
Abstract
Objective
There are limited data on bone dimension and cartilage thickness of the distal humeral articular surface. This study aimed to evaluate sex- and age-related bone dimension and cartilage thickness differences and assess the effect of cartilage thickness on distal humeral shape.
Design
Elbow magnetic resonance images of 180 healthy participants were evaluated. Cartilage thicknesses of the trochlea and capitellum were measured at 19 points using coronal and axial images. In addition, bone diameters were measured from the flexion-extension axis to the 19 points on the coronal and axial magnetic resonance images. Sex differences were evaluated, and the correlation between age and measurement parameters was assessed.
Results
Significant sex differences regarding the diameters of the axial trochlear bone, coronal lateral trochlear bone, and medial capitellar bone, cartilage thickness at the apex of the lateral trochlear ridge in the axial and coronal plane and at the most lateral point of the capitellar articular surface in the axial plane were observed. A negative correlation was observed between age and axial plane trochlear bone dimensions and between age and coronal plane lateral trochlear and medial capitellar bone dimensions. No significant correlation was found between cartilage thickness and bone dimensions.
Conclusions
Bone dimension and cartilage thickness at the distal humerus vary according to sex and age. The data could be used in the donor site selection and graft preparation while osteochondral autograft transfer and allograft transplantation, and in the development of gender-compatible hemiarthroplasty implants.
Introduction
Disorders affecting the elbow joint can cause severe activity limitations. 1 Additionally, aging, traumatic events, and sports injuries may cause disability by affecting proper functioning of the joint cartilage and bone.2-4 Although the elbow joint is a complex structure and comprehensive knowledge of normal elbow anatomy is important in evaluating disorders and planning treatment, 5 the anatomic dimensions of the distal humerus have been investigated relatively less.6-10 Of the studies that have researched distal humeral anatomy, few have investigated relative cartilage distribution and demographic differences. In addition, most of them utilized direct radiographs or computed tomography (CT) images. There are few magnetic resonance imaging (MRI) studies that have considered distal humeral bone and cartilage morphology together. To our knowledge, only one study evaluated the extent of the cartilage layer along the distal humerus, including trochlea and capitellum joint surfaces with the effect of different articular surface dimensions on the shape of the distal humeral bone. 11 This study had a population age range between 21 and 32 years. To the best of our knowledge, no study has investigated the distal humeral cartilage and bone dimensions in a population with a wide age range. Therefore, the aims of this study were (1) to investigate the comprehensive cartilage and bone thickness of the distal humerus, (2) to assess the variations of bone dimension and the articular cartilage according to sex and age, and (3) to investigate the effect of cartilage layer on the distal humeral shape. It was hypothesized that cartilage thickness varies on the distal humeral articular surface according to age, sex, and anatomic location and that it affects the distal humerus morphology.
Methods
Magnetic Resonance Imaging and Software Utilization
To comprehensively evaluate the distal humeral bone diameter and cartilage thickness, MRI of 180 skeletally mature patients, 90 women and 90 men, were conducted. Participants’ ages ranged from 18 to 79 years with a mean age of 45.2 ± 18.3 years. Patients with a history of elbow disorder or any other disorder that might affect the elbow joint (previous ipsilateral upper extremity surgery, inflammatory arthritis, upper extremity deformity, or neurologic impairment) were excluded. Elbow radiographs of all patients were evaluated before MRI. High-definition magnetic resonance images (2 mm thickness) were obtained with a 1.5-T high-field scanner (Magnetom Symphony, Siemens AG, Erlangen, Germany) using an 8-channel knee-dedicated coil, positioned with the elbow in full extension and the forearm in full supination. Coronal, sagittal, and axial planes were determined by 3D Slicer software (v 4.10.0; Brigham and Women’s Hospital, Boston, MA, USA). Cartilage thickness and bone diameter measurements were collected using INFINITT PACS System (Infinitt Healthcare Co., Seoul, South Korea) with an accuracy of 0.01 mm.
Bone and Cartilage Measurement Acquisition
To assess cartilage thickness, axial cuts were used to measure the anterior and posterior articular surfaces and coronal cuts were used to measure the inferior articular surface. Bone diameter measurements were conducted on the axial and coronal cuts by measuring the perpendicular distance between the flexion-extension axis and 19 previously determined points on the articular surface.
In the coronal plane, 8 points (a to h) ( Fig. 1 ) were identified as (a) the apex of the trochlear medial ridge, (b) the midpoint between the trochlear medial ridge and the trochlear groove, (c) the deepest point of the trochlear groove, (d) the midpoint between the trochlear groove and the lateral ridge, (e) the apex of the trochlear lateral ridge, (f) the deepest point of the trochleo-capitellar groove, (g) the point of greatest convexity of the capitellum, and (h) the most lateral point of the capitellar articular surface. The midpoint between the trochlear medial ridge and the trochlear groove was defined as the point that lies halfway between 2 parallel lines that were perpendicular to the flexion-extension axis and that transect the medial ridge and trochlear groove (TG), respectively. The midpoint between the TG and lateral ridge was defined as the point that lies halfway between 2 parallel lines that were perpendicular to the flexion-extension axis and that transect the TG and lateral ridge, respectively.
