
Abstract
My practice-based research is situated at the intersection of design and healthcare. My research investigates what design can do, on the topic of death, inside the hospital. The methodological approach includes a systematic review of literature, codesign with informed consent and making practice. Death does not exist, therefore it needed to be constructed. My research constructed death theoretically through studies of physiology, psychology, culture, philosophy, and the social practice of death. I used these critical theoretical frameworks, amongst others to develop a visual cartography of death, which I now call the Bioscope. The Bioscope was designed as a tool to facilitate conversations about death. Engaging with the Bioscope can make you familiar with death and transform your understanding of it. Most people die in the hospital. I took the Bioscope to the hospital to improve and evaluate it via codesign with palliative care practitioners. Through the two codesign workshops at the hospital, I investigated what a cartographic mapping of death should look like. Insights from the participants in the codesign workshops informed the content of the Bioscope. The Bioscope has been prototyped as a tapestry embroidered on fabric. The four-part backdrop of the Bioscope allows it to be assembled, displayed, and used in various formats. It has 40 text-based sites and 27 ornamental icons that provoke conversation. My practice remakes death so that it can be spoken about in a sophisticated manner. The Bioscope restyles the banal into something that is beautiful and approachable. The story of crafting the artefact embodies and reflects on my transition research and creative practice.
Introduction
When the subject is death if it has not been said before – by philosophers, artists, religious thinkers, and other mortals – it is probably not true. (Fairfield 2014, 10)
This research is situated at the intersection of design and death. Historically there are several ways in which human beings, cultures and societies have been known to respond to death. It is possible to do many different creative projects on death, but it is a sensitive and complex subject. It is challenging to theoretically construct death to identify a scholarly project that is worth doing. Through this research I have cultivated a new creative practice with palliative care experts.
My research explores if there is room for intrusion into the medical space by creative people. This text invites you into my creative practice and reveals how I have learnt to think about death - as a designer, researcher, and a mere mortal. My research is empirical - therefore my text is often descriptive of my practice and sometimes performative.
Some of the questions I ask myself are: What is the way to do something in this kind of space? How do we talk about death and dying? Why have a lot of people not written about this kind of a topic? Why have they talked about death, but not so much about dying? What is the last 18 months of a persons’ life like? Why has dying been left to the medical people? Why don’t we have cultural constructions of dying or creative practitioners?
The Bioscope project has been carefully carved out of a broader practice. A neat outline of the project includes: a theoretical construction of death; the research design in relation to working with the hospital; securing approvals from hospital based Human Research Ethics Committees; the co-design workshops; the data analysis; the making practice; and my reflection upon the designed outcome. This text is divided into three sections namely: theory, codesign, and creative practice.
Theory
Death is a very interesting problem, but nobody really knows what death is. There are multiple ways to approach death. For example, death can be culturally constructed. The anthropology of death is fascinating, and it usually focuses on after-death-care rituals. Murray (2011), in her book, Making an Exit explores end-of life practices from around the world. She writes of the figurative coffins from Ghana, which are a popular case study in the work of many scholars, including Bonetti (2012) and de Witte (2003).
Medical anthropologist Sjaak van der Geest in his article “Funerals for the Living: Conversations with Elderly People in Kwahu, Ghana” observes that, “the Akan society of Ghana [...] seem more interested in post-mortem than in pre-mortem care”. Geest suggests that caring for a person while they are alive is more important than caring for them after they have died (2000, 104–107).
There is a distinction to be made between death and dying. During World War 1, Alan Segar wrote the poem “I Have a Rendezvous with Death” (1916, 144). When writing the poem, Seeger would have been in Europe, it may have been raining on that winter day and he may have been in the trenches. In the last paragraph of his poem Seeger writes: God knows 'twere better to be deep Pillowed in silk and scented down, Where Love throbs out in blissful sleep, Pulse nigh to pulse, and breath to breath, Where hushed awakenings are dear ... But I’ve a rendezvous with Death At midnight in some flaming town, When Spring trips north again this year, And I to my pledged word am true, I shall not fail that rendezvous.
Seeger died in battle soon after he wrote the poem. He saw it coming. Almost like when a person is diagnosed as terminally ill. The last 18 months of life following a terminal diagnosis in a hospital are considered as palliative.
Jacqueline Watts, a British Academic teaching at the Faculty of Health and Social Care, states that “sharing the writing of poetry with terminally ill clients can enable expression of individuals’ deepest unspoken concerns, those of both the client and the carer.” (2009, 104).
So, death and dying can be creative constructs too. Death does not exist, but we can metaphorically think of it as a door between two places. Death is a social construct, that marks a transition from dying to after death.
Historically death has been mediated by religious practitioners. Following the death of God, the hospital has colonised death. Jurgen Habermas, as quoted by Fairfield (2014, 48) to illustrate a point, describes a new age secular funeral without a religious ceremony held at a church in Zurich. The discomfiture of the entire event, as recounted by Habermas, makes it evident that the shift from a religious ritual to a more secular one caused a tremendous loss of meaning. Following the colonisation of death by the hospital we have lost the socio-cultural know how of doing death. Philosopher Paul Fairfield in his book, Death: A Philosophical Inquiry, states: The advantage of the secular death is that it is free of illusion, mythology and false consolation. The disadvantage, in a word is that it is also empty [...] A secular age replaces the priest with the doctor, lawyer, undertaker, and psychiatrist and not one of these managerial roles is able to tell the dying or the grieving what any of it means. These are service providers, not interpreters of the human condition and the consequence of our excessive reliance upon them is that death has become quite literally a meaningless event. (2014, 49–50)
Most philosophers have something to say about death. The philosophy of death and dying focuses upon a theoretical construction as opposed to the sociology of death and dying which focuses upon its practice. Cameron Tonkinwise, Professor of Design Studies, observes “‘the practice turn’ in sociology and anthropology” which gives a traditionally theory and field-based discipline access to practice (Yee et al. 2013). As a designer, I am interested in using theory to inform my creative practice and trigger social transformation.
