
Abstract
Objective
There is scant research examining the prevalence of thinness in early childhood, despite its potential negative consequences for health and development across the life course. The objective of this study was to assess bone status through measurement of bone mineral density and biochemical bone turnover markers, with special attention paid to carboxylated (c-OC) as well as undercarboxylated (uc-OC) forms of osteocalcin, in the groups of thin and normal-weight children.
Design
The study included 80 healthy prepubertal children (median age 7.0 years), who were divided (according to Cole’s international cutoffs) into 2 subgroups: thin children (n = 40, body mass index [BMI] = 13.5 kg/m2) and normal-weight children (n = 40, BMI = 16.1 kg/m2). Bone mineral density (BMD) and bone mineral content (BMC) were assessed by dual-energy x-ray absorptiometry method. Serum concentrations of C-terminal telopeptide of collagen type I (CTX), total osteocalcin (OC), and c-OC, and uc-OC forms of osteocalcin were determined using enzyme-linked immunosorbent assays.
Results
In thin children, we observed higher levels of bone resorption marker CTX compared with normal-weight peers. Total osteocalcin concentrations were comparable in both groups of children; however, in thin children we observed higher median values of uc-OC (34.40 vs. 29.30 ng/mL, P < 0.05) and similar c-OC levels (25.65 vs. 28.80 ng/mL). The ratio of c-OC to uc-OC was significantly lower (P < 0.05) in thin than in normal-weight children. Total BMD and BMC were significantly decreased (P < 0.0001) in thin children compared with normal-weight peers (0.724 ± 0.092 vs. 0.815 ± 0.060 g/cm2 and 602.7 ± 159.2 vs. 818.2 ± 220.1 g, respectively).
Conclusion
Increased concentrations of CTX and uc-OC might lead to disturbances in bone turnover and a decrease in bone mineral density in thin children.
Keywords
Introduction
Mesenchymal stem cells possess an extensive potential to proliferate and differentiate, for example, into osteoblasts, osteocytes, adipocytes, and chondrocytes. Chondrocytes are cells that maintain cartilage, while osteoblasts as well as osteocytes maintain bone. They both originate from mesenchymal stem cells, which show great potential for cartilage structure and bone tissue architecture. 1 Measurements of bone mineral density (BMD) using densitometry techniques are recognized as a gold standard of assessing bone status; however, these measures do not reflect the dynamic of bone turnover. Biochemical markers, which show global skeletal activity, were validated for the assessment of bone formation and bone resorption processes. 2 Among them, C-terminal telopeptide of collagen type I (CTX) and osteocalcin (OC) are considered to be clinically useful. CTX is an epitope, consisting of 8 amino acids (Glu-Lys-Ala-His-Asp-Gly-Gly-Arg). It is liberated into the bloodstream during degradation a molecule of collagen and was proven to be a sensitive marker of bone resorption. 3 OC, which was the first protein to be identified as bone specific, is synthesized by bone cells osteoblasts during the mineralization phase of osteogenesis and accumulates in the bone matrix. A small amount of OC, which is released into the circulation, is important for the biochemical measurements. Serum level of OC is used as a sensitive marker of bone formation. OC has 3 potential γ-carboxyglutamic acid residues that are responsible for the binding of OC to hydroxyapatite.4,5 The posttranscriptional modification of glutamic acids catalyzed by γ-carboxylase requires vitamin K as a cofactor. OC may exist in 2 forms: carboxylated OC (c-OC), which is fully carboxylated osteocalcin and undercarboxylated (uc-OC) osteocalcin, in which 0 to 2 residues were carboxylated. 6 Carboxylated osteocalcin binds to hydroxyapatite in bone and plays a regulatory role in bone formation and mineralization. uc-OC plays an active role in glucose homeostasis and additionally is recognized as a functional marker of vitamin K status.7,8 Despite many biological and clinical studies, specific functions of OC and its forms remain unclear.
