
Abstract
Objective
Osteochondral lesions of the talus are common injuries, with one of the leading treatment options being the M-BMS (matrix-augmented bone marrow stimulation) + I/III collagen scaffold. Osteotomy of the medial malleolus is not unusual but presents the risk of malunion or irritation by hardware. The aim of the study was to analyze data from the German Cartilage Society (Knorpelregister DGOU) to evaluate the influence of medial malleolar osteotomy on clinical results of M-BMS + I/III collagen scaffold.
Design
The ankle module of the Cartilage Register includes a total of 718 patients, while 45 patients met the inclusion criteria. Patients were treated with an M-BMS + I/III collagen scaffold of the medial talus, 30 without and 15 with an osteotomy of the medial malleolus. The follow-up evaluations included FAAM (Foot and Ankle Ability Measure), FAOS (Foot and Ankle Outcome Score), and VAS (visual analogue scale).
Results
Forty-five patients (22 male, 23 female) aged between 18 and 69 years (mean: 34 years) were included in this study. Between preoperative and 12 months postoperative, we noted a significant improvement in FAAM-ADL (Activity of Daily Living) (P = 0.004) as well as FAOS-Pain (P = 0.001), FAOS-Stiffness (P = 0.047), FAOS-ADL (P = 0.002), FAOS-Sport (P = 0.001), and FAOS Quality of Life (P = 0.009). There was no significant difference between patients who underwent an osteotomy or not.
Conclusion
The results show a significant improvement in patients’ outcome scores following a M-BMS + I/III collagen scaffold. No statistical difference was noted among those undergoing medial malleolar osteotomy.
Keywords
Introduction
Osteochondral lesions of the talus are more and more common among injuries of the ankle with the majority of the lesions being a result of trauma.1,2 Although most of these traumatic lesions heal conservatively, a serious number persist and lead to ankle pain with a corresponding decrease in pain-free activities.
The German Cartilage Register, which is a working group of the German Society of Orthopedics and Traumatology (DGOU), started collecting data for patients treated with a cartilage defect of the ankle in 2015. The main inclusion criterion is a chondral or osteochondral lesion of the ankle, either tibial or talar, that underwent operative treatment. Different treatment options are known: Small lesions up to 1.5 cm2 are usually treated using microfracture.3-5 For bigger lesions or those with subchondral cysts, this procedure might be insufficient. Therefore, more advanced procedures may provide a more viable solution. ACI (autologous chondrocyte implantation) and OATS (osteochondral autologous transplant) harvest cartilage from a donor site, different from the lesion itself, to fill the defect. In addition to that, ACI is a 2-step procedure and therefore time consuming and expensive. Recently, newer techniques have been described and examined, such as MACI (matrix-induced autologous chondrocyte implantation), 6 HD-ACI (high-density autologous chondrocyte implantation), 7 and MAST (matrix-associated stem cell transplantation). 8 Another treatment option, first described by Behrens et al. 9 in 1999 is the AMIC (autologous matrix-induced chondrogenesis). The most used procedure uses a collagen type I/III bilayer matrix (Chondro-Gide, Geistlich Pharma AG, Switzerland) to cover the superclot after bone marrow stimulation of the lesion. Significant pain reductions and improvements in patient outcomes, as well as return to sports, following this procedure has been documented in mid-term studies with up to 8-year follow-up.10,11
Often, the procedure requires an osteotomy of the medial malleolus due to the location of the lesion on the medial talus. Even though an osteotomy might be necessary in some cases, complications can occur. While different approaches have been described for the osteotomy of the medial malleolus,12,13 all of them contain the risk of a displacement of the fragment with a step of the articular surface of the joint, with a dislocation of 2 mm showing a risk of up to 30% for malunion. 14 Another common postoperative complication derives from the necessity to remove implants, such as plates or screws, due to persistent irritation or discomfort, which may occur in up to 70% of patients. 15 While there are a number of studies that have published outcome data, these have tended to be from small patient cohorts, where patient selection can introduce a bias into the study. Therefore, we evaluated the data from the Cartilage Register into which more than 150 surgical centers are currently including patient data.
The purpose of this study was to evaluate whether a medial malleolar osteotomy has an influence on the clinical outcome of talar osteochondral lesions.
