
Abstract
Objective
Hip cartilage quality is essential for the success of joint-preserving surgery for osteonecrosis. This study aimed to characterize cartilage changes in osteonecrosis of femoral head (ONFH) using delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC).
Design
Fifteen asymptomatic (control) and 60 ONFH subjects were included in this study. The ONFH subjects were stratified in accordance with the Association Research Circulation Osseous (ARCO) classification (n = 15 hips per ARCO stage). All participant hips were investigated using dGEMRIC and theT1Gd data were collected and analyzed.
Results
T1Gd value was significantly lower in the ONFH group (365.1 ± 90.5 ms; range 200-498 ms) compared with the control group (546.1 ± 26.0 ms; range 504-580 ms) (P < 0.001). The T1Gd values of ARCO stage I-IV ONFH were 460.2 ± 17.3 ms (439-498 ms), 408.9 ± 43.4 ms (337-472 ms), 359.9 ± 34.5 ms (303-412 ms), 231.5 ± 15.1 ms (200-253 ms), respectively. Decreased T1Gd value was found to correlate significantly with increased ONFH severity (P < 0.001). T1Gd value in collapse stage was significantly lower than that of noncollapse stage (295.7 ± 70.3 ms [range 200-412 ms] vs. 434.6 ± 41.7 ms [range 337-498 ms]; P < 0.001).
Conclusions
dGEMRIC identified hip cartilage as abnormal in ONFH, even at early-stage, as represented by decreased T1Gd, and this was further aggravated by ONFH collapse.
Introduction
Osteonecrosis of the femoral head (ONFH) is a disease that commonly affects young adults, characterizing by progression of subchondral fracture and collapse.1-3 Collapse in ONFH can lead to hip osteoarthritis and disability, often requiring hip replacement. Because the majority of ONFH patients are young, they inevitably require several operations to preserve the affected joint. Because cartilage quality is essential for joint function, it is critical to investigate hip cartilage health in ONFH patients to identify optimal treatment strategies to preserve the joint.
Magnetic resonance imaging (MRI) is used to directly assess articular cartilage because it can visualize soft tissues. However, MRI only provides assessment of cartilage thickness with limited insight into tissue quality. Advanced methods to evaluate the morphologic and biochemical status of cartilage are therefore necessary to better understand cartilage health in ONFH. Delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC) has been developed to evaluate cartilage degeneration.4-7 dGEMRIC is regarded as a molecular imaging technique to examine the relative distribution of glycosaminoglycan (GAG) content in cartilage and can provide useful information beyond that available from radiography in the assessment of hip cartilage.8,9 Furthermore, dGEMRIC has been shown to be reliable at identifying early cartilage metabolic changes and predicting outcomes with joint preserving surgery in hip dysplasia 10 . However, there are no prior reports in English that describe dGEMRIC findings of cartilage at various stages of ONFH.
We have previously reported application of this method for ONFH assessment in a Chinese article. 11 . The purpose of this current study was to describe correlation of the dGEMRIC findings of ONFH hip cartilage health at different stages in accordance with the Association Research Circulation Osseous (ARCO) classification 12 and to examine the relationship between cartilage quality and collapse.
Methods
This study was carried out with approval from the China-Japan Friendship Hospital Ethics Committee and with informed participant consent. Fifteen asymptomatic volunteers (control) and 60 ONFH patients were included in this study.
Patients were diagnosed with ONFH based on clinical history, physical examination, and radiological evaluations (X-ray, computed tomography, and MRI) in accordance with a previously reported Chinese Guideline for Diagnosis of ONFH in Adults. 13 Inclusion criteria were ONFH diagnosis and age 18 to 50 years. Exclusion criteria were previous hip cartilage–related surgical treatment, associated dysplasia, or previous hip problems, including infection, femoral head fracture, and Legg-Perthes disease. A group of 15 asymptomatic volunteers aged between 18 and 50 years were selected from a larger pool of volunteers to represent the study control group. None of the control subjects had a history of hip problems, hip pain, or hip deformity. All control subjects were asked to complete functional questionnaires and were scored as full according to the Harris Hip Score System. 14
A total of 60 ONFH patients were included in the study: 36 males and 24 females. Twenty-four of these patients were affected bilaterally and 36 unilaterally. Because of the scan time, one hip from each of the control and bilateral ONFH patients was selected at random to undergo dGEMRIC scans. Subject demographics with regard to case number, age, gender, side scanned, Harris Hip Score, and body mass index (BMI) are shown in Table 1 .
