
Abstract
Objective
Successful clinical outcomes following cartilage restoration procedures are highly dependent on addressing concomitant pathology. The purpose of this study was to document methods for evaluating concomitant procedures of the knee when performed with articular cartilage restoration techniques, and to review their reported findings in high-impact clinical orthopedic studies. We hypothesized that there are substantial inconsistencies in reporting clinical outcomes associated with concomitant procedures relative to outcomes related to isolated cartilage repair.
Design
A total of 133 clinical studies on articular cartilage repair of the knee were identified from 6 high-impact orthopedic journals between 2011 and 2017. Studies were included if they were primary research articles reporting clinical outcomes data following surgical treatment of articular cartilage lesions with a minimum sample size of 5 patients. Studies were excluded if they were review articles, meta-analyses, and articles reporting only nonclinical outcomes (e.g., imaging, histology). A full-text review was then used to evaluate details regarding study methodology and reporting on the following variables: primary cartilage repair procedure, and the utilization of concomitant procedures to address additional patient comorbidities, including malalignment, meniscus pathology, and ligamentous instability. Each study was additionally reviewed to document variation in clinical outcomes reporting in patients that had these comorbidities addressed at the time of surgery.
Results
All studies reported on the type of primary cartilage repair procedure, with autologous chondrocyte implantation (ACI) noted in 43% of studies, microfracture (MF) reported in 16.5%, osteochondral allograft (OCA) in 15%, and osteochondral autograft transplant (OAT) in 8.2%. Regarding concomitant pathology, anterior cruciate ligament (ACL) reconstruction (24.8%) and meniscus repair (23.3%) were the most commonly addressed patient comorbidities. A total of 56 studies (42.1%) excluded patients with malalignment, meniscus injury, and ligamentous instability. For studies that addressed concomitant pathology, 72.7% reported clinical outcomes separately from the cohort treated with only cartilage repair. A total of 16.5% of studies neither excluded nor addressed concomitant pathologies. There was a significant amount of variation in the patient reported outcome scores used among the studies, with the majority of studies reporting International Knee Documentation Committee (IKDC) and Knee Injury and Osteoarthritis Outcomes Score (KOOS) in 47.2% and 43.6% of articles, respectively.
Conclusions
In this study on knee cartilage restoration, recognition and management of concomitant pathology is inadequately reported in approximately 28% of studies. Only 30% of articles reported adequate treatment of concomitant ailments while scoring their outcomes using one of a potential 18 different scoring systems. These findings highlight the need for more standardized methods to be applied in future research with regard to inclusion, exclusion, and scoring concomitant pathologies with regard to treatment of cartilage defects in the knee.
Introduction
Articular cartilage lesions of the knee are exceedingly common; occurring in both athlete and general populations across all genders.1-3 Management has evolved dramatically since cartilage restoration surfaced more than 25 years ago.4-6 As such, primary articular cartilage restoration employs a variety of procedures that include the cartilage restoration procedures themselves and the associated procedures to address comorbidities.4-6 Unfortunately, significant variation has developed and has been noted within primary cartilage restoration literature. 7 In the knee specifically, articular cartilage lesion measurements (size and depth), grade, classification (International Cartilage Repair Society [ICRS] vs. Outerbridge), and morphology (chondral vs. osteochondral) are all highly variable with regard to reporting lesion characteristics. 7 Such variations in reporting falsely directs advancements, making standardization of reporting necessary moving forward. 7
Currently, it remains standard of care that articular cartilage restoration procedures such as microfracture (MF), autologous chondrocyte implantation (ACI), osteochondral allograft (OCA), and osteochondral autograft transfer (OATs) are conducted while also repairing other ailments of the knee joint.8-14 These comorbidities include ligament instability, malalignment in varus or valgus, and meniscal injury.10-14 Unfortunately, some inadequacies with regard to reporting of these concomitant procedures have been suggested, however, they have not been well studied. 7
The purpose of this study was to document methods for evaluating concomitant procedures of the knee when performed with articular cartilage restoration techniques, and to review their reported findings in high-impact clinical orthopedic studies. We hypothesize that there will be great variation in scoring and reporting concomitant procedures of the knee joint. Our goal is to increase awareness to establish a more consistent process for scoring and reporting concomitant procedures in future publications from high-impact journals.
