
Abstract
Objective:
We report the long-term clinical outcomes of patients who underwent autogenous bone grafting of large-volume osteochondral defects of the knee due to osteochondritis dessicans (OCD) and osteonecrosis (ON). This is the companion report to one previous published on the biological response. We hypothesized that these grafts would integrate with host bone and the articular surface would form fibrocartilage providing an enduring clinical benefit.
Design:
Three groups (patients/knees) were studied: OCD without a fragment (n = 12/13), OCD with a partial fragment (n = 14/16), and ON (n = 25/26). Twenty-five of 52 patients were available for clinical follow-up between 12 and 21 years. Electronic medical records provided comparison clinical information. In addition, there were plain film radiographs, MRIs, plus repeat arthroscopy and biopsy on 14 patients.
Results:
Autogenous bone grafts integrated with the host bone. MRI showed soft tissue covering all the grafts at long-term follow-up. Biopsy showed initial surface fibrocartilage that subsequently converted to fibrocartilage and hyaline cartilage at 20 years. OCD patients had better clinical outcomes than ON patients. No OCD patients were asymptomatic at anytime following surgery. Half of the ON patients came to total knee replacement within 10 years.
Conclusions:
Autogenous bone grafting provides an alternative biological matrix to fill large-volume defects in the knee as a singular solution integrating with host bone and providing an enduring articular cartilage surface. The procedure is best suited for those with OCD. The treatment for large-volume articular defects by this method remains salvage in nature and palliative in outcome.
Introduction
We report the clinical experience and long-term clinical status of 51 patients after autogenous bone grafting of large-volume defects of the knee due to osteochondritis dissecans (OCD) and osteonecrosis (ON). This is the companion report to a previously published study on the biological response. 1 At the time this study was initiated, the medical literature held no prospect for sustainable cartilage repair while the biological fate of various approaches to cartilage repair remain controversial.2-8 The surgical treatment in the early 1980s for large-volume femoral condyle defects was total knee arthroplasty or a cadaver osteochondral allograft.9,10 Physicians and patients were reluctant to consider cadaver allografts due to the unknown risk surrounding the discovery of AIDS in the early 1980s. 11 Total knee arthroplasty was an emerging technology without long-term follow-ups at that time, so patients were reluctant to sacrifice the entire joint for a localized lesion. The consideration of autogenous bone grafting was a reasonable alternative because most cartilage repair procedures at that time were limited to a two-dimensional superficial defect of the articular cartilage. 12 Subsequently, such procedures have been used for larger defects.13-15 In recent years, autogenous osteochondral grafts were introduced for large-volume defects. 16 The treatment for large-volume articular defects remained salvage in nature and palliative in outcome.
The rationale for this novel approach evolved with time and experience. It was known that fixation of fragments from OCD absent a bone graft may fail to unite. 17 This knowledge led to the use of adjunct autogenous bone grafting for osteochondral lesions. In cases in which the available OCD fragment was small, the bare area of exposed bone graft became covered with a blood clot. 18 Biopsies of the previously exposed grafted surfaces of these cases at 8 weeks showed histomorphology similar to that observed after abrasion arthroplasty. 1 It had been observed that fibrocartilage formed over surgically abraded exposed bone in the arthritic knee survived for 2 years. 19 Animal studies supported a similar biological fate of autogenous bone grafting to large osteochondral defects.20,21 It was reasoned that the autogenous bone grafting method would avoid the risk of disease transmission and that the autogenous bone graft matrix would fill the osteochondral defect.
It has been reported that surgical removal of the OCD fragment had poor outcomes. 22 Therefore, a variety of surgical procedures have been reported with attempts at preservation of the joint surface in OCD. These have included in situ drilling, replacement, screw fixation, osteochondral autografts and allografts.23-27 Present treatments for ON include drilling, cancellous packing, unicompartmental replacement, tibial osteotomy, and total knee arthroplasty.28-32 Various commercial biological matrixes have been proposed in recent years for the treatment of large osteochondral defects.33-35 However, autogenous bone appeared to be a cost-effective, readily available matrix without the risk of infection from the allograft. These observations prompted the use of autogenous bone graft as a matrix for larger osteochondral defects in selected cases of OCD when the fragment was absent as well as for ON. Precedent for neither this novel approach nor the clinical outcome of such a procedure was known to the authors.
The purpose of this study was to review the long-term clinical outcome of patients undergoing autogenous bone grafting of large-volume osteochondral defects due to OCD and ON. This report focuses on the preoperative conditions, patient selection, the operative technique, the postoperative management, and the resultant clinical course. It was hypothesized that the autogenous bone graft would integrate and the articular surface would form fibrocartilage that would endure and provide a clinical benefit. 1
Methods
The study was initiated before the advent of institutional review board (IRB) jurisdiction in our community. The subsequent clinical and radiological long-term follow-up was under Michigan State University IRB approval. An indexed and searchable comprehensive office-based proprietary electronic medical record (EMR) existed for all patients in this study. The EMR documented the clinical course from the initial visit through the index surgery and the clinical course with preoperative and interval radiological studies. In addition, there were comprehensive follow-up opportunities when these patients subsequently presented with other conditions.
Subjects
Patients of any age with OCD and ON and large-volume lesions were considered for this type of surgery. Those with superficial or recent traumatic lesions, instability, ankylosis, or severe diffuse degenerative arthritis were excluded. Between September 29, 1987, and August 8, 1994, there were 52 patients (55 knees) treated with autogenous bone grafting for a large-volume osteochondral defect. The patients were placed in three diagnostic groups based on their index clinical diagnosis and surgical findings (patients/knees): OCD with no fragment (n = 12/13), OCD with fragment (n = 16/16), and ON (n = 25/26). Three patients had bilateral involvement. One such patient had a knee placed in two different categories—ON and OCD with no fragment. Therefore, the patent count on the category designation ends up at one more than the 52 original patients. Two patients in the ON group were not of spontaneous origin, but iatrogenic. 1 One patient’s ON was due to a YAG laser used at time of the previous arthroscopy, and the other patient’s ON was due to leukemia chemotherapy treatment including cortisone.
Twenty-five of the 52 patients returned for the in-person long-term clinical assessment between 12 and 21 years after procedure (mean 16 years). In this group, there were 7 females and 18 males, aged between 13 and 82 years (mean 47 years). Three patients had bilateral involvement accounting for 28 knees, which were divided into three groups based on the etiology and surgical method: OCD/fragment (n = 8), OCD graft only (n = 11), and ON (n = 9). The in-person long-term clinical assessment included an up-to-date medical history, physical examination, and radiological imaging including an MRI.
