
Abstract
Objective:
Complex fractures of the tibial plateau are difficult to treat and present a high complication rate. The goal of this report is to describe a combined biological and mechanical approach to restore all morphological and functional knee properties.
Methods:
We treated a 50-year-old woman, who was affected by a posttraumatic osteochondral lesion and depression of the lateral tibial plateau with knee valgus deviation. The mechanical axis was corrected with a lateral tibial plateau elevation osteotomy, the damaged joint surface was replaced by a recently developed biomimetic osteochondral scaffold, and a hinged dynamic external fixator was applied to protect the graft and at the same time to allow postoperative joint mobilization.
Results:
A marked clinical improvement was documented at 12 months and further improved up to 5 years, with pain-free full range of motion and return to previous activities. The MRI evaluation at 12 and 24 months showed that the implant remained in site with a hyaline-like signal and restoration of the articular surface.
Conclusion:
This case report describes a combined surgical approach for complex knee lesions that could represent a treatment option to avoid or at least delay posttraumatic osteoarthritis and more invasive procedures.
Introduction
Complex fractures of the tibial plateau are difficult to treat and represent a challenging problem in orthopedic surgery. Tibial plateau fractures, which are usually a result of high-impact injuries, have a high incidence of severe complications.1-3 These injuries are characterized by articular depression, fracture comminution and displacement, and severe associated injury to the soft tissue envelope of the proximal tibia with potentially devastating consequences.3,4 In fact, inadequate treatment of these fractures may result in long-term pain, instability, deformity, stiffness, and ultimately posttraumatic osteoarthritis (OA). A significant number of patients, even if operated on, develop OA and require a total knee arthroplasty. 5
To achieve good results, the aims of the treatment should be anatomic reduction and stabilization of the articular surface, restoration and maintenance of the mechanical axis of the leg, preservation of the soft tissue envelope of the proximal tibia, and restoration of a functional range of motion (ROM). 6 In the management of complex tibial plateau fractures, therefore, no single treatment modality can be applied; the optimal treatment should be a multiple approach restoring all the morphological and functional characteristics, with prevention of posttraumatic joint deformity, axial misalignment, and possibly OA development.
In the present study, we describe the treatment performed on a 50-year-old woman, who was previously treated with a plate and screws for a Schatzker type II tibial plateau fracture, with residual depression, valgus deviation, and a large osteochondral lesion of the external tibial plateau.
For the restoration of the correct mechanical axis of the lower limb, something that most authorities consider a critical factor in the long-term function and prevention of knee OA, 7 we performed a tibial plateau open-wedge elevation osteotomy with a homologous bone graft. The synthesis was done through minimal internal fixation to avoid excessive invasiveness, which implies additional trauma caused by operative soft tissue stripping and dissection and, therefore, stiffness, pain, deformity, instability, and soft tissue problems.3,8 To restore the joint congruity, we replaced the damaged articular surface with a recently developed composite scaffold, which mimics the biochemical and biophysical properties of the different layers of native osteochondral structures. This scaffold, composed of type I collagen and nanostructured hydroxyapatite (HA), was designed for the treatment of cartilaginous and osteocartilaginous defects and shown to support cartilage and bone tissue formation in our preclinical animal studies and in the clinical practice.9-15 Finally, to protect the bone graft and the osteochondral scaffold, we applied a recently developed hinged dynamic external distractor, which avoids the dangerous effects of weightbearing and shear forces on the grafts and at the same time reproduces the normal knee kinematics, allowing postoperative joint mobilization with partial weightbearing and early functional recovery. 16
Case Report
A 50-year-old woman had a Schatzker type II tibial plateau fracture of the left knee, who was treated with a plate and screws through a lateral approach and cast for 40 days. After the treatment, she complained of pain and instability in the left knee even when performing normal everyday activities and also of frequent episodes of effusion. Walking was possible only with a limp, and her quality of life was reduced. The patient came under our observation after 3 years. At the physical examination, we observed some moderate joint swelling and acute pain in the lateral compartment during palpation. The knee was valgus with a limited ROM (20° lower than the contralateral healthy knee), and the patient experienced pain at high flexion degrees. Moreover, there was instability in the varus stress. The International Knee Documentation Committee (IKDC) objective evaluation finding was “abnormal”; the IKDC subjective and EuroQol visual analog scale (EQ-VAS) scores were 40.2 and 49, respectively; and the sport activity level assessed by the Tegner score was 0. Radiographs showed a valgus alignment of the leg in comparison with the other side due to bone loss and extended osteochondral damage of the lateral tibial plateau ( Fig. 1 ).