Demographic Data of Patient and the Control Groups.
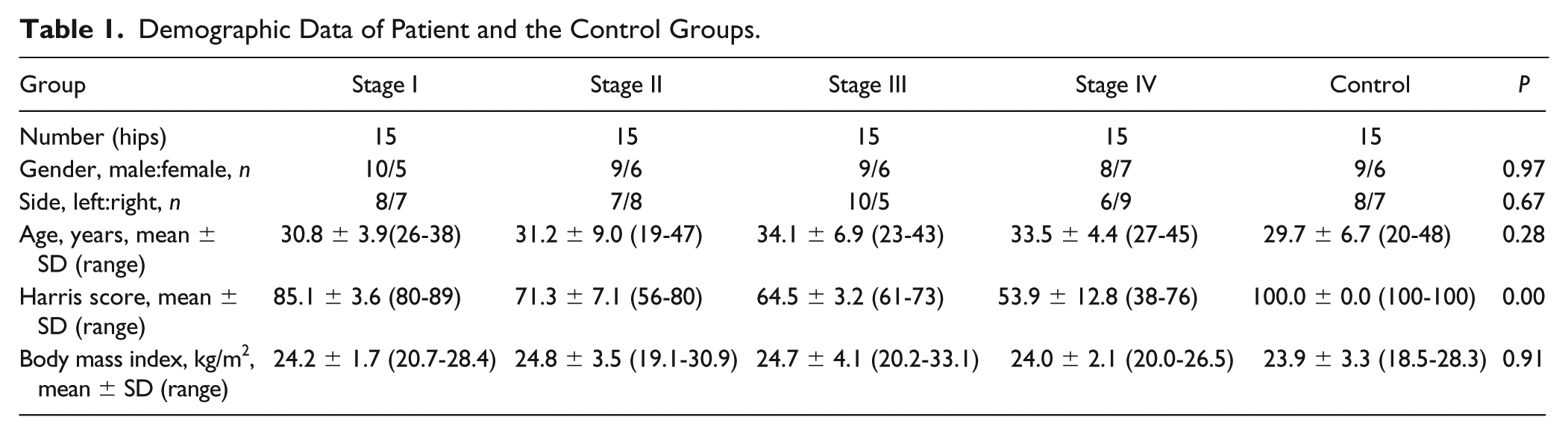
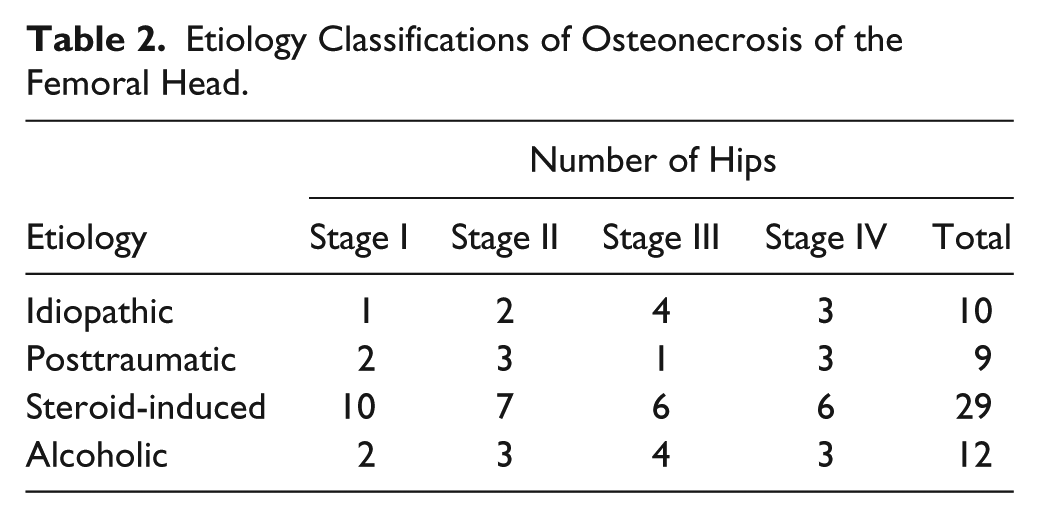
Mean ONFH patient age was 32.4 ± 6.4 years (19-47 years), similar to the control group (29.7 ± 6.7 years; 20-48 years) (P = 0.144). Average BMI in the ONFH and control group was 24.4 ± 2.9 kg/m2 (19.1-33.1 kg/m2) and 23.9 ± 3.3 kg/m2 (18.5-28.3 kg/m2), respectively (P = 0.574). Thirty-one ONFH hips were affected on the left side and 29 hips on the right side. With regard to ONFH etiology, 10 hips were affected by idiopathic osteonecrosis: 1 at stage I, 2 at stage II, 4 at stage III, and 3 at stage IV. Nine ONFH hips were posttraumatic: 2 at stage I, 3 at stage II, 1 at stage III, and 3 at stage IV. Twenty-nine hips were affected due to corticosteroid therapy: 10 at stage I, 7 at stage II, 6 at stage III, and 6 at stage IV. Twelve hips were affected from alcoholism: 2 were at stage I, 3 at stage II, 4 at stage III, and 3 at stage IV ( Table 2 ).
Etiology Classifications of Osteonecrosis of the Femoral Head.
Hips in the control and ONFH groups were imaged using the dGEMRIC. MRI was performed on a GE Signa Twin Speed 1.5-T scanner equipped with Excite technology (GE Healthcare, Waukesha, WI). Control and ONFH subjects were given an intravenous injection of the MRI contrast agent dimeglumine gadopentetate (Gd-DTPA2−, 0.4 mL/kg body weight) (Beilu Co. Ltd, Beijing, China). Following injection, the subjects walked for 65 minutes and were scanned in a supine position using the unified scanning method. Inversion recovery fast spin echo (IRFSE) sequence was used in the scan, and relative parameters were set as follows: inversion time (TI) = 100, 300, 500, 800, 1600 ms, with a repetition time (TR) = 3000 ms, echo time (TE) =14 ms, field of view (FOV) 160 mm × 160 mm, and matrix 256 × 256. dGEMRIC maps were generated with a pixel-by-pixel parameter fit using MATLAB 7.1 (The Math Works, Natick, MA). The dGEMRIC index was calculated as the average T1Gd across all pixels in a region of interest (ROI) encompassing the hip cartilage. ROI for hip cartilage was from the acetabular rim to the acetabular fossa. The regional distribution of dGEMRIC indices were illustrated using surface color plots. High indices were colored blue to signify estimated high GAG content, whereas conversely, low indices were colored red.
