
Abstract
Objective:
Tissue repair that occurs after microfracture does not include hyaline-like cartilage. Therefore, other treatment modalities must be combined with microfracture to improve repair tissue quality. In this study, we combined exogenous hyaluronic acid with microfracture.
Design:
Thirty mature New Zealand rabbits were randomly divided into 3 groups as control, microfracture (MF), and microfracture and hyaluronic acid (MFHA). Four-millimetre full-thickness cartilage defects were created in the medial femoral condyle of each rabbit. Microfracture was performed on defects in the MF and MFHA groups. At 1 week following surgery, 1 mL of saline was injected into the knees of the control and MF groups, whereas 1 mL (15 mg/mL) hyaluronic acid was injected into the knees of the MFHA group 3 times weekly. At 6 months postsurgery, defects were evaluated according to the ICRS (International Cartilage Repair Society) and Wakitani scales.
Results:
According to the ICRS and Wakitani scales, the quality of repair tissue was improved in MF and MFHA groups as compared the control group (P = 0.001 and 0.001, respectively). No significant difference was observed between the MF and MFHA groups (P = 0.342).
Conclusions:
According to the model in this study, no beneficial effect was obtained when HA injection was combined with microfracture in the treatment of full-thickness cartilage defects.
Introduction
Management of cartilage defects poses problems because of the avascular nature of the cartilage tissue and the limited proliferation capacity of chondrocytes. 1 Although many management modalities have been described, a method that maintains the biomechanical characteristics of the cartilage for a long time and promotes the formation of new cartilage tissue that remain healthy is not yet available. Currently, microfracture technique, autologous chondrocyte transplantation, and mosaicplasty have gained wide acceptance. 1 Microfracture technique is based on the differentiation of bone marrow stem cells to chondrocytes for repairing the chondral defect. 2 This method is a relatively simple, cheap, and minimally invasive technique that can be performed in one session. 2 On the one hand, comparable outcomes are possible with either microfracture technique or autologous chondrocyte transplantation. 3 On the other hand, some studies have reported insufficient differentiation of stem cells with microfracture resulting in fibrocartilagenous repair tissue formed on the defect site without regeneration of hyaline cartilage, which essentially determines the quality of repair. 4 However, Steadman et al. 2 indicated that tissue developed after microfracture repair is a mixture of fibrous and hyaline cartilage tissue, and the repair process occurring in the defect site can last for nearly 2–3 years, with tissue formed during this period undergoing physiologic remodeling. In addition, some investigators have also stated that new modifications should be added to the microfracture technique with the intention of decreasing the prolonged duration of physiologic remodeling and improving the quality of the repair tissue.2,5
Hyaluronic acid (HA) is a substance found in normal synovial joints with favorable effects on lubrication, chondroprotection, and maintenance of glycosaminoglycan stability. 6 It is a widely used exogenous method for the management of osteoarthritis. The antiinflammatory, anabolic, analgesic, and chondroprotective effects of HA have long been recognized. 6 In one study, HA was shown to increase the proteoglycan content of cartilage and promote DNA replication resulting in an enhancement of chondrocyte proliferation. 7 Hagewald et al. 8 suggested that HA might increase formation of the extracellular matrix by ensuring differentiation of matrix cells into mesenchymal stem cells.
Kang et al. 9 reported that one-time HA injection after microfracture improves quality of the repair tissue. However, this study relied on observational results rather than quantitative reports. Strauss et al. 10 stated that although the quality of repair tissue does not significantly improve at the end of 6 months after 3 HA injections, other cartilaginous tissues outside of the repair site showed less degeneration. A study consisting of subchondral drilling and concomitant HA injection revealed an improvement in repair tissue; however, the short period of HA action time was reported as a major disadvantage. 11
The objective of the current study is to investigate whether HA injections are effective in enhancing the quality of repair tissue after microfracture. If HA improves the quality of repair tissue regenerated after the application of the microfracture technique, then it might be included in the clinical management protocol so as to increase the success rate of the microfracture technique.