It is known that not only vitamin K but also vitamin D and mineral elements (calcium, phosphorus) are essential for organic bone matrix synthesis. Recent studies show that manganese plays a significant role in the biosynthesis of chondroitin sulfate, which comprises the most important step in cartilage structure. It was reported that skeletal abnormalities, such as osteoporosis, and congenital disorders of skeleton including chondrodystrophy were significantly linked to prolonged deficiency in manganese concentrations. 9 Since vitamin D receptors are found in human chondrocytes, it is suggested that vitamin D may directly affect cartilage and bone biology. 10
Serum levels of bone turnover markers are not stable throughout life and are greater in infants and children than in adults.3,11 Many factors influence bone markers levels, such as age, gender, pubertal stage, and hormonal and nutritional status. The widespread applicability of bone metabolism markers is limited by the availability of normative data. Contrary to adults, children have increased bone markers concentrations due to their skeletal growth velocity and high rate of bone turnover.12,13 There is scarce information about bone markers, especially about concentrations of c-OC and uc-OC in pediatric population.
It is known that both extremes of the spectrum of weight, from obesity to underweight, may have serious health consequences for the individuals. 14 Studies on obese patients and at the opposite end of the weight spectrum patients with anorexia nervosa, have shown associations between body mass and bone status.15-17 In adults low body weight predicts low bone mineral density and is a risk factor for fracture. 18 There are only a few reports assessing BMD and bone turnover markers in thin children.19-21 It is an important problem, because the prevalence of thinness among children, especially girls has increased according to data from several countries.
The aim of this study was to assess bone status through measurement of bone mineral density and biochemical bone turnover markers, with special attention paid to c-OC and uc-OC, in thin and normal-weight children.
Methods
Participants
The study included healthy prepubertal children (median age 7.0 years), recruited between January 2014 and April 2016 from a group of consecutive patients attending the Gastroenterology Clinic at the Institute of Mother and Child in Warsaw (Poland). Children participating in this study were well-nourished, without endocrine disorders or genetic syndromes and without diseases that could affect nutritional status, growth, and pubertal development. None of the children was taking bone sparing drugs, or experienced any bone fractures and they were all on unrestricted diet. Pubertal stage was assessed according to the Tanner criteria. The subjects were divided into 2 groups: thin (mean body mass index [BMI] = 13.5 kg/m2) and normal-weight (mean BMI = 16.1 kg/m2) children according to Cole’s international cutoffs. 22 They have extended the adult term of thinness to children. The international BMI cutoffs in adults allow distinctions between different grades of thinness: grade 1 (17 to <18.5 kg/m2, mild thinness), grade 2 (16 to <17 kg/m2, moderate thinness), and grade 3 (<16 kg/m2, severe thinness). These criteria correspond to appropriate cutoff points for BMI for thinness grades 1, 2, and 3 for exact ages in boys and girls. Normal-weight group consisted of children with BMI, which corresponds to 18.5 kg/m2 or higher in adults. Underweight or obese children were excluded from this study.
This study was approved by the Ethics Committee at the Institute of Mother and Child in Warsaw. Written informed consent was obtained from the parents of all examined children.
Procedure
Anthropometric measurements such as body height and weight were performed and BMI was calculated as body weight (kg) divided by height squared (m2). Bone mineral content (BMC) and BMD in the total body and in the lumbar spine were measured by dual-energy x-ray absorptiometry (DXA) using Lunar Prodigy (General Electric Healthcare, Madison, WI). We obtained BMD z-scores using pediatric reference population database enCORE software version 9.30.044, which allows the use of nationality-based reference data. This database are supported by studies conducted at university medical centers and clinics in the United States, Australia, and Europe (Germany, Finland, Sweden, Russia, Spain, Netherlands, and Poland) on population of healthy girls and boys from 5 to 19 years. The subject’s BMD is compared with the average BMD of a reference group of the same age, sex, and ethnicity.