One joint surgeon (ZQD) and 1 musculoskeletal expert (CY) performed the MRI analysis, independent of the radiographic analysis. For reliability assessment, MRI measurements were repeated by the 2 authors after 3 months. To describe the dGEMRIC findings at various radiographic stages of ONFH, the dGEMRIC index for ROI of each hip was plotted according to the ARCO stage. The average T1Gd value of the four measurements was used for analysis. Intra- and interobserver reliabilities were evaluated using the intraclass correlation coefficient which was interpreted as follows: 0.21 to 0.40 indicated fair agreement, 0.41 to 0.60 indicated moderate agreement, 0.61 to 0.80 indicated substantial agreement, and 0.81 to 1.0 indicated excellent agreement.
A chi-square test was performed to compare the rate of different stages, sides, and gender groups. The t test was performed to determine statistically significant differences between 2 groups. A 1-way analysis of variance was performed for comparison of clinical and radiographic outcomes among different groups. All statistics were analyzed with software SPSS version 17 (SPSS Inc, Chicago, IL, USA). A P value <0.05 was considered statistically significant.
Results
The mean basic values of the ONFH and the control subjects are shown in Table 1 . The dGEMRIC images of different stages of the ONFHs and the control are shown in Figure 1 . Inter- and intraobserver reliabilities of the measurements were 0.87 and 0.89, respectively. As shown in Table 1 , no significant differences were found between groups with regard to age, side, gender, and BMI (P > 0.05). However, a significant difference was found in the Harris hip score value (P < 0.001), reflecting that disease severity was increased with ARCO stage.