Materials and Methods
The study was performed on >6-month-old 30 New Zealand mature rabbits following approval of the local ethics committee. The rabbits were randomly allocated to 3 groups, each consisting of 10 animals as control, microfracture (MF), and microfracture and HA (MFHA).
Surgical Procedure
The rabbits were anesthetized with 10 mg/kg ketamine and 8 mg/kg xylazine. For prophylaxis, 20 mg/kg intramuscular cephazoline sodium was used. The right hind leg of each rabbit was shaved, stained with antiseptic solution, and covered with a sterile drape. The knee joint was entered through an anterior midline longitudinal incision. After medial parapatellar arthrotomy, the patella was luxated laterally to expose the knee joint completely. In all animals, a full-thickness cartilage defect was created on the weight-bearing surface of the medial femoral condyle, without injuring subchondral bony structure, under proper magnification using a 4-mm dermal punch and a special curette. During formation of the defect, special care was used to protect the subchondral bony structure and avoid any bleeding from the base of the defect. In the control group, the defect was not subject to any additional interventions. In groups MF and MFHA, 2-mm-deep microfracture holes were created using a 0.5-mm Kirschner wire on the defect region beginning from the periphery to the center of the defect, leaving intact tissue between the holes. From each hole, bleeding was ensured. For each defect, 4 holes were created. Later, the patella was reduced and arthrotomized, and then skin incisions were closed with continuous 4,0 Vicryl (Ethicon, San Angelo, TX) and 4,0 Prolene (Ethicon) sutures. After the intervention, no activity restrictions were applied to the rabbits. For analgesia, 1–2 mg acetaminophen was added to 100 mL of the drinking water. Oral feeding was permitted ad libitum, and rabbits were fed with standard rabbit chow.
In the MFHA group, 1 mL intraarticular HA (15 mg/mL, Orthovisc, Anika Therapeutics, Bedford, MA) injections were started at the first postoperative week and were continued on the basis of 1 injection per week for a total of 3 weeks. In the control and MF groups, 1 mL physiologic saline was injected into the corresponding knee joints of the rabbits at identical time points.
Evaluations
At 6 months postsurgery, the rabbits were sacrificed and histopathological examinations were performed. The distal part of the right femur of each rabbit was dissected away from soft tissues and the tibia and incubated first in 10% formaldehyde followed by 10% EDTA for decalcification. Finally, samples were embedded in paraffin blocks. Afterwards, five 4-µm sections were obtained from the frontal plane of each prepared block and stained with hematoxylin–eosin and safranin O. Stained sections were evaluated quantitatively according to ICRS (International Cartilage Repair Society) 12 and Wakitani criteria. 13 The ICRS scale consists of parameters related to surface, matrix, cellular distribution, cell population viability, subchondral bone, and cartilage mineralization. A high score for each parameter indicates good-quality repair tissue. The Wakitani scoring system consists of parameters related to cell morphology, matrix staining, surface regularity, thickness of cartilage, and integration. A low score indicates good-quality repair tissue. Histopathological assessments were performed by a pathologist blinded to the study design.
Statistical Analysis
One-way analyses of variance were used to compare the ICRS and Wakitani scales among the 3 groups. For multiple comparisons, the least significant differences test was used. The ICRS and Wakitani total scores are shown as means and standard deviations. A P value lower than 0.05 was accepted as statistically significant. Statistical calculations were performed using commercial software (PASW, ver. 1.8, SSPS Inc., Chicago, IL).
Results
During follow-up examinations, 1 rabbit in the control group and 2 rabbits in MF and MFHA groups were excluded from the study because of death from unknown causes and development of systemic infection, respectively. Thus, the study was completed with 9 rabbits in the control group and 8 rabbits in the MF and MFHA groups. When the contralateral intact knees were examined during 6-month control visits, functional restrictions and decrease in ROMs (ranges of motion) of the operated knees were not detected.
