease in all of the knee joint specimen photography. These raters included a novice rater, a rater with moderate exposure to arthritic knee joints and cadaveric assessments of OA and two raters with substantial experience assessing cadaveric specimens with OA. Assessment of interrater reliability using Krippendorff’s alpha (Kα) showed the scale was not reliable (α = 0.5975) in the knee joint OA model when assessing scores from all 4 raters. According to the authors of the statistical test, if α exceeds 0.8, the interrater agreement is strong. An α less than 0.67 is considered poor interrater agreement. 17 Given the initial outcome of Kα, the assessment was ran again using only the DSS ratings from the 2 experienced raters. Running Kα with only the 2 experienced investigators’ DSS ratings achieved a strong score (α = 0.8361) indicating that the use of this scale is influenced by the familiarity and background of the rater. Implementation of the Kovler OA scale in other joints affected by OA or repetition studies in the knee joint should be carried out with this consideration. All raters involved should have experience with the assessment of diseased synovial joints, aging and variations in anatomy.
This study demonstrated statistically significant increases in severity of OA on the femoral condyles with aging by qualitative measure. This was the anticipated outcome based on previous assessments in this cadaveric model along with hallmark literature in the field of OA.3,5,7 The novel findings seen with this assessment relate to gender and location of disease. This study showed that there was no detectable, visual difference between male and female specimens within each age group with respect to the severity of degeneration and the location of the most severe degeneration. This was statistically assessed for the 70- to 79-year-old population and the ≥80-year-old population. There were only 2 female specimens in the <70-year-old population, therefore this age group warrants future investigation for gender dimorphism of pathology. Within the overall population, gender did correlate strongly with the DSS rating (τb = 0.24, P < 0.01) but there were no statistically significant differences in male and female DSS ratings within the age groups. This indicates that men and women are likely affected by the same biomechanical changes that spur on OA in their eighth decade of life (70s) and later.