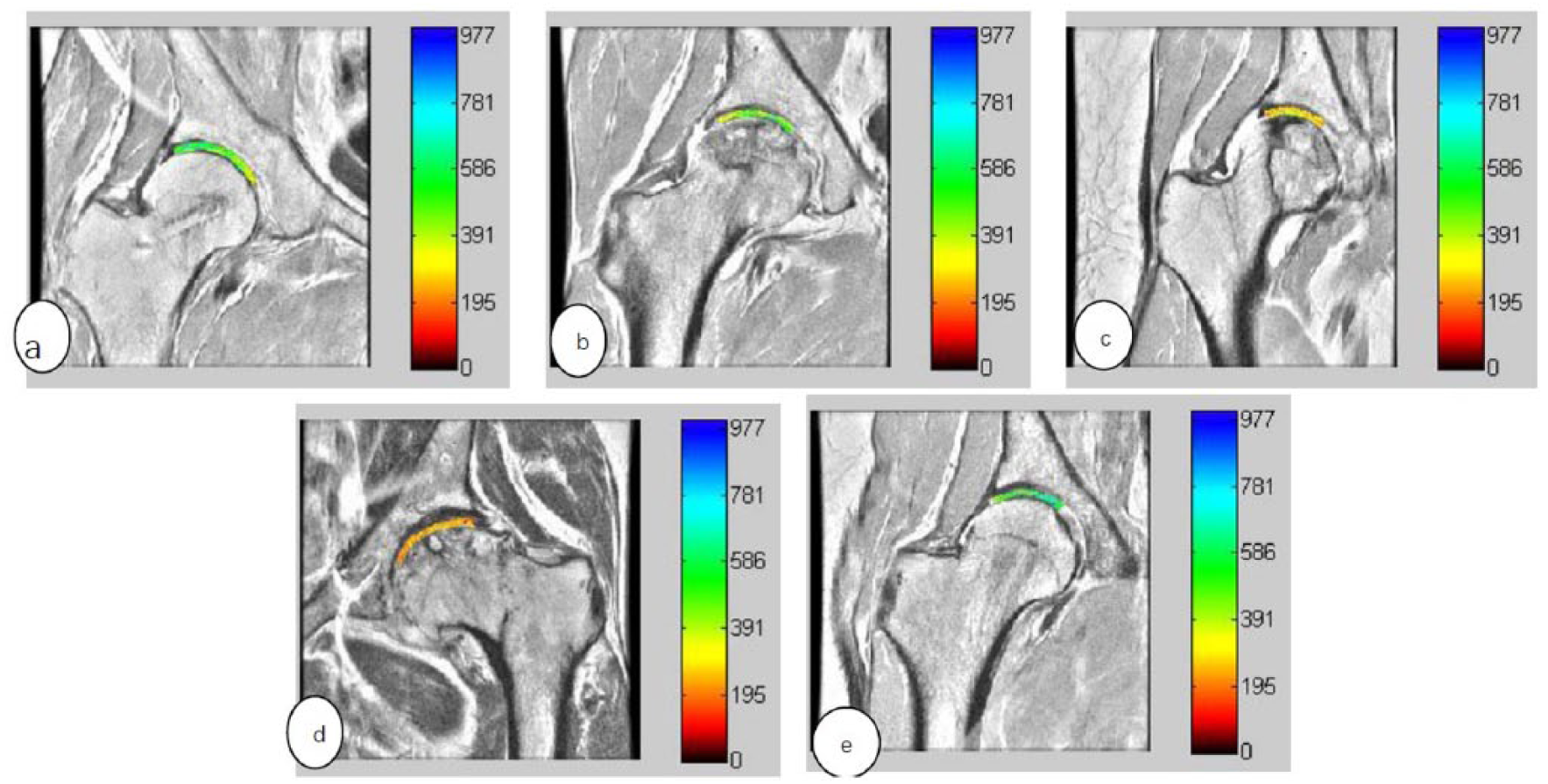
The delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC) images of different groups are shown in the figure. (
The T1Gd value for the control group was 546.1 ± 26.0 ms (504-580 ms), whereas conversely, the mean T1Gd value in ONFH group was 365.1 ± 90.5 ms (200-498 ms). When the data between ONFH and the control group were compared, the T1Gd value in ONFH group was significantly lower than that of the control group (healthy volunteers) (P < 0.001).