For biochemical analyses, venous blood was taken in the morning hours after an overnight fast. Serum samples were collected after centrifugation (1000 × g for 10 minutes at 4°C) and were stored at −20°C until biochemical assay (no longer than 2 months). Concentrations of bone metabolism markers were determined by commercial enzyme-linked immunosorbent assay (ELISA). Serum OC and CTX concentrations were measured by kits from IDS (Boldon, UK). The intra- and interassay coefficients of variation (CVs) were 1.3% to 2.2% and 2.7% to 5.1% for OC and 1.7% to 3.0% and 2.55 to 10.9% for CTX, respectively. Levels of carboxylated and undercarboxylated forms of osteocalcin in serum were measured by commercial kits from Takara Bio Inc. (Shiga, Japan), which had intra- and inter-assay CVs of 3.0% to 4.8% and 0.7% to 2.4% (c-OC) and 4.4% to 6.6% and 5.6% to 9.8% (uc-OC), respectively.
Statistical Analysis
Statistical analyses were performed using the Statistica software program, version 10.0 PL. Normality of variables was performed by Shapiro-Wilk test. The symmetrically distributed data are expressed as mean ± standard deviation (SD) and the asymmetrically distributed as median with 25th and 75th percentiles. Student’s t test was used to calculate differences between means and the Mann-Whitney U test was used to compare asymmetric variables. Pearson’s or Spearman’s rank correlation test was used to evaluate the possible relationships between various parameters. The statistical significance was set at P < 0.05.
Results
In total, 80 children aged 5 to 10 years were recruited to this study. Among them, the group of thin children consisted of 40 subjects (21 girls and 19 boys, median age 6.8 years) and group of normal-weight children consisted of 40 subjects (19 girls and 21 boys, median age 6.6 years). In our studied group of children there were no significant