Males and females in all age groups of this study uniformly displayed their most severe signs and symptoms of OA on the patellar fossa. Studies that specifically investigated patellofemoral pain and instability showed that under different positional and loading conditions, patellar malalignment was greater in OA patients compared with asymptomatic controls, being greatest in full extension.18-21 Adding to this body of work, a recent study just verified that patellofemoral OA presents with comparable malalignment that was documented in the studies assessing patellofemoral pain and instability. These findings suggest that patellofemoral pain and patellofemoral OA may exist on a disease continuum. 22 Typical malalignment is discussed to relocate the patella to a more laterally and proximally displaced position with more lateral tilt compared to asymptomatic knee joints ( Fig. 4A-D ).18-22
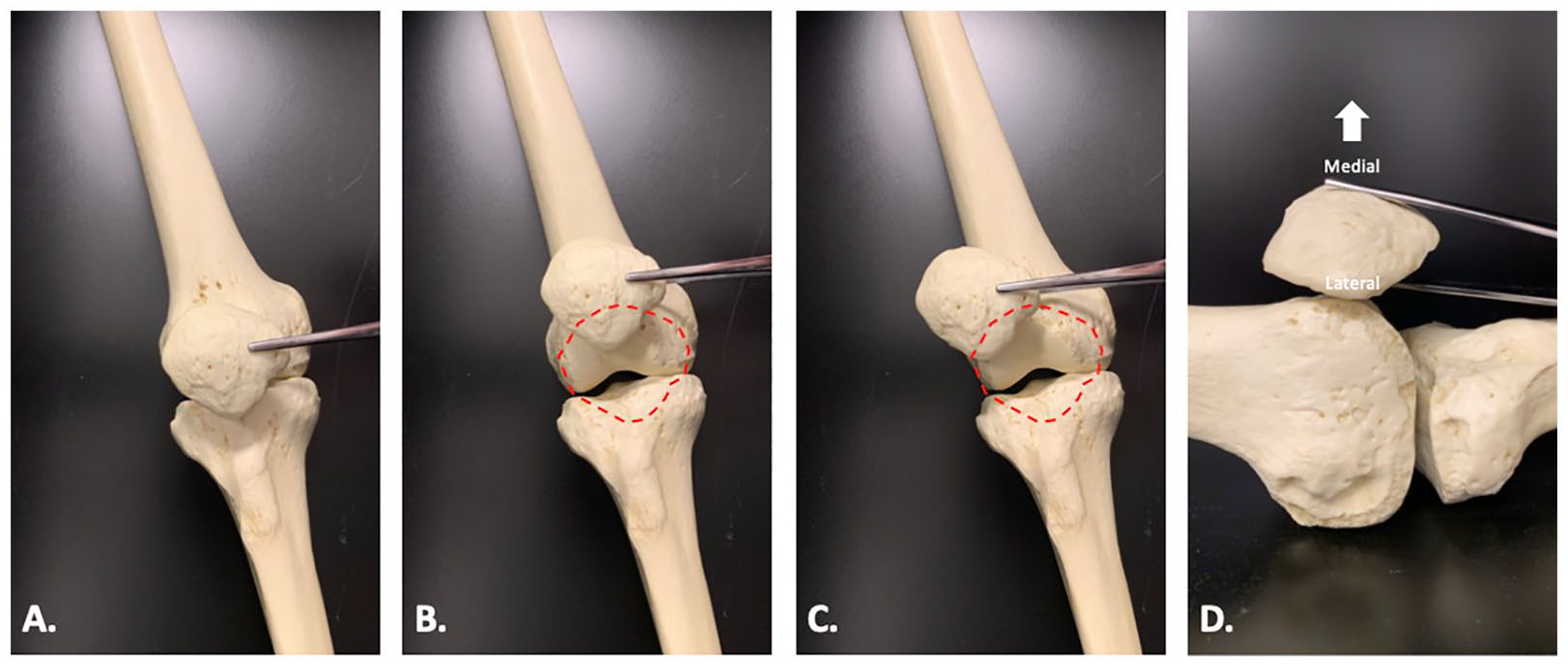
Bone Clones model of the right femur, tibia, and patella demonstrate typical malalignment of the patella with relation to the femoral condyles. (
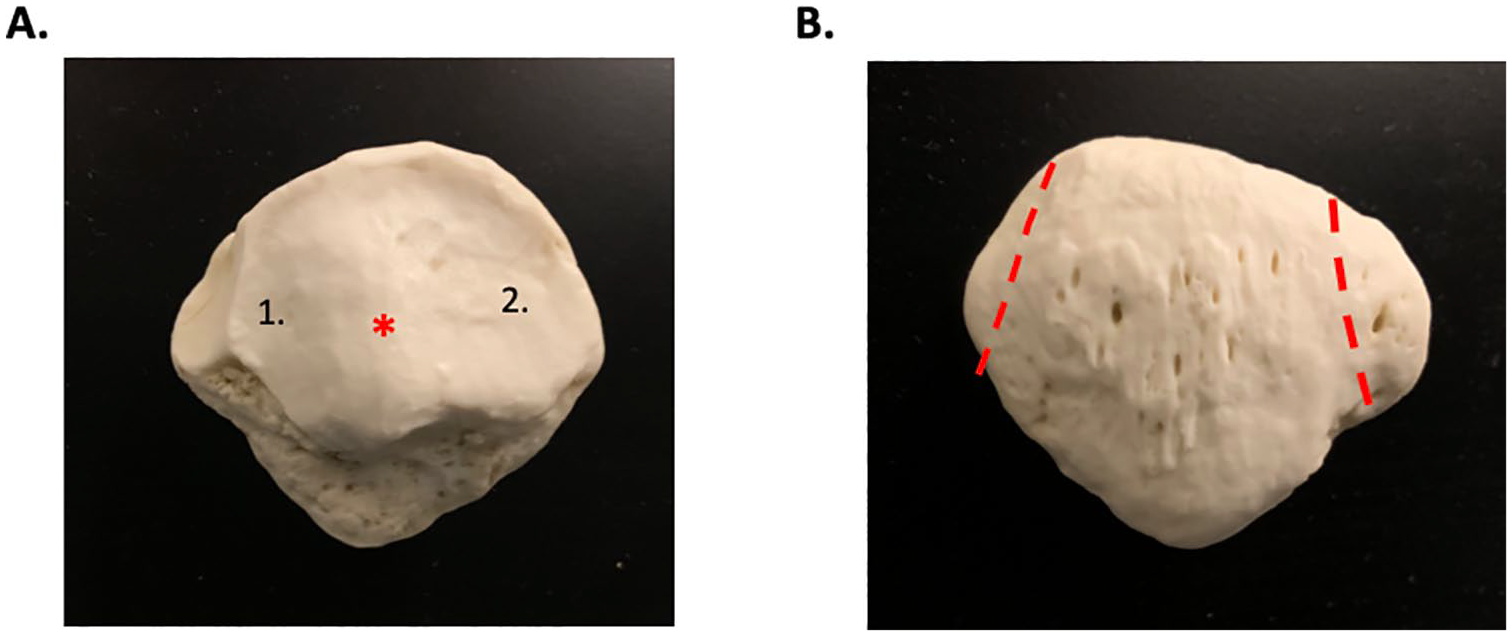
Valgus orientation at the knee joint is common with joint pathology, particularly with demanding functional tasks such as jumping. 22 It could be hypothesized that the initial valgus malalignment translates and tilts the patella with relation to the femoral condyles to change biomechanics at the patellofemoral joint. These biomechanical changes may then alter inflammatory signaling pathways in the cartilage to create early signs of OA. Valgus orientation may shift the vertical ridge of the patella, a posterior eminence of the patella that tracks in the patellar fossa of the femur, over the lateral condyle to create an abnormal site of friction ( Fig. 5A ). Unequal atrophy or hypertrophy of the vastus lateralis and the vastus medialis muscles, both forming attachments to the margins of the patella, could potentially sway the patella laterally and away from its typical site of tracking ( Fig. 5B ).