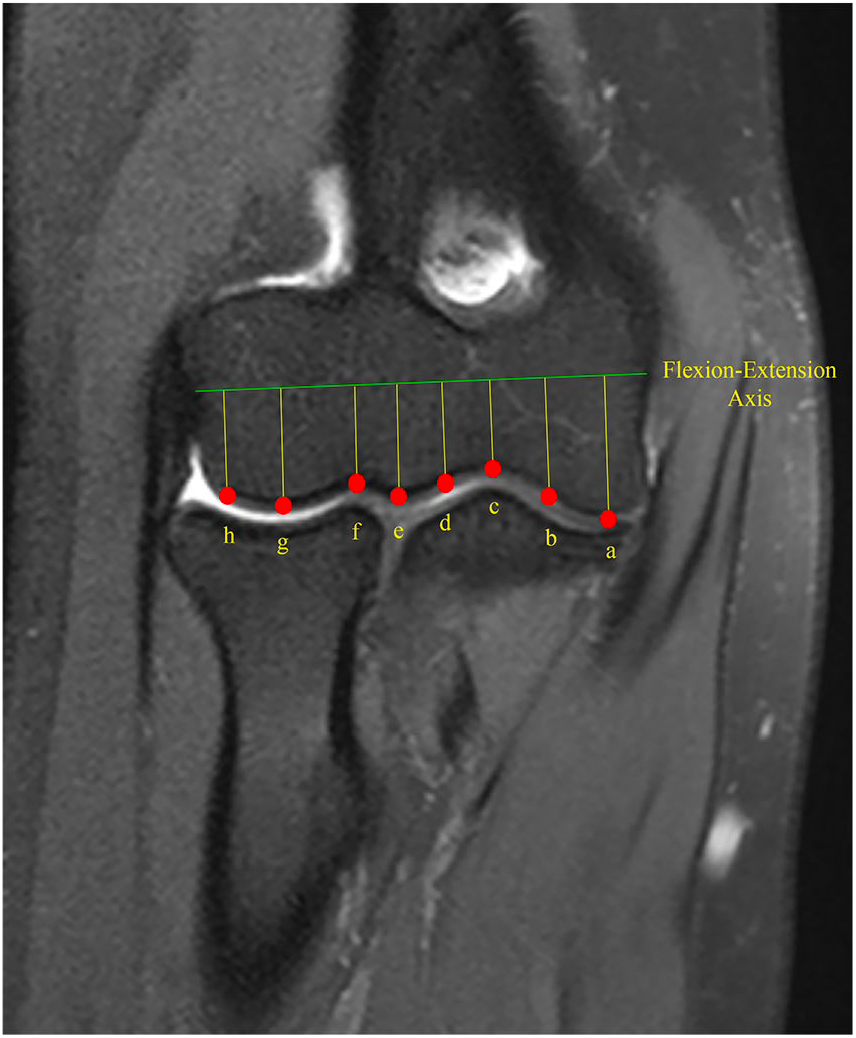
Determined points for the measurement of cartilage thickness and bone diameters on the joint face in the coronal image.
In the axial plane, 11 points (A to K) ( Fig. 2 ) were defined as (A) the apex of the trochlear medial ridge, (B) the midpoint between the trochlear medial ridge and the trochlear groove, (C) the deepest point of the trochlear groove, (D) the midpoint between the trochlear groove and the lateral ridge, (E) the apex of the trochlear lateral ridge, (F) the deepest point of the trochleo-capitellar groove, (G) the point of greatest convexity of the capitellum, (H) the most lateral point of the capitellar articular surface, (I) the posterior trochlear groove, (J) the level of the posterior trochlear lateral ridge, and (K) the level of the posterior trochlear medial ridge.
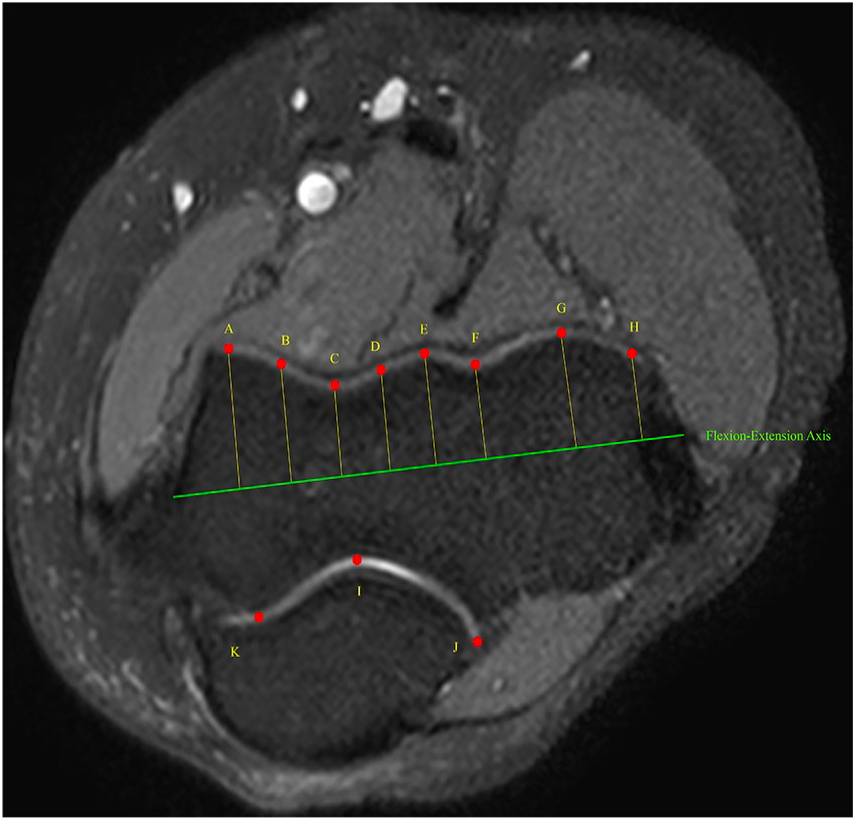
Determined points for the measurement of cartilage thickness and bone diameters on the joint face in the axial image.
