
Abstract
Nonsurgical treatment such as exercise is the preferred method for management of knee osteoarthritis (OA). A combination of aerobic, muscle strengthening, and flexibility exercises is recommended for older adults. However, effects of the exercise intervention on cartilage metabolism remain unclear. This study used biomarkers to investigate the effects of well-rounded exercise program on cartilage metabolism in 42 women (mean age: 59 years). Participants started a weekly supervised exercise program and continued for 12 weeks. Before and after the program, we measured physical performance on the Timed Up-and-Go Test, 3-Minute Walk Test, and 30-Second Chair Stand Test. We collected serum and urine samples at the start of the program until 24 weeks and measured the concentrations of 4 biomarkers related to type II collagen metabolism: serum cartilage type II procollagen carboxy propeptide (sPIICP), urine C-terminal telopeptide of collagen type II (uCTX-II), urine cleavage of type II collagen by collagenases (uC2C), and serum cartilage oligomeric matrix protein (sCOMP). Participants were divided into pre-OA and OA groups based on X-ray findings. The pre-OA group showed significant increases and decreases in sPIICP and uCTX-II concentrations with improved physical performance, respectively. sCOMP concentrations significantly increased in both groups. The exercise also improved physical performance with no detrimental effect on type II collagen metabolism in the OA group. Thus, well-rounded exercise may not only improve physical capacity but also have beneficial effects on type II collagen metabolism, especially in people without radiological OA.
Introduction
Osteoarthritis (OA) is one of the most common chronic joint diseases. OA can potentially affect most of joints in the whole body, but the knee is one of the most frequently affected, most severely impaired joints. In other words, knee OA substantially causes disability and reduces the quality of life. To prevent knee OA, exercise has been constantly recommended. Exercise training for older adults ideally includes a combination of aerobic, muscle strengthening, and flexibility exercises. Such a well-rounded exercise program is considered to be effective for attenuating deterioration in functional fitness associated with aging and a sedentary lifestyle. 1 The Osteoarthritis Research Society International has recently published a guideline for the nonsurgical management of knee OA, which strongly recommends exercise as one of the core treatments for people with knee OA regardless of their comorbidities. 2 Several studies regarding knee OA have shown that exercise has positive effects on pain and function, and is cost-effective, and increasing muscle strength improves joint stability and reduces pain and disability.3-7 On the other hand, OA affects articular cartilage, subchondral bone, synovium, and ligaments, but articular cartilage degradation, from a pathophysiological point of view, is considered to be one of the main causes of OA progression.8-10 Therefore, there is concern about whether physical exercise causes further degeneration of articular cartilage, especially in elderly people. 11 To our knowledge, no prospective research has been designed to show whether physical exercise has protective or damaging effects on articular cartilage.
To assess the effects of exercise on articular cartilages, biomarkers may be useful for evaluating the biological status of OA, which cannot be determined using standard imaging techniques such as X-ray, computed tomography, or magnetic resonance imaging (MRI).12,13 The articular cartilage degenerates slowly in knee OA, but it is not easy to evaluate a patient’s status precisely even with the use of intra-articular imaging by fine MRI techniques such as T2 mapping. 13 Thus, researchers and clinicians have searched for biomarkers of knee OA that can be used to diagnose and evaluate OA, assess a patient’s current status, and predict the prognosis of the disease.