(
Due to the complexity of the lesion, we decided to apply an integrated approach, restoring the previous anatomic features with both mechanical and biological treatments. The surgical procedure was performed with the patient under spinal anesthesia and in the supine position. A pneumatic tourniquet was placed on the proximal thigh. The first step was to remove the previous hardware and to perform a tibial lateral plateau open-wedge elevation osteotomy, implanting a homologous bone graft, wedge shaped from a femoral head and fixed with a minimally invasive synthesis (2 screws) to correct the tibial plateau depression and the misalignment. The dorsolateral fragment, visible on a computed tomography (CT) scan, was not remodeled because it did not interfere with the correct kinematics of the knee joint. Once the normal height of the joint line was recovered, we proceeded by treating the joint surface with a new biomimetic nanostructured osteochondral scaffold (Maioregen, Fin-Ceramica Faenza S.p.A., Faenza, Italy) ( Fig. 2 ). The defect of the lateral tibial plateau was prepared using a handheld curette: nonviable cartilage tissues were removed to create a stable shoulder for the articular lesion. The lesion was templated, using aluminum foil, to obtain the exact size of the graft needed to cover the entire defect. The template was then used to prepare the graft, which was implanted through a press-fit technique. Because of the intrinsic adhesive properties of this scaffold, additional fixation devices were not necessary. However, after the tourniquet removal, stability was tested with cyclic bending of the knee while visualizing the graft. Afterwards, 2 intra-articular suction drains were placed. The wound was then closed layer by layer. Finally, we decided to utilize a recently developed hinged dynamic external fixator (EF) 16 to protect the grafts and at the same time allow for early flexion-extension knee movement. The correct placement was checked intraoperatively by repeated flexion-extension movements, positioning the hinge axis nearly parallel to the transepicondylar axis. The EF was then fixed using 2 pins in the tibia and 2 in the femur ( Fig. 3 ).
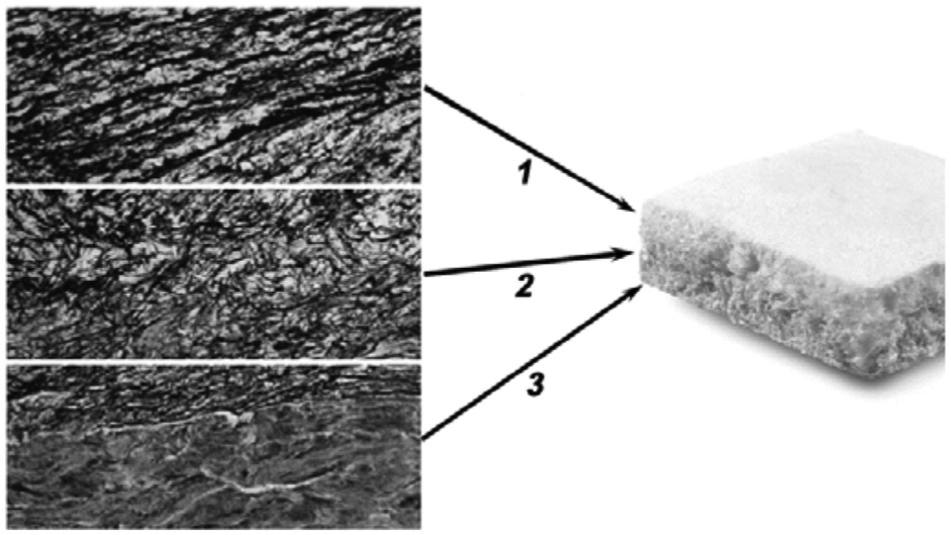
Osteochondral biomimetic scaffold: 1) cartilaginous layer, consisting of type I collagen; 2) intermediate layer (tidemark-like), consisting of a combination of type I collagen (60%) and hydroxyapatite (HA) (40%); and 3) subchondral bone layer, consisting of a mineralized blend of type I collagen (30%) and HA (70%).

Intraoperative images of the external fixator STAR 90 F4 (CITIEFFE s.r.l., Calderara di Reno, Italy) that permits the flexion-extension movement of the knee.
In the postoperative period, rehabilitation started with continuous passive motion the day after surgery from 0° to 100° for the first week. The control of the knee swelling was performed with icing 20 minutes 4 times daily for 2 weeks and afterward once after every rehabilitation session. For the next 4 weeks, active ROM was allowed as possible. Walking with partial weightbearing and isometric exercises was gradually allowed from the day after surgery. The EF was removed 40 days after surgery; subsequently, the patient intensified motion and strengthening exercises, and progressive weightbearing was allowed. Swimming and cycling were allowed at 45 days and 3 months, respectively. Seven months after the surgery, the screws were removed, and at 12 months, after MRI evaluation, joint impact activities (jogging, jumping) were allowed.