The EMRs were reviewed for outcomes on the patients not available for the long-term in-person clinical assessment. There were an additional 16 patient knees with EMR follow-up data available with the same information as the long-term cohort at 12 years or more but did not return for the in-person long-term evaluation. Eleven patients were lost to follow-up or deceased before 12 years.
Hundreds of matching data points from the comprehensive initial encounter and follow-up EMR modules were used for identifying any changes in symptoms, physical findings, and function over the long term. No attempt was made to correct for missing values or for no responses on the questionnaire. Video tapes of all surgeries were cataloged and archived through the end of this study to provide a means of review and clinical correlation.
Surgical Procedure
All surgeries were performed by one surgeon. The index surgeries included other procedures: partial meniscectomy (15), abrasion arthroplasty (9), chondroplasty (8), resection osteophytes (2), wide synovectomy (1), and loose body removal (19). All cases had the base of the lesion debrided by arthroscopy. The post debridement defects were estimated to be between 6 and 75 cm3. Hinged OCD fragments were replaced into the defect for fixation. The screw lengths were 24 to 28 mm. All chondral fragments were resected in ON cases reasoning they were too thin with little bone attached for internal fixation and or healing.
The margins of the defects were undercut arthroscopically with motorized instrumentation in order to physically secure the free autogenous graft in place. Multiple cancellous bone grafts were packed into the defect. The bone grafts were pressed together so that the graft’s bone spicules engaged each other and the host bone akin to Velcro ( Fig. 2 ). The graft was physically secured in place with an instrument until clot formation.
Valgus producing high tibial osteotomy was performed for medial lesions that involved a large surface area and/or when there was a coexisting varus deformity. Osteotomy was performed on 4/14 knees with OCD and graft only. No osteotomy was performed on those with OCD and a fragment replacement. Osteotomy was performed on 15/26 knees with ON ( Table 1 ).
Summary of Index Surgery on Entire Cohort and the Long-Term Follow-Up Group.
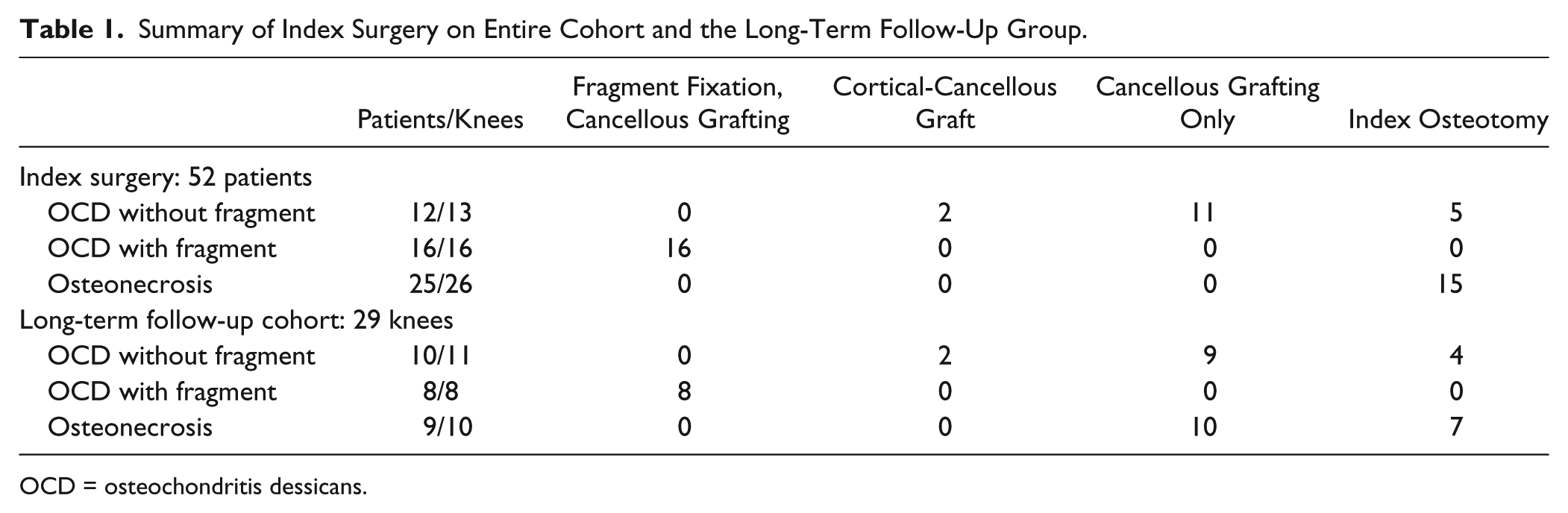
OCD = osteochondritis dessicans.
There was an evolution of the surgical procedure with time and experience. The first cases with small OCD lesions were performed by arthroscopy, cancellous grafting, and internal fixation with cannulated screw fixation of the fragment ( Fig. 1 ). Subsequently, 15 patients with a large-empty defect underwent an open surgical procedure using a cortical-cancellous bone graft (n = 14). The donor site used Gerty’s tubercle with its convex surface to replicate the femoral condylar geometry or bone removed by the closing wedge osteotomy. Subsequently, it was learned that exposed bone graft adjacent to a reattached OCD fragment developed a subchondral bone plate. 1 Thereafter larger defects were treated arthroscopically with multiple fragments of a cancellous graft ( Fig. 2 ). The donor site was the proximal tibial in all but three patients. The cancellous grafts were obtained with an oversized syringe type harvesting device via a cortical drill hole ( Fig. 2A and B ) (Medical Product Resource, Burnsville, MN). In three patients the defect was so large that additional bone was harvested from the iliac crest 1 ( Fig. 3 ). All bone grafts were recessed from the articular surface to be contiguous with the adjacent level of host bone ( Fig. 3 ).