Materials and Methods
This study was modeled after the original works by Jones et al., 7 recently published in Cartilage. Six high-impact orthopedic journals were selected to obtain studies of interest: (1) American Journal of Sports Medicine, (2) Journal of Bone & Joint Surgery—American Volume, (3) Knee Surgery, Sports Traumatology, and Arthroscopy, (4) Clinical Orthopaedics and Related Research, (5) Arthroscopy, and (6) Cartilage. Studies published between January 2011 and December 2017, were identified and reviewed to document reporting clinical outcomes for treatment of articular cartilage defects of the knee. Inclusion criteria were primary research articles reporting clinical outcomes data following surgical treatment of articular cartilage lesions with a minimum sample size of 5 patients. Review articles, meta-analyses, and articles reporting only nonclinical outcomes (e.g., imaging, histology) were excluded. 7
Two computerized databases (PubMed, EMBASE) with a comprehensive index of each of the six journals were searched to identify relevant primary clinical studies. 7 “Cartilage” or “chondral” was searched with the phrases [“knee”] and [“outcomes”] as well as relevant iterations. 7 All articles were screened initially by title and abstract to exclude irrelevant studies. 7 Two researchers independently performed full-text review of the remaining studies to determine eligibility for inclusion. 7 Discrepancies between reviewers were resolved through consensus with the senior authors. 7
While our previous work focused on assessing the reporting with regard to the cartilage lesion characteristics (size, depth, location, and grade with corresponding classification system, lesion morphology), 7 this study focused on assessing the reporting with regard to concomitant procedures, or their independent scoring/reporting if not excluded. For each article, the exclusion criteria noted in the “Methods” section was analyzed to assess whether or not individual studies included patients that had concomitant pathology, and if those pathologies were corrected by the time of the primary cartilage restoration procedure. Various grading/classification systems for ligamentous instability, malalignment, and meniscal injury were also noted to help identify concomitant conditions and their independent scoring/reporting when discussed. All scoring systems listed in the articles were analyzed to determine which were most utilized, and to illustrate the degree of variation amongst article scoring/reporting with respect to these systems. Only scoring systems noting outcome measures with respect to concomitant ailments noted above were included.
Results
Reporting of Characteristics for Primary Articular Cartilage Restorative Procedures in the Knee
A total of 133 articles reporting clinical outcomes with respect to treatment of articular cartilage lesions of the knee were identified ( Table 1 ). The identified articles reported outcomes on a variety of primary procedures, including ACI, OCA, MF, OATs, and other novel procedures. ACI was the most commonly reported procedure (42.86% of articles). Data on MF, OCA, and OATs were reported in 16.54%, 15.04%, and 8.27% of articles, respectively ( Fig. 1 ).
Number of Articles Included by Journal Name and Impact Factor. a
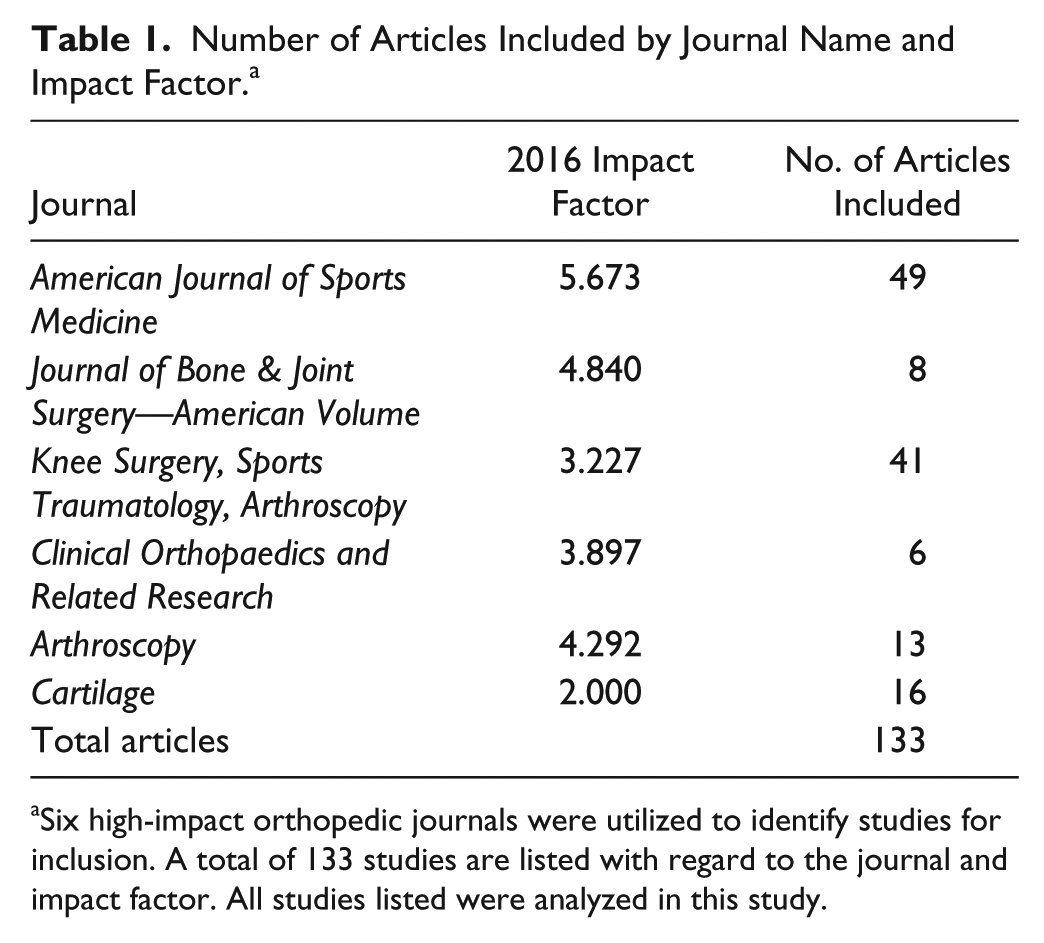
Six high-impact orthopedic journals were utilized to identify studies for inclusion. A total of 133 studies are listed with regard to the journal and impact factor. All studies listed were analyzed in this study.
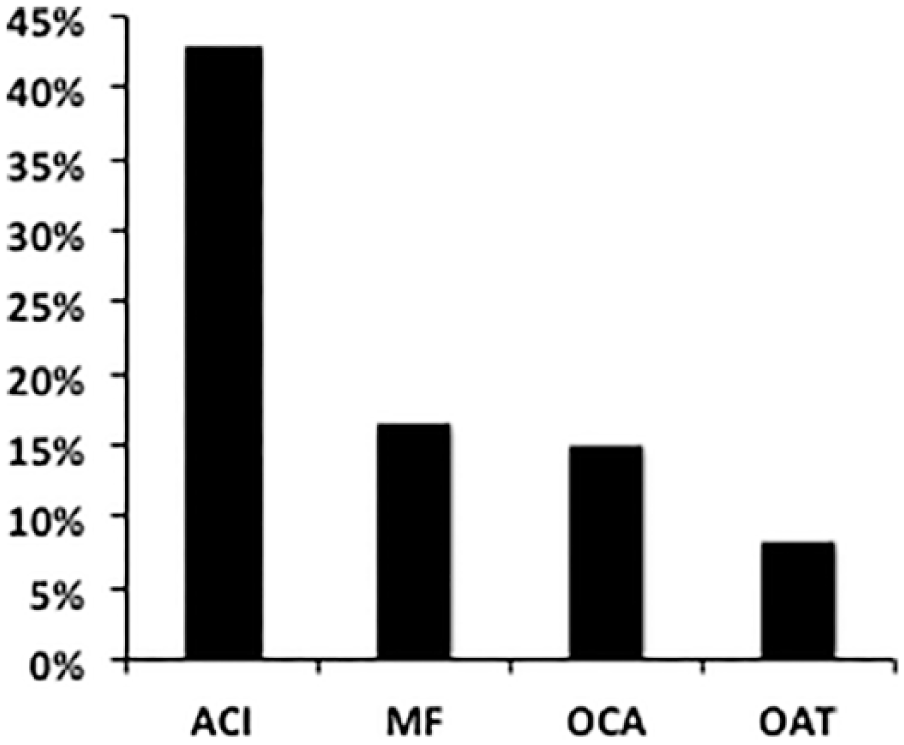
Primary intervention reported in identified article cohort (N = 133 studies). Microfracture (MF), autologous chondrocyte implantation (ACI), osteochondral allograft (OCA), and osteochondral autograft transfer (OATs) represent the most common treatment modalities for the management of primary cartilage defects in the knee, with ACI being most common.
Reporting or Excluding: Based on Studies Noting Concomitant Pathologies and Procedures
Concomitant pathologies included ligamentous instability, malalignment or maltracking, or meniscus insufficiency. Overall, 42.11% excluded patients with comorbidities, 41.35% included patients with comorbidities and treated those with concomitant procedures, and 16.54% did not report whether comorbidities were addressed.
As far as exclusion by comorbidities, the following criteria were most common: varus/valgus malalignment (38.35%), meniscal lesions (36.09%), and ligamentous instability (70.68%). Arthritis of any etiology was also used to exclude patients in 60.90% of studies.
Patients who underwent concomitant anterior cruciate ligament (ACL) reconstruction were included in 24.81% of articles of the total cohort and 60.00% of the cohort that treated comorbidities; concomitant meniscus repair in 23.31% of the total cohort and 56.36% of the cohort that treated comorbidities; osteotomies for malalignment in 11.28% of the total cohort and 27.27% of the cohort that treated comorbidities. Patients undergoing other concomitant procedures, such as lateral retinaculum release, were reported in less than 5.0% of the total cohort and 10.91% of the cohort that treated comorbidities ( Fig. 2 ). Of the studies that included these variables and required correction of the pathology at the time of cartilage repair, 72.73% (30.01% of all articles) of them scored outcomes separately ( Table 2 ).
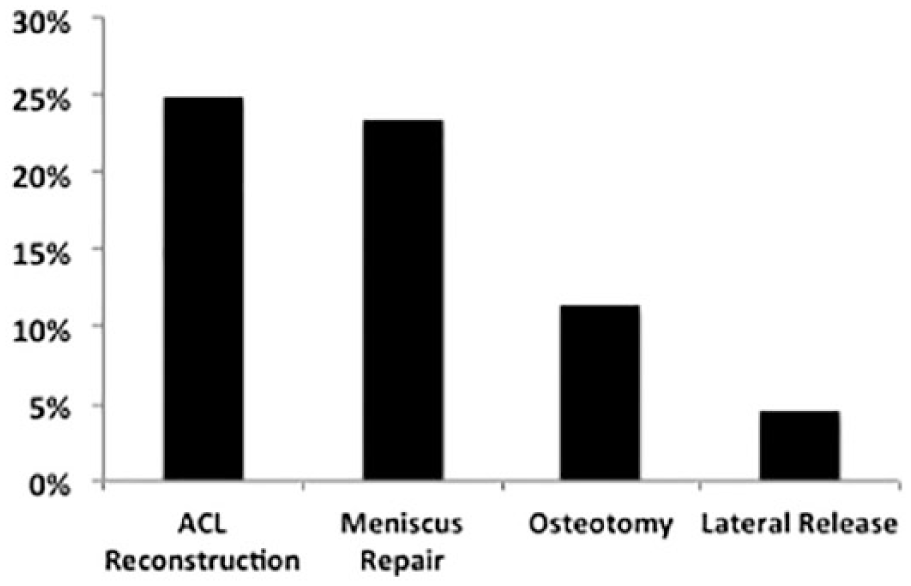
Concomitant procedures reported in identified article cohort (N = 133 studies). Concomitant pathologies included ligamentous instability, malalignment or maltracking, or meniscus insufficiency. Most common concomitant procedures listed as treatments to address these ailments shown. Anterior cruciate ligament (ACL) reconstruction and meniscus repair were noted to be the most common.
Variations in Exclusion Criteria with Regard to Concomitant Procedures. a
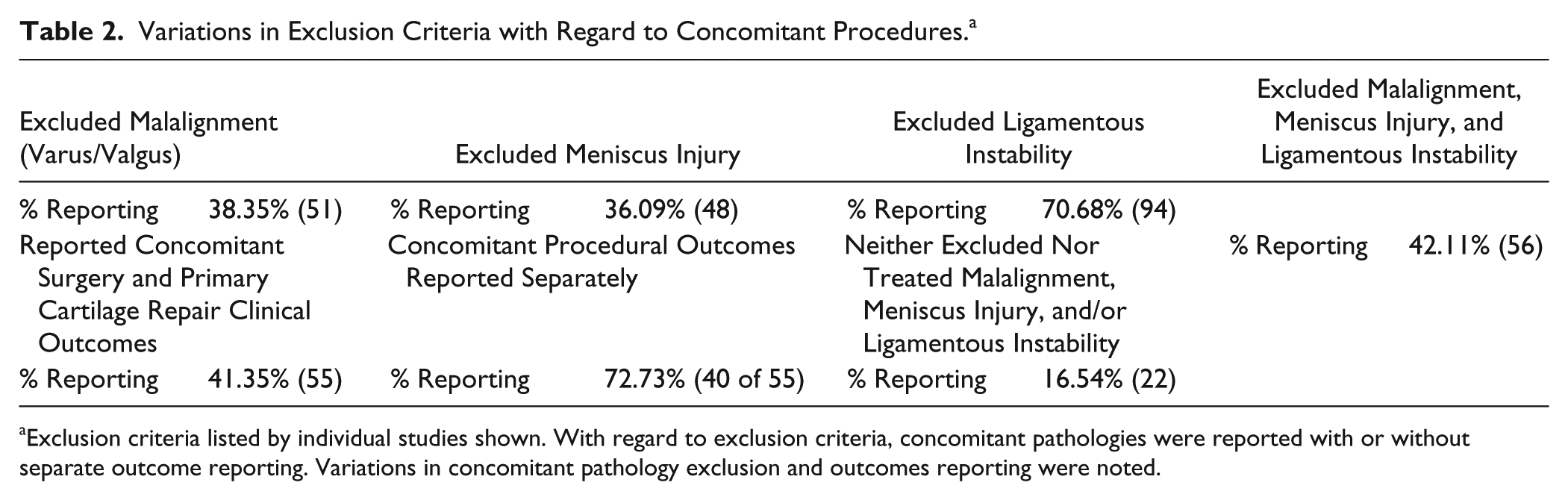
Exclusion criteria listed by individual studies shown. With regard to exclusion criteria, concomitant pathologies were reported with or without separate outcome reporting. Variations in concomitant pathology exclusion and outcomes reporting were noted.
Reporting Scoring of Concomitant Procedures Separately: Which System Was Used
Outside of the Knee Injury and Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) scoring systems, mentioned in 43.6% and 47.2%, respectively, the most commonly reported separate scoring systems mentioned in identified articles used were: Tegner (34.55%), Lysholm (30.91%), Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) (29.09%), and the visual analogue scale (VAS) (29.09%). All other scoring systems were reported in less than 17% articles, with a total of 18 different scoring systems utilized in total.
Discussion
Our most important findings noted that of the 133 total studies, 41% excluded concomitant pathologies, focusing solely on the treatment of articular cartilage defects. Nearly 42% of studies did not exclude concomitant pathologies, and properly treated these ailments along with the cartilage restoration procedure; the majority of which were ACL reconstructions and meniscal surgery. However, (27.81%), ultimately did not report data adequately, by not reporting if and how comorbidities were excluded or addressed (16.54%) or not reporting the outcomes separately (11.27%). Additionally, 18 different scoring methods were utilized, none of which was employed more than 50% of the time.
Outcomes following cartilage restoration surgery, regardless of type, depend on several patient and lesion specific factors, including body mass index (BMI), age, weight, lesion size, lesion depth, and morphology.7,15-20 Unlike patient factors, which tend to negatively influence outcomes, such as increased age or BMI, lesion specific factors do not all follow the same trends.7,15-20 This is further complicated when addressing comorbidities, which serve as confounders when reporting on chondral/osteochondral defects in the knee joint.8-14 Therefore, concomitant procedure specific factors should be strongly considered when reporting outcomes in clinical studies. As such, this study sought to evaluate the variability in concomitant procedure reporting, focusing on the following: exclusion criteria when disregarding concomitant ailments, independent concomitant procedure selection and outcomes scoring, and scoring system selection. By addressing these inadequacies, future reports will indirectly address confounders, allowing authors to focus solely on articular cartilage restoration of the knee.
Typically, lesions less than 2 to 4 cm2 can be treated via MF and OATs while larger lesions have better outcomes with ACI and OCA procedures.7,21-28 However, those guidelines are based on the assumption that prior literature properly acknowledge the role and results of the concomitant procedures and of the cartilage procedure itself. As reported in this study, 17% of primary clinical articles published since 2011 inadequately exclude concomitant pathologies, which serve to confound their reports. Therefore, while this is a minority of studies, questions may arise regarding the validity of such claims given such inconsistencies in reporting. Nonetheless, if these concomitant pathologies were addressed, arguments for confounding within current data on articular defects in the knee are without merit.
As such, it is currently believed that comorbidities such as malalignment (tibiofemoral or patellofemoral), meniscal injury or deficiency, ligamentous instability (including patellar) are not contraindications to cartilage repair procedures if they are addressed in a staged fashion or at the time of cartilage restoration.8-14 Ultimately, the correction of those factors cannot be overemphasized as failure rates are high if left untreated. This is supported by the improvement in clinical outcomes after surgical correction of concomitant comorbidities in treatment management.8-15,18 As seen with high tibial osteotomies (HTO), cartilage regeneration and correction can be successful when correcting for varus deformity. 29 Furthermore, combining tibial osteotomy procedures with cartilage restoration provides reliable improvement in functional status. 30 While some ligamentous insufficiencies such as ACL instability have clearer definitions, treatment guidelines, and more dichotomous status, many others have a large and continuous spectrum, from normal to severely abnormal. That is especially pertinent with regards to malalignment (coronal tibiofemoral and patellar) and meniscus status. As such, questions such as how many degrees of varus or valgus, and how much remaining meniscus are acceptable remain controversial and evidence currently relies on individual surgeon experience and opinion. Hence, without objective information regarding presence of concomitant pathology and its correction, these comorbidities can become confounding factors, leading to biased results and interpretations. Furthermore, defining the thresholds for malalignment and meniscus insufficiency that need to be addressed is not possible if those issues are not adequately evaluated and reported in a standardized manner in the first place. Despite the relevance of addressing and evaluating comorbidities and its treatment, nearly 17% of articles neither excluded nor treated concomitant pathologies identified in their study. These studies, along with the 15 studies that did not report a separate evaluation with regard to performing concomitant procedures, resulted in a total of 37 studies (27.81%), which ultimately did not report data adequately.
Of note, 40/55 studies focusing on articular cartilage defects while simultaneously addressing concomitant pathologies did adequately score outcomes independently, as mentioned above. However, 18 clinical scores were used, and none more than 50% of the time. Without common outcomes measures, high-level evidence with meta-analyses cannot be performed. As such cartilage surgeons must decide to narrow the choices to most effectively report on such concomitant procedures.
This study should be considered in the context of its limitations. As with our previous study, we included only studies published in 6 high-impact clinical orthopedic journals. 7 We therefore utilized the impact factor to help narrow our search, instead of gathering any/all resources from large databases, such as Pubmed, in general. Furthermore, the study only included articles published between 2011 and 2017, which further limits our sample size. Therefore, our results may not fully represent the average standards of publication for clinical studies in cartilage repair, as they represent a small, but representative, collection of modern literature. In addition, only articles from the high-impact journals listed previously were included which could underestimate the true degree of underreporting concomitant procedure outcomes. Lastly, the 133 articles (see the appendix) utilized may be prone to selection error during the literature search despite our best efforts. Nonetheless, while our sample of studies from various high-impact orthopedic journals does not encompass the entire research landscape, we believe that the inclusion of additional studies from lower impact journals would likely reinforce the results of the study.
Conclusion
In this study on knee cartilage restoration, recognition and management of concomitant pathology is inadequately reported in approximately 28% of studies. Only 30% of articles reported adequate treatment of concomitant ailments while scoring their outcomes using one of a potential 18 different scoring systems. These findings highlight the need for more standardized methods to be applied in future research with regard to inclusion, exclusion, and scoring concomitant pathologies with regard to treatment of cartilage defects in the knee.
Footnotes
Appendix
Authors’ Note
This study was primarily performed at the Department of Orthopedic Surgery in the David Geffen School of Medicine at UCLA
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.