
Abstract
Background
Sinonasal pathology, such as chronic inflammatory disease or neoplasm, can cause secondary nasolacrimal duct obstruction (sNLDO). There is a paucity of data on dacryocystorhinostomy (DCR) techniques and outcomes for NLDO secondary to known sinonasal pathologies.
Objective
To describe case characteristics, management, and surgical outcomes of sNLDO at a tertiary academic center.
Methods
Charts of DCR cases with at least 3 months follow-up done at a single institution over a 5-year period (2018-2022) were reviewed. Patient and surgical characteristics were recorded and compared between secondary and primary NLDO groups. The primary outcome was early functional success of DCR, assessed by improvement or resolution of epiphora at 3 months.
Results
A total of 236 cases were included. Of those, 79 (33.5%) were classified as secondary NLDO associated with sinonasal pathology. Reasons for sNLDO were sinonasal cancer (46.8%), chronic inflammatory disease (24.1%), trauma (16.5%), or prior head and neck radiation (31.6%). When comparing primary acquired NLDO to sNLDO cases, DCR for sNLDO was more likely to be performed endoscopically (68.4% vs 31.8%, P < .01), by a multidisciplinary team of rhinologist and oculoplastic surgeon (70.9% vs 8.3%, P < .01), and required bilateral surgery (36.7% vs 5.7%, P < .01). The overall functional success rate was 79.7% for sNLDO compared to 87.9% for primary acquired NLDO (P < .01). Revision surgery for sNLDO, history of sinonasal malignancy, and radiation were associated with lower functional success rates (66.7%, 70.3%, and 68.0%, respectively). Canalicular pathology was more common in sNLDO cases (29.0% vs 8.3%, P < .01).
Conclusions
Secondary NLDO was more commonly managed with an endoscopic approach by a multidisciplinary team. Revisions for sNLDO, as well as cases with a history of sinonasal malignancy and radiation, had a markedly lower success rate, and sNLDO was frequently associated with canalicular obstruction. These findings may facilitate surgical planning and patient counseling.
Keywords
Introduction
Dacryocystorhinostomy (DCR) is the surgical standard of care for treatment of symptomatic nasolacrimal duct obstruction (NLDO) and may be performed by oculoplastic surgeons or rhinologists. While most cases are classified as involutional without identifiable cause and referred to as primary acquired NLDO (pNLDO), obstruction can also occur due to sinonasal pathology such as neoplasm, radiation, midface trauma, iatrogenic disruption in prior sinus surgery, or chronic inflammatory disease affecting the nasal and sinus mucosa. 1 This is classified as secondary acquired NLDO (sNLDO). The success rate of endoscopic and external DCR for pNLDO is around 90% across many multicenter studies and meta-analyses. 2 However, it must be noted that success rates can decline over time, and late failure may not be captured in some studies. In comparison, there is a paucity of data on DCR for sNLDO associated with known sinonasal pathology.
In an effort to optimize success rates, prior studies have investigated risk factors for failure after external and endoscopic DCR. In failure cases after external approach, common identifiable causes were endonasal adhesions between the ostium and middle turbinate or nasal septum, anatomical abnormalities such as a deviated septum or concha bullosa, and chronic rhinosinusitis. 3 For the endoscopic approach, incomplete exposure of the lacrimal sac, inadequate ostium size, and unopened agger nasi cells were reported as reasons for failure.4–6 Existing studies on sNLDO provide limited data on risk factors for DCR failure or variability of outcomes in different subgroups.7–9 This study compares patient characteristics, clinical practice patterns, and surgical outcomes of DCR for pNLDO and sNLDO and identifies variables associated with DCR failure, thus improving surgeons’ ability to anticipate complicating factors and manage patient expectations.
Methods
Data Retrieval
A retrospective review was conducted of all endoscopic and external DCR cases performed at a tertiary academic institution over a 5-year period (2018-2022). Cases were identified by Current Procedural Terminology code with a proprietary electronic medical record search tool (Mayo Data Explorer). All cases with complete medical records and a follow-up of minimum of 3 months were included. Manual chart review was performed, and data pertaining to patient characteristics, surgical technique, and clinical outcomes were extracted and documented using Microsoft Excel. Patients with incomplete medical records or follow-up of less than 3 months were excluded.
Group Assignment
Nasolacrimal duct obstruction cases were classified as primary or secondary based on the presumed etiology per consult notes by the surgeon. Cases were considered secondary when there was a history of sinonasal malignancy, midface radiation exposure, chronic sinonasal inflammatory disease, prior sinus surgery with iatrogenic disruption of nasolacrimal structures, or midface trauma involving the bony surrounds of the nasolacrimal system. Additional recorded variables included the presence of anatomical variants previously implied to affect DCR outcomes (ie, nasal septal deviation to the side of the obstruction), coexisting punctal or canalicular pathology, classification of surgery (primary vs revision), and presence of dacryocystitis at the time of surgery. We also interrogated whether preoperative imaging in the form of CT sinus, maxillofacial, head, or orbit was obtained and/or reviewed to aid in surgical planning.