At the 1-year follow-up evaluation, the patient did not complain of knee pain, had full ROM, and returned to her previous activities ( Fig. 4 ). The IKDC objective score was “normal”; the IKDC subjective, EQ-VAS, and Tegner scores were respectively 63.2, 83, and 4. At 24 months of follow-up, the activity level was maintained, whereas a further improvement was observed in the IKDC subjective score and EQ-VAS evaluations (70.1 and 89, respectively). At the 5-year follow-up, activity level and EQ-VAS remained stable, and IKDC subjective score further improved to 88.5. The patient was also evaluated using MRI at 12 and 24 months after surgery ( Fig. 5 ). The implant remained in site and showed a hyaline-like signal with restoration of the articular surface at both follow-up times. Subchondral edema progressively decreased with time and at 24 months was barely evident in the tibial plateau.

The patient recovered and returned to normal daily activities with full knee range of motion at 12 months of follow-up.
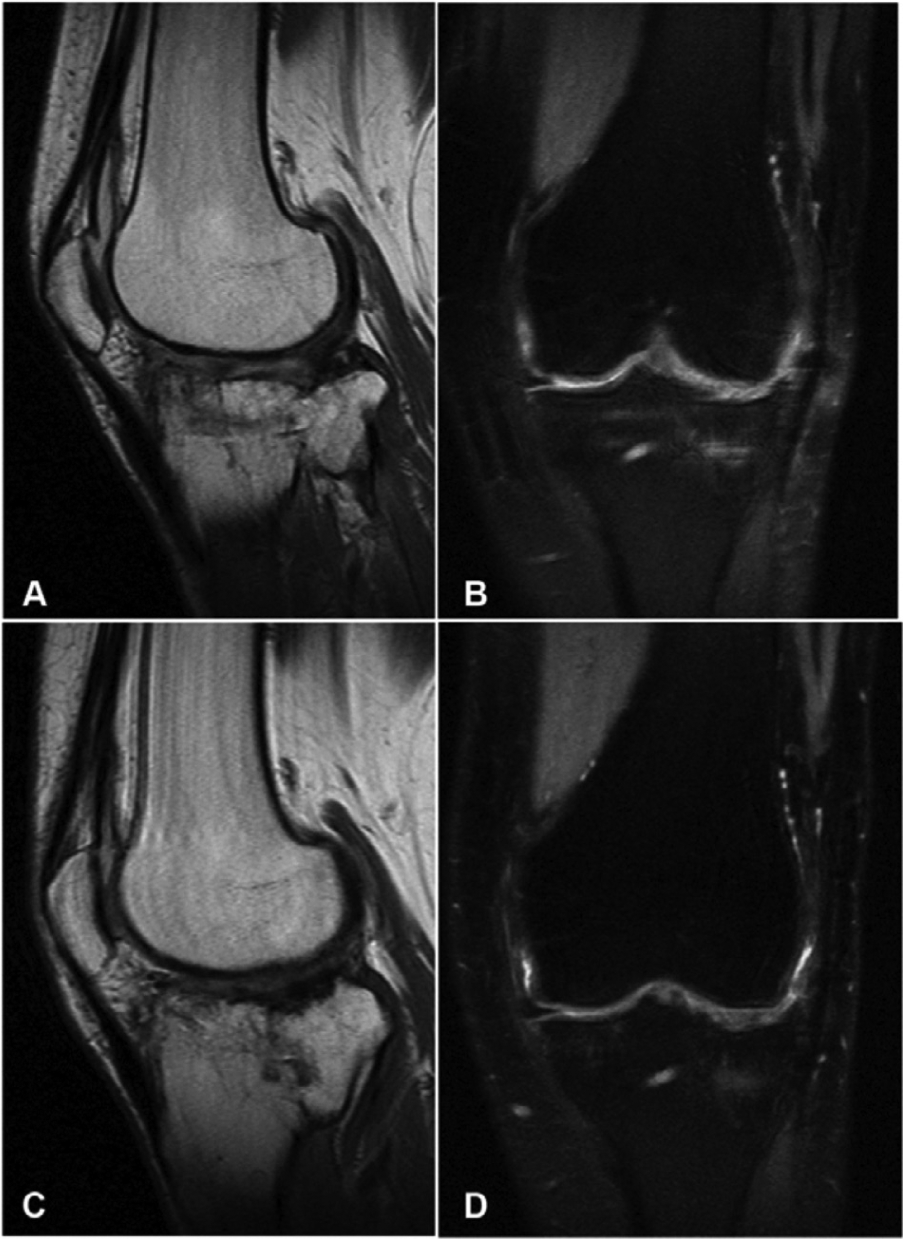
MRI evaluation at 12 (
Discussion
The management of complex tibial plateau fractures with bone loss and depression is challenging. The goals of the treatment firstly consist of restoring the articular surface as much as possible, obtaining a pain-free ROM, and the full recovery of the previous activity level. Methods of acute open reduction and internal fixation with plates and screws of complex fractures of the tibial plateau have a high rate of complications, such as posttraumatic deformities and poor outcome despite articular reduction because of stiffness, pain, instability, residual dysfunction, and many others. 17 In our case, the patient came under our observation with a valgus knee and a limp, complaining of stiffness, joint swelling, pain in the lateral compartment, and instability. The complexity of the lesion required an integrated approach to restore the correct mechanical alignment and repair the damaged articular surface.
A tibial plateau lateral open-wedge elevation osteotomy was performed to correct the depression and the misalignment. A homologous bone graft was implanted to support the elevated articular surface after reduction, and it was stabilized using minimal internal fixation with 2 screws. After recovering the normal height of the joint line, the second step was to treat the damaged lateral tibial plateau surface. Articular chondral defects are hard to treat, and when the damage involves the subchondral bone, the treatment is even more problematic. For osteochondral defect repair, several authors have highlighted the need for biphasic scaffolds to reproduce the different biological and functional requirements for guiding tissue regrowth. 18 Following this rationale, in 2007, we started a clinical experiment on a recently developed cell-free composite scaffold, which mimics biochemical and biophysical properties of the different layers of native osteochondral structures. 9 Technical notes and early stability evaluations of the first 13 patients of this pilot study were documented in an earlier publication, with promising preliminary results. 14 More recently, the pilot study on 30 patients was published, confirming the good results at 2 years of follow-up for the treatment of chondral and osteochondral lesions, and the scaffold is becoming available in many countries for clinical application. 15
The Maioregen scaffold (Fin-Ceramica Faenza S.p.A.) ( Fig. 2 ) is an osteochondral nanostructured biomimetic material with a porous 3-dimensional trilayer composite architecture, mimicking the anatomy of the osteochondral unit. The cartilaginous layer has a smooth surface to favor joint flow and consists of type I collagen. The intermediate layer, tidemark-like, is a combination of type I collagen (60%) and HA (40%). The lower layer consists of a mineralized blend of type I collagen (30%) and HA (70%), reproducing the subchondral bone. Each layer is separately synthesized using a standardized process starting from an atelocollagen aqueous solution (1% w/w) in acetic acid, isolated from equine tendon. The upper nonmineralized chondral layer consists of type I collagen, whereas the intermediate and the lower layers are obtained by nucleating bone-like nanostructured nonstoichiometric HA into self-assembling collagen fibers, as occurs in the biological process of neo-ossification. The final product is obtained by physically combining the layers on top of a Mylar sheet (DuPont, Wilmington, DE) and freeze-drying and gamma-sterilizing it at 25 kGy.
To protect both grafts, we decided to apply an EF, increasing the joint stability and avoiding negative forces on the articular surface. There is little agreement in the literature about which type of EF should be used for the treatment of complex fractures of the tibial plateau. 17 We preferred to utilize an innovative hinged dynamic distractor, which presents, with respect to the other classic EFs, the advantage of an immediate and safe joint mobilization, with less stiffness and a faster functional recovery. This EF is a new device, STAR 90 F4 (CITIEFFE s.r.l., Calderara di Reno, Italy), recently developed by our group, 16 and reproduces the 4-bar linkage model of the knee. Due to the design of this model, it allows knee flexion-extension movements and posterior rollback as in the natural knee with the axis rotation, which changes during flexion. Internal-external rotations that normally occur on the longitudinal axis are fixed. The knee is allowed to move only in the sagittal plane with a reduced range (0°-100°). The normal flexion-extension axis of the knee is nearly parallel to the transepicondylar axis, which passes through the epicondyles and close to the posterior cruciate ligament femoral insertion. Therefore, it is very important to align as much as possible the fixator axis with the knee flexion-extension axis to reproduce the natural knee motion that is performed by the hinge of the EF. The hinge presents a central body made of radiotransparent material, and the shaft and distraction ring nuts are made of light alloy. The use of these materials permits the building of a very strong but light EF, thus protecting the joint but also allowing the patients to easily walk and move the knee. 16
The patient, previously unsuccessfully treated for a complex lateral tibial plateau fracture, was able to achieve good results, as assessed by clinical evaluation and MRI, and to return to a satisfactory functional level. We documented an integrated surgical treatment that comprehends both mechanical and biological procedures. In this way, it is possible to restore previous anatomic features and obtain good clinical outcome even in complex fractures with damaged articular surface, bone loss, and residual deformity. This case report describes an interesting surgical approach even for difficult cases that otherwise are doomed to a poor clinical outcome and represents an alternative treatment option to avoid or at least delay posttraumatic OA and more invasive procedures.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.