Methods
Database
The current study uses the database of the ankle module of the Cartilage Register (Knorpelregister DGOU). The register was initiated in 2013 for the knee and extended to the ankle in 2015. The German Cartilage Register is financially supported by the Deutsche Arthros Hilfe e.V. and the Stiftung Oskar-Helene-Heim.
At the time of the data extraction, 718 patients had been entered into the register by 151 centers via a remote data entry system. The register gathers the following data:
Demographics (age, gender, weight, height)
Prior treatment
Duration of symptoms
Etiology, defined as traumatic (<12 months), posttraumatic (>12 months) or degenerative (no relation to trauma)
Defect classification (ICRS [International Cartilage Repair Society], Berndt and Harty/Loomer)
Surgical details
Patient-reported outcome measure (PROM) questionnaires, selected according to the joint being treated, are sent to the patients following the surgery. For the ankle module, it includes the Foot and Ankle Ability Measure (FAAM), the Foot and Ankle Outcome Score (FAOS) and the visual analogue scale for pain (VAS).
Patient Selection
The inclusion criteria were 1 osteochondral lesion (OCL) of the medial talus treated with M-BMS + I/III collagen scaffold, either with or without osteotomy of the medial malleolus. The exclusion criteria were OCL of the central or lateral talus, distal tibia, and treatment other than M-BMS + I/III collagen scaffold. Out of the 718 patients that had been entered in the register at the time of the analysis, we identified 45 who met all the aforementioned criteria. The patient selection is depicted in Figure 1 .
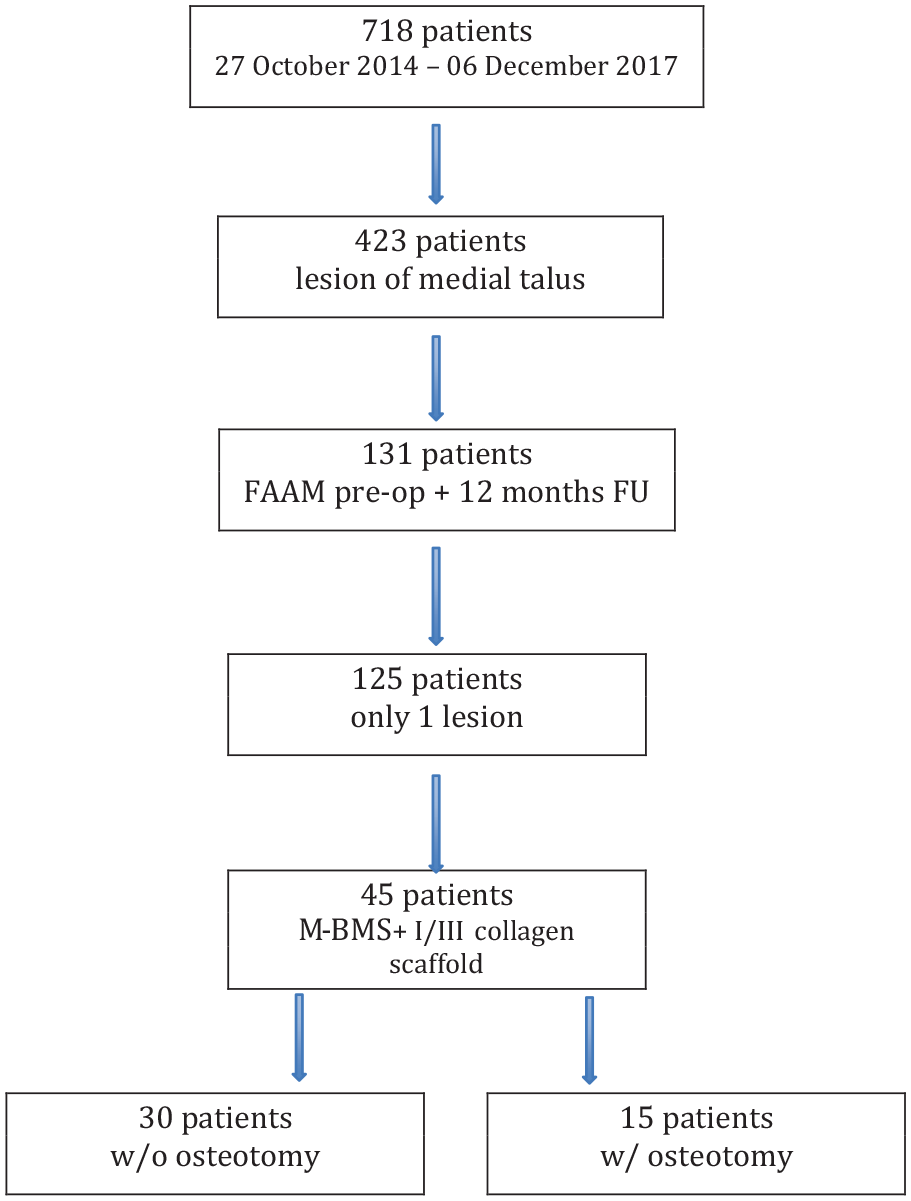
Patient selection. FAAM, Foot and Ankle Ability Measure; FU, follow-up; M-BMS, matrix-augmented bone marrow stimulation.