Examining the sociology of death helped me identify and map my field of practice. Aubrey Incorvaia in her article “Death Positivity in America: The Movement-Its History and Literature” states: Death-Positive or Positive Death Movement are frequently used terms; previous scholars have also referred to this era as the Happy Death Movement. Yet others frame the phenomenon, more generally, as falling within the Death and Dying Movement or as the ongoing expression of the Death Awareness Movement. Regardless of naming convention, the consensus is that a movement has begun and is underway. (2024, 17)
Is the Death Awareness Movement a response, to the recent hegemonic colonisation of death by the hospital? This heightened era of death awareness is evidenced by the emergence of Death Cafés, Death Over Dinner events, the services of end-of-life doulas, the Voluntary Stopping Eating and Drinking practice and the shift towards green burials (Incorvaia 2024, 17).
The hospital however is the preeminent site that provides care at end-of-life. American Physician Cassell (1974, 31–32) observes that the death in the hospital is a technological death, where the doctor focuses on the physiology and treats the patient’s body as a mechanic would repair a car. Is there is an absence of empathy and imagination in the technological death? Is that why the Palliative Care Physician BJ Miller asserts that “healthcare was designed with diseases and not people at its centre. Which is to say that it was badly designed. And nowhere are the effects of bad design more heart-breaking or the opportunity for good design more compelling than at end-of-life” (2015).
The medical profession helps us to manage pain and prolong life. However, doctors are not well poised, to prepare us for death and dying. In her article titled “Good Deaths, ‘Stupid Deaths’: Humane Medicine and the Call of Invisible Bodies”, with reference to the hospice movement, Maura Ryan states that “in principle, the turn to the whole person should have been a powerful antidote to the pathologies of the anatomo-clinical model. However, Bishop shows that palliative care, aimed at addressing pain and suffering comprehensively, suffers from the same reliance on a functional metaphysics as medicine more generally and, therefore, the same blindness” (2016, 647).
This is to say that in the hospital – death is seen as a physical malfunction, an evil to be defeated, a problem to be solved, and not as a natural end to life. My research was embedded in the hospital, but it seeks to de-medicalise death. It seeks to empower people, with the ability to confront their own mortality.
In the 2022 “Report of the Lancet Commission on the Value of Death: bringing death back into life”, Libby Sallnow et al., observe that: Although death and dying are increasingly controlled by health systems, most care of the dying, hour by hour, is the responsibility of the dying patients themselves, family, friends, and the community. When patients are in hospital nurses spend about 5 percent of their time in face-to-face interactions with patients and doctors spend only about 13–15 minutes a day in contact with an individual patient. The time spent with patients dying at home is even less […] 95 percent of the care of the dying is undertaken by lay communities despite the dominance of healthcare systems. (2022, 853)
Our own care and that of our family, at end-of-life is often thrust upon us. But we no longer know how to deal with it, because death is invisible on the social landscape, because it is a taboo subject. Not knowing and not being able to act, to support better experiences at end-of-life, can result in a feeling of negligence and guilt.
During codesign enabled conversations with palliative care practitioners at Peter MacCallum Cancer Centre, Geraldine McDonald, Director of Prevention and Wellbeing and stated that “If you get cancer, you got to go to cancer school. You have to learn a new language; you have to learn how to advocate and how to access”. An experienced healthcare practitioner, McDonald emphasises on the importance of developing better systems for wayfinding and patient navigation at end-of-life.
One of the more significant problems that the idea of death poses, is the existential anxiety and suffering associated with the dying process. Doctor Ira Byock in his book Best Care Possible clarifies that “Dying doesn’t cause suffering, resistance to dying does” (2012).
An evolved death awareness can help us, to overcome denial and accept our own mortality. It can also prompt a profound awakening to life, which is the idea of authenticity, that Heidegger refers to in his work Being and Time (Blattner 2007). An evolved awareness of death can be cultivated through talking about death. A tool is required to talk about death and dying.
I have developed the Bioscope, as cartography of death and a tool to facilitate conversations about end-of-life. The word bio translates to ‘life’ in Latin, and a scope is a tool that allows us to look at things. The concatenated word Bioscope contains the meaning ‘looking at life’. The deepest truth for any living thing is, that 1 day it will cease to exist. In this way life and death are intertwined. The deep truth of death is more powerful than the sun itself, more powerful than religion, than philosophy, than the economy and even science. Because it is only death that is certain.