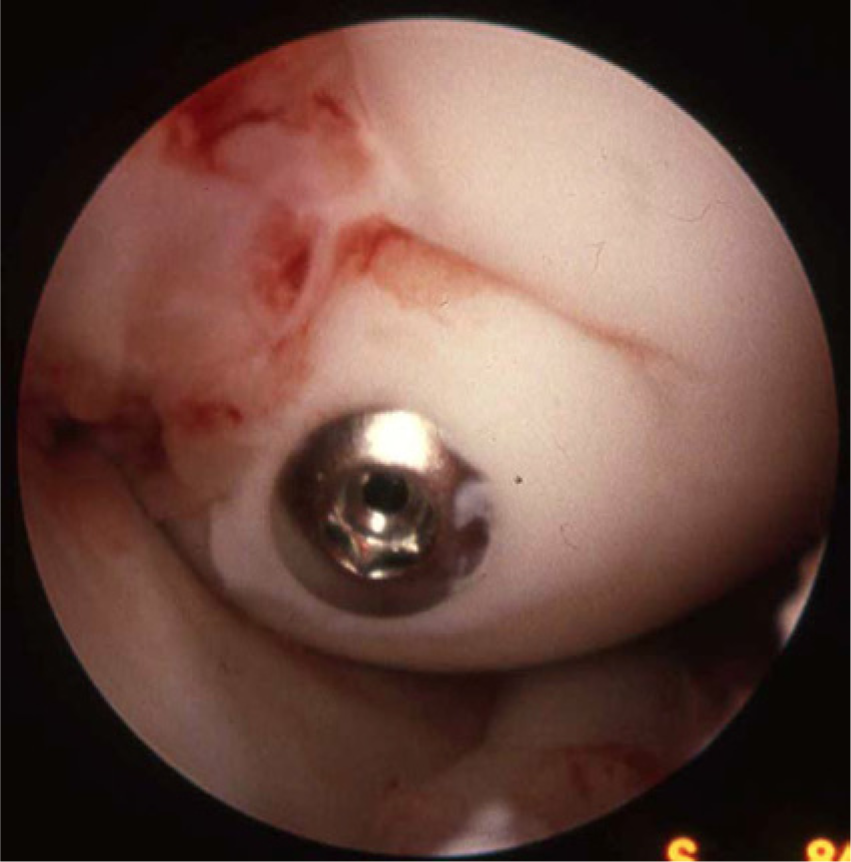
Patient with OCD who had fragment reattachment and bone grafting under and along side. Arthroscopic view of healing OCD fragment at time of screw removal at 8 weeks. Notice the early fibrous tissue healing adjacent to the fragment. OCD = osteochondritis dessicans.
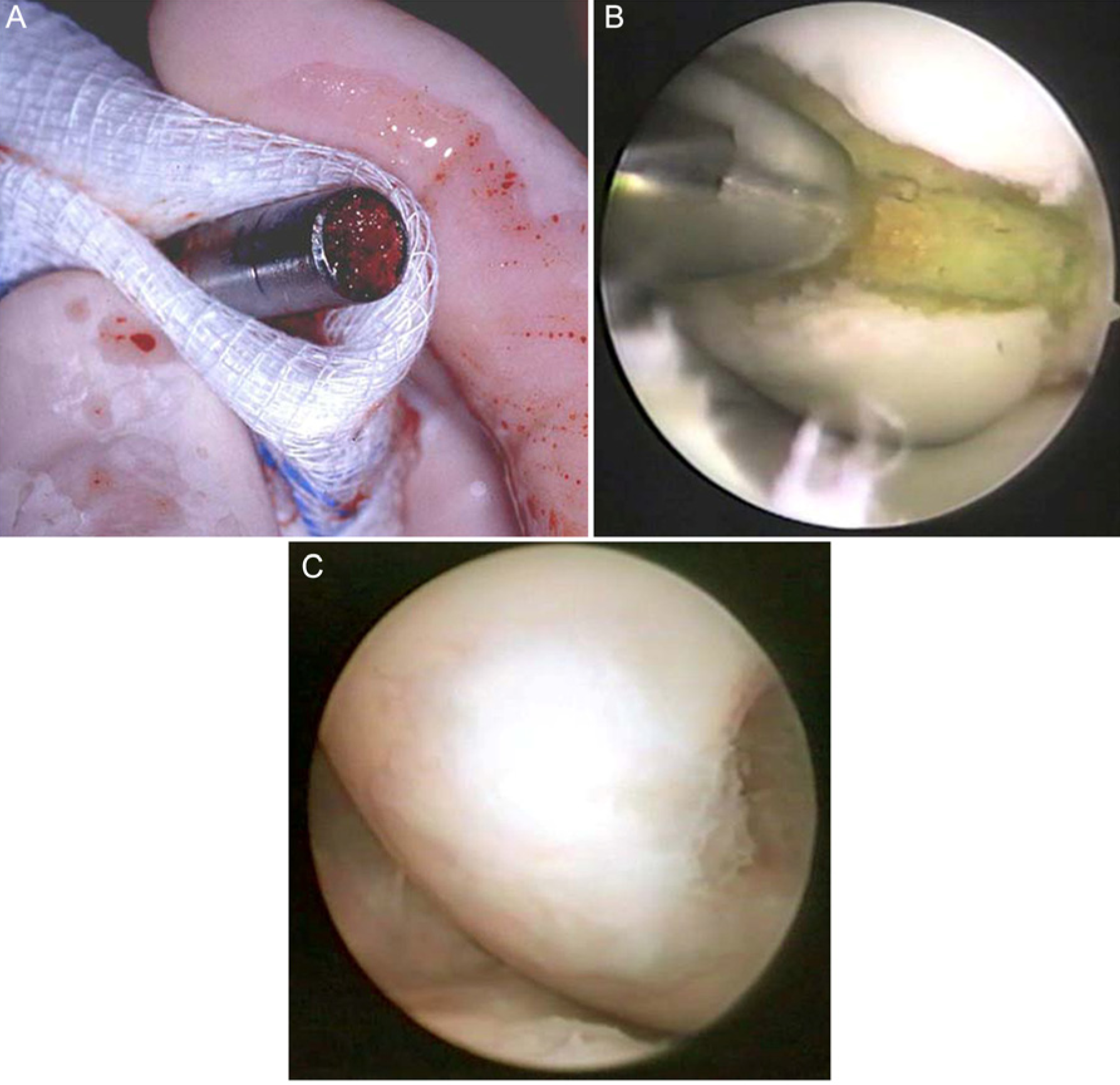
A 24-year-old woman who had previous complete removal of OCD fragment undergoing arthroscopic transcutaneous bone grafting.

Patient with a large osteonecrotic (ON) lesion secondary to chemotherapy and cortisone treatment for acute leukemia (in remission at time of the surgery). He presented with large defects of both medial femoral condyles and both ankles. The size of the lesion necessitated open surgery and bone grafts from both tibial metaphyses and same side iliac crest. Photographs of his right knee were previously reported.
1
The postoperative care included 2 months of non-weight-bearing ambulation with crutches including intermittent active range of motion exercises. Those patients without internal fixation used a knee immobilizer for 2 week.