Scores
Foot and Ankle Ability Measure
The FAAM has been translated into German by Hauck et al. 16 in order to detect functional deficits of the ankle. It contains 21 questions asking about the patients’ ability to perform certain activities of daily living (ADL) with an additional question to rank the function in daily life. The second part of the questionnaire contains 8 questions about sport-related activities. For both the FAAM as well as the sports subscale, a higher score indicates greater functional ability.
Foot and Ankle Outcome Score
The FAOS is a 42-item questionnaire, which, like the FAAM, has been translated and validated in German. 17 It contains 5 subscales, including stiffness, pain, ADL, sport activities, and quality of life. A higher score indicates fewer problems as well as fewer functional limitations.
Visual Analogue Scale for Pain
In this PROM, the scale ranges from 0 to 10, where 0 equals no pain while 10 equals the worst pain that the patient has ever experienced.
Classification
Two scores are used in the German Cartilage Register. The ICRS score describes the defect of the cartilage. 18
Another score was popularized by Berndt and Harty classification, modified by Loomer, which is based on radiographic appearance. 19
Outcome Variables
Primary Variables
The FAAM ADL (Foot and Ankle Ability Measure of Activities of Daily Living) preoperative and at 12-month follow-up was the primary outcome variable.
Secondary Variables
Secondary outcome variables were the overall FAAM, FAOS, and VAS. Additionally, the covariates of age, gender, BMI (body mass index), size of lesion, and symptom duration were tested for their effect on PROMs.
Statistics
Statistical analysis was performed using the software package SPSS (version 22; IBM Corp, Armonk, NY, USA). Data were tested for normal distribution using the Kolmogorov-Smirnov test (P = 0.028), which showed no normal distribution. Therefore, values are presented as median (IQR [interquartile range]), if not it is stated differently. Group comparison was conducted using the Wilcoxon signed rank test or Mann-Whitney U Test, where appropriate. Correlations were determined by calculating the Spearman coefficient (rho). A P value <0.05 was considered to be significant.
Results
Patient Selection, Demographics, and Etiology
Out of 718 patients from the database, 45 met the inclusion and exclusion criteria. Thirty patients underwent M-BMS + I/III collagen scaffold without and 15 with an osteotomy of the medial malleolus. The detailed patient selection is depicted in Figure 1 . The median age was 34 (24) years. A total of 51% of the patients were female; the median BMI was 26 kg/m2 (6). The median duration of symptoms was 19 (38) months.
In all, 16% of the cases were related to trauma with a medical history less than 12 months while 40% of the patients had a posttraumatic history exceeding 12 months. However, most cases were not related to a trauma and therefore classified as degenerative (44%). 58% of the patients had undergone previous surgery and 92% of these were related to the cartilage injury.
For the classification of the lesion, 2 different grading scales were given. Among the patients, 4% were rated grade II for the ICRS classification, 20% grade III and 76% grade IV. According to the Berndt, Harty, and Loomer classification, 7% were type II, 40% type III, 18% type IV and 36% type V including a subchondral cyst. The mean area of the lesion was 1.7 ± 1.25 cm2 and the volume was 1 ± 1.38 cm3. A corresponding tibial lesion was detected in 24% of the cases (22% ICRS I-II and 2% ICRS III-IV).
The majority of the surgeries were performed by an arthrotomy alone (56%) or by arthroscopy (11%). An osteotomy of the medial malleolus was performed in 15 cases (33%). Additional procedures, which included hindfoot alignment, debridement of the impingent or ligament stabilization were performed in 58% of the patients.
Scores
As shown in Table 1 , the values for FAAM-ADL and sports, and all FAOS subscales improved significantly. While the VAS had also decreased over the 12-month follow-up, this was not a statistically significant change (P = 0.129).
The Pre- and Postoperative PROMs for all patients.
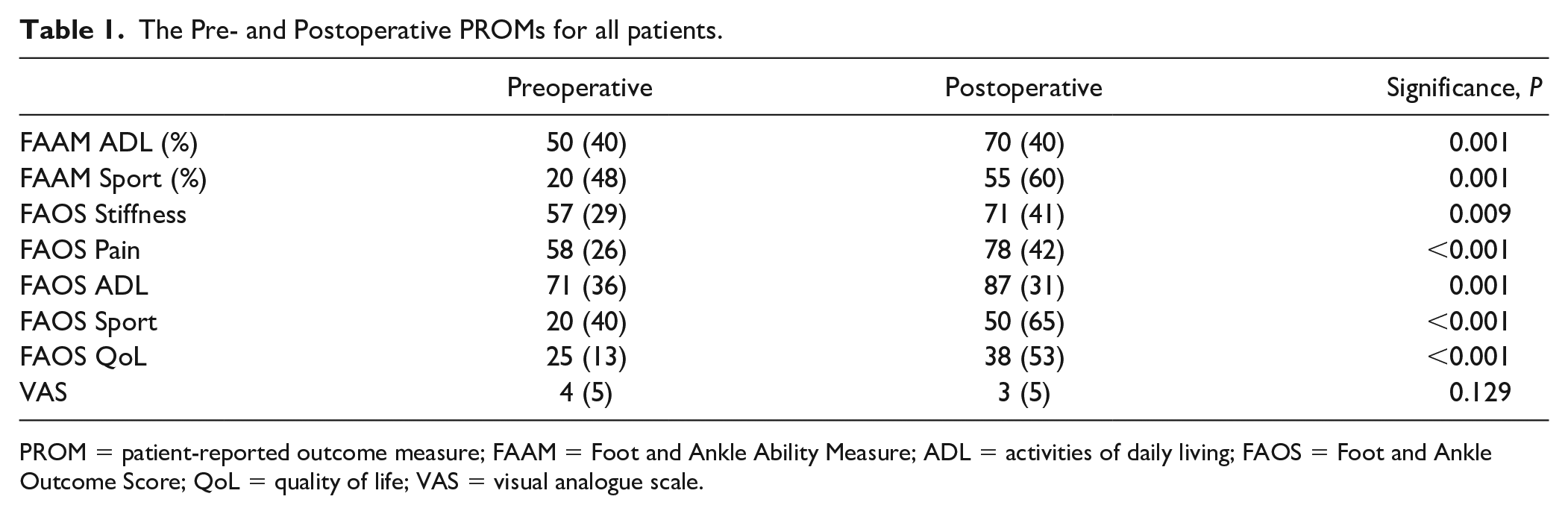
PROM = patient-reported outcome measure; FAAM = Foot and Ankle Ability Measure; ADL = activities of daily living; FAOS = Foot and Ankle Outcome Score; QoL = quality of life; VAS = visual analogue scale.
In comparing the outcomes of the patients who underwent osteotomy to those who did not, we compared the baseline values between these 2 groups as well as the postoperative values. These are depicted in Figure 2 and Supplement 1. There were no differences between these 2 groups at either preoperative assessment or at the 12-month follow-up.
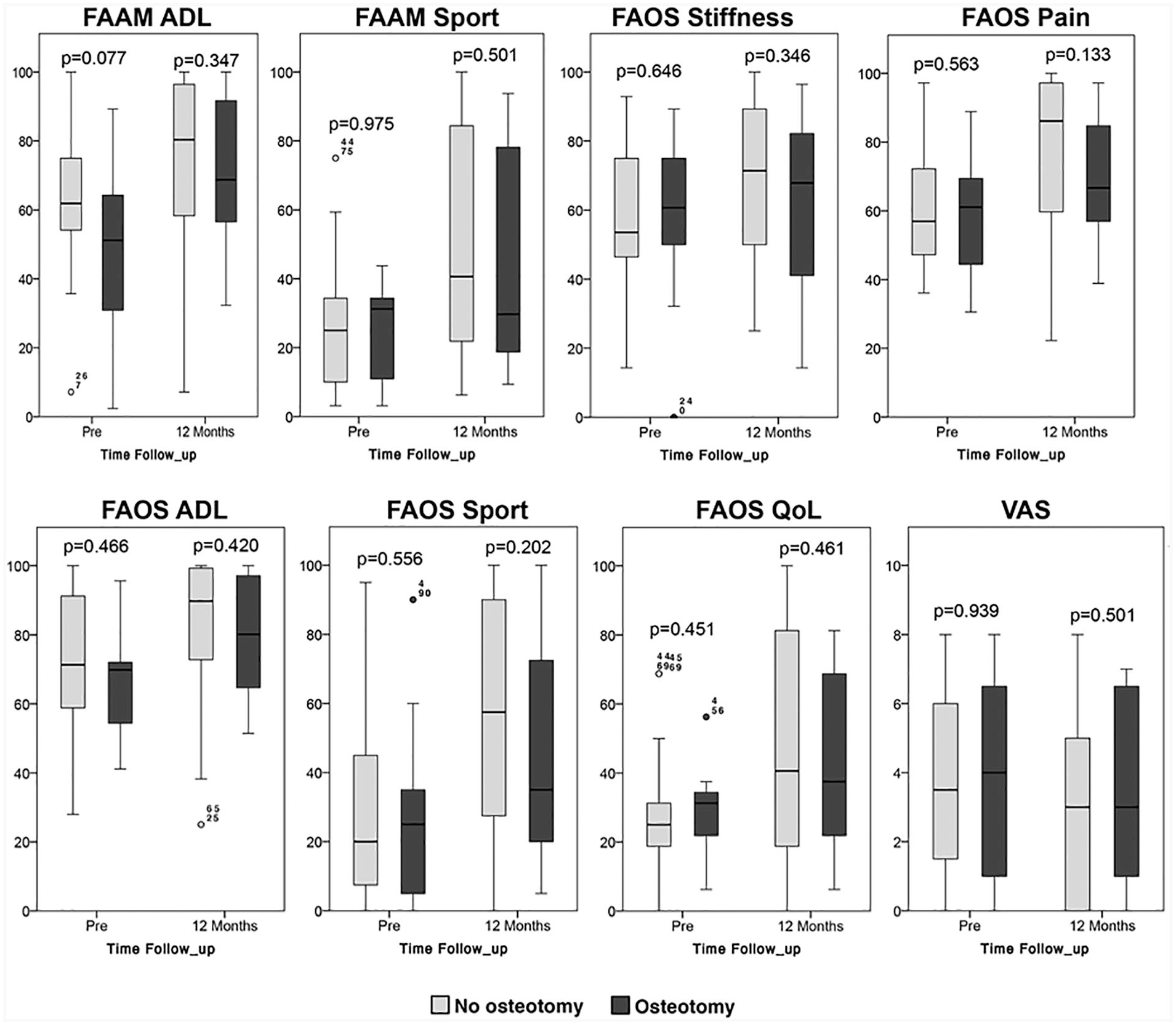
Boxplots pre- and 12 months postoperative for all PROMs comparing patients undergoing a M-BMS + I/III collagen scaffold with or without an osteotomy of the medial malleolus. PROM, patient-reported outcome measure; M-BMS, matrix-augmented bone marrow stimulation; FAAM, Foot and Ankle Ability Measure; ADL, activities of daily living; FAOS, Foot and Ankle Outcome Score; QoL, quality of life; VAS, visual analogue scale.
Finally, no significant correlation was noted between the outcome scores and the covariates of age, gender, BMI, duration of symptoms, location of the lesion, and ICRS classification ( Table 2 ).
Correlation of Covariates on Clinical Outcome.
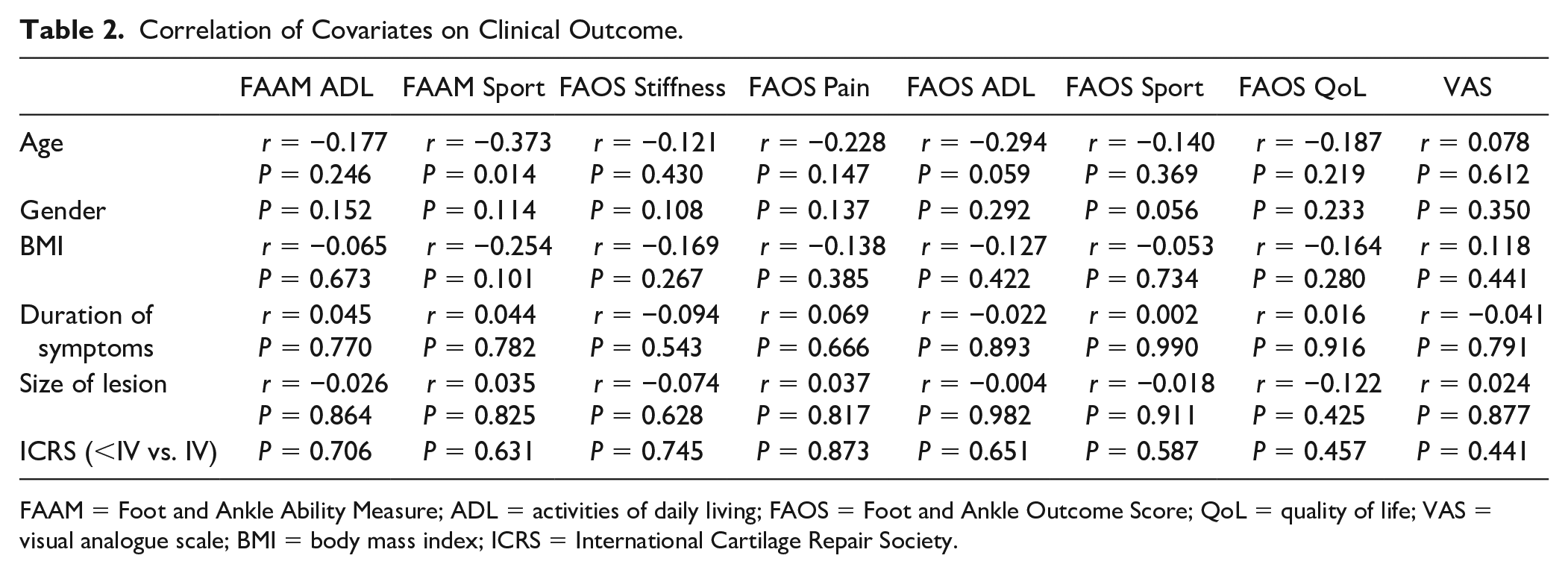
FAAM = Foot and Ankle Ability Measure; ADL = activities of daily living; FAOS = Foot and Ankle Outcome Score; QoL = quality of life; VAS = visual analogue scale; BMI = body mass index; ICRS = International Cartilage Repair Society.
Discussion
Walther et al. 20 described the reconstruction of focal cartilage defects in the talus with mini-arthrotomy instead of performing an osteotomy of the medial malleolus. Galla et al. 21 have shown that AMIC procedure can be performed via an anterolateral or anteromedial approach to the ankle without an osteotomy of the medial malleolus. Among the patients in that study, all 23 patients remaining in the final analysis had the surgery performed without an osteotomy and demonstrated good clinical and MRI results. Another study by Sadlik et al. 22 stated that osteochondral lesions of the medial talar dome could be addressed without performing an osteotomy of the medial malleolus. Due to the documented problems related to the osteotomy of the medial malleolus, which included a 6% long-term morbidity, 15 a malunion rate up to 30% with an average of 2 mm of incongruence 14 as well as soft tissue irritation by the screws, it seems there is a need for alternatives. But at the same time, it is important to have a closer look and differentiate between lesions regarding size, location and, importantly, the existence of subchondral cysts as large cysts at the dorsomedial aspect of the talus can make a medial malleolar osteotomy inevitable. 23 Therefore it would be interesting to see if the patients included in this study develop osteotomy-related problems in the future. A longer-term study will also allow the evaluation of differences in outcomes between patients with regard to an osteotomy.