In the axial and coronal plane, the width of the distal humeral articular surface was measured via the distance between 2 lines of the most lateral and most medial points of the articular surface perpendicular to the flexion-extension axis ( Fig. 3 ). As an indirect measurement of humerus length, patient height was used. These measurements were performed by 2 blinded observers, once each, 4 weeks apart. The order of magnetic resonance images was randomized for the 2 observers at both the first and second evaluation sessions.
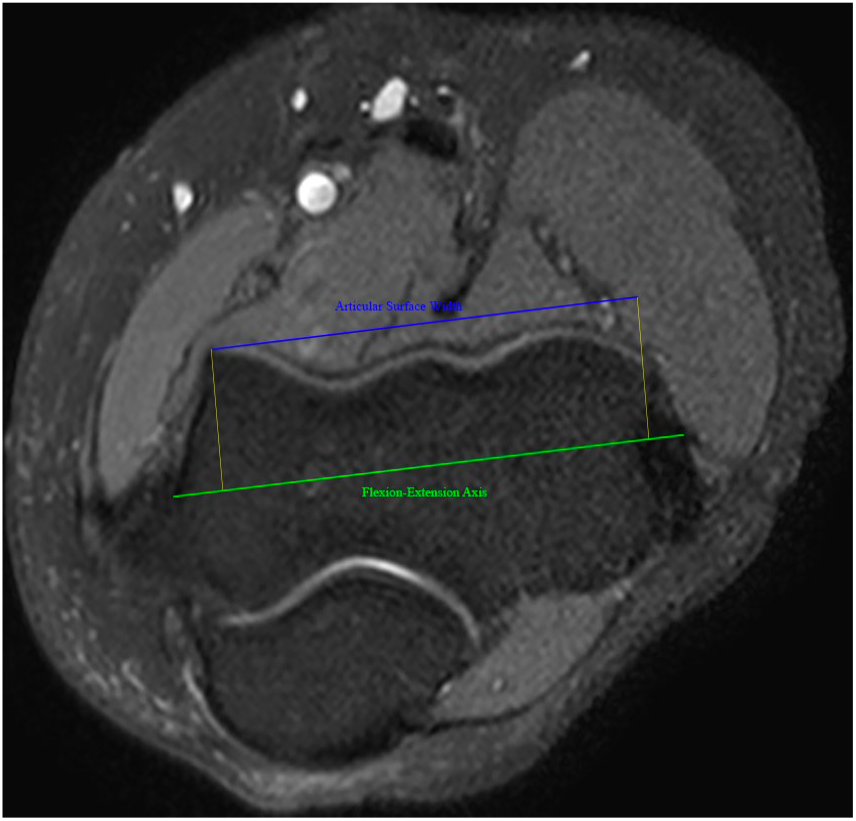
Articular surface width measurement method in the axial and coronal images.
Statistical Analysis
The mean, standard deviation, median, lowest and highest values, frequency, and ratios were determined for descriptive statistics. The distribution of measurements was evaluated using the Kolmogorov-Smirnov test. The Mann-Whitney U test and independent-sample t test were used to analyze independent quantitative data. The Pearson correlation test was used to evaluate the relationship between measurement parameters and age. An intraclass correlation coefficient was used to evaluate the correlation between individual measurements. A P value <0.05 was considered statistically significant. SPSS V22 software (IBM Corp., Armonk, NY, USA) was used to conduct statistical analyses.
