
Abstract
Objective
Focal chondral defects alter joint mechanics and cause pain and debilitation. Microfracture is a surgical technique used to treat such defects. This technique involves penetration of subchondral bone to release progenitor cells and growth factors from the marrow to promote cartilage regeneration. Often this results in fibrocartilage formation rather than structured hyaline cartilage. Some reports have suggested use of growth hormone (GH) with microfracture to augment cartilage regeneration. Our objective was to test whether intra-articular (IA) GH in conjunction with microfracture, improves cartilage repair in a rabbit chondral defect model. We hypothesized that GH would exhibit a dose-dependent improvement in regeneration.
Design
Sixteen New Zealand white rabbits received bilateral femoral chondral defects and standardized microfracture repair. One group of animals (n = 8) received low-dose GH by IA injection in the left knee, and the other group (n = 8) received high-dose GH in the same manner. All animals received IA injection of saline in the contralateral knee as control. Serum assays, macroscopic grading, and histological analyses were used to assess any improvements in cartilage repair.
Results
Peripheral serum GH was not elevated postoperatively (P = 0.21). There was no improvement in macroscopic grading scores among either of the GH dosages (P = 0.83). Scoring of safranin-O–stained sections showed no improvement in cartilage regeneration and some evidence of increased bone formation in the GH-treated knees.
Conclusions
Treatment with either low- or high-dose IA GH does not appear to enhance short-term repair in a rabbit chondral defect model.
Introduction
Structural integrity and continuity of articular cartilage is critical for maintaining homeostasis, and providing a low-friction surface for joint motion and load transmission. 1 Focal, full-thickness chondral defects alter normal mechanics,2,3 cause significant pain and discomfort, 4 and degradation of surrounding cartilage often ensues.5,6 The true prevalence of chondral defects is difficult to assess accurately, as many are asymptomatic, and as such are unreported. 4 However, an estimated 60% of knee arthroscopies yield some evidence of chondral defects, regardless of surgical indication.7-9
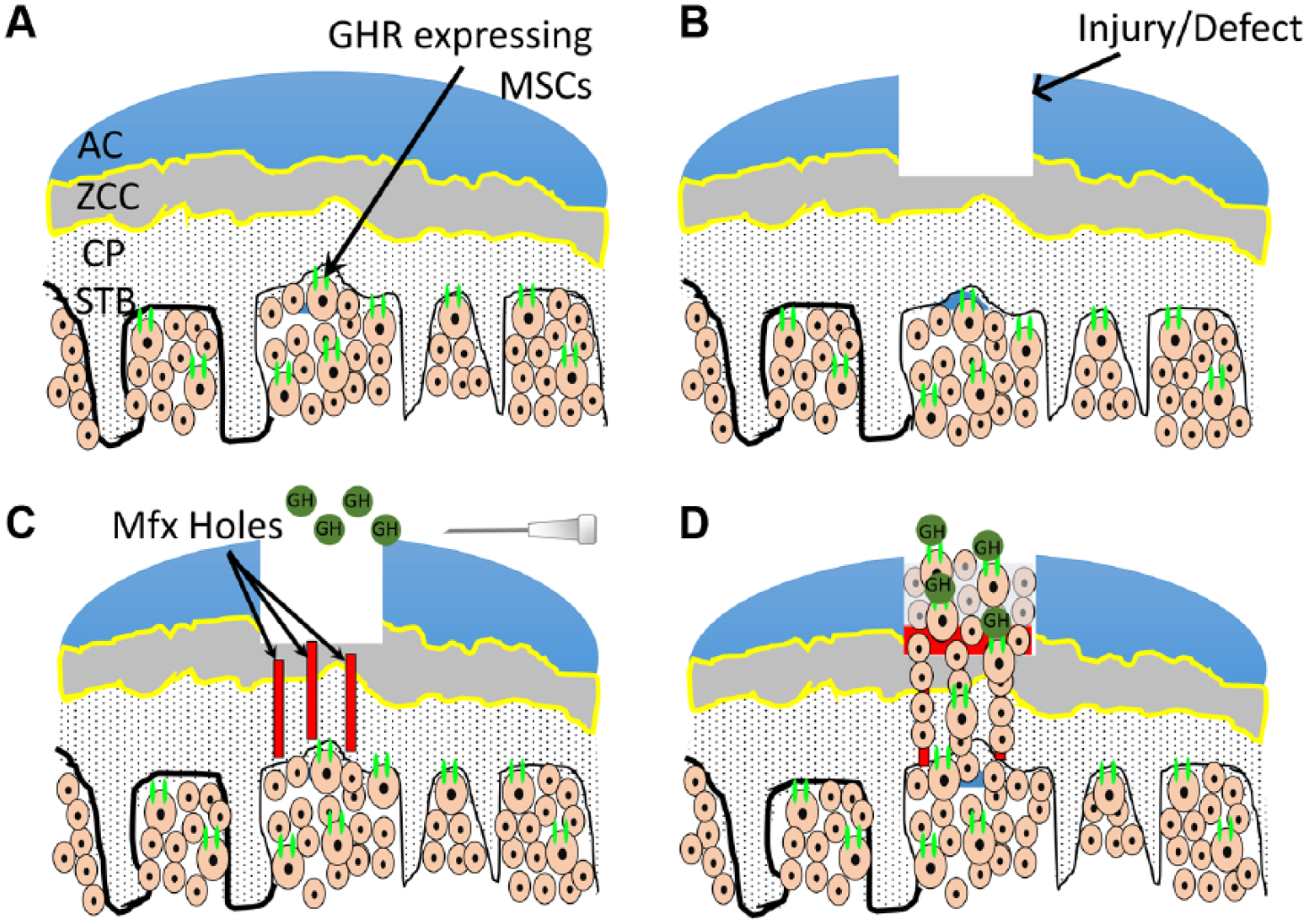