On macroscopic examination of femoral condyles after sacrifice, defects obviously persisted in the control group ( Fig. 1A ). In the MF and MFHA groups, the defect areas were apparently filled with repair tissue, whereas the surface of the repair tissue was found to be uneven and ragged relative to normal cartilage tissue ( Fig. 1B , C ).
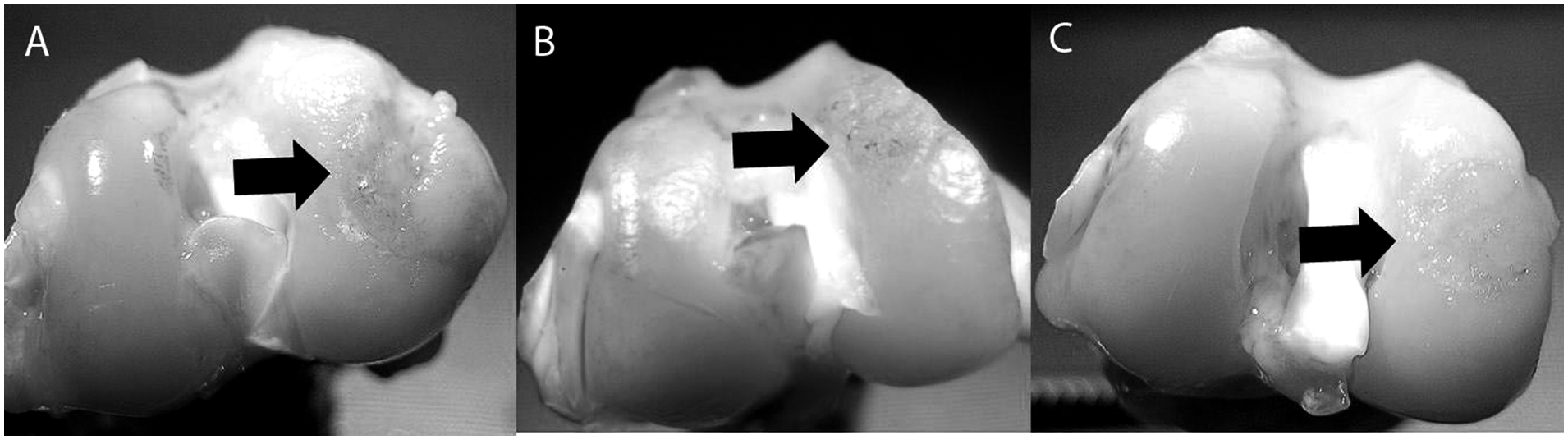
Macroscopic examination. (
In the histopathological evaluation, the regeneration of a marked repair tissue was not observed in the defects of the control group ( Fig. 2 ). In MF and MFHA groups, defects were found to be replenished with repair tissue, and safranin O staining was substantially less than that detected in the adjacent cartilage tissue around the defect with safranin O–stained sections. Also, in both groups, the cellular contents of repair tissues were different relative to adjacent cartilage tissue. However, an improved integration was observed histologically between the repair and normal cartilage tissues in both groups. The thickness of repair tissue was found to be less than that of the normal cartilage tissue ( Fig. 2 ).