(
The second most degenerated location of condylar cartilage did not remain the same in the three age populations. The <70-year-old age group demonstrated more severe degeneration on the lateral femoral condyle whereas the 70- to 79-year-old and the ≥80-year-old age groups demonstrated more severe degeneration on the medial femoral condyle. Given that patients <70 years old had more lateral condylar cartilage degeneration compared to medial, one would expect when those patients reach 80 years of age and above, they would have lesions on both condyles. Although severity was indicated to be present on the medial condyle most regularly, all specimens in the ≥80-year-old age group demonstrated signs of OA on both condyles with the exception being the 2 male specimens with a DSS <2. Future projects aim to quantify the surface area damages on the condylar cartilage to specifically determine the percentages of loss on each condyle.
Overall, the site of severity findings suggests there are at minimum 2 mechanisms of action for developing gross, OA pathology of the condylar cartilage that are age dependent. Important to the youngest age group, over two-thirds of the American population is currently overweight or obese. 23 Obesity sways tibiofemoral compression forces to the lateral aspect of the joint and contributes to valgus orientation. Tibiofemoral compression forces are 1.6 times an individual’s body weight during isometric contraction and up to 3 times an individual’s body weight during 60° of knee flexion. 4 With an abnormal valgus orientation at the knee joint, these forces become much greater in the lateral compartment of the joint, thereby altering inflammatory signaling and exacerbating lateral cartilage erosions produced by OA. Valgus orientation at the knee joint can be due to other biomechanical, anatomical, and pathological issues beyond obesity but the prevalence of the problem in the United States suggests it would be a leading cause. 14
Specimens in the 70- to 79-year-old and the ≥80-year-old age groups typically demonstrated more severe degeneration on the medial condyle opposed to the lateral. An increase in shearing forces in the knee joint may be due to muscular atrophy accompanied by or independent of a loss of integrity to other structure supporting the joint such as the ACL. This represents a general yet, informative change in biomechanics: Younger patients often degenerate laterally until their 70s. In or around the eighth decade of life (70s), medial degeneration becomes the more predominate site of OA pathogenesis. This statement can help predict a specific patient’s OA symptom presentation by location in the aging population.
According to the U.S. Department of Health and Human Services, in 2015-2016, the prevalence of obesity among adults aged 20 to 39 years was 35.7%. Adults aged 40 to 59 years and those aged ≥60 years displayed 42.8% and 41% obesity, respectively. 24 Although by percentage the change in obesity between the 40- to 59-year-old population and the ≥60-year-old population seems minor (1.8%), it represents a transition where older individuals become less likely to experience obesity and lateral knee joint degeneration and more likely to experience medial degeneration. The same public health advisory group prepared a publication based on data from 2007-2010 that indicated that the prevalence of obesity among Americans aged 75 years and older was 27.8% which was significantly lower than the documented 40.8% of Americans who were considered obese in the 65- to 74-year-old population. The lower prevalence among Americans in the more elderly group was observed in both men and women. 25 If statistics were available to indicate the specific percentages of obesity seen in Americans in their 70s, 80s, and 90s in a more current time frame, one would expect the decreasing trend to persist and show more momentous decreases in population obesity in the later decades of life. The pathogenesis related to obesity seen in individuals in their 20s to 70 relates to decreases in total energy expenditure. Resting metabolic rate, physical activity, and hormone availability or responsiveness all decrease. 26
It has been documented that aging is associated with substantial changes in body composition. After 20 to 30 years of life, fat-free body mass progressively decreases whereas fat mass increases. Fat-free body mass, which is composed of primarily skeletal muscle, typically decreases by 40% from 20 to 70 years old. Maximum fat mass is documented to be reached somewhere between 60 and 70 years and then declines with further aging. Therefore, individuals in their eighth or ninth decade of life (70s and 80s) have experienced considerable decreases in their fat mass as well as their fat-free mass (skeletal muscle).26-30 It should be considered that the medial compartment of the knee joint bears greater than half (60%) of the tibiofemoral compression force in the knee joint during gait. 4 This fact, accompanied by a loss of fat-free mass, which are structures responsible for resisting shearing forces at the knee joint, makes the elder age groups more likely to display medial degeneration.