differences in birth weight, Apgar score, gestational age, or maternal age at birth. In the group of thin children, we assessed mild thinness (grade 1) in 29 (72.5%), moderate thinness (grade 2) in 8 (20%), and severe thinness (grade 3) in 3 (7.5%) children. The data on children’s characteristic and anthropometry are presented in Table 1 . Generally, the growth and development of all children was correct and there were no significant differences in body height between thin and normal-weight children. However, thin subjects had significantly lower (P < 0.0001) body weight and BMI. The median values of total BMC and spine BMC were significantly decreased in the group of thin children compared with the normal-weight group (P < 0.0001 and P < 0.001, respectively). Total and lumbar spine BMDs as well as z-scores BMD and BMD L2-L4 were significantly lower in thin children compared with normal-weight peers.
Children’s Characteristics and Anthropometry. a
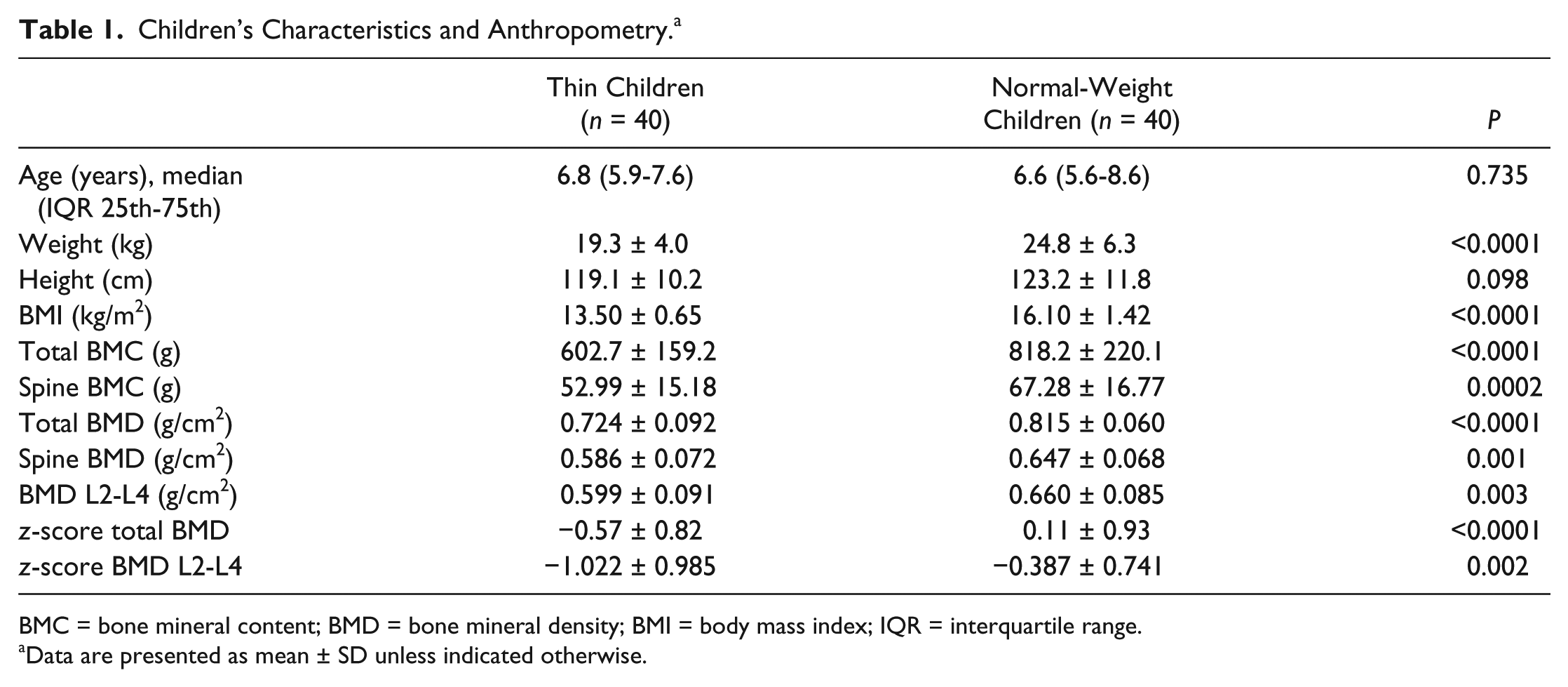
BMC = bone mineral content; BMD = bone mineral density; BMI = body mass index; IQR = interquartile range.
Data are presented as mean ± SD unless indicated otherwise.
According biochemical bone turnover markers, we observed higher serum CTX levels in the group of thin children than in normal-weight peers and comparable concentrations of total OC and c-OC ( Table 2 ). However, in thin children, we noticed higher (P < 0.05) median values of uc-OC. Hence the ratio of c-OC/uc-OC was lower (P < 0.05) in thin than in normal-weight children. Additionally, the ratio of c-OC to total OC was similar in both groups of children, but the ratio of uc-OC to total OC was significantly higher (P < 0.05) in thin than in normal-weight subjects (0.489 vs. 0.305). The ratio of OC/CTX was slightly lower in thin subjects, but this difference was not statistically significant.