Codesign
Initially I used literature to develop the Bioscope (Figure 1). This early cartography and proposed tool for conversations needed to be evaluated. I took the Bioscope to the hospital, to be improved and evaluated, via codesign enabled conversations about death with palliative care practitioners. The project became situated at the Alfred Hospital through securing an ethics approval from the hospital-based Human Research Ethics Committee. Early version of the Bioscope constructed using literature, as a vector artwork on Adobe Illustrator.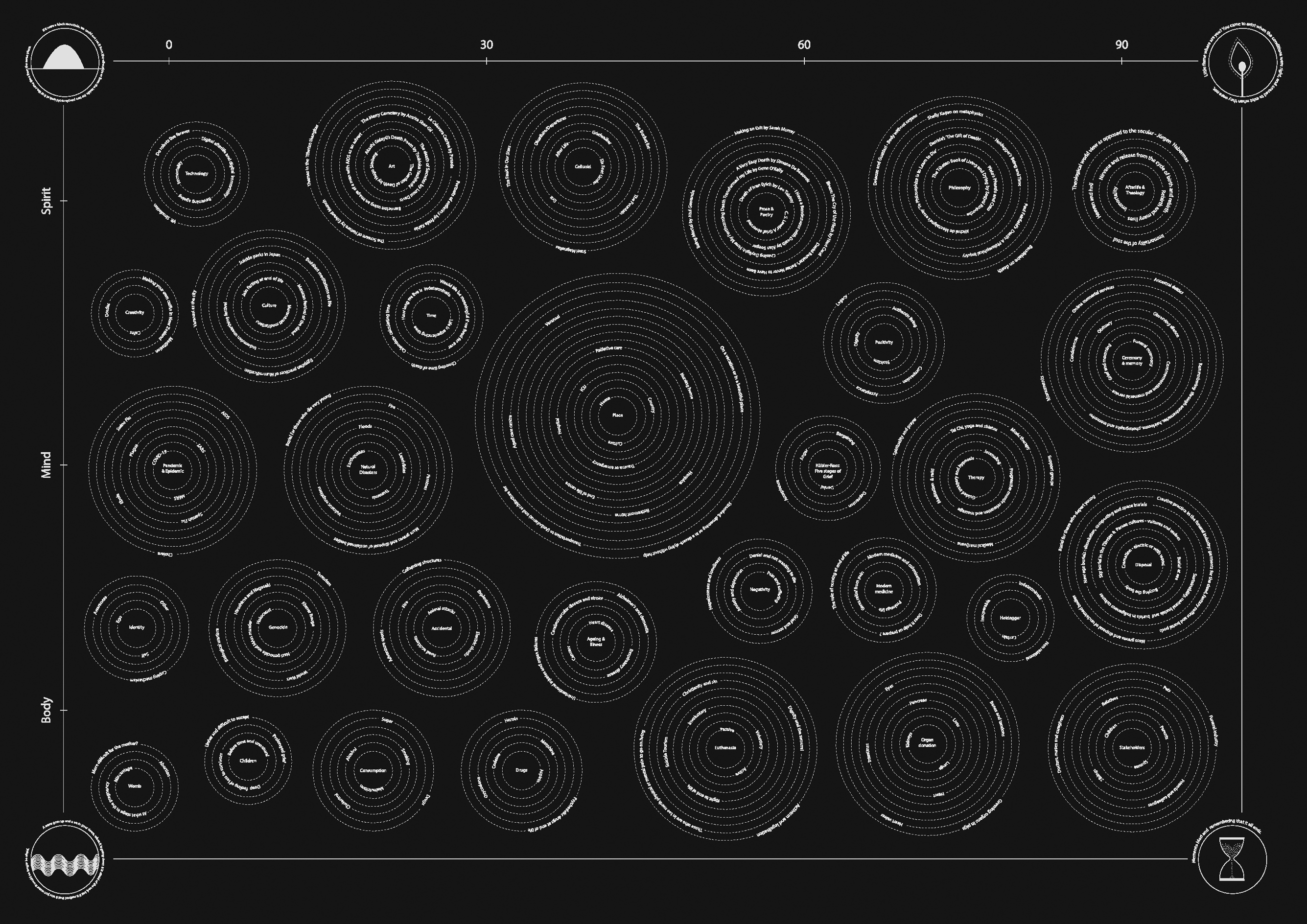
My starting point for participant engagement, was the Experience Based Co Design method (Donetto et al. 2015) - which involves all stakeholders in the codesign process. My overall strategy was to use the Bioscope, to engage with caregivers and patients, following a first stage of development with palliative care practitioners. Developing the Bioscope with palliative care practitioners, made it more sensitive to the needs of people at end-of-life. I did not involve patients or their families in the codesign activity because they are vulnerable as research participants.
My ethics application requested for 2 hours of clinician time, because clinician time is precious. I planned to do two workshops of 1 hour each, over a period of 1 year. This allowed me time for recruitment, securing consent from participants, data management, analysis, design, and planning before and after the workshops.
The Death Café and Death Over Dinner events, use the World Café Format, it became the obvious choice, to facilitate my codesign activity or focus group study. However, due to the COVID-19 pandemic, access to the hospital became restricted. I had to transition to digitally enabled codesign (Figure 2). I recreated the World Café format online using breakout rooms. The digitally enabled setup was limiting, because of the screen-based format and because of the inequitable digital literacy of participant groups. Illustration of the zoom workshop with all the participants in the main session during introduction, summaries, and conclusive remarks.