Surgical microfracture is a technique where a pointed awl is used to penetrate and deliberately breach the subchondral bone, which is typically exposed by injury, within the defect region. The newly created holes theoretically allow transport of blood, stem cells, and growth factors from the subchondral marrow into the defect site, to facilitate its repair and stimulate cartilage regeneration ( Fig. 1 ). This technique has been shown to increase cartilaginous coverage within the defect site, but the resulting tissue is often poorly organized fibrocartilage.10-12 Despite the relative inferiority of the replacement tissue in terms of microarchitecture and mechanical properties, 13 clinical investigations have shown some favorable pain scores and functional improvement.14-16 Nonetheless the long-term efficacy of the approach has been questioned, with some recent data demonstrating return of symptoms between 18 and 36 months postoperatively.15,17-19
(
Thus, in an effort to improve this outcome, complementary biological therapeutics are being investigated to determine whether their use, alone or in conjunction with microfracture, can improve cartilage regeneration in the treatment of chondral defects.20-26 Growth hormone (GH) is one such biological factor, which has potential to stimulate improved regeneration. GH has been shown to stimulate chondrocytes in culture27,28 and has been targeted for its potential role in early cartilage repair and osteoarthritis.29-31 Specifically, following intra-articular injection, GH has been shown to promote chondrogenesis, while inhibiting chondrocyte maturation and apoptosis.32-36 To better understand the mechanism by which GH might improve cartilage regeneration following microfracture, we aimed to use intra-articular delivery of GH at 2 dosage levels, in conjunction with microfracture, in a rabbit chondral defect model to determine its potential to improve cartilage regeneration.
Materials and Methods
Chondral Defect Model
This study utilized a validated rabbit chondral defect model, whereby a circular lesion is created in the articular cartilage on the medial femoral condyle, and microfractures are created within the defect to enhance repair. 26 Surgery was performed on skeletally mature New Zealand white rabbits (female, n = 16) according to our Institutional Animal Care and Use Committee (IACUC)–approved protocol. After the induction of anesthesia, both lower extremities were prepped with betadine and draped under sterile technique. A medial parapatellar approach to each knee was performed with a #15 blade, and the patella was dislocated laterally to allow full exposure of the articular surfaces. Using a standard dermal biopsy punch, a 4-mm full-thickness chondral defect was introduced on the weightbearing area of the medial femoral condyle. Curettage debridement was used to expose the underlying subchondral bone. Then, 3 microfracture holes in an inverted triangle configuration were created within the chondral defect using a small pointed awl. Bleeding from each hole was confirmed visually to ensure adequate penetration through the subchondral plate.