As shown in Figure 2 , significant differences in T1Gd values were found between different stages of the ONFH group (P < 0.001). The T1Gd value of ARCO stages I to IV were 460.2 ± 17.3 ms (439-498 ms), 408.9 ± 43.4 ms (337-472 ms), 359.9 ± 34.5 ms (303-412 ms), and 231.5 ± 15.1 ms (200-253 ms), respectively. Decreased T1Gd values correlated with increased ONFH severity, especially for the late stage (P < 0.001). Compared with the healthy control group, T1Gd values of ONFH stages I, II, III, and IV were 15.8%, 25.1%, 34.1%, and 57.6% lower, respectively (P < 0.001).
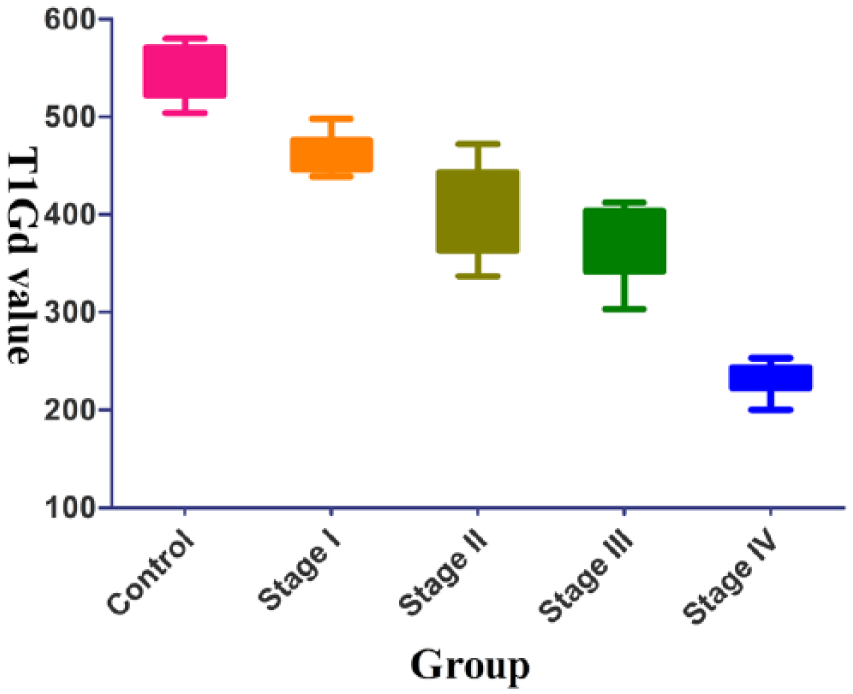
The T1Gd value for the control group was 546.1 ± 26.0 ms (504-580 ms). The T1Gd value of Association Circulation Osseous (ARCO) stages I to IV osteonecrosis of femoral head (ONFH) were 460.2 ± 17.3 ms (439-498 ms), 408.9 ± 43.4 ms (337-472 ms), 359.9 ± 34.5 ms (303-412 ms), and 231.5 ± 15.1 ms (200-253 ms), respectively. The decrease of T1Gd was aggravated with worsening of ONFH, and the difference was of significance (P < 0.001).