Serum Concentrations of Biochemical Bone Metabolism Markers in Thin and Normal-Weight Children. a
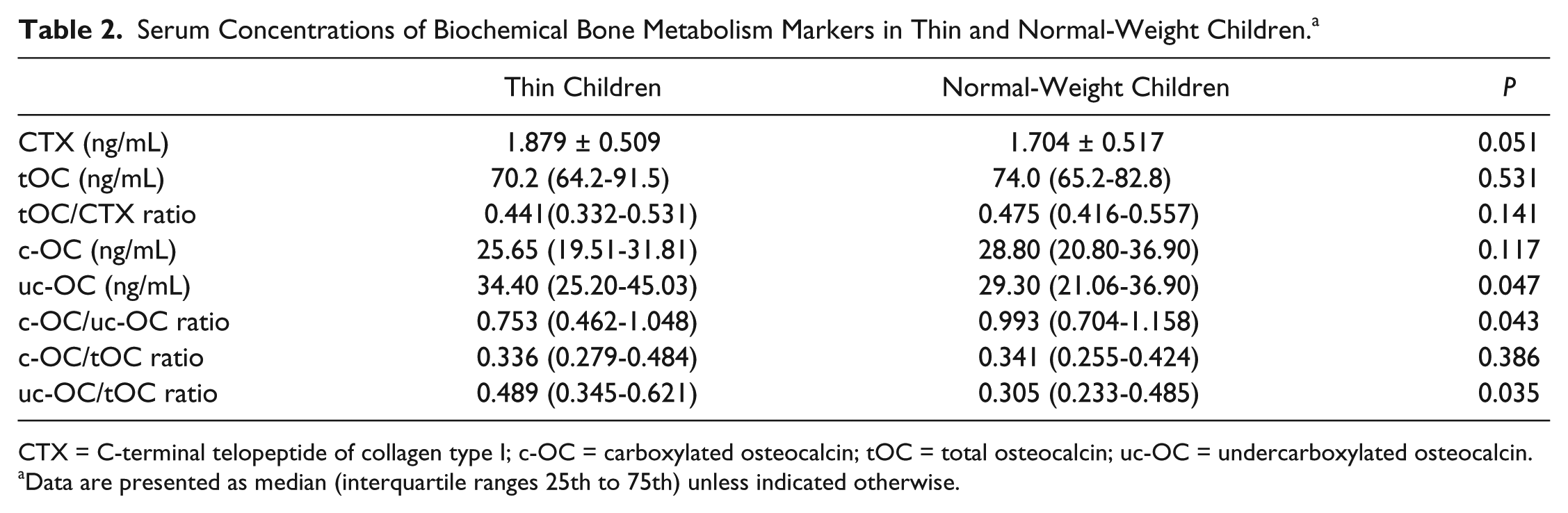
CTX = C-terminal telopeptide of collagen type I; c-OC = carboxylated osteocalcin; tOC = total osteocalcin; uc-OC = undercarboxylated osteocalcin.
Data are presented as median (interquartile ranges 25th to 75th) unless indicated otherwise.
As expected, in both groups of children we found positive correlations between BMI and BMC (P < 0.001) and between BMI and BMD (P < 0.05). In Table 3 , we present correlations between bone turnover markers (OC and CTX) and anthropometric as well other biochemical parameters. Serum levels of OC was positively correlated with body weight (P < 0.05) and height (P < 0.01) in both groups of children and additionally with CTX (P < 0.05) and uc-OC (P < 0.001) but only in thin children. In the group of normal-weight children we found positive correlation between serum CTX concentration and body weight and height as well as between CTX and spine BMC. We did not found such relations in the group of thin children. In addition, we did not observe correlations between the ratios of OC/CTX and c-OC/uc-OC and anthropometric and other biochemical parameters in any of the studied groups of children.
Correlations Between Serum Bone Turnover Markers (OC, CTX) Concentrations and Anthropometric as Well as Other Biochemical Parameters in Thin and Normal-Weight Children.
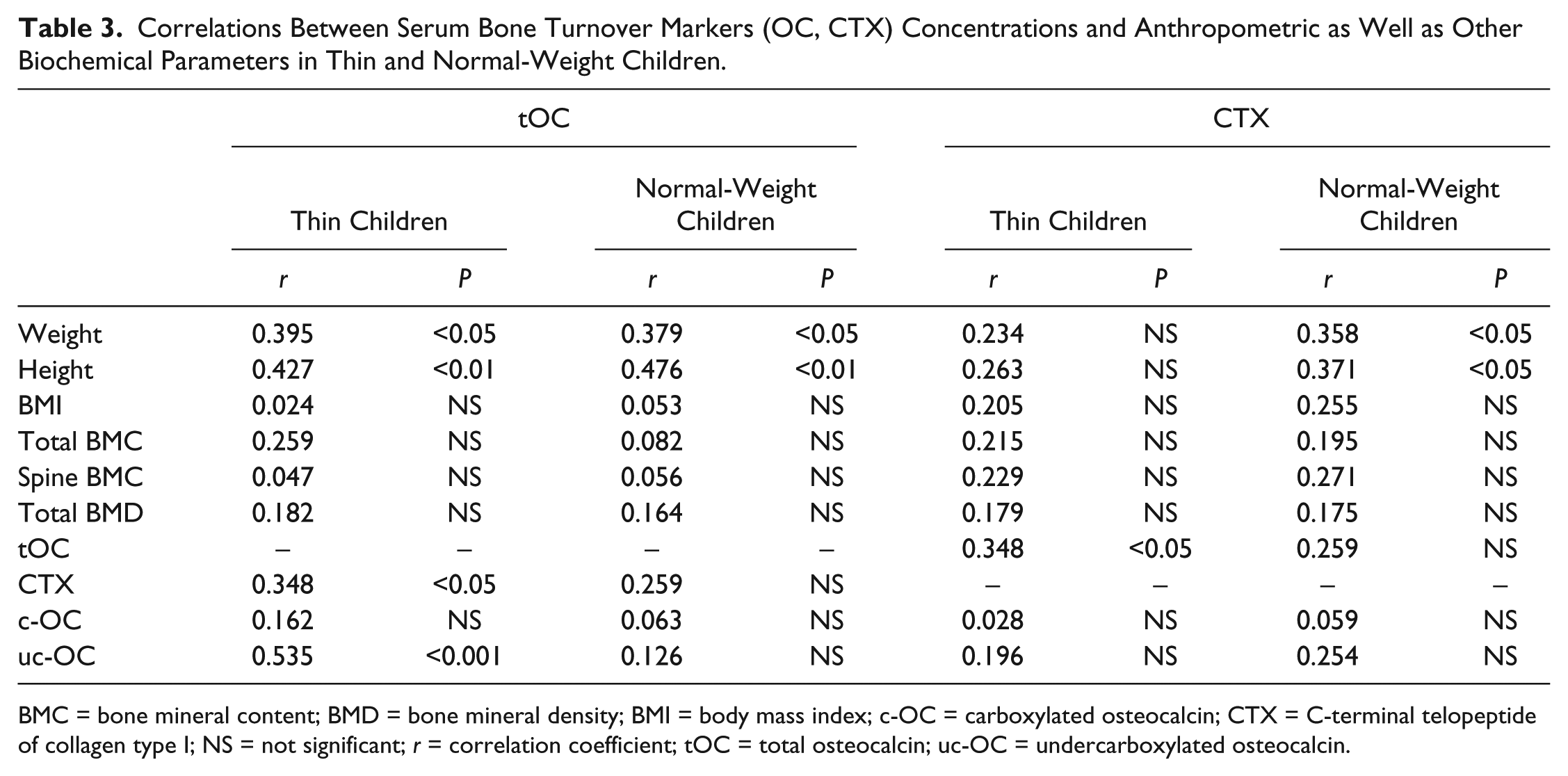
BMC = bone mineral content; BMD = bone mineral density; BMI = body mass index; c-OC = carboxylated osteocalcin; CTX = C-terminal telopeptide of collagen type I; NS = not significant; r = correlation coefficient; tOC = total osteocalcin; uc-OC = undercarboxylated osteocalcin.
Discussion
According to our study, thin children had decreased BMC and BMD, and we suggest that these deficits may be the effect of increased resorption and less effective bone formation. Since childhood and adolescence are known a crucial periods for skeletal growth, it is important to monitor body weight and BMD during these periods to achieved optimal peak bone mass. According to Lee et al., 23 longitudinal BMD loss was significantly associated with loss of cartilage volume and loss of tibial cartilage thickness.