Radiographic Evaluations
Plain radiographic studies were obtained throughout the course of patient care and at the time of formal follow-up evaluation. All had preoperative plain films in five views: bilateral standing AP, standing Rosenberg view, Merchant view, supine notch view, and lateral. The long-term radiological evaluation included the same plain films of both knees. MRI studies were obtained on 23 patients between 12 and 21 years. One patient with a cardiac pacemaker had a CT scan. One patient from Columbia, South America, was now too elderly to travel, but submitted follow-up history modules and plain film x-rays.
Magnetic resonance imaging was performed at 3 T (GE Healthcare) with a quadrature knee coil. Structural imaging parameters were selected for characterization and differentiation of cartilage, subchondral and cancellous bone, and joint fluid using the following sequences: axial proton density, axial fat suppressed T2, sagittal proton density, sagittal fat suppressed proton density, coronal proton density, and coronal fat suppressed proton density. Nominal in plane resolution was 0.6 × 0.3 mm with 4 mm slice thickness. The biological fate of the donor and host sites were documented by MRI, CT, and biopsy 1 ( Figs. 3 and 4 ).

Coronal proton density MRI shows cancellous bone graft site on medial femoral condyle. There was radiological evidence of bone graft integration.
Results
Clinical outcome information was available on 41 of the 52 patients of 12 years or more. There were no intraoperative or immediate postoperative complications related to this operation. There were no thromboembolic phenomena, hemorrhage, or infections. There were no perisurgical hospital readmissions or deaths.
For clarity, the results are reported by patient knees in each category as three patients had a bilateral condition and one patient had one knee in each of two surgical treatment categories.
All but the physical examination and radiological readings were patient responses to a questionnaire. Therefore, the data had some missing values due to failure of the patient to fill in their responses.
Osteochondritis Dissecans without a Fragment
The preoperative clinical presentation is summarized in Table 2 . There was prior arthroscopic surgery (n = 12) and open procedure in one patient for removal of the OCD fragments and loose bodies.
Preoperative Clinical Presentation: Summary of Common Complaints.
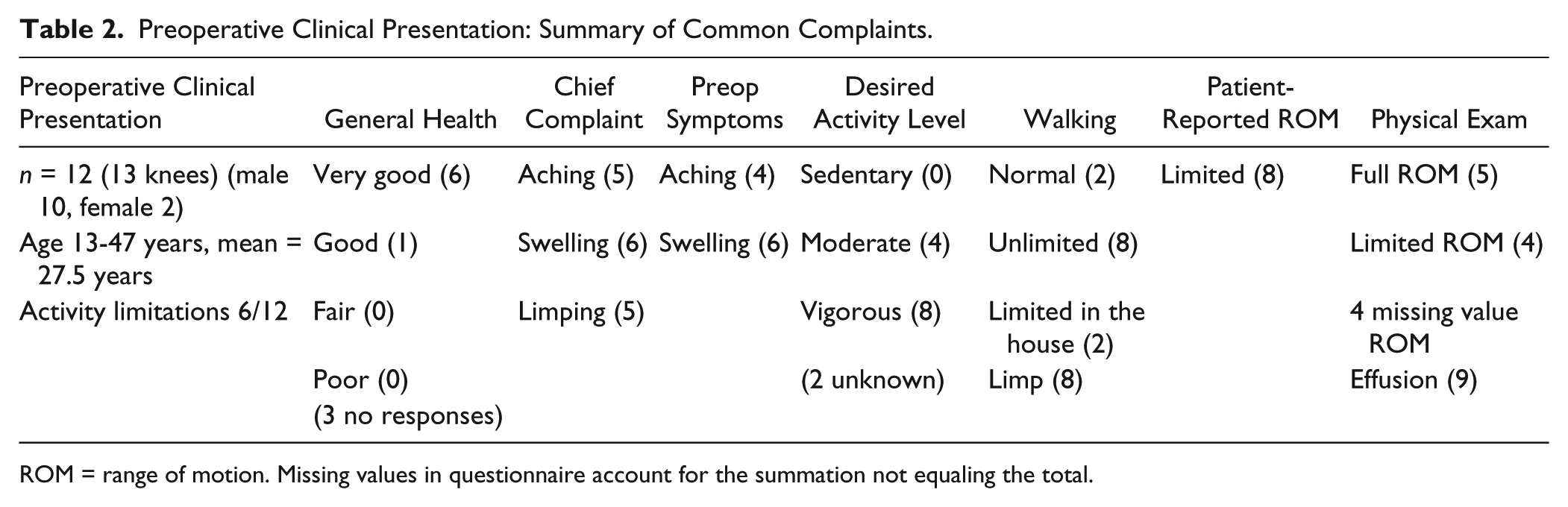
ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
The long-term clinical outcomes showed that symptoms persisted in this group ( Table 3 ). One patient had an unplanned second arthroscopy due to synovitis at 2 years and findings illustrated in the companion report. 1 Ten patients reported they were improved and there was no response in the record for two.
Long-Term Clinical Outcomes: Summary of Common Complaints.
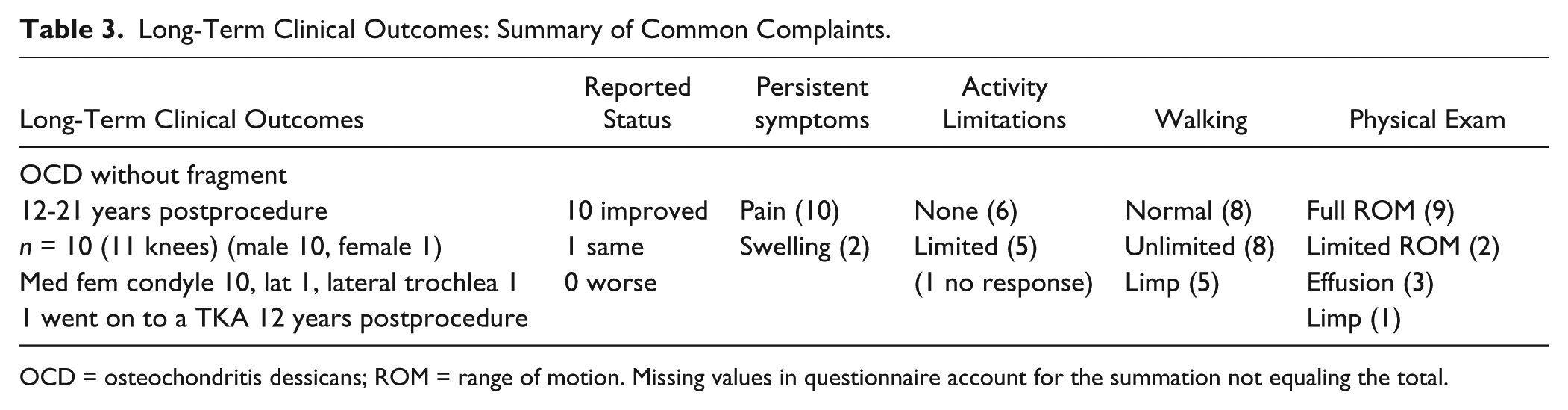
OCD = osteochondritis dessicans; ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
Osteochondritis Dessicans with Fragment
The preoperative clinical presentation for this group is summarized in Table 4 . There was a prior arthroscopic surgery (4) and open surgery (1).