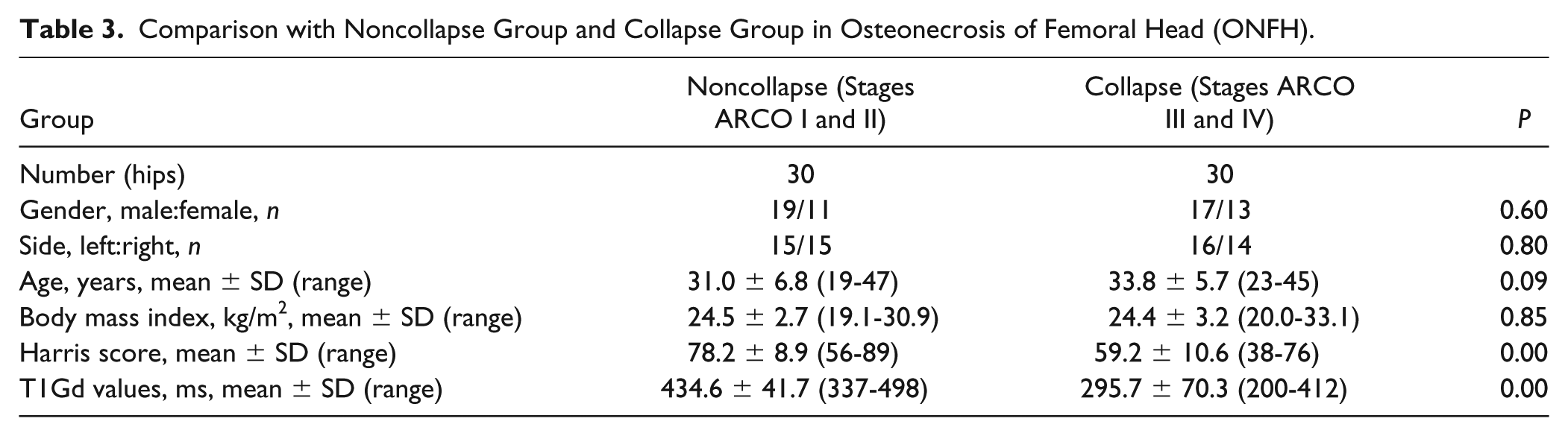
As collapse was considered a risk factor for osteoarthritis, the collapse stages ARCO III and IV were pooled together to compare with the noncollapse stages (stages ARCO I and II). The T1Gd value in the collapse group was significantly lower than that of noncollapse group (295.7 ± 70.3 ms (200-412 ms), 434.6 ± 41.7 ms (337-498 ms), P < 0.001) ( Table 3 ).
Comparison with Noncollapse Group and Collapse Group in Osteonecrosis of Femoral Head (ONFH).
Discussion
ONFH is a common disease characterized by osteocyte and bone marrow cell apoptosis, often resulting in femoral head collapse and osteoarthritis in 70% to 80% of patients if left untreated 15 . Because the majority of ONFH patients are young, the aim of treating ONFH is to preserve of the involved hip joint. 1 Cartilage is so essential that degeneration can lead to osteoarthritis. Cartilage is mainly composed of proteoglycans, collagen, and water.16,17 Proteoglycans primarily exist as aggregates formed by a high density of negatively charged GAG. The interaction between GAG and ionic interstitial fluid is responsible for structural integrity of the cartilage and its mechanical properties. Previous studies have suggested that loss in GAG content precedes other components during cartilage degeneration and can be regarded as an early indicator of cartilage degeneration. 18 The dGEMRIC index indirectly evaluates articular cartilage health by estimating GAG content. This technique has previously been validated in studies of early cartilage degeneration as a direct indicator of GAG concentration.9,19 It has also been shown to be a reliable modality for detecting degeneration of articular cartilage in hip dysplasia and in identifying hips at risk for early failure following Bernese periacetabular osteotomy. 20 Bittersohl et al. 21 assessed cartilage damage in femoroacetabular impingement using dGEMRIC and found that dGEMRIC had higher sensitivity than standard MRI assessment. Domayer et al. 22 believed that dGEMRIC was a technique for noninvasive assessment of cartilage health and cartilage repair in morphologic analysis. These studies provide strong evidence for the inclusion of the dGEMRIC method into ONFH analysis for enhanced study of cartilage.