In our cohort, 44% of the lesions were classified as degenerative, which is contrary to most published data. 5 Since “simple” ankle sprains are often related to an osteochondral injury, patients might not connect their problem to this injury, especially if there was a delay of months to years between the sprain an the onset of symptoms.
Cofactors and their influence on the pathology have been frequently discussed. A correlation between pain and increased BMI has been reported for female patients with lesions of the ankle. 24 Also, it seems that BMI is correlated to the lesion size. 25 However, even heavy patients with larger lesions did show a significant improvement in symptoms. 26 Körner et al. 27 reported a correlation between the Berndt, Harty, and Loomer classification in regard of the relevance for predication of patients complaints. However, this was not confirmed in our study. A reason for that might be the different sample size.
In our study, age did not have an influence on the outcomes, as shown by the clinical scores. This is in accordance with the data from D’Ambrosi et al., 28 who reported a good clinical outcome in young as well as older patients with no significant difference between the age cohorts.
Most of the clinical scores, including FAAM and FAOS include questions for well-being or limitations regarding the previous week. This may lead to a bias representing an especially bad or good week and may not necessarily be representative of a general picture.
Our patient selection was performed by including all patients from the German Cartilage Register who met the inclusion and exclusion criteria. The 45 patients included (out of 423 patients treated for an osteochondral lesion of the medial talar dome in the register) provided a representative cohort needed for the analysis. However, some of the patients included in this study had prior surgery related to their cartilage injury, which might influence the outcome. Another potential criticism is the large number of surgeons who provided their data for the register. This may cause a different interpretation of the intraoperative findings, although standardized classification systems have been used. In spite of the limitations, this data provides evidence that M-BMS + I/III collagen scaffold is a useful tool to improve pain and function, whether as primary and/ or secondary procedure, and that a medial malleolar osteotomy does not have an impact on PROMs. More studies are necessary with larger numbers of patients, longer follow-ups and standardized evaluation methods in order to get an improved idea of the outcomes following different treatment options, as the effects of the different parameter seems to be low. The low power of the study carries a high risk for ß-error missing factors influencing the result. One theory might be that the individual capacity to heal is more important for the final result than any of the parameter assessed with scores and classifications. However, it will be a challenge for future research to identify the factors that have a significant impact on the final result after complex cartilage reconstruction involving techniques other than microfracture.
In conclusion, osteochondral lesions of the medial talus show a significant improvement, from pre- to postoperatively, in all subscales of the FAAM and FAOS. Different parameters such as age, gender, size of lesion, duration of symptoms, or ICRS classification did not have an impact on the outcome.
The data from this study shows that there is a significant improvement in the FAAM and the FAOS, as well as all subscales, after cartilage reconstruction with a M-BMS + I/III collagen scaffold. However, no significant difference could be detected between the patients who underwent an osteotomy of the medial malleolus and those who did not.
Supplemental Material
Supplemental_table_1 – Supplemental material for Influence of the Medial Malleolus Osteotomy on the Clinical Outcome of M-BMS + I/III Collagen Scaffold in Medial Talar Osteochondral Lesion (German Cartilage Register/Knorpelregister DGOU)
Supplemental material, Supplemental_table_1 for Influence of the Medial Malleolus Osteotomy on the Clinical Outcome of M-BMS + I/III Collagen Scaffold in Medial Talar Osteochondral Lesion (German Cartilage Register/Knorpelregister DGOU) by Oliver Gottschalk, Sebastian Felix Baumbach, Sebastian Altenberger, Daniel Körner, Matthias Aurich, Christian Plaass, Sarah Ettinger, Daniel Guenther, Christoph Becher, Hubert Hörterer and Markus Walther in CARTILAGE
Footnotes
Authors’ Note
Matthias Aurich is also affiliated with Department of Orthopaedics, Trauma – and Reconstructive Surgery, University Hospital Halle (Saale), Halle (Saale), Germany and Department of Trauma- and Reconstructive Surgery, BG Trauma Center Bergmannstrost, Halle (Saale), Germany.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval:
Ethical approval for this study was obtained from Ethics-Committee (Fribourg; # 520/14).
Informed Consent:
Written informed consent was obtained from all participants.
Trial Registration:
DRKS00005617
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.