It seemed that the best way to do the workshop, would be through conversation-based sessions, using simple trigger images. The Bioscope has many locations or sites because it is a cartographic mapping of death. I was able to extract sites from the Bioscope, to use as trigger images. In the first workshop, I tested two sites to understand what they meant and what they should be (Figure 3). One of the Bioscope sites used in Workshop 1 was titled place. The site was used along with the trigger question: ‘When you look at this image or at these words, what does it bring out for you? What are your responses and reactions?’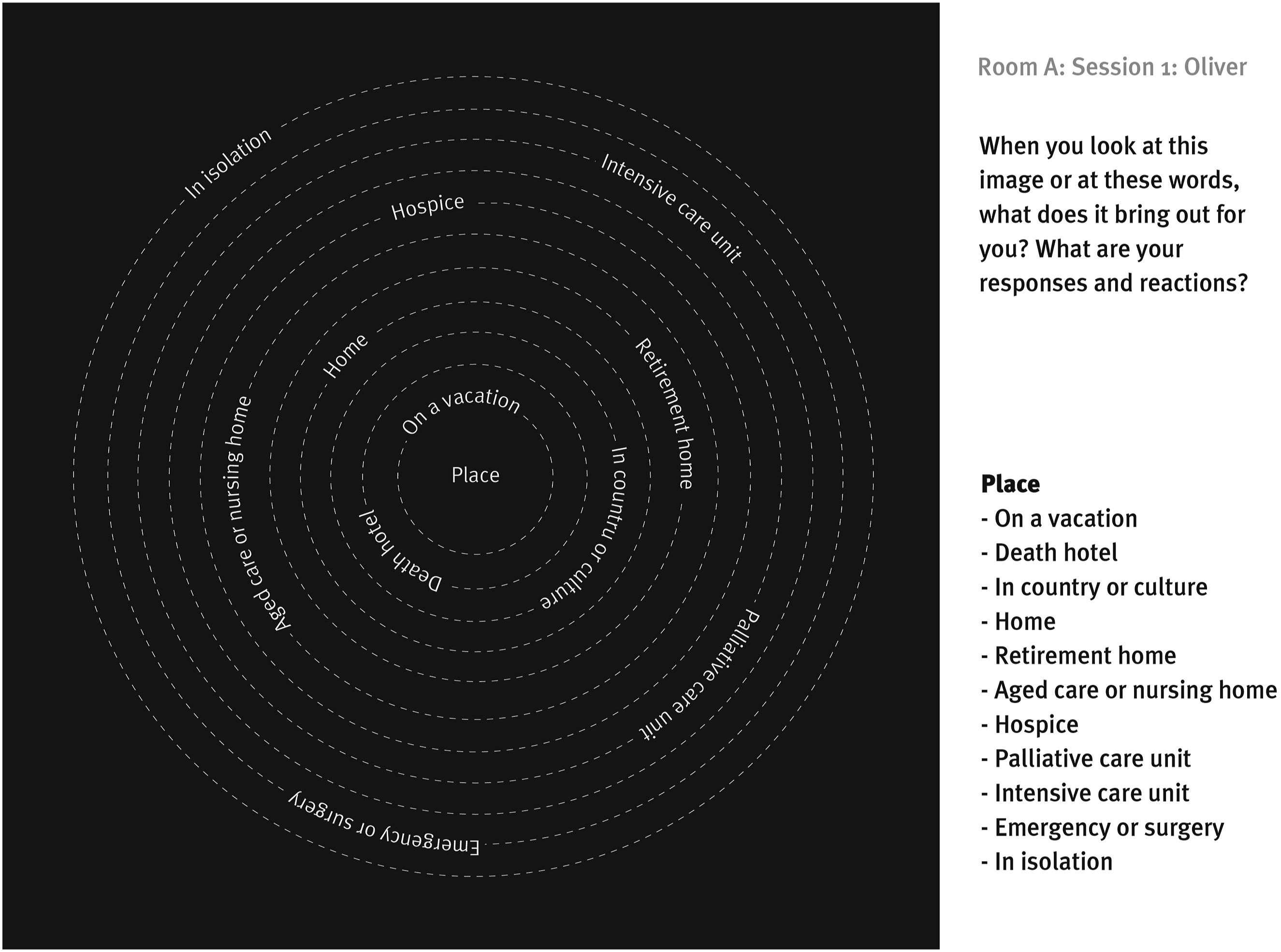
One of the sites was called Place. The clinicians discussed it at length. For example, a physician observed that “on vacation sounds like a nice way to die, but in reality, I mean I don’t know how many people can”. Another clinician stated, “There’s something about planning things in birth and death that never quite go according to plan and that is just both the challenge and the beauty of it, you know.”
Eventually, I understood that there are only four, predictable options with reference to place and death. And they are:
Dying at home,
Dying at residential aged care facility,
Dying in a hospice, and
Dying at the hospital.
Certain conversations are encoded into the sites. Alongside the project at Alfred Hospital, I had another ongoing ethics approved project, at the Peter Mac Callum Cancer Centre. As part of the study at Peter Mac, I was able to shadow a doctor, on his routine rounds of the palliative care unit. Here I witnessed the doctor having a conversation, about place and death with a patient and their family. Often people may prefer to be cared for at home, however, when the burden of care becomes too much for the family and caregivers the patient may choose to move to a hospital.
The data from the first workshop, gave me a good understanding of how Palliative Care Practitioners think and talk about death. I was also able to better understand how I should construct and populate the sites on the Bioscope. For example, it became important, to use language that is consistent, across existing palliative care material.
In the second workshop, the overall structure of the Bioscope and its sites was broadly reorganised. It was interesting to observe how the clinicians examined certain sites. For example, a palliative care practitioner asked, “Just with Kubler Ross stages - have been superseded or are they still relevant in the discussion around death?”
Another palliative care practitioner responded, “I think it’s very clear that it’s talked of in a linear progression of griefs, and it looks like that would not be the case of how we would talk now. But I think because it’s such a big, and seminal piece of work I would be in favour of having it there. And because I still think that it's a launching pad for where you are on this, and I think it’s really a nice way to normalize that things don’t happen in a linear fashion.”
The two workshops helped refine and develop the contents of the Bioscope. It became evident that the sites on the Bioscope were useful triggers to facilitate conversations about death and dying. More importantly it became evident that the clinicians benefitted from these conversations. A physician participating in the codesign workshop observed that, “I personally think it’s invaluable to have these discussions and I don’t think we have them enough or more importantly we don’t possess all the skills to have them […] so this is a good sort of way to explore all avenues to get to those fruitful discussions about what the true values of the patient are.”
During the workshops the Bioscope became a collective experience - a cartography constructed together to reveal a nuanced understanding of death and dying that the clinicians at Alfred Hospital now share with each other.
To me the pharmacological sites were more fascinating. However, the physicians loved the sites about art, poetry, and especially philosophy. To quote a participant, “Surely, the specific advice about the medications, neuropathic agents or opioids is something that you are going to discuss with your doctor. Whereas this is something that people cannot discuss with the doctor. They might discuss it in the Cafe and may get a lot more out of this. This is a much bigger way to approach death and living? Or a much fuller way. I think these things are very important to remind clinical staff as well. You know, people are made up of a whole lot more than just a list of medications and diseases.”