Following microfracture, the articular surfaces were irrigated with normal saline and the knee was extended to reduce the patella. The knee capsule was then tightly closed with simple interrupted 2-0 vicryl sutures. After capsular closure, the left knee was injected under direct visualization with 1 mL of sterile bovine growth hormone (Harbor-UCLA Medical Center, Torrance, CA) reconstituted in Hank’s buffer solution. Each knee was inspected to ensure that the injected fluid did not escape the knee capsule. 37 Eight rabbits were given a dose of 0.125 mg/kg (low-dose GH) by intra-articular delivery in the left knee, while the remaining animals (n = 8) received the higher dose 0.625 mg/kg (high-dose GH). Bovine GH has been used before for various applications in rabbit animals models, thus we selected this approach for our study.38-40 The right knee of each animal received delivery of Hank’s buffer solution to serve as a control (0 mg/mL of GH). Following the injection, the skin was closed with running subcuticular 4-0 monocryl sutures and Dermabond. Postoperatively, the animals were permitted to move freely within their cages. The procedures were performed over multiple days consistently between 7 AM and 12 PM to account for natural GH secretion, which is dependent on circadian rhythm.
Peripheral Blood Assays
In vitro studies have shown that GH acts relatively quickly, on the order of minutes, via activation of the JAK2-STAT signaling pathway. 41 However, to ensure our GH delivery did not immediately pass from the intra-articular space into the circulation, we assayed serum levels of GH, calcium, and glucose preoperatively, and at 1, 24, and 48 hours postoperatively to determine whether GH would enter systemic circulation after intra-articular delivery. Serum was isolated by centrifuging samples at 2200 rpm for 15 minutes and then frozen until testing. The level of GH was assessed using a commercial enzyme-linked immunosorbent bovine growth hormone (somatotropin) assay kit (ELISA, MyBioSource, MBS880082; San Diego, CA, USA). The sensitivity of this kit was 0.5 ng/mL, with a detection range of 2.5 to 80 ng/mL. No significant cross-reactivity or interference between this analyte and any relevant analogues was expected. Manufacturer quality controls showed that both intra-assay and inter-assay coefficient of variation was less than 15%. The levels of serum calcium and glucose were assessed by standard, commercial colorimetric assay kits (Abcam, ab102505 and ab65333; Cambridge, MA, USA).
Macroscopic Evaluation
After 12 weeks, rabbits were euthanized according to IACUC protocol and bilateral knees were harvested from each animal. Knees were fixed in 4% paraformaldehyde. Evaluation of gross morphological features of the chondral defect repair sites was carried out by 3 blinded and independent graders for each knee utilizing a modified component of the macroscopic cartilage repair score from O’Driscoll et al. 42 Briefly, this score specifically assesses 4 features of articular cartilage: coverage, neocartilage color, integration of defect margins, and surface smoothness. Each feature was scored from 0 to 4, for a maximum possible score of 16.
Histological Defect Repair Scoring
After macroscopic scoring, distal femurs were fixed in 4% phosphate-buffered formalin, trimmed, and decalcified in ethylenediamine tetraacetic acid and then processed and embedded in paraffin for histological evaluations. Paraffin-embedded coronal sections (5 µm; n = 9-11 per defect) were taken at the approximate center of the defect at standardized 200-µm intervals to avoid biased section sampling. Staining with hematoxylin and eosin and safranin-O staining was carried out according to routine histological protocols. The histology sections were blindly scored by one investigator, using a modified O’Driscoll scoring system. The individual components included the amount of hyaline cartilage present within the boundaries of the defect, the structural characteristics of regenerated cartilage, the bonding of the cartilage adjacent to the defect edges and the presence of any degenerative changes in cartilage adjacent to the defect.
Statistical Analysis
Descriptive statistics were initially calculated to visualize each data set. Wilcoxon rank sum tests were used to assess differences in serum parameters at each time point, and the same test was used to test differences between each treatment group at 12 weeks postoperatively.
Results
Overall, the surgical procedures were successful and well tolerated by all animals. With the exception of 1 animal, which died during surgery due to anesthesia-related complications and was excluded from the study, there were no other cases of post-operative complications.