In the literature there are many studies presenting the prevalence of childhood thinness, including severe thinness in low-income countries.24-26 In developed European countries, thinness has been reported to range from about 5% to 12% among girls, and 3% to 9% among boys.27-30 In Poland, depending on the standard used, the prevalence of thinness was diagnosed in about 6% of boys and 11% of girls 31 or according to the OLAF study in 10% of boys and 13% of girls. 32 Clinical studies conducted in Australia, demonstrated that thin school children might be less muscular, weaker, and less active than healthy-weight peers 33 but the risk of developmental vulnerability among thin and normal-weight children generally did not differ in studied population. 34 Children with low body weight might be predisposed to low bone mass and disturbances in bone turnover. Our previous study 35 as well as the observations of other authors support the hypothesis that in thin children a close association between body weight and BMD occurs.20,21 Moreover, bone status during childhood might be a strong predictor of bone status in young adulthood, when peak bone mass is achieved. 36
In the present study, the group of thin children had decreased values of total BMC, total BMD, and lumbar spine BMD compared with the normal-weight group. Also, z-scores BMD and BMD L2-L4 were significantly lower (P < 0.0001) in thin children than in normal-weight peers. In both groups of children BMC and BMD were positively correlated with body weight, body height, and BMI. Vaitkeviciute et al. 19 observed that underweight 12-year-old boys had significantly lower body mass, BMC, and BMD compared with normal-weight boys and suggested that being an underweight boy at baseline is related to higher chance (P < 0.01) of lower total BMD in the future (2 years at follow-up) development compared with normal-weight boys. Du et al. 21 reported lower bone age, BMC, and BMD in group of 12- to 14-year-old thin girls. The authors suggested that primary health care and appropriate interventions (nutrition, physical activity, and supplementation) need to be implemented among thin children to improve their growth and bone health.
Results concerning biochemical bone turnover markers in thin children are limited. In the present study, we observed higher serum CTX level in thin children than in normal-weight peers and comparable concentrations of total OC. Chen et al. 37 reported that increased bone resorption may have an influence not only on alteration in bone structure but also on articular cartilage damage. There is little information about serum levels of c-OC and uc-OC forms in children. We assessed for the first time serum levels of carboxylated and undercarboxylated osteocalcin in prepubertal thin children. We observed similar concentrations of serum c-OC in both groups of children, but significantly higher median value of uc-OC in thin children. Moreover, the ratio of c-OC to uc-OC was significantly lower in thin than in normal-weight children. Only a few authors assessed OC forms in children.38,39 Tubic et al. 38 analyzed total OC and its forms in normal-weight and overweight Swedish 2- to 9-year-old children. They found no difference for total OC and for uc-OC between normal and overweight groups, but significantly lower c-OC level in overweight subjects than in the controls. Additionally, the authors noted a trend of higher uc-OC value in overweight subjects, but these differences were not statistically significant. Prats-Puig et al. 39 determined 103 healthy Spanish children aged 6.6 years and found weight-dependent association between different forms of OC. Similarly to us, the authors observed higher uc-OC to c-OC ratio in leaner children than in the heavier ones. They found independent association between c-OC (active form in the bone) and both BMI and adiponectin, which suggests that carboxylation of OC affects regulation of bone mass by adipokines in healthy children. We did not observe correlations between biochemical bone metabolism markers and BMC as well as BMD, but in both groups of studied children serum levels of total OC were positively correlated with body weight and height. Additionally, concentration of OC correlated with levels of CTX and uc-OC, but only in thin children. Similar to us, Tubic et al. 38 noticed that in normal-weight children total OC as well as its forms did not correlate with BMC and BMD values.