The Bioscope and its sites are not fixed. They can change. There is no custodian of what should be inscribed on it. A return to theory may result in the addition of more sites, and further restructuring. Taking it to a different hospital for codesign may also shift it. I continue to speculate on how it should grow and evolve.
I have observed that people who have experienced loss or confronted mortality, feel drawn to the Bioscope. The object can bring conversations and experiences, related to death and dying to the fore. Different things are meaningful to different people, so patterns of participant engagement are also significantly different. Some conversations can be more intense and confronting than others. For example, the nature and seriousness of a conversation about after death care, is different from a conversation about death and place, or about Voluntary Assisted Dying. However, I imagine that it is important for the Bioscope to hold space and allow for every kind of conversation.
People can often feel overwhelmed by the scale of the Bioscope at first, and there is usually some time between first contact and response. What is interesting is that people respond to the Bioscope, like they respond to the taboo subject of death. And this is so, despite me taking care to not use the word death on it. Of course, doctors are comfortable with the term, so now it appears in a few places on the Bioscope. Otherwise, the Bioscope would have been cartography of end-of-life, that did not directly refer to or use the term “death” at all.
Creative Practice
By the time I had completed the codesign, as per the protocol outlined in the ethics application, the restrictions imposed by the pandemic were beginning to ease. At this stage, I could have taken the Bioscope, back into the hospital for a third time, so that the palliative care practitioners could perfect its content. However, I really like to make things. The digital images of the Bioscope and even the early prints on the fabric did not do justice to its content.
As the codesign activity was coming to an end, I began to invest a considerable amount of time to become familiar with the process of digital embroidery (Figure 4). I made test samples on different fabric swatches, using different coloured threads (Figure 5). I tested lines and line thicknesses, fonts, and font sizes. I identified a legible size for the text, a good contrast value and a colour scheme. Barudan embroidery machine at work, in the Machine room, Industrial Design Makerspace, RMIT Building 515. Testing colour schemes, threads, fabrics, and lines.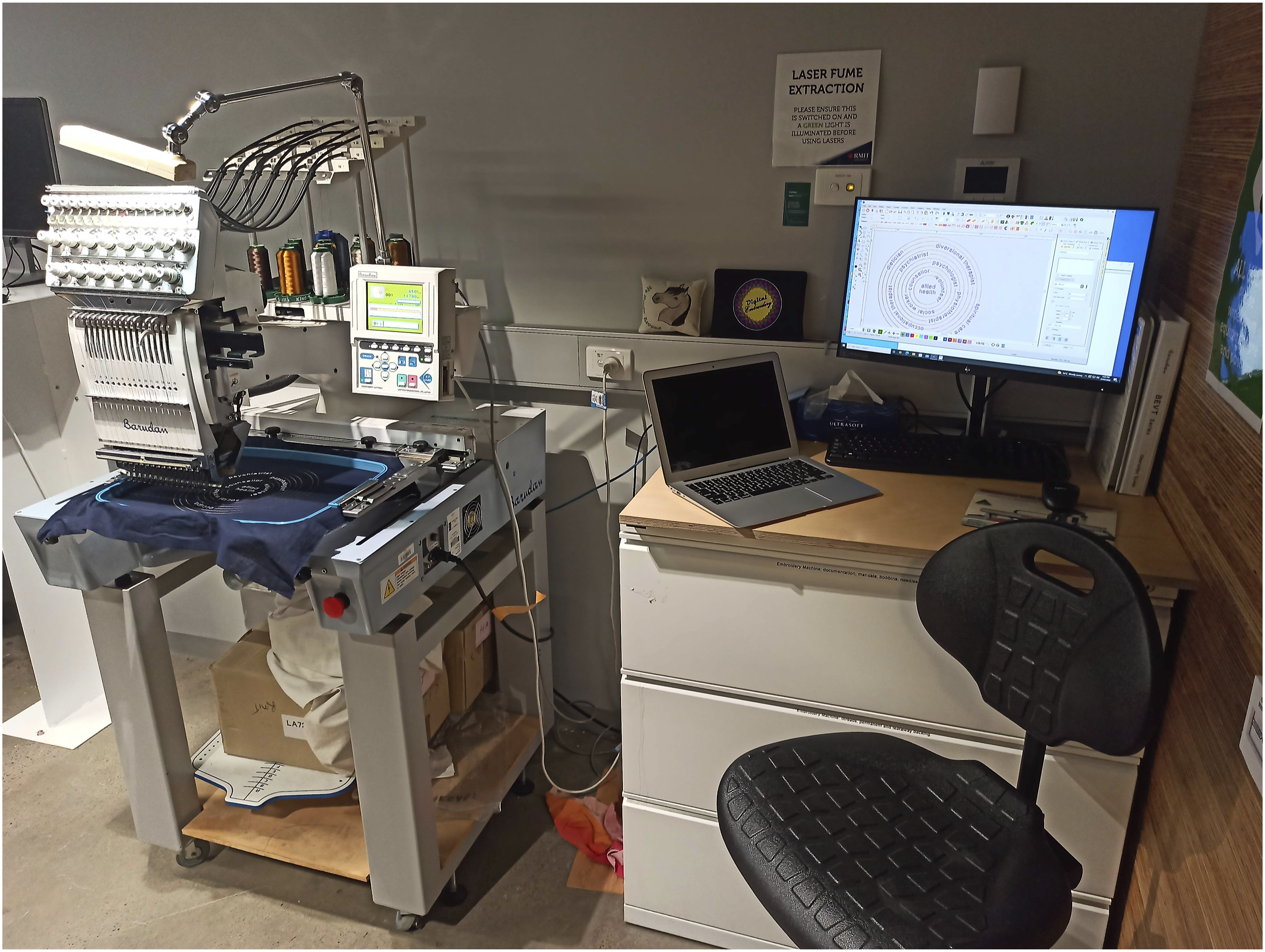

Death is often spoken about in metaphors. In Cambodia, I came across the tung or the crocodile flag. In his book Death Power: Buddhism’s Ritual Imagination in Cambodia, Eric Davis observes: the acharya, or a member of the family, will usually post a white Dang Kraboe, or ‘crocodile flag,’ at the entrance to the deceased’s property, signifying that there has been a death. The origin story of the crocodile flag concerns the tragic death of a princess eaten by a crocodile. Her father captured the crocodile and cut it open in an attempt to save her, but was too late. The king posted the crocodile’s skin near her funerary monument, and this was taken as a model for the cloth and paper crocodile flags. Two large crocodile flags are flown outside of the vihara on tall flagpoles as a necessary part of a proper temple. (2015, 57)
The crocodile flags in Cambodia are now made in fabric. The bigger ones for the monastery, are stitched together by the community (Figure 6). The tung inspired my first visualisations of the Bioscope tapestry. Crocodile tung at the Lower Wat Phnom Krom Pagoda in Siem Reap, Cambodia at the funeral of the founding monk of the monastery. Photograph on 14 Jan 2020.