Preoperative Clinical Presentation: Summary of Common Complaints.
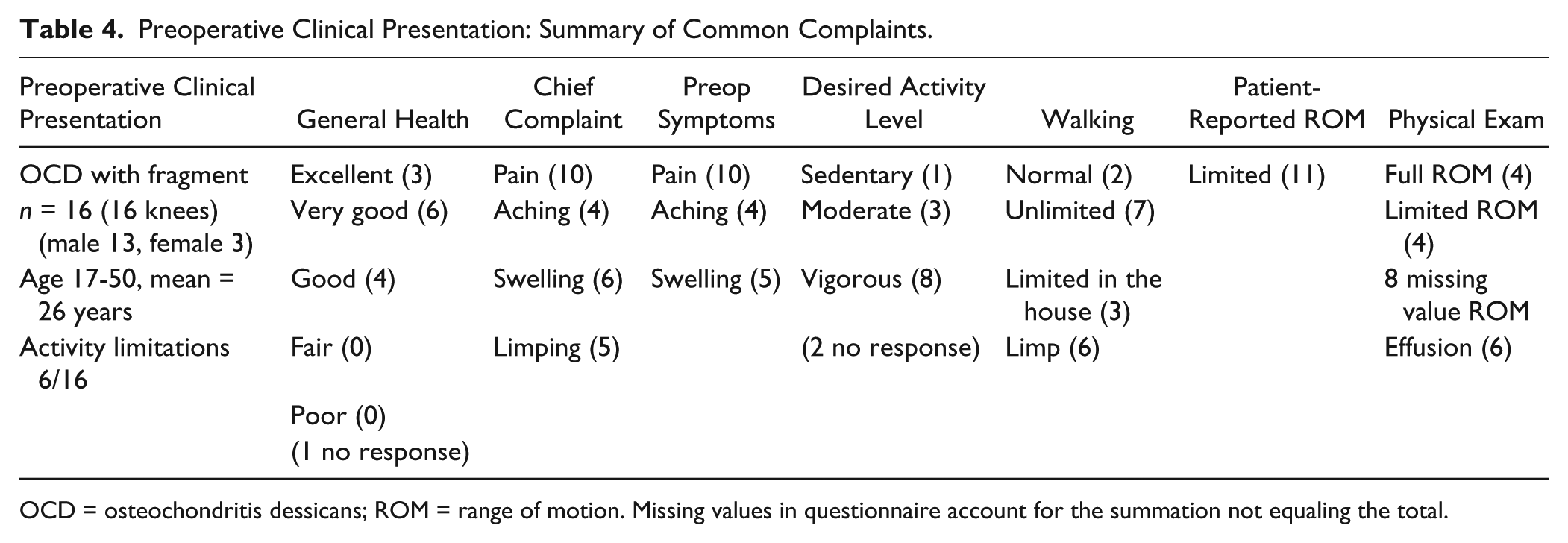
OCD = osteochondritis dessicans; ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
The long-term clinical outcomes showed that symptoms persisted in this group ( Table 5 ). All patients had a planned second operation for implant removal. All patients united the fragment and healed lesion. Seven patients reported they were improved and one was unchanged. However, symptoms persisted in these patients.
Long-Term Clinical Outcomes: Summary of Common Complaints.
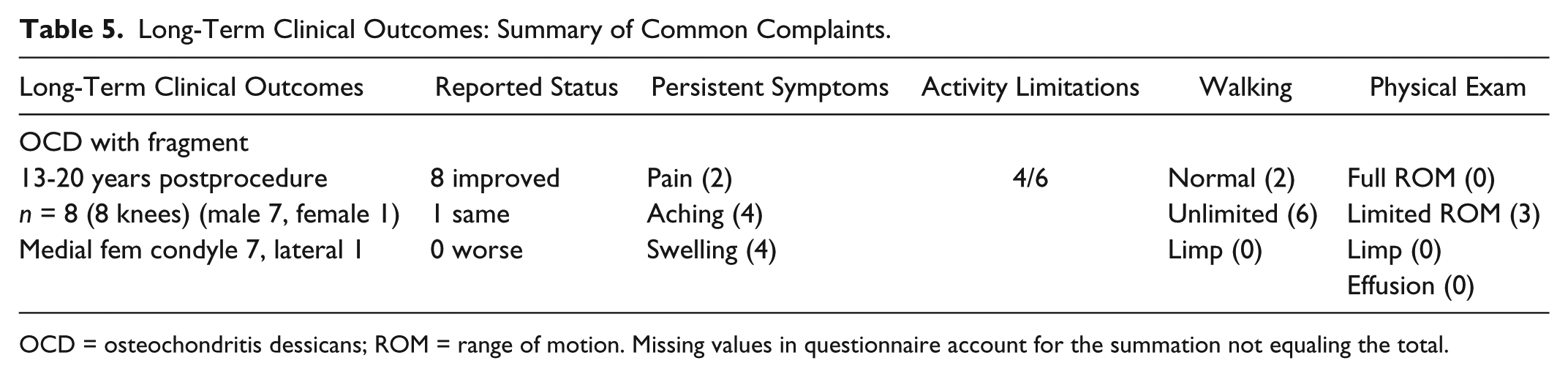
OCD = osteochondritis dessicans; ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
Osteonecrosis Cohort
The preoperative clinical presentation is summarized in Table 6 . This group had prior arthroscopic surgery (11) and open procedures (2).
Preoperative Clinical Presentation: Summary of Common Complaints.