Peripheral Blood Assays
Figure 2 demonstrates serum assay analyses for growth hormone, calcium, and glucose preoperatively and at 1, 24, and 48 hours postoperatively. Results of peripheral blood assays pre- and postoperatively show that GH was not increased systemically following intra-articular administration. In fact, there appeared to be a slight reduction from baseline in the 1 hour postoperative group, although this difference was not significant. In addition, there were no significant differences between baseline and 24- or 48-hour group’s postoperative GH levels. Similarly, postoperative levels of calcium were not significantly different between baseline and any of the postoperative time points, suggesting that calcium levels also remained unchanged. Finally, there was also no statistical difference between baseline glucose levels and levels at 1-, 24-, and 48-hour postoperative levels.
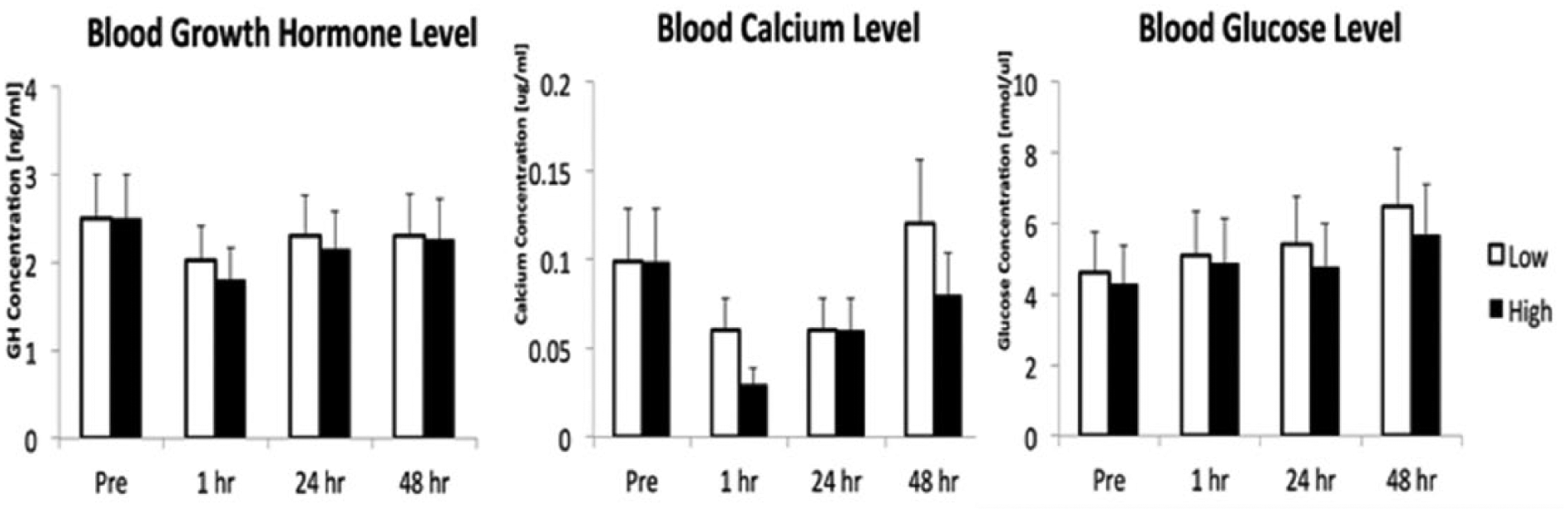
Serum assay data from analyses of growth hormone, calcium, and glucose (left to right) demonstrating the effect of low- and high-dose growth hormone (GH) on each substrate from the preoperative time point to 1, 24, and 48 hours postprocedure.
Macroscopic Evaluation
Figure 3A-C demonstrates representative images and scoring data of gross anatomical specimens for macroscopic assessment at 12 weeks postmicrofracture from control group, low-GH intra-articular treatment group, and high-GH Intra-articular treatment group, respectively. Figure 3D shows the mean macroscopic scoring values in each group. Assessment of the gross appearance of the articular cartilage defect sites revealed that the average score following treatment with low-dose GH was 10.2 ± 3.8 compared with 9.8 ± 3.3 in contralateral control knees. Treatment with high-dose GH resulted in an average macroscopic score of 9.6 ± 3.8 compared with 9.9 ± 3.5 in controls. There were no significant differences in the macroscopic scores among any GH treatment groups.
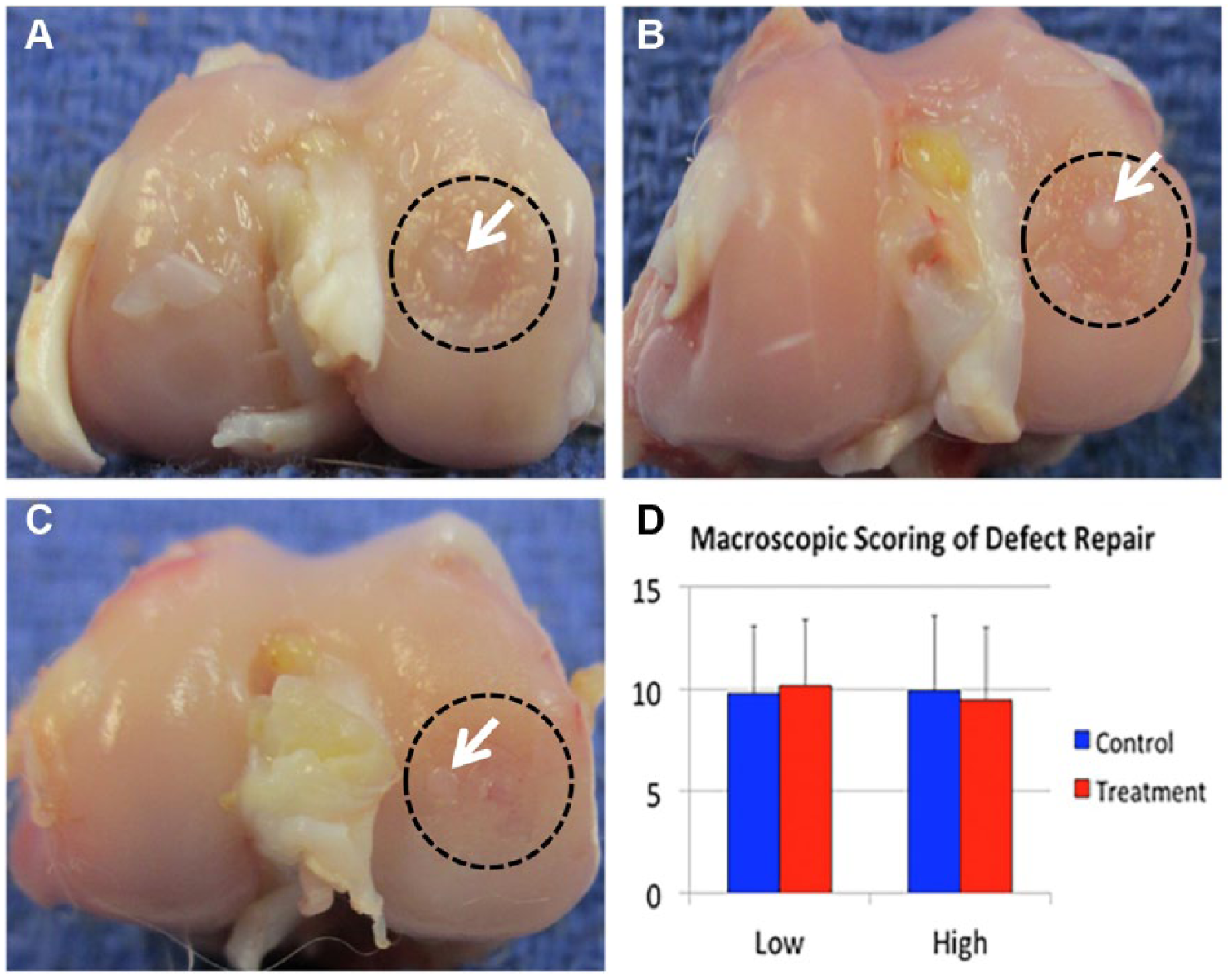
Representative images from macroscopic soring of cartilage defect and repair site. (
Histological Defect Repair Scoring
Figure 4 demonstrates representative images of safranin-O–stained histological sections for microscopic assessment at 12 weeks postmicrofracture from control group, low-GH intra-articular treatment group, and high-GH intra-articular treatment group, respectively. Figure 5 shows mean histological scoring data from each group. Histological assessment of the regenerative capacity of articular cartilage within the defect sites revealed that the average combined score following intra-articular treatment with low-dose GH was 2.0 ± 4.3 compared with 2.1 ± 7.3 in contralateral control knees. High dose treatment resulted in increased histological scoring compared with controls. There were no significant differences in the histological scores within the defect sites among any GH treatment groups, which was likely due to the variability present in these datasets.