Fabric can be thought of as second skin - soft and tactile. It can be kept on the body, on a table, on a bed or hung on the wall. The embroidered text on the fabric needs large counters. The embroidery provides texture. Senses that may have become dull with age or illness, are likely to respond well to large text and haptic feedback.
The Bioscope was embroidered in fragments, because of the size of the embroidery hoop and because a seamlessly embroidered piece would never get completed - owing to the frequency of man-made and machine-made errors that occur during the embroidery process.
Once the sites had been embroidered, it would have been easiest to stitch the many site fragments, together into one tapestry. But this would mean that the sites, and their proximity to other sites would become permanently fixed.
During the codesign process I realised that people like to change and reposition the sites. Some sites work better together in certain contexts. I confess that I have personally enjoyed curating the Bioscope sites using different thematic and taxonomical frameworks. And so have others.
When it was time to make the Bioscope, I was thrilled and eager to make something in such a large scale. The Bioscope became a labour of love, and it took me over 600 hours of machine embroidery. It was important to make the Bioscope as an object, because it is difficult to look into people’s eyes and talk about death. Death is intense – and that is why Duc De La Rochefoucauld (2017, maxim 26) says that ‘Death, like the sun cannot be looked at steadily.’
If you provide an object, then people can look at the object and talk freely. The object becomes an anchor and allows us to keep returning to the subject of conversation. The cartographic format with its many sites is also important, because it covers a large terrain populated by many conversations.
In a Death Café, the participants and the facilitators tend to bring, only their own thoughts and understanding of death to the table. Having a cartography or a map allows for new conversations to emerge, and for new territory to be explored.
The way death is spoken about in the hospital is technical and banal. The Bioscope had to be beautiful, because it makes death accessible and invites people to engage with it. The Bioscope I made also had to contain, the infinite respect that is owed to the dying. The artefact had to be awe inspiring – I wanted it to hold space for contemplation, but I also wanted it to be able to give voice.
Eventually, I assembled the Bioscope using a four-part backdrop, that can be zipped together (Figures 7 and 8). This modularity allows it to be assembled and displayed, in variety of different permutations and combinations. Every individual site can be easily removed or replaced back onto the magnetic backdrop. In a Death Café setting you can pick any site and take it to a table for a conversation. Building modularity into the Bioscope, made its construction more complex, but it also made the artefact more versatile. The Bioscope has a fluid structure, which allows us to approach death, and navigate conversations about end-of-life, in a multiplicity of ways. The fully assembled Bioscope as on 16 March 2023. Closeup view of a portion of the Bioscope.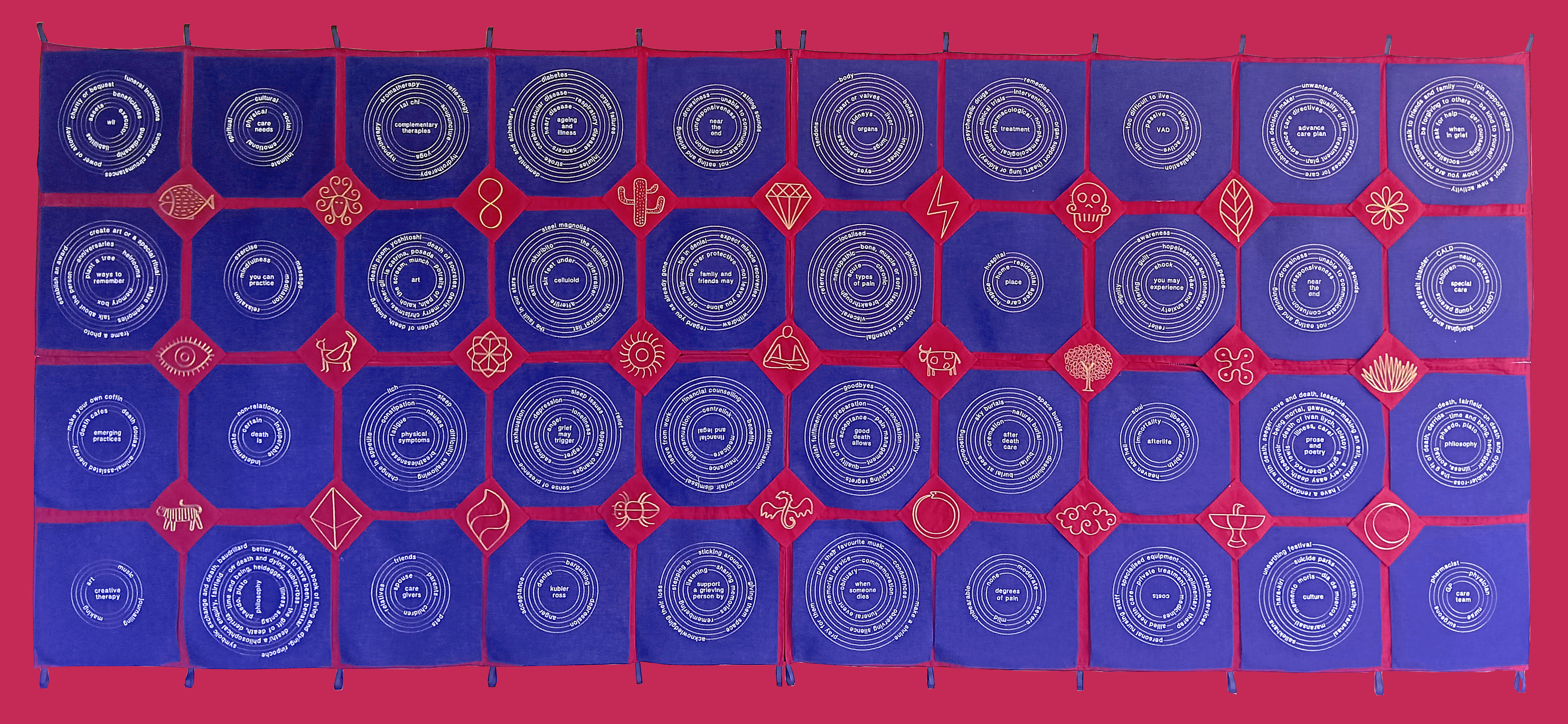

I see the Bioscope as a place-maker because it can by its mere presence create a space for conversations - about death! It is the first such cartography of death, and the clinicians at Alfred Hospital observed that they do not have access to any other such tool at present.