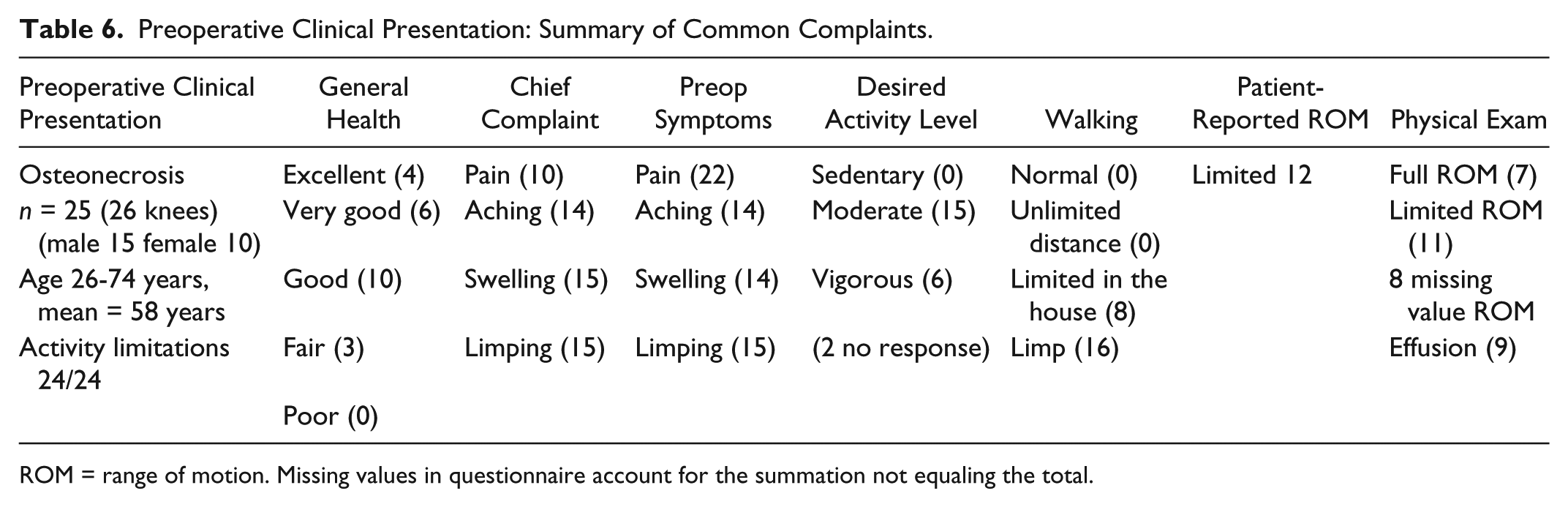
ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
The long-term clinical outcomes showed that symptoms persisted in this group ( Table 7 ). There was a planned reoperation is this group for implant removal (n = 4). One patient with a pending medical malpractice case had second look arthroscopy at 6 and 12 years. This patient died of natural causes shortly thereafter. The patient with the very large lesions had manipulation and adhesiolysis on each knee ( Fig. 3 ). One patient had an arthroscopic debridement at 6 years. Ten patients had a total knee replacement between 1 and 12 years, with an average of 6 years. Four of the 25 patients were known to have died. Four patients were lost to follow-up.
Long-Term Clinical Outcomes: Summary of Common Complaints.
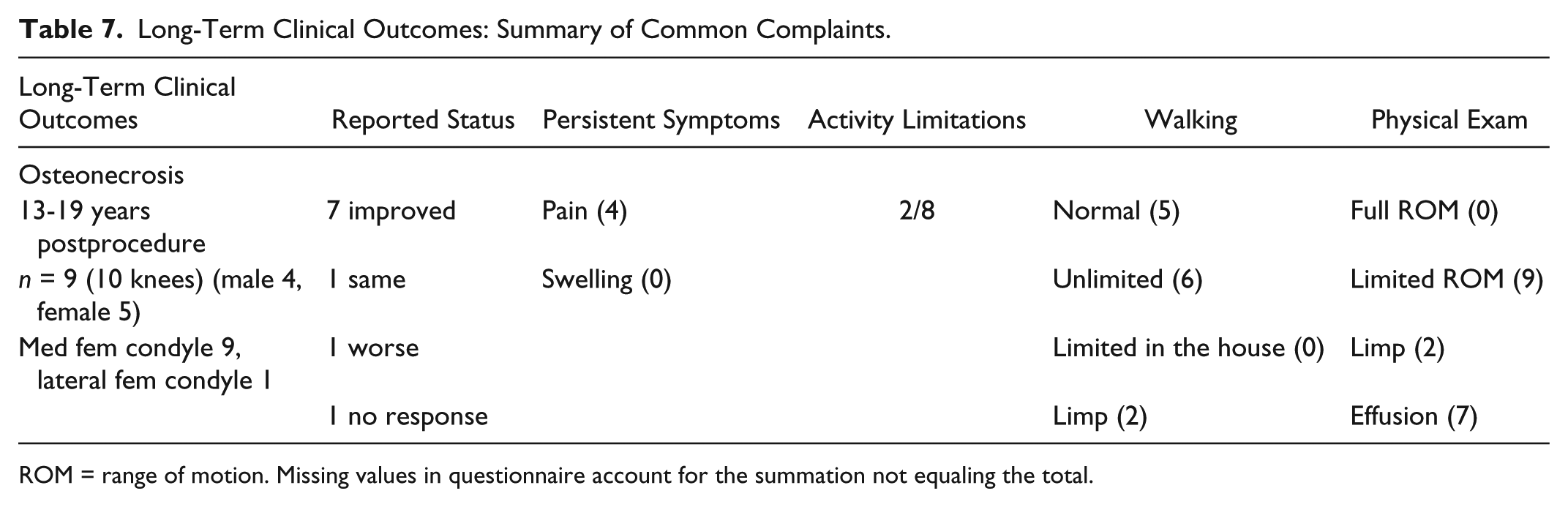
ROM = range of motion. Missing values in questionnaire account for the summation not equaling the total.
The medical record database search of the 16 patient (17 knees) in the interval group evaluations showed that those reporting from this group assessed their outcome condition as improved (2), same (1), or worse (14). The nine patients in the long-term evaluation group reported their condition as follows: improved (7), same (0), worse (1), no response (1). Because the attrition was great and only nine patient knees with in-person assessment, numerical comparisons between the preoperative and postoperative symptoms and physical examination were not meaningful. It should be noted that improvement was not evident in any parameter and an effusion was present in seven of the nine knees examined.
Repeat Surgery
There was planned repeat surgery when internal fixation was used. The unplanned repeat surgery was for screw tightening (1), loose bodies (3), adhesiolysis and manipulation (2), chondroplasty of irregular graft surface (4), arthroscopic debridements (7), medical legal assessment in one patient (X2), and second look for synovitis (1). The patient with the massive lesions of both medial femoral condyles ( Fig. 3 ) developed adhesions at the graft site requiring two subsequent arthroscopic debridement and adhesiolysis procedures with manipulation. The other patient with the iatrogenic ON had two subsequent arthroscopies related to symptoms and an unsettled medical legal case. 1 The second look arthroscopy at 6 and 12 years showed the gross anatomy to be firmer to palpation and congruent with the adjacent surface consistent with all prior observations. 1 One patient who was asymptomatic for 20 years injured his knee and underwent an arthroscopy and biopsy that showed diffuse moderate degenerative change throughout the joint as well as on the surface of the previous autogenous bone graft site. 1
A summary of the subsequent total knee surgery is in Table 8 . The patient with progressive lupus had a total knee at 1 year. There was one total knee replacement in the OCD without fragment group at 12 years. This patient at age 34 had two prior surgeries and degenerative arthritis. He had total knee replacement at age 45.
Subsequent Surgical Interventions.
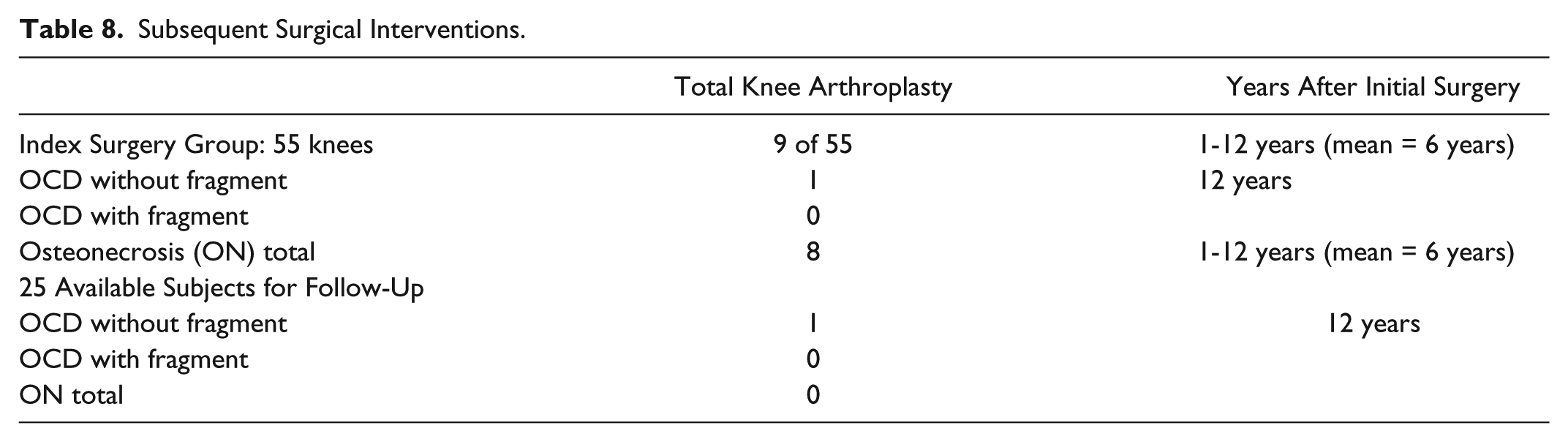
Relationship of the Index Osteotomy to Subsequent Total Knee Surgery
Sixteen of the 54 knees had an accompanying valgus producing high tibial osteotomy. Fifteen of the 26 knees in the ON group had an index osteotomy and 7 of those had a subsequent total knee. One in this group was lost to follow-up. Only 3 of the 11 ON knees without osteotomy came to total knee surgery with two lost to follow-up.
Radiological Follow-Up
Twenty-five of the 51 patients were available for radiological follow-up between 12 and 21 years. During the course of the long-term follow-up evaluations, it was apparent that there was a soft tissue covering seen on MRI over the area of the autogenous bone grafts 1 ( Fig. 4 ). All donor bone sites healed. 1 Continuity of trabecular bone detail with a smooth transition from graft bone to native cancellous bone was consistent with graft integration ( Figs. 4 and 5 ). However, there were occasionally areas of cystic change seen in the grafts. Bone did not grow out beyond the level of the adjacent cortex. The surface tissue overlying the graft consistently had an MR appearance of intermediate signal intensity between that of joint fluid and meniscus, similar to that of hyaline cartilage remote from the area of grafting. 1 The presence of mild signal heterogeneity in the articular surface on some of the subjects was present and was typical of degenerative change. There was osseous incorporation of the graft material in all groups of patients imaged including those with fixation of the native OCD fragment, combined cortical-cancellous grafts, and those with solely cancellous grafting procedures.
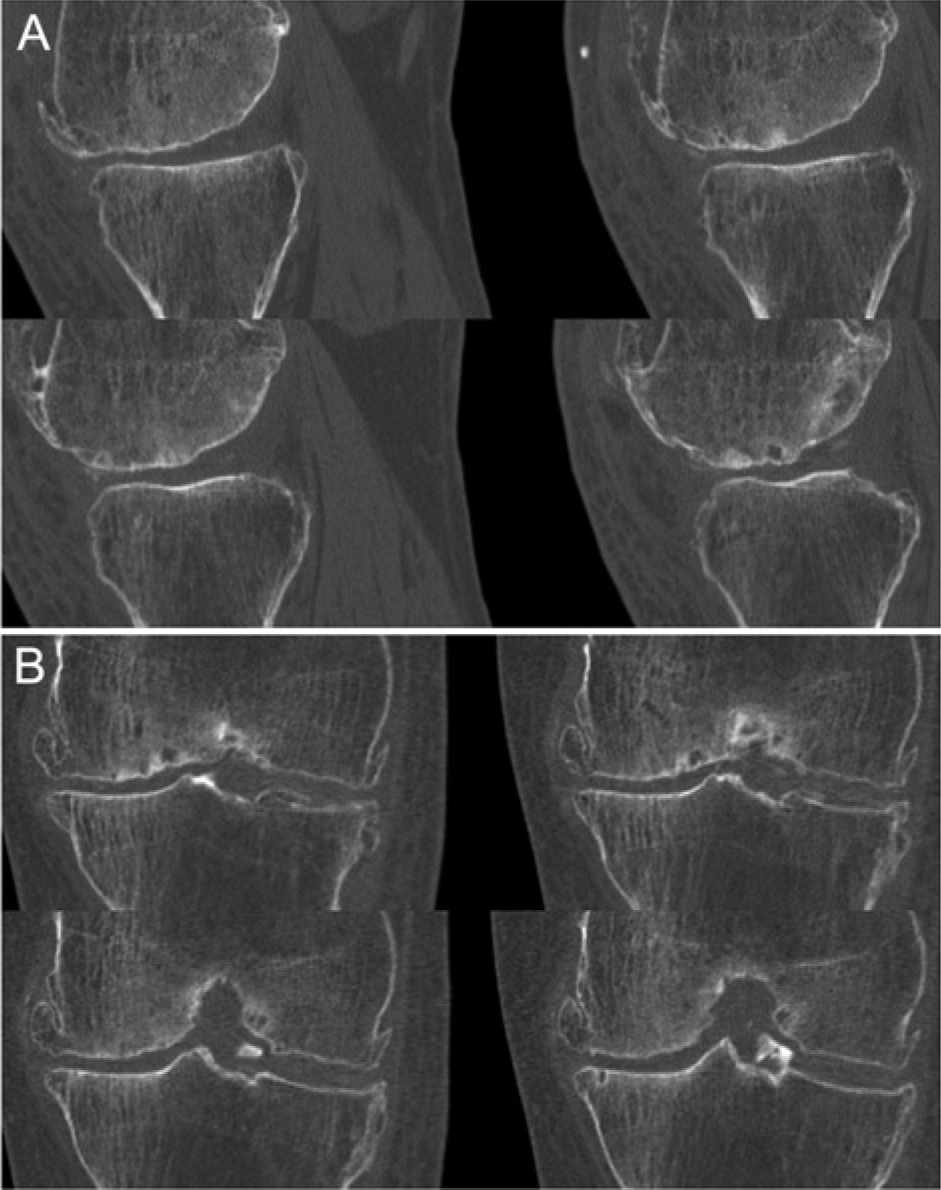
CT scan in another patient at 15 years 9 months postprocedure shows bone integration on medial femoral condyle after grafting for ON:
Discussion
As previously reported, the hypothesis was confirmed that the autogenous bone grafts integrated and formed an articular surface that would endure for many years. 1 However, the uniform biological response of bone graft integration and the subsequent articular cartilage surface repair was not necessarily predictive of the clinical results. Each patient’s EMR was carefully reviewed from the clinical perspective to ensure the proper diagnostic designation and therapeutic categories. Therefore, the category assignments based on clinical factors differed from those made solely on a pathological basis in the prior report. 1
There was clinical improvement for patients with OCD. The original concept for the use of autogenous bone grafts to ensure union of the OCD fragment remains reasonable. 17 At long-term follow-up, patients who reported they were improved were not completely asymptomatic and were not normal on physical examination. Patients with large OCD defects should be given realistic expectations that they will have persistent low-grade pain and swelling and a reduced activity level especially for vigorous sports. However, it is unlikely they will have a total knee replacement in next 20 years. This autogenous grafting procedure may be a viable alternative for those patients with OCD; however, the question concerning retention of the fragment in OCD is not settled by this study because those with and without fragment retention had similar clinical outcomes. Patients with multiple small fragments for reattachment might better have the fragments removed and the entire defect grafted.
The patients with idiopathic ON had less favorable clinical results. Their results indicate a 50% likelihood of having a total knee replacement within an average of 6 years. Even those patients reporting a clinical benefit still had symptoms of pain, swelling, and definite loss of activities following surgery. Therefore, patients with idiopathic ON especially in the presence of osteoarthritis probably should consider primary unicompartmental replacement or total knee arthroplasty.