Results
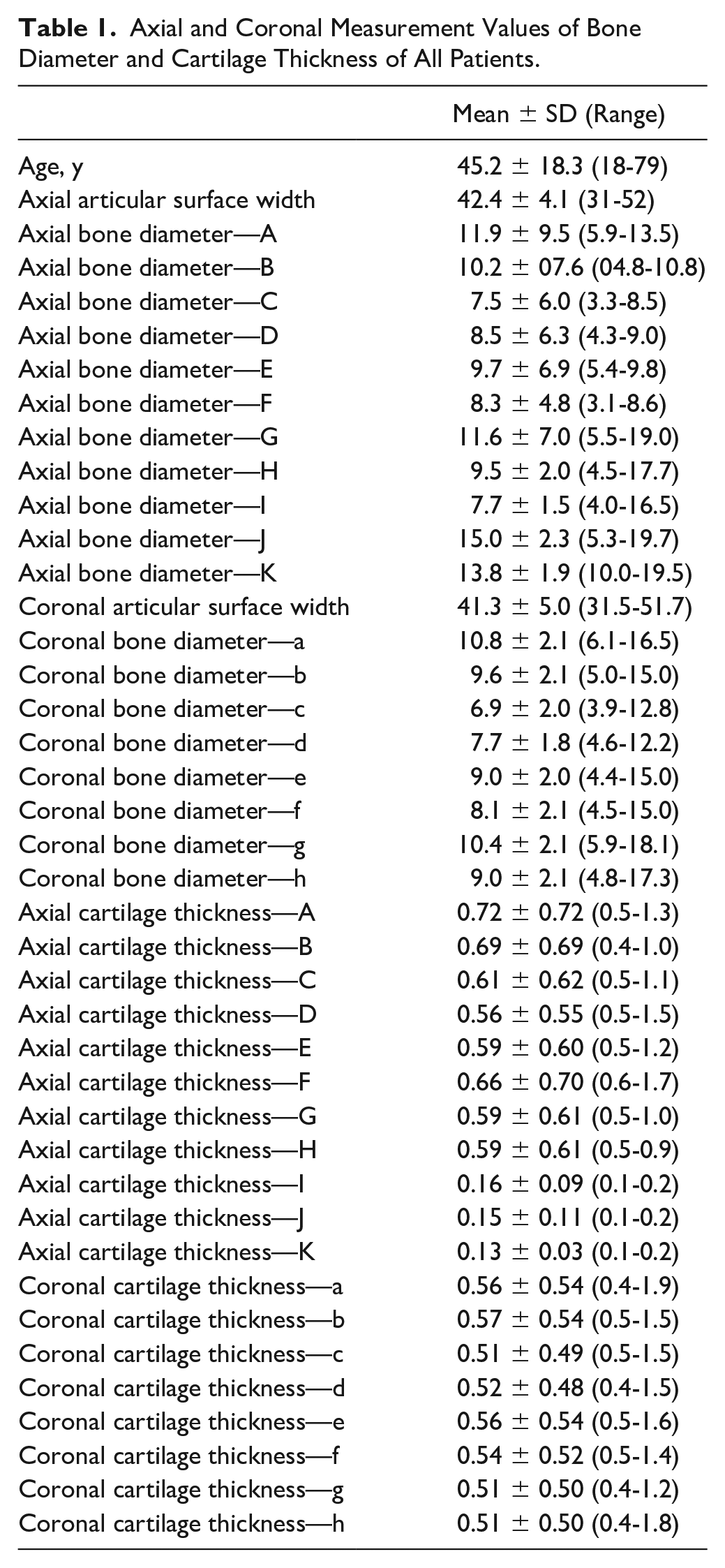
The descriptive statistics of all patients are summarized in Table 1. The mean patient height was 171.8 ± 23.7 cm (range 154-192 cm). No significant correlation was found between patient height and axial or coronal cartilage thicknesses (P > 0.05). There was no significant side difference regarding any measurement parameters (P > 0.05). There was a significant difference in axial (articular surface width, bone diameters A, B, D, E, G, H, I, J, and K) and coronal (articular surface width, coronal bone diameters a, g, and h) measurements between male and female patients. In addition, there was a significant difference in chondral thickness at axial points E and H and at the coronal point e between male and female patients ( Table 2 ; Figs. 4 and 5 ).
Axial and Coronal Measurement Values of Bone Diameter and Cartilage Thickness of All Patients.
Bone and Cartilage Measurement Parameters According to Sex.
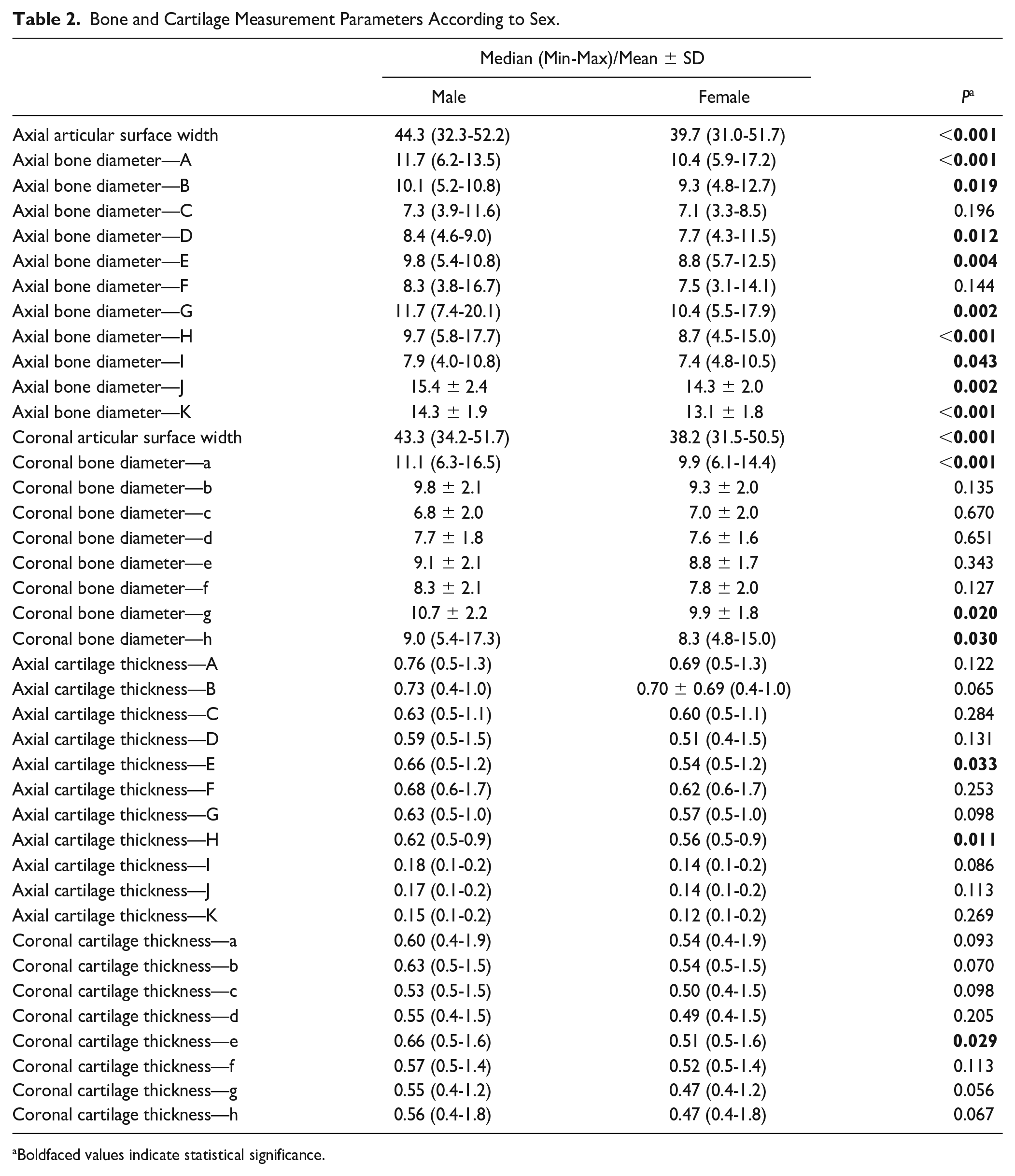
Boldfaced values indicate statistical significance.