A limitation of this assessment exists with respect to the fact that shearing forces in the knee joint are responsible for the initiation or progression of OA in the older age populations (70-79-year-old age group and the ≥80-year-old age group). It has been documented in previous morphometric studies that the ACL grossly thins with aging.7,31 It was not determined in individual specimens if thinning of the ACL leads to shearing or if shearing participates in the mechanical stretch of the ACL. This is an important determination as corrective measures and public health advisory could be improved with this information. 31 If shearing stretches the ACL, maintenance and ideally hypertrophy of musculature supporting the joint becomes critical. If histological changes to the ACL produce stretch, then other metabolic and signaling systems needs to be investigated to reduce the propensity for patients to experience ACL degeneration. It is likely safe to say that muscular atrophy and weakened extracapsular support participates to a certain extent in both scenarios. Future directions of this study involve assessing the ACL for microalterations such as collagen fiber disorganization, cystic occurrences and calcium phosphate crystal infiltration to determine if histological pathology is present and leading to chondral degeneration.
This is the first experiment in this cadaveric program of morphometric analysis of gross signs of OA in the knee joint that has implemented qualitative assessment. Previous assessments of chondral lesions in the knee joint were carried out on the tibial plateau. Due to the lack of contour on the tibial plateau compared to the femoral condyles a quantified assessment of surface area degeneration of the articular cartilage was carried out. It appears that the qualitative data collected in this experiment correspondences with the quantitative, aging data collected on the ACL, medial meniscus, and tibial plateau cartilage. 7 The qualitative scale used in this study carries face validity based on its use in other studies. Interrater reliability was also statistically shown for the first time. These facts should justify the use of the technique and the legitimacy of the findings, countering the view that qualitative assessment limits the strength of the results.
Conclusion
As anticipated, the DSS ratings increased with aging and were statistically higher in females when assessing the overall population. The novel findings in this study were unveiled when specimens within the specific age populations were analyzed by sex. There were no statistical differences seen the male and female DSS rankings when assessing the specimens within the 70- to 79-year-old population and the ≥80-year-old population. There were also no differences found between the sexes in the aging populations regarding the sites of most severe femoral degeneration. This indicates that men and women are likely affected by the same biomechanical changes that spur on OA in their eighth decade of life and later.
This study showed that younger patients often experience lateral cartilage degeneration until their 70s; once a patient reaches their 70s, medial degeneration become the more predominate site of pathogenesis. These findings can help predict a patient’s OA symptom presentation by location in the aging population and may lead to improved treatment. It is recommended that public health advisory committees target OA patients by 3 age groups while indicating where the transition from obesity-related OA to atrophy-related OA exists. The Centers for Disease Control and Prevention should provide individualized information on OA and preventative measures to young adults (20s, 30s, and 40s), those in their later adult years (50s and 60s) and the elderly (70s, 80s, 90s, and 100s). Young adults will benefit greatly as they are in a physiological position to increase skeletal muscle and prevent future shearing at the joint whereas older populations have already experienced the initiation of disease. Physical therapy and orthopedic specialists are best prepared to make clinical advisement to the older patient populations but moving forward into the next millennia these patients and their propensity to develop OA in the knee joint should be considered 40 years sooner.
Supplemental Material
Submission_Cover_Letter_Femoral_Condyles_Manuscript_Revisions_2020 – Supplemental material for Assessment of the Degree of Osteoarthritis in Aging Male and Female Femoral Condyles: A Cadaveric Study
Supplemental material, Submission_Cover_Letter_Femoral_Condyles_Manuscript_Revisions_2020 for Assessment of the Degree of Osteoarthritis in Aging Male and Female Femoral Condyles: A Cadaveric Study by Jessica Immonen, Kelsey Stevens, Alexa Albin, David Chaus, Lesley Gilmer and Matthew Zdilla in CARTILAGE
Footnotes
Authors’ Note
This work was completed at Rocky Mountain University of Health Professions in Provo, UT and the University of Utah in Salt Lake City, UT.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by internal grants from Rocky Mountain University of Health Professions’ Office of Sponsored Projects and Research and the University of Utah School of Medicine’s Department of Anatomy and Neurobiology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This project (Protocol 150430-04) was reviewed and approved by Rocky Mountain University of Health Profession’s Institutional Review Board in Provo, UT. This project was determined to be research not involving human subjects.
Informed Consent
Not applicable.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.