Conclusion
On one Thursday afternoon in October 2023, after completing my dissertation, I took the Bioscope back to Alfred Hospital to show it to the doctors. The materiality and aesthetics of the Bioscope had a profound impact on the doctors. The doctors engaged with the object for one full hour, and their response was heartening. The doctors wanted to use the Bioscope with patients.
The Director of Palliative Care at the meeting suggested that “the Bioscope is something that should be adopted by all palliative care settings in Australia.” This was a big win for me! As Bon Ku and Ellen Lupton, in their book Design for Health, observe “Change is difficult in a hospital, where mistakes are costly and can seriously damage human lives. Not every proposal is implemented, and not every intervention succeeds. Change requires the space and the courage to test new ideas. Human-centred design is one crucial tool for distributing medical advances to more communities, not just to the most privileged” (2020, 18).
It is not difficult to talk about death, but there are many ways, to think about significant moments like death. But what is the right way to talk about death in the hospital? This has not been explored, and the people who are wanting to say things, are not very sure about the right way to say those things. In doing this project, I have realised that there is no right way. There never will be a right way. There will perhaps only be ways - that individuals will have to construct. They will have to be authors of their own ways, but the giving of permission is what my project does. Having a Bioscope and using the Bioscope gives agency to patients, gives agency to staff, gives agency to carers, gives agency to relatives and gives agency to children.
In the palliative care context design for transition may take on a specific meaning. In the article “Transitions as experienced by persons in palliative care circumstances and their families – a qualitative meta-synthesis” the authors state that: Transitions are a phenomenon of change affecting individuals and groups. In Transitions Theory, people are described as more vulnerable to health risks while experiencing transitions. In palliative care, transitions are characterized by individuals experiencing a change due to deterioration or improvements of their health status […] For persons with palliative care needs, experiences of transitions are accompanied by distress and feelings of disruption, as transitions often occur suddenly and confront persons with palliative care needs and their families with new life situations. (Fringer et al. 2018)
The journey from good health to death is a transition that needs to be navigated with care. The theory of change that inspired the Bioscope project was seeking to support better experiences at end-of-life by helping overcome denial through enabling an evolved awareness of death. Initially I had imagined that different hospitals would commission me to make more Bioscopes. The vision of project Bioscope is to normalise conversations about death in Australia and around the world. This requires the Bioscope to be adopted for use in community-based settings. I am developing a pro bono practice that uses the Bioscope to facilitate conversations about death at my local community centre in Melbourne. This is part of my ongoing practice that seeks to embed the Bioscope in community-based settings and to evaluate its impact.