We did not retain the thin, loose articular wafer on any ON patient, thinking it was too thin for internal fixation. The retention of the fragment in ON may have improved the results in our patients considering the favorable report with fragment retention and bone grafting in a more elaborate procedure including periosteum reported by Rijnen et al. 29 The unloading of the joint for ON patients by high tibial osteotomy in hopes of a better result may not be important because those in our series with and without had a similar incidence of subsequent total knee replacement.
The two patients with an iatrogenic ON etiology had a favorable clinical and biological result in spite of massive bilateral lesions in one ( Fig. 3 ) and pending litigation in the other patient. 1
Although various biologics bone matrixes have been proposed in recent years, autogenous bone appears to be a cost-effective, readily available matrix for large osteochondral defects. The autogenous nature removes the risk of potential complications of the allograft and results in a long-lasting biological solution for both the bone and articular surface 1 ( Figs. 2 - 4 ). The presence of stem cells in cancellous bone perhaps is the reason for the pluripotential progenitors resulting in two phenotypes. 36
The bone graft need only be placed to the level of the adjacent bone as the soft tissue will grow out to the level of the adjacent cartilage. 1 When placed to the level of the adjacent bone it did not recede. 1 Second look arthroscopy demonstrated the grafted surfaces were soft to palpation, unlike the adjacent firm native articular surface. In the largest of grafted surfaces there were postoperative adhesions to the irregular surface requiring subsequent arthroscopic debridement ( Fig. 3 ). The adhesions did not penetrate the intact fibrocartilage.
The contour of the bone graft achieved at the index surgery will remain unchanged 1 ( Fig. 3 ). Therefore, every effort should be made to replicate the convex geometry of the articular surface at the index surgery. A cortical cancellous graft from the convex Gerty’s tubercle area may be necessary as illustrated in the companion report. 1
Reoperations were planned for implant removal. Unplanned open reoperations were infrequent ( Table 7 ). The patient with the largest lesions ( Fig. 3 ) had two subsequent surgical adhesiolysis. There were subsequent loose body removals in 3 of the 51 patients, the origin of which could not be determined. It may have been loose graft material or preexisting as 19 of the 51 patients had loose bodies at the index surgery.
The radiological evidence confirmed the bone graft integration to the host, but it was not homogeneous as evidenced by MRI 1 ( Fig. 4 ). The soft tissue covering over the bone graft retained its integrity for up to 21 years. 1
The downside safety of this procedure is the absence of the original HIV infection risk, absence of intraoperative and postoperative complications, and the viability of the bone as a matrix reconstructing the bone stock for any future surgery. Although various biologic bone matrices have been proposed in recent years, autogenous bone is a cost-effective, readily available matrix for large osteochondral defects.
The strengths of this report were the prospective nature, long-term follow-up, the searchable matching data points in the EMR, and the archived video tapes for exact identification of locations of prior surgical sites. Patients’ follow-up responses were not influenced nor edited. Few patients were lost to follow-up in the short term. Twenty-five of the 52 patients were evaluated in person between 12 and 21 years.
The weakness of this study was that it was nonrandomized with only historical controls. Standardized knee outcome evaluation protocols were not used. The study had a hiatus between the clinical care and the long-term assessment. Some interval radiological studies were lost due to hospital purging of records. The operative surgeon performed the follow-up evaluations, which may have induced bias.
Autogenous bone graft is a readily available osteochondral matrix. This procedure may be a reasonable alternative for selective lesions but remains grouped with others for OCD and ON as both salvage and palliative in nature.23-32
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The clinical and radiological long-term follow-up was under Michigan State University IRB approval.