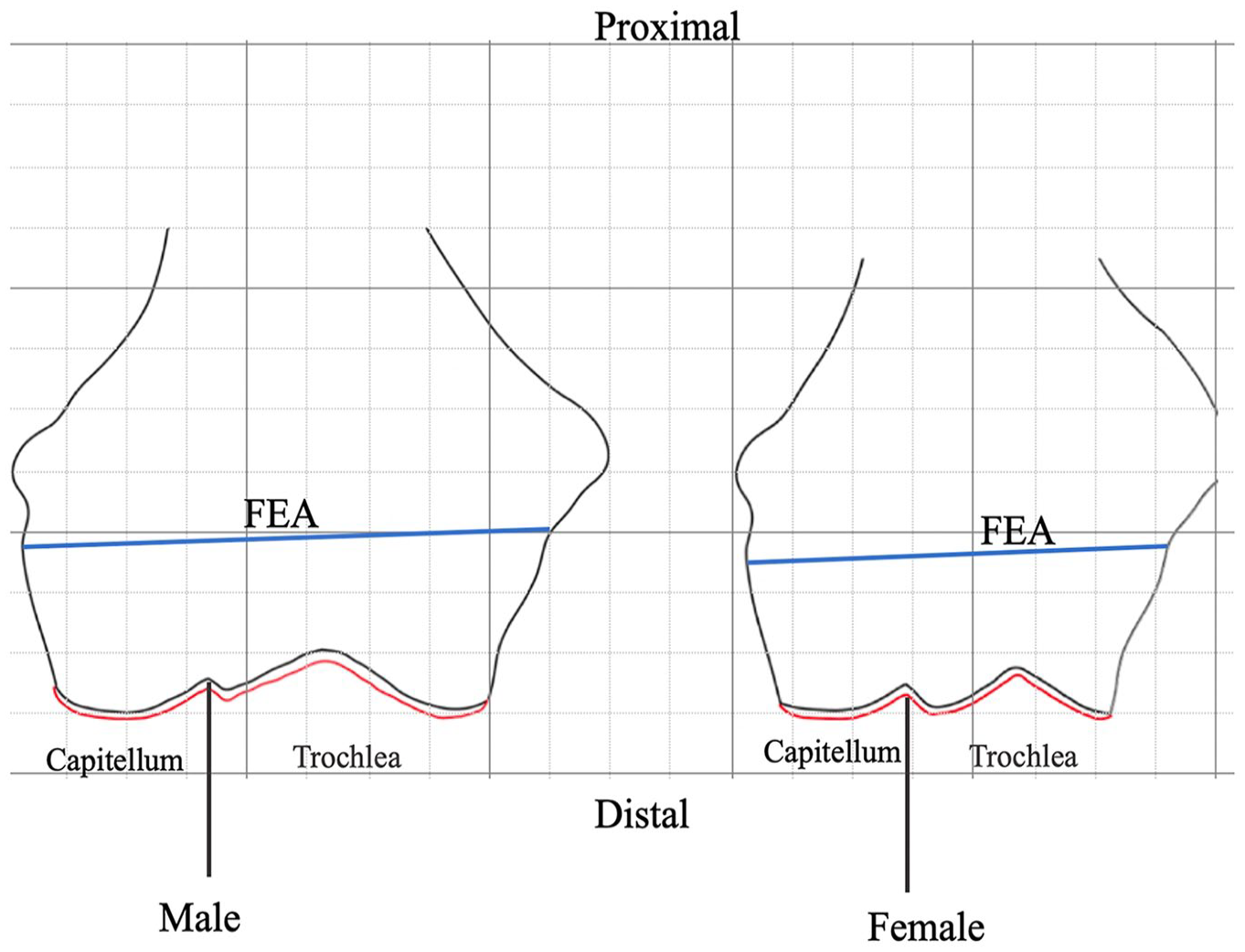
Visual representation of coronal bone diameter and cartilage thickness differences in male and female participants. The black line indicates borders of bone and the red line indicates borders of cartilage. FEA = flexion-extension axis.