I recently spoke about the Bioscope project at the Design Outlook Conference in Melbourne 2024. I developed a slide that was intended as a pun on what a typical journey map might look like (Figure 9). A journey map of our lived experience shared at the Design Outlook Conference 2024.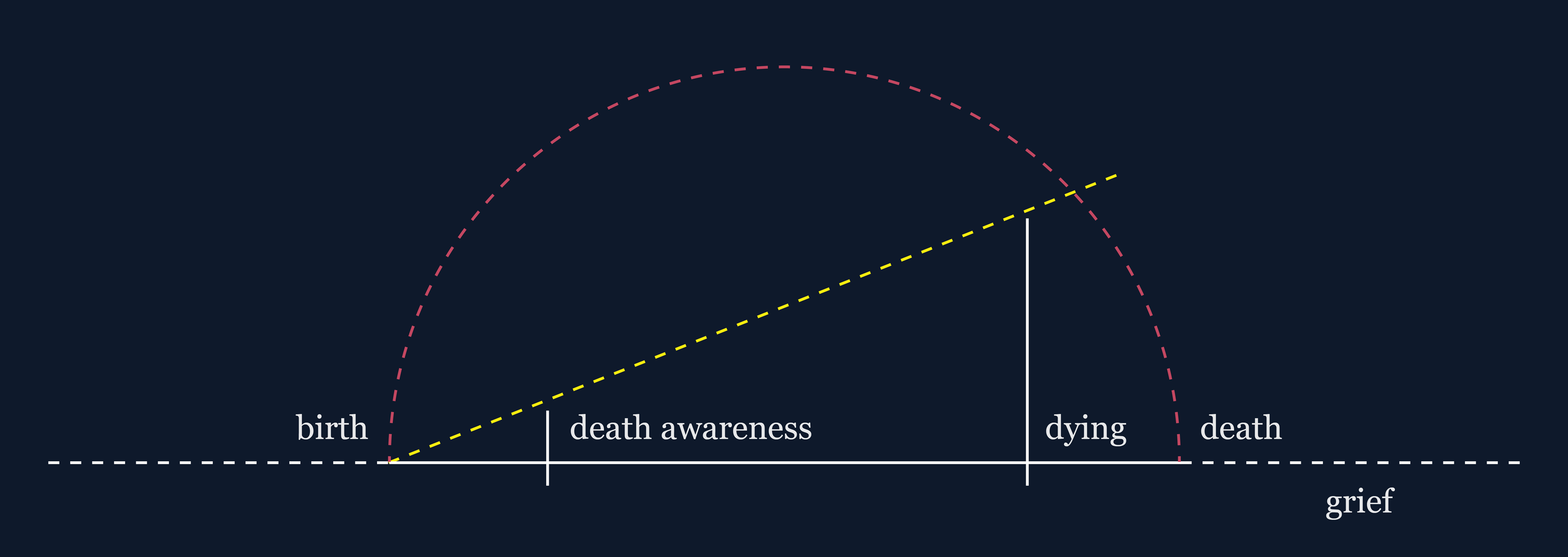
However, this model (Figure 10) has now become definitive of my design practice which seeks to design for birth, for death, for care between these two life events, for the relationship of our species to the ecology and for our relationship to society. A model that has become definitive of my design and research intentions.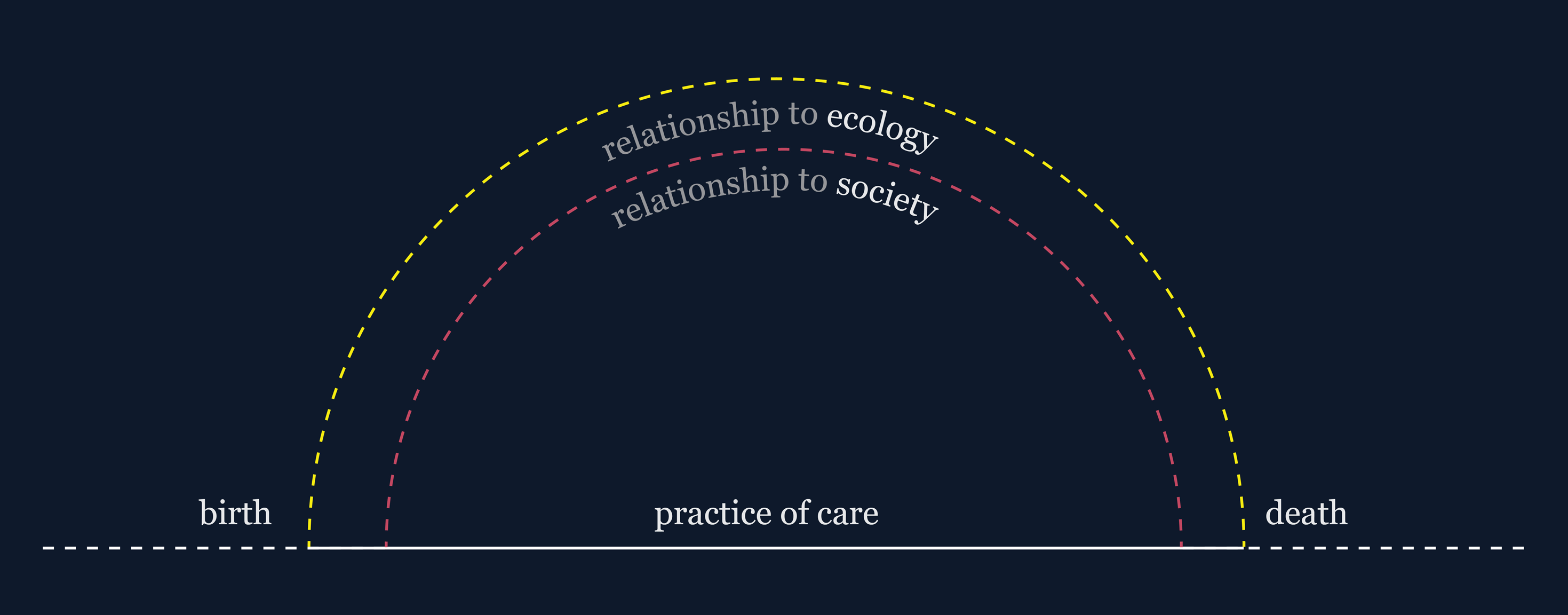
The article “Transition Design: An Educational Framework for Advancing the Study and Design of Sustainable Transitions” identifies one of the distinguishing characteristics of Transition Design as “Designing solutions that protect and restore both social and natural ecosystems through the creation of mutually beneficial relationships between people, the things they do and make (design) and the natural environment” (Irwin et al. 2020).
To some degree my model of practice resonates with the distinguishing characteristics of Transition Design. The Bioscope project is a Transition Design case study specifically design for death and dying. The project makes a bridge between design and the hospital. I believe that many more designers need to work within the hospital, because they bring different perspectives, and they make different things. Like the Bioscope that I have made.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.