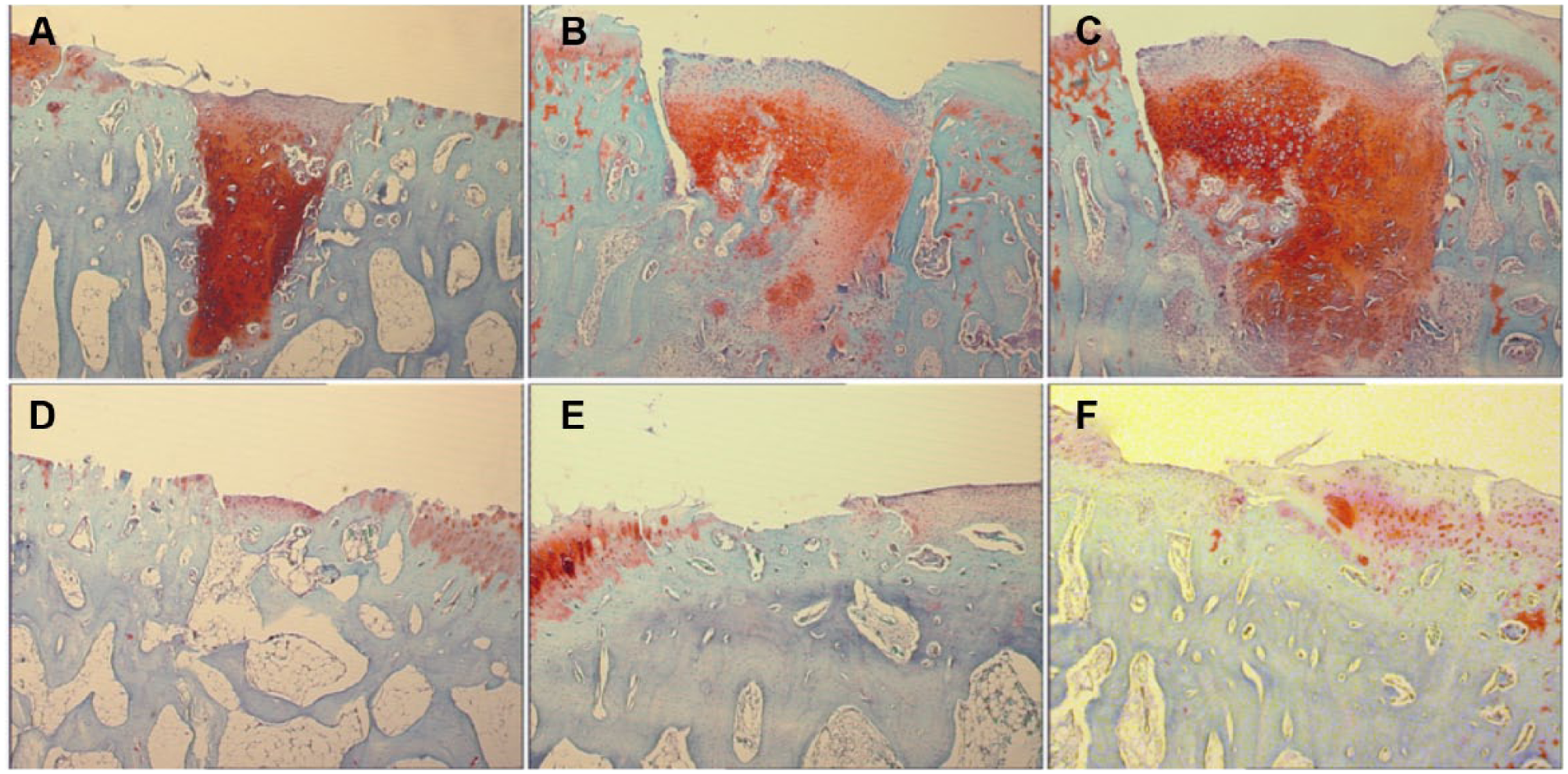
Representative images safranin-O–stained histological sections of the medial femoral condyle in the sagittal place for evaluation using a modified O’Driscoll scoring system at 12 weeks postmicrofracture. (
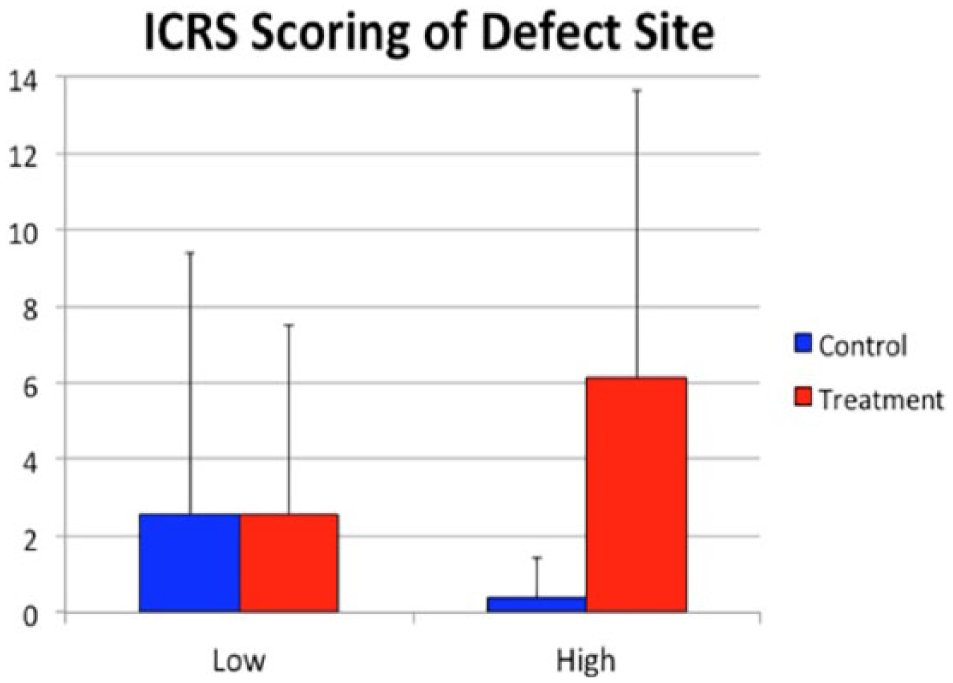
Quantitative analyses showing mean histological scoring data for both the control group as well as low– and high–growth hormone (GH) treatment groups at 12 weeks postmicrofracture. ICRS, International Cartilage Repair Society.
Discussion
There is an ever-increasing need for alternative strategies to address chondral defects which, if left untreated, lead to progressive pain and loss of joint function. This need has led to the development of several new techniques and biological approaches for enhancement of tissue regeneration. The current study sought to investigate the efficacy of intra-articular delivery of growth hormone as an adjuvant therapy for microfracture in the setting of discrete chondral defects within the articular cartilage of the knee.
An important consideration regarding the use of intra-articular GH, or any biological compound which is intended for localized use, is the potential for systemic migration after delivery. The average adult rabbit secretes 0.2 to 0.6 mg of GH per day, which correlates to the magnitude of the doses used in this study. To assess this, the levels of growth hormone, glucose, and calcium levels were analyzed in peripheral blood preoperatively and at a series of predetermined time points postoperatively. These blood assays showed that systemic GH levels experienced a transient nonsignificant decrease immediately postoperatively, and then returned to baseline levels after 24 hours and remained constant thereafter. Additionally, postoperatively serum GH levels did not exceed the baseline levels in the systemic circulation, which would have been expected based on the dosage used. This finding is supported by our data on serum calcium levels, which also remained constant at each time point. We did observe a general trend toward increasing postoperative blood glucose levels, which may be attributed to a progressive response from the surgery procedure itself rather than any specific biological action of GH. This is further reinforced by the fact that there was no difference between the low-dose GH compared with high-dose GH, despite the increasing trend being present in both. We conclude that intra-articular GH does not enter the systemic circulation in our model, and at the time points we studied.