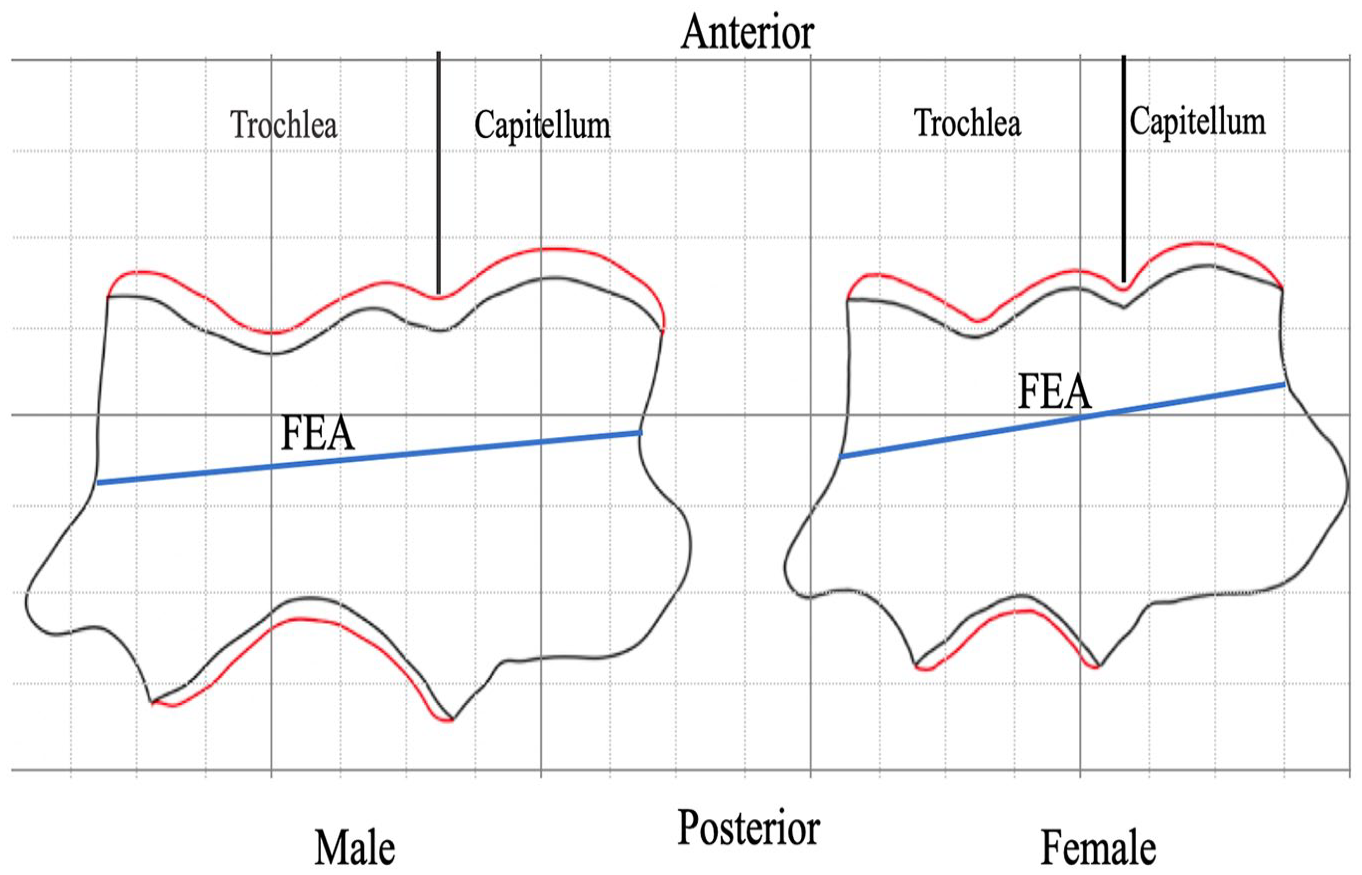
Visual representation of axial bone diameter and cartilage thickness differences in male and female participants. The black line indicates borders of bone and the red line indicates borders of cartilage. FEA = flexion-extension axis.
A negative correlation was observed between age and both axial (points B, C, D, E, and F) and coronal (points d, e, f, and g) bone diameter. Additionally, a weak positive correlation was observed between age and both axial (point D) and coronal (points a, e, and g) cartilage thickness ( Table 3 ).
Correlation Table Regarding Age and Measurement Parameters. a .
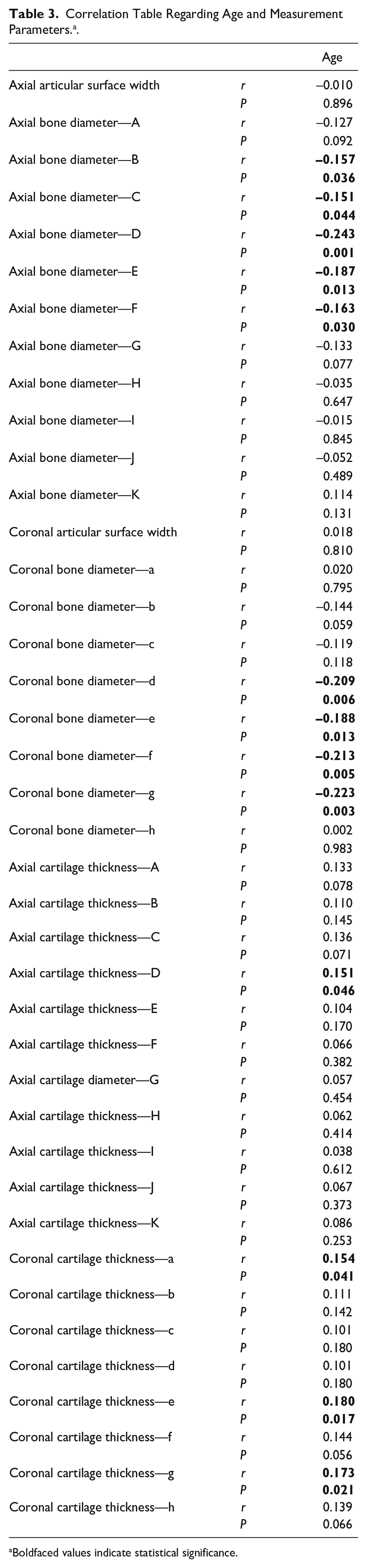
Boldfaced values indicate statistical significance.
A positive correlation was observed in axial and coronal cartilage measurement parameters, with the exception of posterior trochlear cartilage thicknesses and coronal cartilage thicknesses (
Table 4
). However, there was no correlation in the majority of axial and coronal bone thickness parameters (
Table 5
). According to correlation analysis, a positive correlation was detected between 3 contiguous points in the axial and coronal planes. Correlation was weakened with increasing distance between points (
Tables 4
and
Correlation Table Regarding Axial and Coronal Cartilage Thickness Values. a .
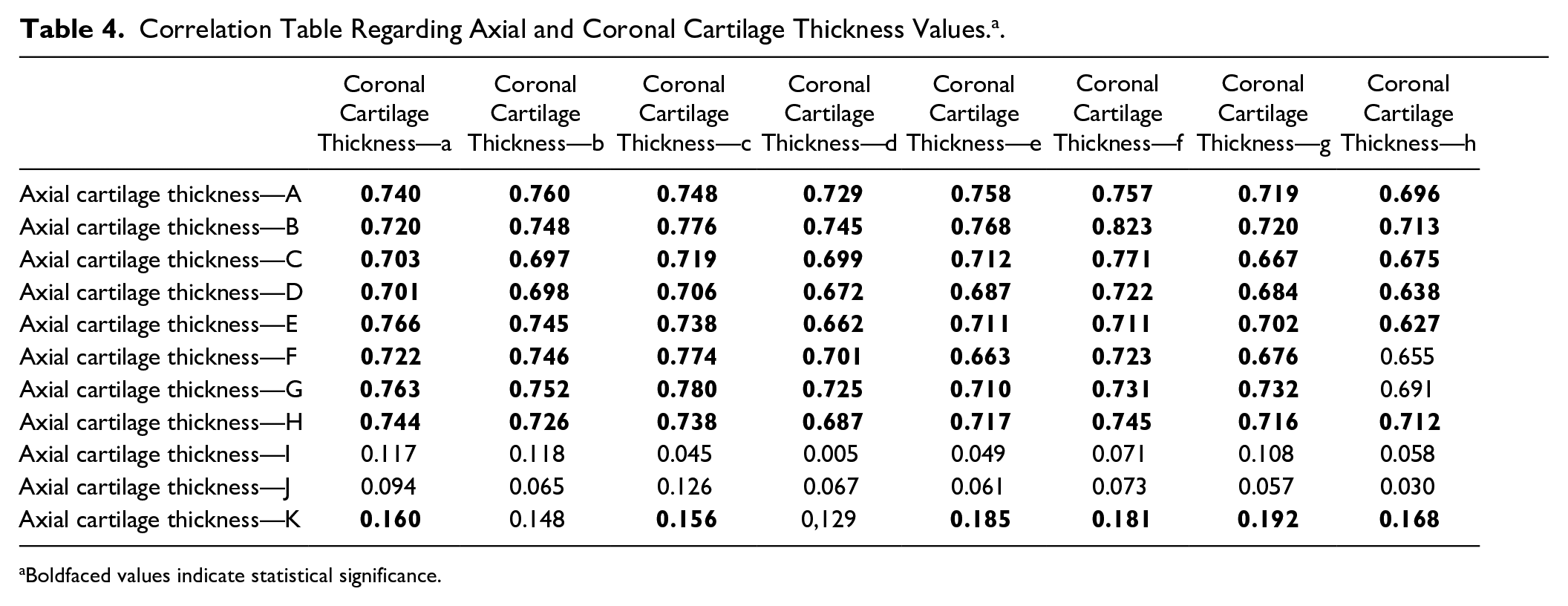
Boldfaced values indicate statistical significance.
Correlation Table Regarding Axial and Coronal Bone Diameter and Articular Surface Width Values. a .
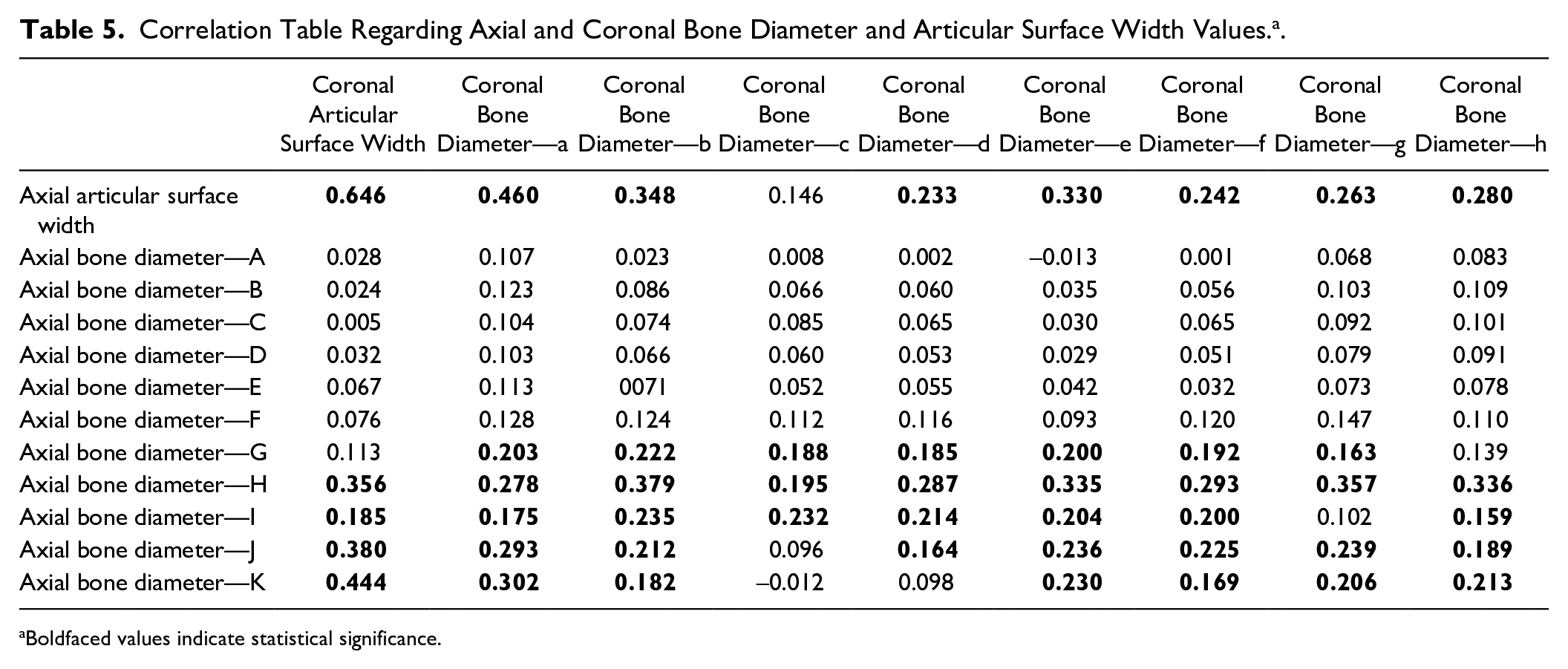
Boldfaced values indicate statistical significance.
Discussion
The most important findings of this study are that there were significant differences in axial trochlear, coronal lateral trochlear, and medial capitellar bone diameters between sexes. In addition, a significant difference was observed between sexes regarding cartilage thickness at the apex of the lateral trochlear ridge in the axial and coronal plane and at the most lateral point of the capitellar articular surface in the axial plane. A negative correlation was observed between age and axial plane trochlear bone diameters and between age and coronal plane lateral trochlear and medial capitellar bone diameters. A weak positive correlation was found between age and lateral trochlea and between age and the medial, central, and lateral most distal joint surfaces cartilage thicknesses. According to these results, the distal humeral cartilage and bone thickness do not show a uniform distribution. Age and sex affect distal humeral cartilage and bone anatomy.
In previous studies, anatomy of the distal humerus was evaluated using CT and MRI. Sabo et al. 9 and Desai et al. 6 examined cadaveric elbows using CT. Their findings demonstrated the flexion-extension axis, mean trochlear and capitellar width, and height. Graichen et al. 8 evaluated cadaveric distal humeri by 3-dimensional MRI. With their images, they measured volume and thickness of the distal humeral articular cartilage. They reported a mean cartilage thickness of 1.35 mm. To assess cartilage depth in osteochondral autografting donor and recipient sites, Schub et al. 10 evaluated distal femur and distal humerus cartilage thicknesses using MRI. They reported mean cartilage thicknesses of 0.78 and 1.32 mm, respectively, in the center of the trochlear groove. In addition, they reported mean cartilage thicknesses of 1.49, 1.54, and 1.06 mm on the lateral third of the capitellum. The measurement values of mean cartilage thickness in the medial third of the capitellum were 1.63, 1.47, and 0.87 mm, respectively.
Giannicola et al. 11 conducted the most extensive anthropometric study of the distal humerus. They assessed axial and coronal plane cartilage thicknesses on the capitellum and trochlea with bone dimensions using high-definition MRI. They reported a significant variation in cartilage thickness (0.4-1.8 mm) independent of side and sex They also observed thinner cartilage thickness at the medial and lateral edges and thicker cartilage thickness at the center of the distal humeral articular surface. In our study, we evaluated bone dimensions and cartilage thickness of the distal humerus in healthy participants between 18 and 79 years. We observed significantly larger axial trochlear, coronal lateral trochlear, and medial capitellar bone dimensions in men. A significantly larger cartilage thickness was also detected at the apex of the lateral trochlear ridge in the axial and coronal plane and at the most lateral point of the capitellar articular surface in the axial plane in men. As one of the distinguishing features of our study, we found a negative correlation between age and axial plane trochlear, coronal plane lateral trochlear, and medial capitellar bone dimensions. Moreover, a weak positive correlation was found between age and lateral trochlear surface and between age and the most medial, central, and lateral joint surfaces of cartilage thicknesses. A wide variation in cartilage thickness (0.3-1.9 mm) was observed in both sexes and age groups.
Articular cartilage has an important effect on stress distribution on the underlying bone. 12 Cartilage thickening due to mechanical stimulation is observed in the joint regions exposed to greater load. 13 In addition, shape differences of distal humeral hemiarthroplasty implants relative to the native joint were found to be responsible for different contact mechanics. 14 We observed increased cartilage thickness values in the central areas of the joint where the joint is subjected to higher loads, particularly in men. These findings contrast those of with the study of Giannicola et al. 11 who found no significant correlation between cartilage thickness and sex.
This study has some limitations. First, our measurements were performed on 2-dimensional MRI. An automated measurement method would give more accurate and more detailed cartilage and bone thickness data. Second, posterior trochlear measurements on axial 2-dimensional MRI caused limitations in our measurements because the joint surface cannot be seen as regular as in other sections. Third, because we performed measurements on specific points of the bone, our data do not show possible significant differences in areas outside of our specified points of measurement.
Conclusion
The distribution of the distal humeral articular cartilage thickness on the articular surface of the bone varies. The central joint areas, which are more exposed to loads, have a thicker cartilage layer and peripheral areas that have less load bearing have a thinner layer of cartilage. Furthermore, there are significant sex differences regarding bone dimension and cartilage thickness in certain areas, and the distal humeral shape is affected from cartilage thickness variations.
Bone dimension and cartilage thickness at the distal humerus vary according to sex and age. The data could be used in the donor site selection and graft preparation while osteochondral autograft transfer and allograft transplantation, and in the development of gender-compatible hemiarthroplasty implants.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Kayseri City Hospital Institutional Review Board (approval date/number: 19.04.2019/25)