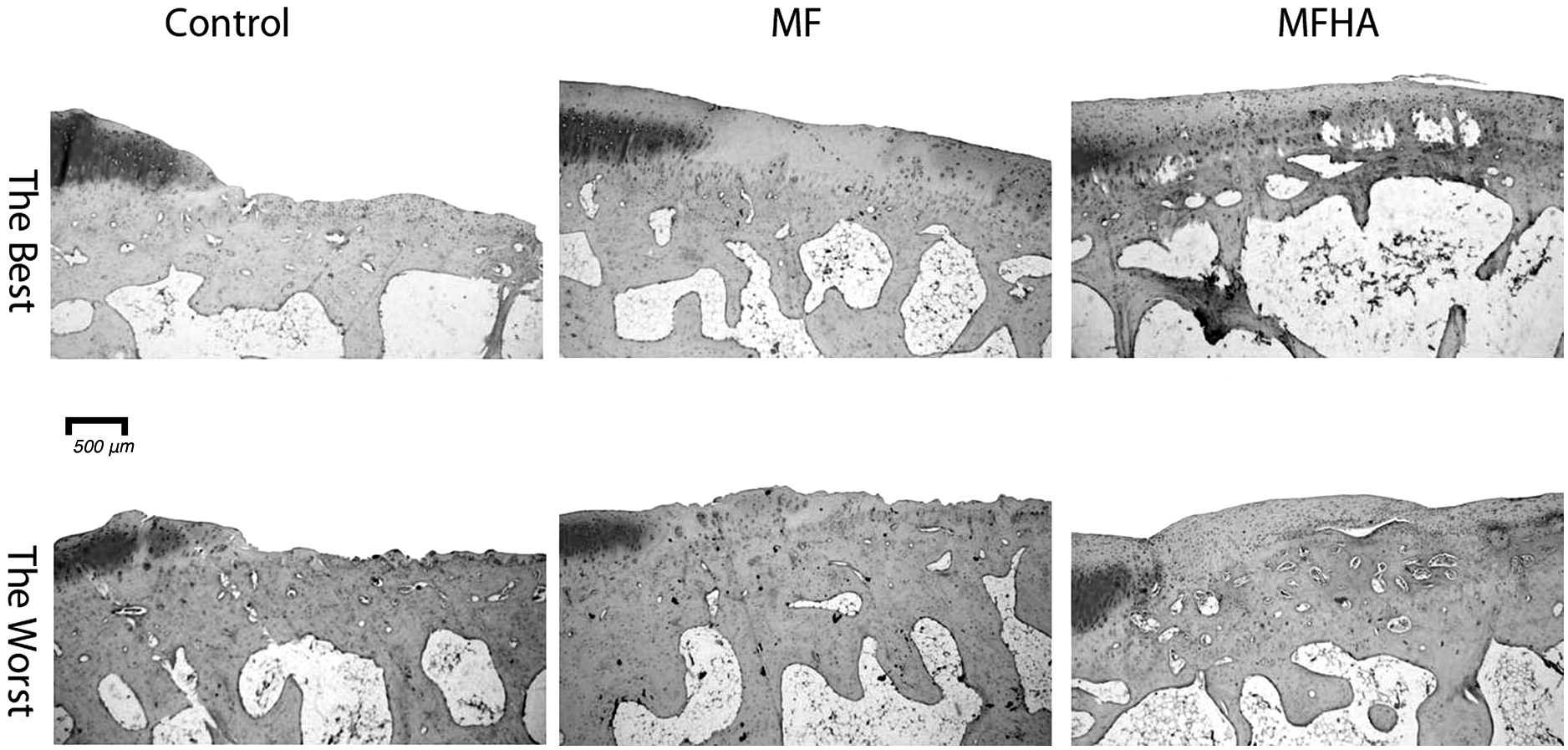
Repair tissues in safranin O–stained sections. The specimens with the lowest and highest scores according to Wakitani and ICRS scales in each group labeled as “The worst” and “The best,” respectively, are shown. In control specimens, there is no repair tissue in defects. Although some repair tissue in defects of both MF and MFHA groups can be seen, the thickness and proteoglycan content of repair tissue are lower than the normal cartilage. Surface integrity and integration between normal cartilage and repair tissue are similar in both MF and MFHA specimens.
The results of quantitative histopathological evaluations according to the ICRS and Wakitani scales are provided in Table 1 . In evaluations performed according to the total ICRS score, results obtained in groups MF and MFHA showed relative improvement, with a significant difference between both groups and the control group (P = 0.001 and 0.001, respectively). Despite a higher total score obtained in the MFHA group, scores did not differ significantly from those of the MF group (P = 0.342). With respect to the ICRS scale, among parameters other than those relating to the subchondral bone, a significant difference was observed in favor of the treatment groups when compared to the control group, whereas significant differences between the treatment groups were not detected.
ICRS and Wakitani Scale Values
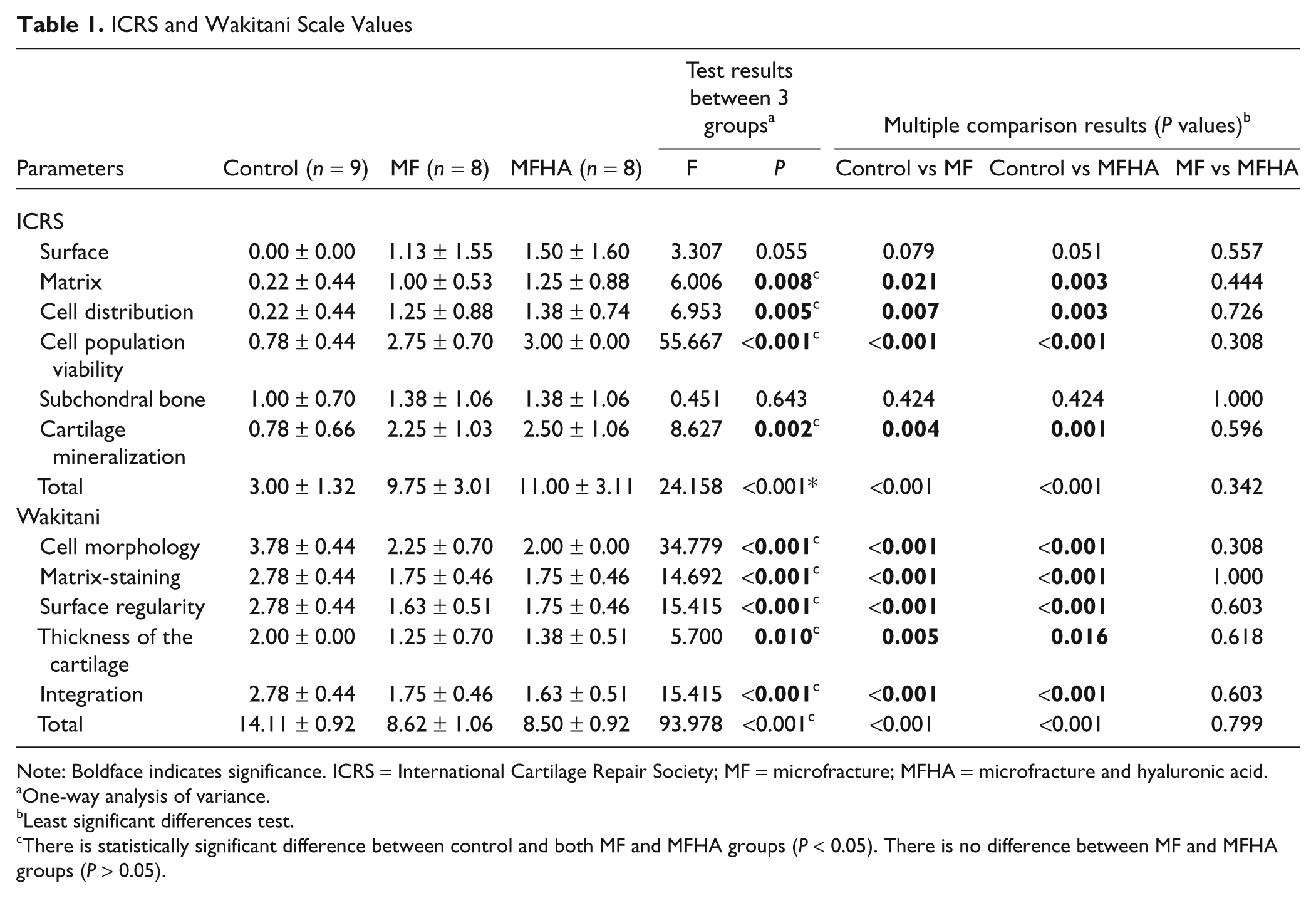
Note: Boldface indicates significance. ICRS = International Cartilage Repair Society; MF = microfracture; MFHA = microfracture and hyaluronic acid.
One-way analysis of variance.
Least significant differences test.
There is statistically significant difference between control and both MF and MFHA groups (P < 0.05). There is no difference between MF and MFHA groups (P > 0.05).
Assessment of Wakitani scores yielded results similar to those obtained with ICRS scores. The total scores of the treatment groups were found to be significantly lower than those of the control group (P = 0.001 and 0.001, respectively). Scores of the MFHA group were lower but not significantly different than the MF group (P = 0.799). Evaluations performed in accordance with Wakitani system parameters revealed a meaningful difference between the treatment groups and the control group, whereas no significant differences were found between the treatment groups.
As a result of evaluations of the ICRS and Wakitani scores, the MFHA group yielded more favorable results that were not significantly different from those of the MF group.
Discussion
In the management of full-thickness cartilage defects, after application of the microfracture technique, the defect area is packed with a “super clot” formed by bone marrow material. 1 In this clot, stem cells originating from bone marrow differentiate under the influence of environmental factors to form new cartilage tissue. Frisbie et al. 5 reported initiation of type II collagen mRNA expression at 6 months and induction of hyaline cartilage formation at 8 weeks after application of the microfracture technique. Mainly, the newly formed repair tissue is a mixture of fibrous and cartilaginous components. 14 Steadman et al. 2 claimed that physiologic remodeling of the newly formed repair tissue would take a long time to occur, and only 70% of normal and type II collagen content could be formed 1 year after the procedure. These researchers also reported a prolonged remodeling process of up to 2–3 postoperative years. 2 Supplementation of the microfracture technique with additional procedures is recommended both to shorten this process and to improve the quality of the repair tissue. 5 To this end, the microfracture technique was combined with placement of a type I collagen sponge soaked with BMP-7 (bone morphogenetic protein 7) in the defect area and good-quality cartilage repair tissue was obtained without causing degenerative changes in the joints. 15 According to the authors, the combined use of the microfracture technique and BMP-7 created a synergistic effect.
Hyaluronic acid is widely used for osteoarthritic knees. In some studies, it has been indicated that HA can modify the disease process and protect the knee from further degeneration,16,17 but its main effect is physical viscosupplementation. 6 Exogenous hyaluronic acid also has a viscosupplementation impact, in addition to its anabolic, analgesic, antiinflammatory, and chondroprotective effects. 6 In cultures of chondrocytes, hyaluronic acid increases DNA replication, the synthesis of glucosamine and hydroxyproline, and accumulation (storage) of type II collagen. 6 It has been stated that these effects are dose dependent.