The study was conducted using dGEMRIC to evaluate the degeneration of articular cartilage in ONFH. The ONFH group demonstrated statistically lower dGEMRIC indices compared with the control group, suggesting greater degeneration of articular cartilage with loss of GAG content in ONFH hips. The T1Gd value at stage I in the ONFH group was 15.8% lower than that of the control group, which reflected that ONFH patients without articular cartilage morphometric influence had underlying metabolic changes. This emphasizes that dGEMRIC is a sensitive measurement of early cartilage pathology in ONFH. In future studies, morphometric metrics using MRI could be combined with dGEMRIC for better assessment of biochemical changes in cartilage. The reason for early degeneration of the articular cartilage may be due to joint synovitis and inflammation. Joint effusion, likely secondary to ONFH related synovitis has been observed in up to 72% of cases regardless of articular collapse. 23 Yamaguchi et al. 24 investigated synovial fluid volume, using interleukin (IL)-6 level to assess hip synovitis, and found ischemic osteonecrosis results in IL-6 production in the articular cartilage through an HIF-1-dependent pathway. IL-6 produced by hypoxic articular chondrocytes stimulates inflammatory cytokine responses in synovial cells. Another finding was that the decrease in T1Gd was aggravated with worsening of ONFH. In the present study, the dGEMRIC indices were generally in the low- to mid-range of values at early stage ONFH. However, the dGEMRIC indices were much lower in late stage ONFH, which was an indicator of the overall level of disease and perhaps demonstrates biochemical degeneration prognosis in the history of ONFH. This differentiation of disease status by dGEMRIC may be a useful approach to define cartilage health in clinical evaluation.
Collapse of the femoral head will cause incongruity of the joint, resulting in altered stress distribution in the femoral head, and eventually leading to secondary osteoarthritic joint degeneration. 25 In the study, we demonstrated a significant decrease of T1Gd value in the collapsed stage compared with the noncollapsed stage. Hip cartilage showed abnormal change before collapse, represented by the loss of GAG, and was aggravated by collapse. Several previous studies have demonstrated degeneration of articular cartilage in collapsed ONFH without any radiographic evidence of joint space narrowing.26,27 Magnussen et al. 26 evaluated the articular cartilage of surgically resected femoral heads with Marcus stage IV ONFH and found degeneration in histopathologic analysis. Ruch et al. 27 reported that degeneration of articular cartilage was found in 36% of collapsed femoral heads on arthroscopic examination for which there were no radiological signs of cartilage degeneration. Magnussen et al. 28 analyzed 13 postcollapse osteonecrotic femoral heads to determine quantitatively the biomechanical and histological properties and found that decreasing cartilage tensile strength correlated with histologic evidence of degeneration. Decreased loading of the cartilage overlying the collapsed ONFH lesions resulted in proteoglycan loss. 28 Therefore, degeneration of articular cartilage was aggravated with collapse of ONFH.
There are several study limitations that should be noted. First, this was a cross-sectional study that cannot reflect the prognosis and clinical outcome of ONFH. Therefore, longitudinal studies are needed to determine whether low dGEMRIC values without collapse could be a predictor of collapse, or whether such cartilage health can improve under appropriate interventions, given that the cartilage may be morphologically intact. Second, sample numbers for each group were relatively low as this was an experimental protocol and not all ONFH patients in our hospital were included to get a dGEMRIC scan. However, it took 3 years to collect the 15 stage I ONFH patients, as the early diagnosis was difficult. Third, differentiation between acetabular and femoral cartilage was strictly impossible in the hip dGEMRIC study and ROI analyses included both as one entity. Although these results are semi-quantifiable, they could be valuable for cartilage assessment of early-stage ONFH as a noninvasive technique, especially to enable an appropriate joint preserving treatment. Fourth, MRI volume measurements and osteonecrosis-type analysis may also provide more detailed understanding of the relationship between cartilage and collapse. Further studies are needed to determine the utility of dGEMRIC investigation in ONFH.
In conclusion, dGEMRIC is reliable at identifying early cartilage health changes in ONFH. Cartilage of the ONFH hip showed abnormal change, even at early stage, represented by a decrease of T1Gd that was aggravated with worsening of ONFH.
Footnotes
Acknowledgments and Funding
We would like to thank the volunteers and patients included in the study for their cooperation. We would also like to thank Jing-Sheng Li in the Bioengineering Laboratory, Department of Orthopaedic Surgery, Massachusetts General Hospital /Harvard Medical School, Boston, MA, USA, for the English improvement. This study was funded by the Beijing Municipal Science and Technology Commission (Grant No. Z171100001017209), the National Natural Science Foundation of China (Grant No. 81703896), and the Capital Health Research and Development of Special Fund (Grant No. 2016-2-4062).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. This study has the permission from the ethical committee of China-Japan Friendship Hospital.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable.