
Abstract
Objective
Inlay arthroplasty (IA) has seen growing interest as a new primary arthroplasty intervention for patients that need to transition from biology to joint replacement. The purpose of this study was to investigate the biological response to this procedure.
Design
Patients presenting with symptomatic mono- or bicompartmental arthrosis and varus malalignment underwent IA and concurrent medial open wedge high tibial osteotomy (HTO). A subset of patients required hardware removal and consented to second-look arthroscopy without biopsy allowing for assessment of IA components and compartment-specific findings related to implant fixation, cartilage flow, propagation of lesions, and opposing tibial surfaces.
Results
In a series of 41 knees (35 patients) treated with combined IA and HTO (mean varus >7°), 26 knees (23 patients, 18 male, 5 female) with a mean age of 52 years (range = 43-67) required HTO plate removal. Concurrent second look arthroscopy was performed at a mean of 14 months (range = 12-19) following the index procedure. On probing, all arthroplasty components showed solid fixation without gap formation. On the medial femoral condyle, 15 mm implants (n = 14) showed a peripheral cartilage flow of 12% (range = 5% to 25%), 20 mm implants (n = 12) of 9% (range 5% to 15%), and trochlear implants (n = 12) of 20% (range 10% to 40%). No progressive deterioration of the index defects or progression of tibial and retropatellar grades were seen.
Conclusion
Joint surface reconstruction using IA showed stable fixation with peripheral cartilage coverage ranging from 9% to 20% and no further chondral damage on opposing surfaces. Future clinical effectiveness studies are required to support the positive biological integration.
Introduction
Painful and disabling focal cartilage defects (FCDs) are most common in middle aged (40-60 years) and active patients1-4 and are a challenging problem for orthopedic surgeons. FCDs that may occur as the result of a single traumatic incident have very limited healing potential, are symptomatic, and if left untreated may progress to degenerative arthritis.5-7 This could result in serious progressive pain with limitations in sports and activities of daily living, eventually leading to a loss of quality of life.3,4,6-9
The treatment of symptomatic FCDs is composed of various options and is usually directed by the patient’s age, location and size of the lesion, and the presence of any joint deformity.3,4,6-8,10-14 As a first-line treatment, conservative therapy composed of analgesics combined with physical therapy may suppress the symptoms until surgical treatment is warranted. Biological techniques to repair the chondral defects including OATS (osteochondral autograft transfer system), mosaicplasty, autologous chondrocyte implantation, marrow stimulation techniques including abrasion chondroplasty, and microfracture have been reported to be increasingly ineffective in middle-aged to older patients and are better suited for younger patients.5,12,14,15,16 Unicompartmental or total knee arthroplasties should be reserved as a last resort in younger patients due to the associated morbidities and the high risk of revision surgery.1,4,7,17-20
There appears to be a need for an interim treatment for patients with Grade IV FCDs until a total or unicompartmental arthroplasty becomes feasible for them. Inlay arthroplasty (IA) is a promising new direction in primary joint replacement as it allows for contoured and patient-specific defect coverage, while preserving healthy bone, cartilage, and soft tissues.1,4,21 Compared with traditional replacement procedures, IA avoids excessive bone resection and reapproximation of joint height and contour by utilizing healthy cartilage margins as a reference for location-specific reconstruction.1,4,21 A basic science report by Kirker-Head et al. 4 described cartilage confluence over the edge of inlay components in a goat model. Markarian et al. 22 published the first case report on the second look of 4 patients treated with IA demonstrating effective defect fill and rim off-loading.
The aim of this study is to present the results from second-look arthroscopy providing insight into the biological incorporation of these implants and their effects on opposing surfaces in patients who underwent IA combined with medial open wedge high tibial osteotomy (HTO).
Methods
This study was approved by the institutional review board. Forty-one knees in 35 patients, with varus alignment of more than 7°, had been previously treated for symptomatic mono- or bicompartmental arthrosis with IA and concomitant HTO.
The rational to perform the combined procedure was to address the cartilage defect in the medial compartment using IA while correcting the mechanical malalignment with HTO avoiding overcorrection and associated risks. HTO plate removal due to pes anserinus irritation was performed at a mean of 14 months (range = 12-19) following the index procedure in 26 knees of 23 patients (18 male, 5 female). Second-look arthroscopy of the implants was performed at that time. The mean age of these patients was 52 years (range = 43-67). Fourteen of these knees had a 15 mm implant while 12 had a 20 mm implant on the medial femoral condyle. Twelve of the 26 knees had bicompartmental arthrosis and had also received a patellofemoral IA. None of the knees had International Cartilage Research Society (ICRS) Grade IV lesions on the opposing sites (medial plateau and patella) and no inlay all-polyethylene resurfacing part of the implant system was applied. During the initial resurfacing procedure, opposing cartilage surfaces were graded as ICRS Grade I in 6, Grade II in 16, and Grade III in 4 medial tibial plateaus. The retropatellar surface was Grade I in 8, Grade II in 3, and Grade III in 1 patient who had concomitant trochlear resurfacing.
Index Surgical Procedure
Patients were previously treated with the HemiCAP Knee System (Arthrosurface, Franklin, MA). This system consists of a cobalt chrome articular component that mates with the fixation component by means of a Morse taper. The IA technique is performed through a mini open parapatellar incision exposing the defect and placing a guide wire into the center of the defect. The cannulated system follows the established perpendicular axis to the joint surface throughout the preparation and implantation steps. After the fixation component has been placed at the correct height, intraoperative mapping of the surface geometry was measured in 2 planes ( Fig. 1A ) and a corresponding surface reamer was used to prepare the implant bed ( Fig. 1B ). The implant gains its support via the fixation screw and subchondral bone bed. The HemiCAP was positioned subchondrally 0.5 mm below the level of osteochondral junction. All implants were checked intraoperatively, to confirm that none were above the level of the peripheral chondral tissue and recessed implantation was achieved. Effective coverage of the cartilage defects with appropriate sized and contoured implants was targeted and achieved. Following the resurfacing procedure, joint congruency was reviewed under fluoroscopy in the AP and lateral planes.
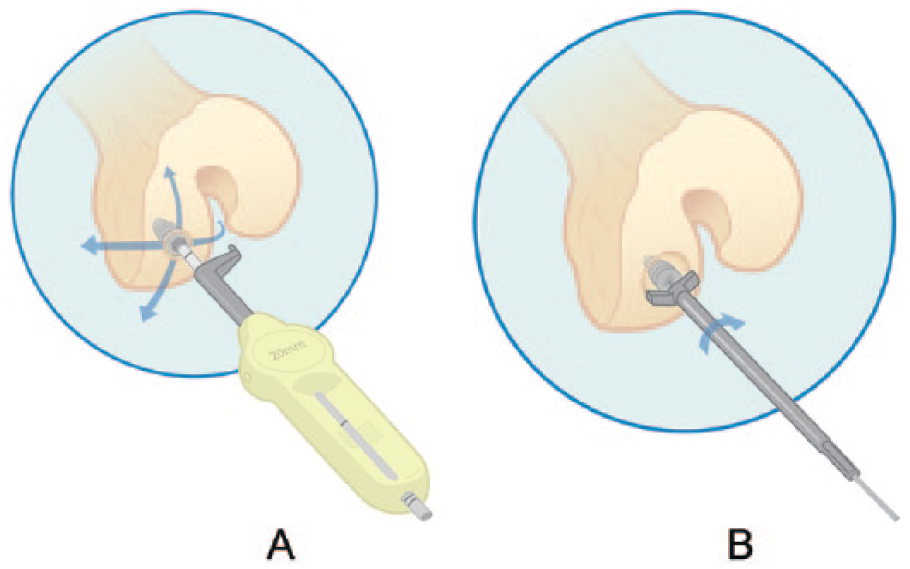
After the screw is placed at the correct height, the surface geometry is measured in 2 planes (
All patients had varus alignment greater than 7° of the proximal tibia, which was corrected with an opening wedge HTO to lateral mechanical axis deviation 0 to avoid the mechanical problems associated with overcorrection. Cartilage defect fill was effectively achieved using IA.
Second-Look Arthroscopy
All patients gave informed consent for a diagnostic arthroscopy without biopsy to evaluate implant stability, cartilage rim, and the ratio of implant surface coverage with cartilage flow. All implants were probed during arthroscopy for stability and gap formation. Opposing native articular surfaces were assessed. The cartilage coverage over the implant was measured from the superior, inferior, medial, and lateral sides of the implant with the tip of a 5 mm arthroscopic examination probe.
Results
All implants were found to be stable with no mechanical loosening or gap formation and showed rigid fixation within the implant bed. Peripheral implant coverage with cartilage flow of the 15 mm implants was 12% (range = 5% to 25%), 20 mm implants showed 9% (range= 5% to 15%), and trochlear implants demonstrated 20% (range = 10% to 40%) cartilage flow over the implant ( Fig. 2 ). Articular cartilage staging was repeated at the time of second-look arthroscopy. Femoral index lesions covered by IA did not show any signs of progression; the tibial baseline articular cartilage stage remained unchanged for all Grade I, II, and III lesions.

Cartilage flow over the trochlear inlay arthroplasty implant.
Discussion
The most important finding of the study was the maintenance of opposing baseline articular cartilage stage at the time of second look confirming no deleterious effects of the contoured implant on the opposing surface. In addition, 9% to 20% coverage of the implants was found without no further degeneration of the index lesion.
Full-thickness FCDs (ICRS Grade IV) in middle-aged patients are usually symptomatic and cause significant impairment in daily activities especially for active patients.1,7,20,21,23,24 Conservative treatment measures including weight reduction, unloading braces, medications (usually nonsteroidal anti-inflammatory drugs) combined with physical therapy applied as the initial treatment method only suppress the symptoms with no additional benefit.3,5-7,10,25,27
If left untreated, these FCDs have been shown to progress, eventually causing increased contact pressure and degenerative joint disease in animal models and humans.9,19,21,26-28 Smaller FCDs were noted to have some capacity to heal on their own,21,27 whereas larger ones were shown not to possess such ability resulting in the collapse of subchondral bone together with the surrounding articular cartilage.15,21,27 Larger defects also have the tendency to affect opposing tibial chondral surfaces with progressive degeneration.1,3,5,9,13,19,27,29 Guettler et al. found that rim stress concentration became a factor for full-thickness osteochondral defects 10 mm (0.79 cm2) and greater in size. 19
Middle-aged patients with symptomatic FCDs seem to be caught in the middle between being too old for a successful result from biological cartilage repair or marrow stimulation solutions and being too young for conventional unicompartmental or total knee arthroplasty, which would subject them to a high risk of complications or revision.1,4,21 Biological cartilage repair treatments were shown to have inferior results in middle-aged or active elderly patients with FCDs.1,6,12,16,20,24,27,28,30-32 de Windt et al. 6 in their study to determine the prognostic factors for the successful treatment of cartilage defects stated that patients aged over 30 years were associated with failure or inferior results. This was confirmed by Levy et al. 14 In a randomized trial comparing the results of autologous chondrocyte implantation to microfracture, Knutsen et al. found that patients younger than 30 years had a significantly better clinical follow-up than older patients, regardless of the treatment. 12 They stated that in patients over 40 years, microfracture treatment showed a significant deterioration in outcome scores and a decrease in function 32 between 18 and 36 months after the procedure; Steadman et al. stated that when compared with younger patients, microfracture in patients between 35 to 45 years of age provided significantly inferior results. 20
Several studies have reported that in order to preserve healthy bone, cartilage, and soft tissues, conventional unicompartmental or total knee arthroplasty should be avoided in middle-aged patients with symptomatic FCDs.4,10,19,21,23,30 Inlay arthroplasty is a novel reconstructive treatment option that allows the filling of the FCD with precisely sized implants that match the contour of the articular cartilage creating a smooth, continuous joint surface. Thus, healthy cartilage, bone, and soft tissues are preserved. A study conducted by Becher et al. 1 showed that, after IA, the majority of patients showed clinically significant improvements with great safety. This study was very promising; however, the question of cartilage coverage and possible chondral damage was still unanswered.
Second-look arthroscopies performed in our study showed a 9% to 20% coverage of the implant with cartilage tissue. Early reports of cartilage flow were basically ignored as it was felt that defects could not regenerate.33,34 This phenomenon was first described by Calandrucci and Gilmer in 1962, 35 and then reported by Ghadially and Ghadially in 1975 33 and Bruns et al. in 1997. 34 Kirker-Head et al. 4 in their basic science study in the goat model showed that the IA implant and the technique were highly efficient with no adverse effects after 1 year of follow-up. According to their histological data, the implant became solidly integrated into the medial femoral condyle with new bone abutting both the anchor and resurfacing components and cartilage flow over the interface of the implant and surrounding cartilage extending into the superficial zone.
Kirker-Head et al. 4 found no ongoing degenerative joint disease apparent 1 year after IA. Some chondral and meniscal damage on the proximal tibia of the operated joints, however, was found in both the operated and unoperated groups. The animals returned very rapidly to weight-bearing with excellent range of motion, which they considered a functional success. They concluded that the treatment is safe and biocompatible. 4
In the latest study by Markarian et al., 22 4 patients had a second-look arthroscopy performed 2 to 25 months post IA for reasons not related to the implant. They observed a 1- to 10-mm cartilage flow across the prosthetic edges. Histological specimens showed hyaline characteristics of the cartilage flow in the femoral condyle with solid fixation into the surrounding tissue while radiographs showed no indication of periprosthetic radiolucency, subsidence, or disassembly in any patient.
Becher et al. stated in their biomechanical study on human cadavers with FCDs that flush implantation showed no statistical increase in peak contact pressures compared with untreated knees. 21 However, they found that 1-mm proud implants increased the peak contact pressures significantly by 217%. Our observations confirm that recessed implantation of IA components results in a favorable biological response covering the implant-cartilage interface.
We have presented the results of our second-look arthroscopies reporting the amount of cartilage coverage over the IA implant. Our study provides further evidence on the reaction of adjacent chondral tissues toward these implants and their effects on opposing tibial sided surfaces in humans. In this study, we have shown that cartilage flow over the implants ranged from 9% to 20% at 14-month follow-up. We have also noted that the corresponding tibial surfaces showed no deleterious effects from implantation.
A limitation of the study was the lack of tissue biopsies covering the implant for histological evaluation. We felt it was important to leave the cartilage intact and we did not obtain patient consent for further analysis.
Conclusion
This study shows that after IA implant cartilage coverage ranging from 9% to 20% can be observed with no chondral damage to the opposing tibial surface. IA appears to be a safe and effective interim solution for middle-aged patients with symptomatic full-thickness (ICRS Grade IV) single focal cartilage defects.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Halic University, Clinical Investigations Ethics Commitee, Approval Number:17
Informed Consent
Written informed consent was obtained from all subjects before the study.