There are many studies describing low BMD related to low body weight in adults, especially in postmenopausal women and in patients with anorexia nervosa or constitutional thinness.40-44 In young women with constitutional thinness (who had low BMI, but close to normal body composition, physiological menstruation, no hormonal abnormalities, no identified eating disorders) BMD positively correlated with BMI and they had significantly (P < 0.0001) lower total and lumbar spine BMD than normal-weight women. 43 About 44% of subjects with constitutional thinness presented tosteopenia, but theirs bone turnover was balanced with normal bone formation (levels of OC) and bone resorption (levels of CTX). Among patients with anorexia nervosa, about 50% presented osteopenia. Conversely with constitutional thinness, anorectic subjects had lower OC levels and higher CTX, which suggested uncoupling bone turnover. 42 Ravn et al. 40 reported than postmenopausal women with low BMI exhibit low bone mass (about 12%) and rapid bone loss because of higher bone turnover (higher levels of N-terminal telopeptide and OC), both of which are independent contributing factors to an increased risk of osteoporosis. In adults, Luukinen et al. 45 observed slight decrease in the c-OC to total OC ratio with advancing age and suggested that high proportions of uc-OC to total OC were associated with the occurrence of fractures in elderly life. In our children, the ratio c-OC to total OC was similar in both groups, but the ratio of uc-OC to total OC was significantly higher in thin subjects (P < 0.05). The mechanism behind the influence of OC forms on increased fracture risk remains obscure. Low c-OC (possibly as a result of inadequate vitamin K status) may be an effect of a decrease in osteocalcin γ-carboxylation, and in consequence elevated proportion of uc-OC. Also, Gundgerg et al. 6 found that high percentage of uc-OC was associated with greater risk of low BMD. Longitudinal and larger studies are needed to further explore the precise roles of different forms of OC in relation to different BMIs not only in adults but also in children of different ages. We suggest that the ratio of c-OC to uc-OC might be one of the indicators of early disturbances in bone metabolism.
Limitations
This study is not without limitations. First of all, our analyses were limited to children who had both anthropometric (densitometry) and biochemical data measured at the same time. That is why our sample size was relatively small, which lacks sufficient power to detect moderate associations with statistical significance. However, the studied group was homogeneous, all children were Caucasian comparable in age, lived in an urban area and of a similar socioeconomic status. Second, we lacked a detailed nutritional and physical activity data for the studied children. However, all the children were healthy, without eating disorders and remained on a traditional mixed diet. We assessed BMI status, which reflects whether the child’s diet had been meeting their nutritional needs for an extended period of time. Some authors suggested that BMI is easier to collect and analyze than other techniques for measuring the intakes of individual nutrients, such as a 24-hour dietary recall. 37 Third, we detected only 2 of bone turnover markers: CTX and OC, but we assessed the ratio of OC/CTX, which gives information about the balance between bone resorption and bone formation processes. Additionally, we determined not only concentration of total osteocalcin, but for the first time also serum levels of c-OC and uc-OC in thin children.
Future research with other novel bone turnover markers is necessary to understand the regulation of bone formation and resorption processes, such as OPG/RANK/RANKL (osteoprotegerin/receptor activator of the nuclear factor κB/receptor activator of the nuclear factor κB ligand) and Wnt/β-catenin (wingless-type signaling β-catenin-dependent) pathways.
Sclerostin (involved in Wnt/ β-catenin pathway) is a small protein expressed by the SOST gene in osteocytes that plays an important role in the regulation of bone remodeling. Recent studies have shown that the SOST gene is also expressed by articular chondrocytes and that modulation of its activity might have effects on articulate cartilage. 46
Conclusion
Our findings demonstrate that as early as in prepubertal age thinness exhibits a decrease in bone mineral density and abnormal levels of bone turnover markers. Decreased BMC and BMD might be associated with higher CTX and uc-OC levels in thin children. Early recognition of underweight and the accompanying consequences on bone and cartilage metabolism are important for the optimization of bone mineral accrual and prevention of bone loss. It is important to protect not only bone but also cartilage structures by proper status of vitamins and minerals. We suggest that monitoring of BMD and biochemical bone metabolism markers might be tools in the diagnosis of bone loss in thin children and help to reduce the risk of osteoporosis in later life.
Footnotes
Authors’ Note
This research was performed at the Institute of Mother and Child in Warsaw, Poland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted with the principles of the Declaration of Helsinki and was approved by the Ethics Committee at the Institute of Mother and Child in Warsaw.
Acknowledgments and Funding
We gratefully acknowledge children and their parents for the contribution to this study. We thank the staff of the Department of Internal Medicine, Endocrinology and Diabetology at the Central Clinical Hospital of the Ministry of the Interior in Warsaw for their help in DXA measurements. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the parents of all examined children.