The overall, macroscopic appearance of articular cartilage is often used as a general surrogate for extent of regeneration when assessed clinically, such as during knee arthroscopy. In this study, no significant differences in the macroscopic scoring of the chondral defect regions were found. Regardless of the presence, absence, or dosage of GH, the potential for cartilage regeneration within the defect was not improved. This could mean that GH has no direct effect on neocartilage regeneration during the response to microfracture. However, this could also be attributed to issues of cross-reactivity between the specific growth hormone that we used and the native rabbit GH receptors. Furthermore, the overall macroscopic scores ranged approximately from 9 to 10 from a possible maximum score of 16. Consequently, the quality of the repair tissue at the chondral defect sites did not represent native, intact articular cartilage. Interestingly, in all groups there was evidence of localized regions of cartilage formation directly above the microfracture hole, but this did not appear to be modulated by treatment, at either concentration level, with intra-articular GH. It is not clear why this phenomenon occurred. However, it does demonstrate that some level of cartilage reformation is possible in this model. Future studies are to expand and confirm this observation.
Histological scoring data from these studies confirmed the macroscopic observations that some regeneration of cartilage tissue did occur directly within the microfracture holes, but this response was not different between groups. It was also clear from the histological sections that neocartilage formation did not extend much beyond the boundaries of the original hole. The individual parts of this scoring system addressed the amount of hyaline cartilage, tissue structural characteristics, cellular changes, defect boundary degeneration, proteoglycan levels, and subchondral bone status. This final component of the scoring system addressed reconstitution of the subchondral bone. While this metric did not constitute a large enough effect in subchondral bone changes to influence the overall score, we did note some qualitative morphological differences in this compartment in the treatment groups, which were not captured by this scoring system. It may also be that the variability in our data is why no conclusive differences were found in this study. We propose that these changes might be quantitatively assessed by full micro–computed tomography analyses and/or dynamic histomorphometry, which were not part of the original experimental design for this study, but would likely be informative studies to complete in future. This will be an important addition to future studies, since enhancing activation of subchondral bone during repair wound not be a favorable outcome in chondral defect repair.
This study has several limitations. First, activity levels of these animals were not controlled. In humans, microfracture procedures are typically followed by a period of non-weightbearing in the operative joint. Thus, differences in weightbearing activity levels in this rabbit model could influence the data reported here. Second, the transport and localization of GH within the synovial capsule is not fully characterized known. Future studies could address this issue by incorporating the use of drug-delivery systems, which could release GH in a more controlled and site-specific manner within the defect region that can be temporally detected to ensure action at the desired location. Such vehicles could take the form of synthetic sponge/scaffolds or encapsulated in small liposomal or other biological carriers. In addition, this study only evaluates a single GH injection at the time of chondral injury, this experimental design was chosen based on translational considerations, whereby the least number of injections (ideally a single one) would be most clinically desirable. Future evaluations should consider multiple injections at different time points.
In this study, we demonstrate that intra-articular GH is not systemically absorbed during the initial 48 hours postoperatively. We have also demonstrated that using our experimental conditions, GH does not augment the formation of fibrocartilage above and within microfracture holes. These data do not support our original hypothesis and suggest that either GH is not suitable as an adjuvant to microfracture for chondral defect repair or simply we have not identified the correct conditions by which it is successful. We also report some qualitative changes in subchondral bone microarchitecture in this study. Future studies will be necessary, using micro–computed tomography and dynamic histomorphometry to quantify the subchondral bone response. Based on the conditions of this study, GH has no effect in short-term chondral defect repair and requires further study to be considered a viable augment for chondral defect repair.
Footnotes
Acknowledgments and Funding
The authors gratefully thank the contributions of Drs. Laith Jazrawi and Guillem Gonzalez-Lomas in the macroscopic scoring section of this article and also Drs. Gordon Roble, and You Jin Lee for veterinary and histological assistance, respectively. The authors gratefully acknowledge funding from AANA grant 13-A0-00-000864-01 for this project.
Authors’ Note
Natalie Danna and Bryan Beutel are co–first authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.S. reports that he is a consultant for the Joint Restoration Foundation. The remaining authors have nothing to disclose.
Ethical Approval
Ethical approval for this study was obtained from IACUC 121201-01.
Animal Welfare
The present study followed international, national, and/or institutional guidelines for humane animal treatment and complied with relevant legislation.