Two main components of articular cartilage have been investigated as possible biomarkers of knee OA: type II collagen and aggrecan. Type II collagen is a major cartilage structural component that accounts for about 95% of all collagen types and forms the fibrils that give cartilage its tensile strength.14-16 In the process of collagen formation, the carboxy-terminal propeptide of type II collagen (PIICP) is removed from the procollagen extracellularly and this directly reflects the rate of type II procollagen synthesis. 17 In progressive joint diseases, the degradation of extracellular matrix proteins and proteoglycans leads to irreversible changes in the properties of the collagen network. In addition, the imbalance in the turnover of matrix proteins often results in increased proteolysis of molecules bound to and exposed at the surface of collagen fibers such as cartilage oligomeric matrix protein (COMP). 18 The COMP fragment is a noncollagenous matrix protein primarily identified in cartilage and is suggested to have a role in regulating fibril assembly as well as a structural role for maintaining the mature collagen network. 19 Following the degradation of cartilage, fragments of carboxy-terminal crosslinked telopeptide of type II collagen (CTX-II) are released into the circulation and are subsequently secreted into urine. 20 Several studies have shown a significant association between radiographic progression of OA and CTX-II concentration.21-23 In addition, the cleavage of type II collagen by collagenases is also excessive in OA cartilage and yields fragments, such as the C2C epitope (COL2-3/4Clong mono), whose concentrations reflect cartilage degradation. The C2C assay is specific for type II collagen, and serum levels of C2C correlate with cartilage degeneration in patients with symptomatic knee OA. 24 Therefore, CTX-II and C2C are considered to be potential biomarkers of cartilage degradation and OA progression. However, there are few reports about whether exercise therapy affects the levels of cartilage biomarkers in serum and urine.
The purpose of this study was to clarify the effects of a well-rounded exercise on cartilage metabolism by analyzing cartilage biomarkers. We hypothesized that well-rounded exercise would influence both anabolic and catabolic biomarkers of type II collagen and COMP in association with improved physical capacity.
Methods
Participant Enrollment
Informed consent for the study was obtained from all participating patients in accordance with the World Medical Association Declaration of Helsinki. Forty-eight adult women aged between 49 and 71 years were recruited from a local society club and participated in this study. Participants were included regardless of the degree of knee pain. Participants with inflammatory joint disease such as rheumatoid arthritis or posttraumatic arthritis, or with comorbidities that would preclude regular exercise were excluded. Participants were also excluded if they had a history of or were expected to receive joint replacement surgery or high tibial osteotomy before the start of the program.
Exercise Program
Participants agreed not to receive any treatment for knee joint pain during the study period before the start of the program. During the first 12 weeks, all subjects participated in a weekly supervised exercise class. The well-rounded exercise program included stretching, balance exercises, walking, and isometric exercises on the floor aimed at improving strength and endurance of the lower extremity. These exercises were performed for 90 minutes once a week under supervision. The participants were encouraged to do self-exercise at home throughout the study period for up to 24 weeks after the start of the program. We defined the start of the exercise program as week 0 (0W), the end of the exercise program as week 12 (12W), and the end of follow-up as week 24 (24W).
Objective Measurements
Before starting the exercise program, a standing anteroposterior knee radiograph was taken for each participant to evaluate the radiological OA status of the knee joint using the Kellgren and Lawrence (K-L) grading system. 25 There is consensus that K-L grade ≥2 indicates radiologically defined knee OA. Both before the start and after the end of the exercise program, we measured the participants’ physical performance on the Timed Up-and-Go Test (TUG), 26 3-Minute Walk Test (3MWT), 27 and 30-Second Chair Stand Test (30s-CST). 28 Each participant performed initial practice trials of these 3 tests to reduce any practice effect. In addition, knee pain and function were evaluated every 4 weeks from 0W to 24W with the Japanese Knee Osteoarthritis Measure (JKOM) 29 including a visual analogue scale (VAS).
Collection and Storage of Blood and Urine Samples
Blood and urine samples were taken every 4 weeks for the 24 weeks. On the day of exercise, these samples were collected before exercise. The blood samples were allowed to clot for 20 minutes at room temperature and centrifuged, and the supernatant was separated as serum and transferred for storage at −80°C until assayed. Urine samples were centrifuged to remove any particles, and the supernatants were stored at −80°C until assayed.
Measurements of Serum and Urine Cartilage Biomarkers
Enzyme-linked immunosorbent assays (ELISAs) were used to measure the concentrations of serum PIICP (sPIICP), urine CTX-II (uCTX-II), urine C2C (uC2C), and serum COMP (sCOMP) using commercial ELISA kits: #MBS164407 from MyBioSource (San Diego, CA, USA); #CSB-E14328h from CUSABIO BIOTECH CO. (Wuhan, Hubei, China); #60-1001-001 from IBEX Pharmaceuticals Inc. (Montreal, Quebec, Canada); and #DCMP0 from Quantikine R&D Systems (Minneapolis, MN, USA), respectively. Our preliminary study analyzing the serum and urine samples from females with similar demographic backgrounds of this study revealed that the four biomarkers showed no significant alteration during 24 weeks with no well-rounded exercise intervention (data not shown).
Statistical Analysis
Comparisons between groups and within groups were performed using the Wilcoxon signed-rank test and Wilcoxon rank-sum test, respectively. The level of significance was defined as P < 0.05. All analyses were performed using JMP software version 12.2.0 (SAS Institute, Inc, Cary, NC, USA).
Results
Three subjects who did not agree to provide informed consent and another 3 who did not participate in the exercise program were excluded. Thus, 42 women aged between 49 and 69 years (mean ± SD: 59 ± 6 years) participated in this study. The participants’ baseline demographics are shown in Table 1 . Throughout the study period, all the mean JKOM scores were <6 out of 100 points, and those of pain VAS were <8 out of 100.
Demographic Data for Participants. a
Values are given as the mean ± SD, unless otherwise indicated.
Changes in the Type II Collagen Biomarkers in All Participants
We measured sPIICP, uCTX-II, uC2C, and sCOMP levels by ELISA to evaluate the effect of well-rounded exercise on type II collagen metabolism. Serum PIICP concentration was significantly greater at 8W than at 0W (P < 0.05). By contrast, uCTX-II concentration was significantly lower at 24W than at 0W (P < 0.01), and uC2C concentration was significantly lower at 12W than at 0W (P < 0.05). Serum COMP concentration was significantly greater at 24W than at 0W (P < 0.01) ( Fig. 1 ).
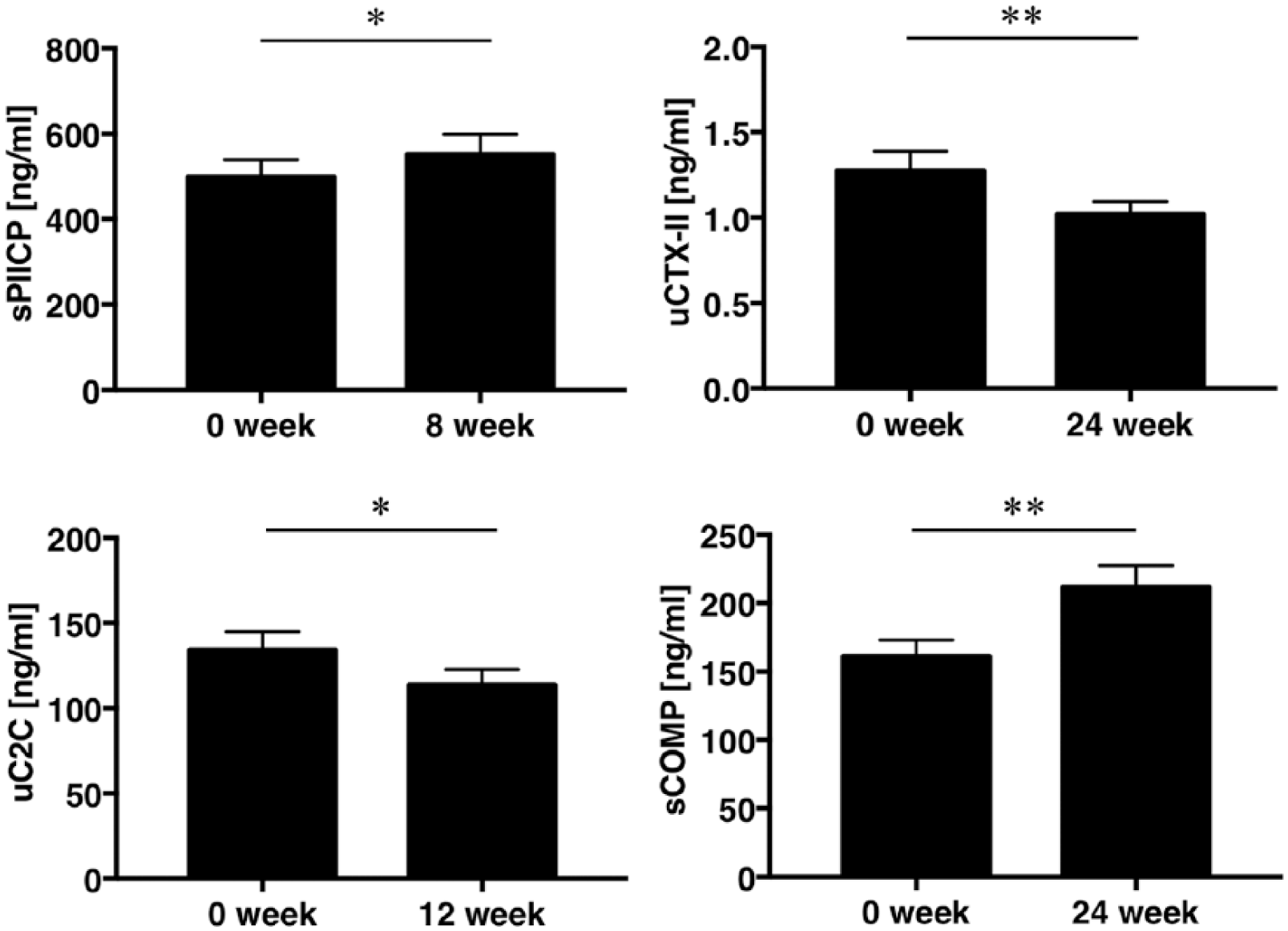
Effects of exercise program on type II collagen biomarkers. Values are given as the mean ± SEM.
Association between Alterations in Type II Collagen Biomarkers and K-L Grades
We further investigated the relationship between radiological OA grading and the changes in the biomarker concentrations because exercise may cause a damaging effect on degenerated articular cartilage. The participants were classified into 2 groups according to K-L grades; K-L ≤1 (preradiological OA) and K-L ≥2 (radiological OA). The baseline data for the 2 groups are shown in Table 2 . Participants in the K-L ≤1 group were significantly younger than those in the K-L ≥2 group (P < 0.01). While the sPIICP concentration was significantly higher at 8W than at 0W in the K-L ≤1 group (P < 0.05), it did not differ significantly between these time points in the K-L ≥2 group. The K-L ≤1 group showed significantly lower levels of uCTX-II at 24W compared with those at 0W (P < 0.01), whereas there was no significant difference in the levels between these time points in the K-L ≥2 group. No significant differences were found in uC2C concentrations between 0W and 12W regardless of the grouping according to K-L grade. In the both groups, sCOMP concentrations were significantly greater at 24W than at 0W (K-L ≤1 group; P < 0.01, K-L ≥2 group; P < 0.05, respectively) ( Table 3 ).
Demographic Data for the Participants Grouped According to Kellgren-Lawrence (K-L) Grade.
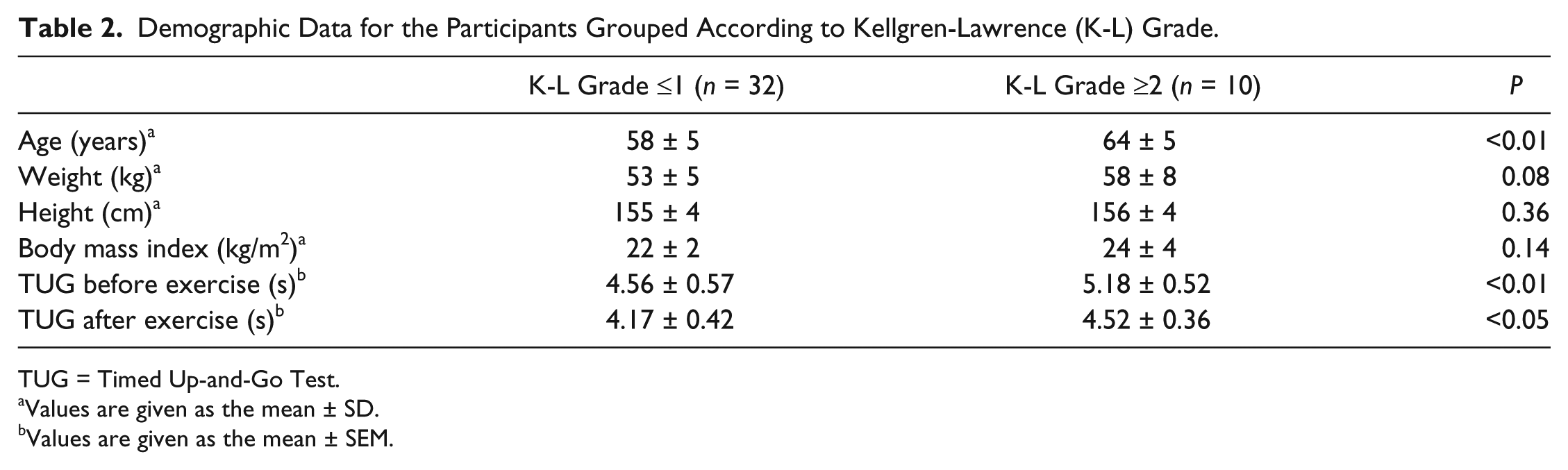
TUG = Timed Up-and-Go Test.
Values are given as the mean ± SD.
Values are given as the mean ± SEM.
Comparisons of Cartilage Biomarker Concentrations in the Participants Grouped According to Kellgren-Lawrence (K-L) Grade. a
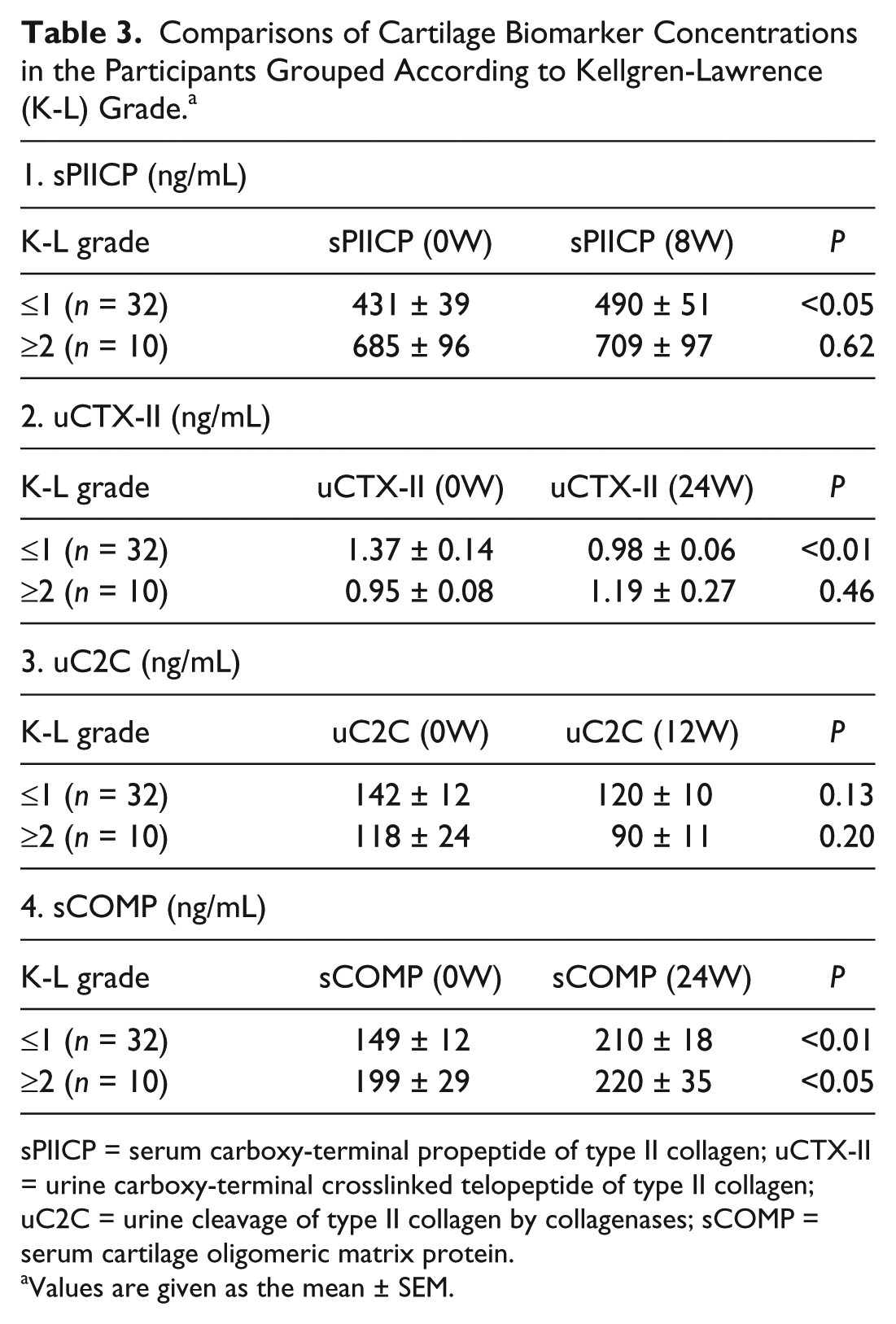
sPIICP = serum carboxy-terminal propeptide of type II collagen; uCTX-II = urine carboxy-terminal crosslinked telopeptide of type II collagen; uC2C = urine cleavage of type II collagen by collagenases; sCOMP = serum cartilage oligomeric matrix protein.
Values are given as the mean ± SEM.
Physical Activity before and after the Exercise Program in All Participants
Performance on all of the 3 tests improved significantly at 12W compared with the baseline (0W). The time to perform the TUG was significantly shorter at 12W than at 0W (mean ± SD, 4.7 ± 0.6 and 4.2 ± 0.4 seconds, respectively; P < 0.001). There was a significantly greater distance walked in the 3MWT at 12W than at 0W (mean ± SD, 314 ± 24 and 327 ± 25 m, respectively; P < 0.001). The frequency was significantly higher in the 30s-CST at 12W than at 0W (mean ± SD, 23 ± 4 and 29 ± 4, respectively; P < 0.001) ( Fig. 2 ).
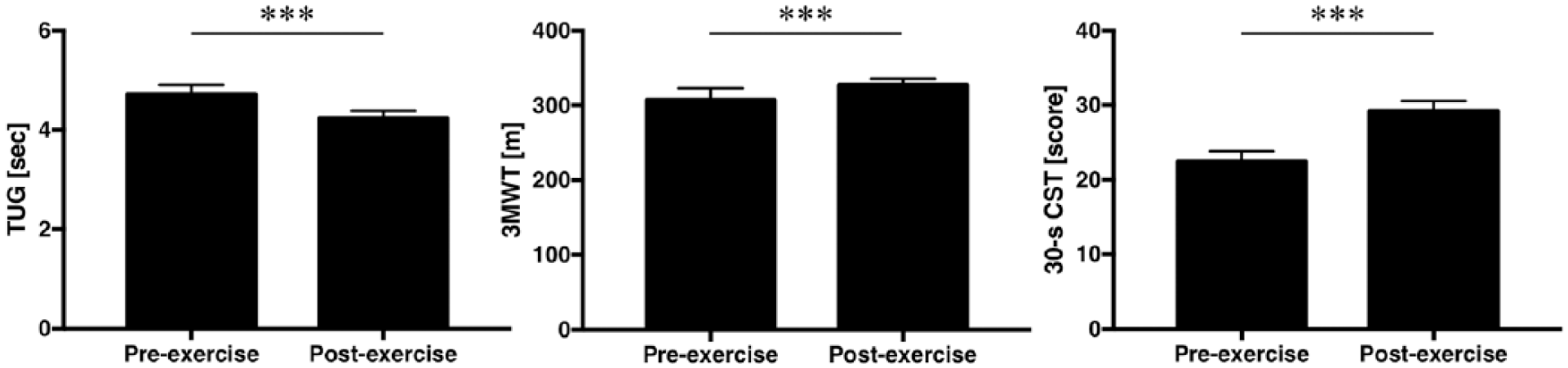
Comparisons of physical performance tests before and after exercise program. Values are given as the mean ± SEM. TUG = Timed Up-and-Go Test; 3MWT = 3-Minute Walk Test; 30s-CST = 30-Second Chair Stand Test.
Discussion
The current study is the first to show that well-rounded exercise program can affect the biological status of the articular cartilage as assessed by biomarkers of type II collagen and COMP. Analyses using the samples from all subjects demonstrated a significant increase in type II collagen synthesis (sPIICP) at 8W and a significant decrease in type II collagen degradation at 12W (uC2C) and 24W (uCTX-II) compared with baseline data at 0W in association with improved physical performance. Serum COMP concentration was also significantly greater at 24W than at 0W. The effect of well-rounded exercise program on type II collagen metabolism was found to be different between pre-OA (K-L ≤1) and OA (K-L ≥2) stages because the participants with K-L ≤1 knees showed an increase and a decrease in type II collagen synthesis and degradation in contrast to the subject with those with K-L ≥2 knees. It is likely, therefore, that well-rounded exercise program could induce a beneficial effect on metabolism of type II collagen and COMP, the essential component of cartilage matrix, especially in the subjects with preradiological knee OA.
Nonsurgical treatments are considered to be the preferred method for the management of knee OA.2,30,31 These treatments include the use of both nonpharmacological and pharmacological therapies. Exercise is representative of a nonpharmacological therapy and is strongly recommended by current clinical guidelines for knee OA. 2 Evidence is unanimously positive on the effects of exercise in reducing pain and improving physical function. In this study, 3 tests were used to determine physical performance both before and after the exercise program, and the subjects’ performance improved on all 3 tests. Additionally, throughout the study period, all the mean JKOM scores were <6 out of 100 points, and those of pain VAS were <8 out of 100. These results suggest that this exercise program improved physical performance without causing knee pain.
It is important to understand the influence of physical activity on the development and progression of OA, particularly on weight-bearing joints like the knee. A systematic review has found strong evidence for no effect of physical activity on radiological joint space narrowing.32-34 However, there is limited evidence on positive association between physical activity and cartilage volume. A recent study reported no association between cartilage volume loss and level of physical activity on MRI, whereas another study using MRI reported a positive relationship between physical activity and tibiofemoral cartilage volume.35,36 A cohort study reported an inverse relationship between physical activity and cartilage defects. 37 These findings suggest that physical activity may be beneficial to joint health without a destructive effect on the knee joint. These findings also indicate the requirement of further studies that examine the effect of physical activity on individual structures of the knee joint rather than the joint as a whole. For example, in an animal study using surgically induced OA rabbit, sCTX-II levels correlate with T2* values of cartilage by MRI. 38 Thus, biomarkers reflect the property of articular cartilage and may be useful for evaluating the effect of physical activity on cartilage structure.
The current results clearly show that a well-rounded exercise has beneficial effects on biomarkers regarding type II collagen in subjects having preradiological OA, but the potential reasons remain to be investigated. One of the possible reasons may be that stimulation by exercises induces anabolic effects on articular chondrocytes which have not yet advanced to degenerative stages in OA cartilages. Indeed, several review articles strongly indicate articular chondrocytes have ability to produce type II collagen by mechanical stimulation in vitro and in vivo.10,39,40 In other words, well-rounded exercises should be started before the articular cartilages have degenerated beyond the point in which one can see OA changes in X-ray.
On the other hand, the biomarkers investigated in this study remained constant after the exercise in radiologically advanced subjects. A report from the Rotterdam study cohort has shown that the uCTX-II concentration is associated with the incidence and progression of radiographic OA and K-L grade. 41 A cross-sectional study has also reported that knee cartilage defect severity is significantly associated with uCTX-II in samples from female OA patients. 42 In line with the systematic review, 32 an important message shown here is that no increase in type II collagen degradation in the participants with radiologically knee OA (K-L ≥2) indicates that the well-rounded exercise program may cause at least no detrimental effect on advanced OA cartilage and should be recommended even for such patients.
It is well-known that articular cartilages have other crucial extracellular matrix other than type II collagen. Among many types of such proteins, COMP has been one of the most investigated noncollagenous extracellular matrix in articular cartilages so far. Previous studies have reported an immediate increase in sCOMP levels after cyclic mechanical loading, such as moderate walking, 43 and running.44,45 On the other hand, synovial fluid COMP concentrations significantly decreased after running and changes in serum and synovial fluid COMP pre- to postintervention were inversely correlated. 45 These findings suggested that cyclic mechanical loading facilitates the movement of COMP from the joint space to the serum, which may be consistent to the present results. In the current study, participants started a weekly exercise program and continued for 12 weeks. Consequently, sCOMP concentrations significantly increased at 24W, regardless of radiological stages. What these changes mean to the articular cartilage status remains to be investigated, but it may be speculated, at least, that the effects of the 12-week exercise program on COMP last at least 12 weeks after exercise.
This study has several limitations. First, this was a prospective study with a single arm. Therefore, the effects of exercise cannot be compared between these subjects and those who did not participate in the exercise program. Second, the duration of the exercise and/or the observation period may not have been long enough. If participants had performed exercise longer or been observed for longer, the results may have been different. Third, neither could we precisely document the activities and/or exercise performed by participants at home nor could we collect data about other treatments during the follow-up period, even though the participants had been instructed not to receive any treatment for knee joint pain other than this exercise program. Fourth, the knees of participants were evaluated by only X-ray images before the study and not by MRI or other modalities. Although the K-L grading system is useful, the grading is ambiguous and may not indicate the active status of the articular cartilage. Fifth, we selected 3 types of biomarkers regarding type II collagen and a noncollagenous extracellular matrix protein, COMP, because those have been well studied and accepted as potential cartilage biomarkers. However, other types of biomarkers such as pro- or anti-inflammatory cytokines may show different patterns and give us useful clues. Finally, the present study was designed to collect data from participants with various knee OA status, although most of the participants had a K-L grade of 0 or 1. Nevertheless, despite these limitations, this is one of the first prospective studies to investigate the effects of an exercise program on the biological status of the articular cartilage of the knee.
In conclusion, the present study found that well-rounded exercise program may facilitate type II collagen synthesis and suppress or slow the collagen degradation, especially in the female participants with pre-radiological knee OA. The exercise yielded no detrimental effect on cartilage metabolism in association with improved physical performance in the subjects with radiological knee OA. Therefore, a well-rounded exercise is highly recommended as chondroprotective activity for the individuals with preradiological knee OA and may be the first choice of treatment for patients with early stage knee OA.
Footnotes
Authors’ Note
The sponsors were not involved in the study design; in the collection, analysis, interpretation of data; in the writing of this manuscript; or in the decision to submit the article for publication.
Acknowledgments and Funding
The authors thank Drs. Masahiro Ishikawa, Hiroko Morise, Takahiro Iwata, and Koichi Murata for their substantial contribution and thoughtful discussion. This work was supported by Grants-in-Aid KAKENHI (25282220).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HI has received a research grant from Bristol-Myers, and Astellas.
Ethical Approval
The protocol for this study was approved by the institutional review board before the start of this study.
Informed Consent
Informed consent for the study was obtained from all participating patients in accordance with the World Medical Association Declaration of Helsinki.
Trial Registration
Not applicable.