Hyaluronic acid has been included in cartilage repair strategies because of the above-mentioned features, and various studies have been conducted to determine this effect. Jansen et al. 18 indicated that after partial lesions of cartilages, a single HA injection decreased cell death (apoptosis) and accelerated cartilage metabolism. Hyaluronic acid administration after autologous osteochondral transfer demonstrated an increase in the chondrocyte viability in a short period of time (3 months). 19
Kang et al. 9 also used microfracture technique and viscoelastic HA solution that is filled in the defect during surgery. In this study, microfracture technique was applied for full-thickness cartilage defects created on rabbit trochleas. Defects in one group were filled with 50 µL (0.5 mg) hyaluronic acid and those in the other group with a mixture of hyaluronic acid gel and transforming growth factor (TGF)–β3. The authors stated that they had detected improved repair tissue in the treatment groups but that TGF-β3 had not provided any additional benefit. However, no quantitative evaluation system was used in this study, and hyaluronic acid was used once during the surgical procedure. Both the application method and preparation of hyaluronic acid used in their study were different from those utilized in our study. Therefore, it was not possible to compare these results with ours. In the study conducted by Stauss et al., 10 after creating a 3-mm-diameter full-thickness defect on the weight-bearing surface of the medial femoral condyles of the rabbits, microfracture technique was performed through 3 holes. One week after the surgical procedure, 3 weekly hyaluronic acid injections were administered in one group and 5 weekly injections in another. For each injection, hyaluronic acid at a dose of 5 mg/0.5 mL was used. The ICRS macroscopic evaluation system and O’Driscoll histologic scoring system were used to determine effects of treatment. The authors indicated that they had obtained better-quality repair tissue in the group where hyaluronic acid was administered and could not find any difference between 3 or 5 injections at the third month. They also could not detect any significant differences in assessments performed at 6 months. They concluded that substantiating microfracture with hyaluronic acid injections had improved the quality of cartilage repair. They attributed this favorable impact to the chondroprotective and antiinflammatory effects of hyaluronic acid. This study showed some similarities to our study, including defect formation and injection techniques. However, the hyaluronic acid dosage was different. Also, the diameter of the defect formed was smaller than that constructed in our study. In addition, the authors considered defects with the smallest dimension of 4 mm in the rabbit model as spontaneously irreparable defects. 20 Despite these discrepancies, their findings at 6 months were similar to ours. Saw et al. 11 performed subchondral drilling on a 4-mm defect created on the trochleas of goats and then injected hyaluronic acid and cultured bone marrow cells into the defect area. They reported that better-quality repair tissue was obtained with hyaluronic acid plus cultivated bone marrow cell injections when compared with isolated hyaluronic acid injections. The authors attributed the impact of isolated hyaluronic acid injections to its neutralization effect on paracrine factors and its microenvironment-modifying characteristics. However, they ascribed the lesser efficacy of HA alone relative to their adjunctive use with bone marrow cells to the short-term effectiveness of HA. The mean half-life of HA injected into patellar joint spaces of sheep was 11.5 hours, 21 whereas it had a half-life of 24 hours when injected into the intrapatellar spaces of intact rabbits. 22 In the studies mentioned above, the authors stated that combining microfracture and exogenous HA injections has a beneficial effect in the treatment of full-thickness cartilage defects.
Bilge et al. 23 administered HA as 3 weekly injections beginning 1 week after microfracture procedure in the treatment of osteochondral lesions of the talus. Improvements in pain and functional scores were observed during the early postoperative period, and they concluded that hyaluronic acid injection did not create a statistically significant difference.
Despite potentially favorable effects of hyaluronic acid on the cartilage, the anticipated beneficial impact could not be obtained according to this study protocol. In this protocol, HA was used in a therapeutic regime and dosages identical to those used in clinical practices. Akmal et al. 7 demonstrated that the favorable effects of hyaluronic acid in chondrocyte cultures were related to the dosage used. Apparently, to achieve the outcomes revealed in such studies, the culture media must contain chondrocytes. Most likely, the administration of hyaluronic acid injections, after the development of chondrocytes in the repair tissue of the defect area, elicits favorable effects. Frisbie et al. 5 reported induction of type II collagen mRNA expression at 6 weeks and formation of hyaline cartilage at 8 weeks after the microfracture procedure. However, Gill et al. 24 have shown that the main healing process was realized between 6 and 12 weeks after the microfracture procedure and that the defect area was mostly filled with differentiated hyaline-like cartilage tissue. Therefore, modification of the timing of injections might yield favorable outcomes. The use of a fixed dose and time points for injections was a weak point of our study.
According to the methods used in this study, after a 6-month follow-up period, a substantial benefit could not be obtained from hyaluronic acid injections in addition to microfracture technique for the management of cartilage defect repair. We suggest that further investigations with different doses and injection times are needed for a better understanding of the effects of HA on repair tissue obtained by microfracture.
Footnotes
The authors received no financial support for the research, authorship, and/or publication of this article.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.