Surgical Details and Outcomes
Surgeries were either performed by an oculoplastic surgeon alone (classified as “ophthalmology primary surgeon”) or as a combined approach with a rhinologist (classified as “ENT primary surgeon”). The data encompassed contributions from multiple Oculoloplastic and ENT surgeons at our institution. Lacrimal silicone stents were placed in all cases. Obstruction of one or both lacrimal canaliculi, which comprise the proximal lacrimal system, was either diagnosed preoperatively or intraoperatively. In cases where both the upper and lower canaliculi are obstructed on preoperative probing and irrigation, the patency of the more distal nasolacrimal duct cannot be assessed. Those patients were scheduled for canalicular reconstruction, with preparation for a DCR in case a coexisting NLDO was identified during surgery, once canalicular passage was restored. Surgical technique of endoscopic versus external approach was recorded, as well as use of adjunct agents such as Mitomycin C, endonasal debridement during postoperative care, the time of stent removal, and length of follow-up. The primary outcome measure was early functional success of DCR, defined as improvement or resolution of epiphora at 3 months. Not all patients had lacrimal irrigation after surgery, but when data were available, anatomical success was determined based on patency during postoperative irrigation. In cases of failure, the time until symptom recurrence was noted.
Data Analysis
Patient and surgical characteristics were compared between complex and simple NLDO groups using χ2 or t tests for categorical and continuous variables, respectively, in Microsoft Excel version 16.9.
Results
A total of 236 DCR cases met the inclusion criteria. Of those, 79 were identified as secondary NLDO associated with sinonasal pathology (Table 1). When comparing secondary and primary NLDO cases, DCR for sNLDO was more likely to be performed endoscopically (68.4% vs 31.8%, P < .01), be undertaken via a combined approach between ENT and oculoplastic surgery (70.9% vs 8.3%, P < .01), and require bilateral surgery (36.7% vs 5.7%, P < .01). Among sNLDO patients, 29% had coexisting punctal or canalicular obstruction, compared to 8.3% in the pNLDO group (P < .01). There were more revision cases in the sNLDO group (27.8% vs 14.6%, P = .012). Patients with sNLDO had stents in place longer and had longer follow-up.
Surgical Details and Outcomes of Secondary Versus Primary NLDO.
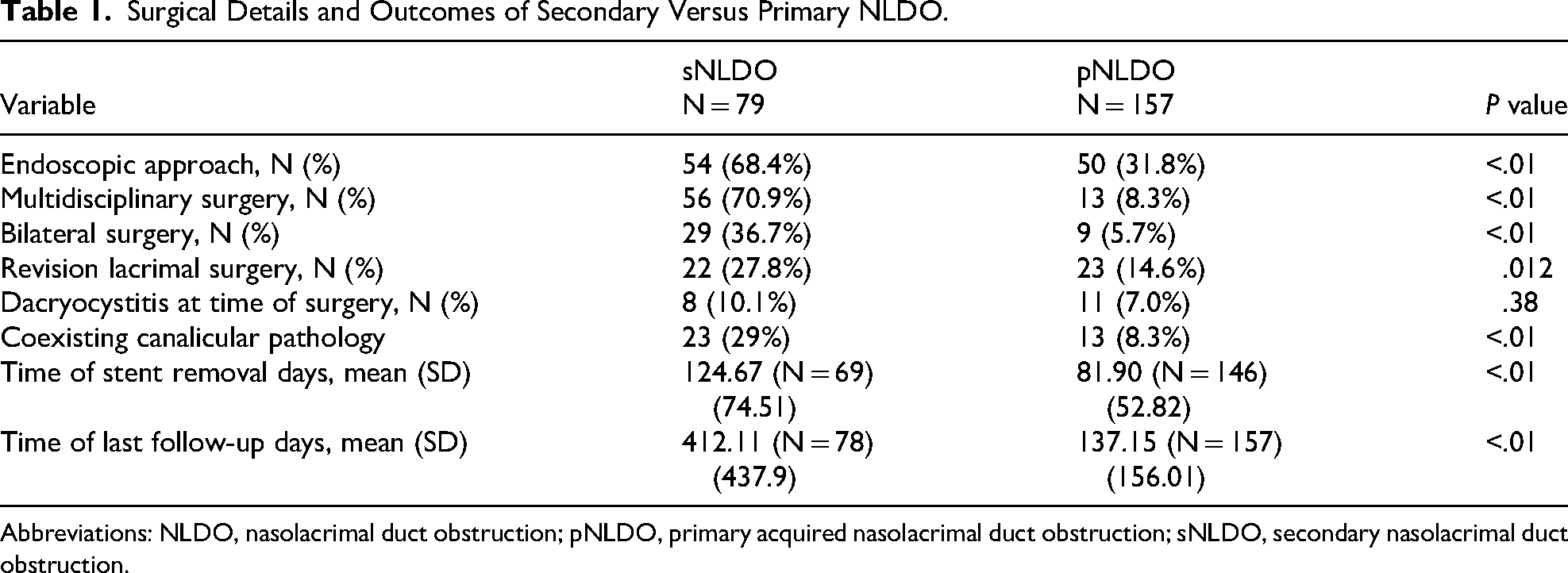
Abbreviations: NLDO, nasolacrimal duct obstruction; pNLDO, primary acquired nasolacrimal duct obstruction; sNLDO, secondary nasolacrimal duct obstruction.
Success rates of DCR for different subsets of sNLDO and pNLDO patients are summarized in Table 2. Following DCR, the overall functional success rate was 79.7% for sNLDO cases compared to 87.9% for pNLDO (P < .01). Analysis of subgroups within the sNLDO cohort showed that functional success was achieved in 83.6% of cases undergoing initial DCR surgery and in 66.7% of those undergoing a revision, compared to 88.2%/85.7% in the pNLDO initial surgery/revision subgroups, respectively. Differences within the initial surgery and revision subgroups were not statistically significant. For sNLDO patients with coexisting punctal or canalicular obstruction, functional success was 69.6%, and 84% when canaliculi were intact (P = .22).
Functional Success Rates of DCR in Different Subgroups.a
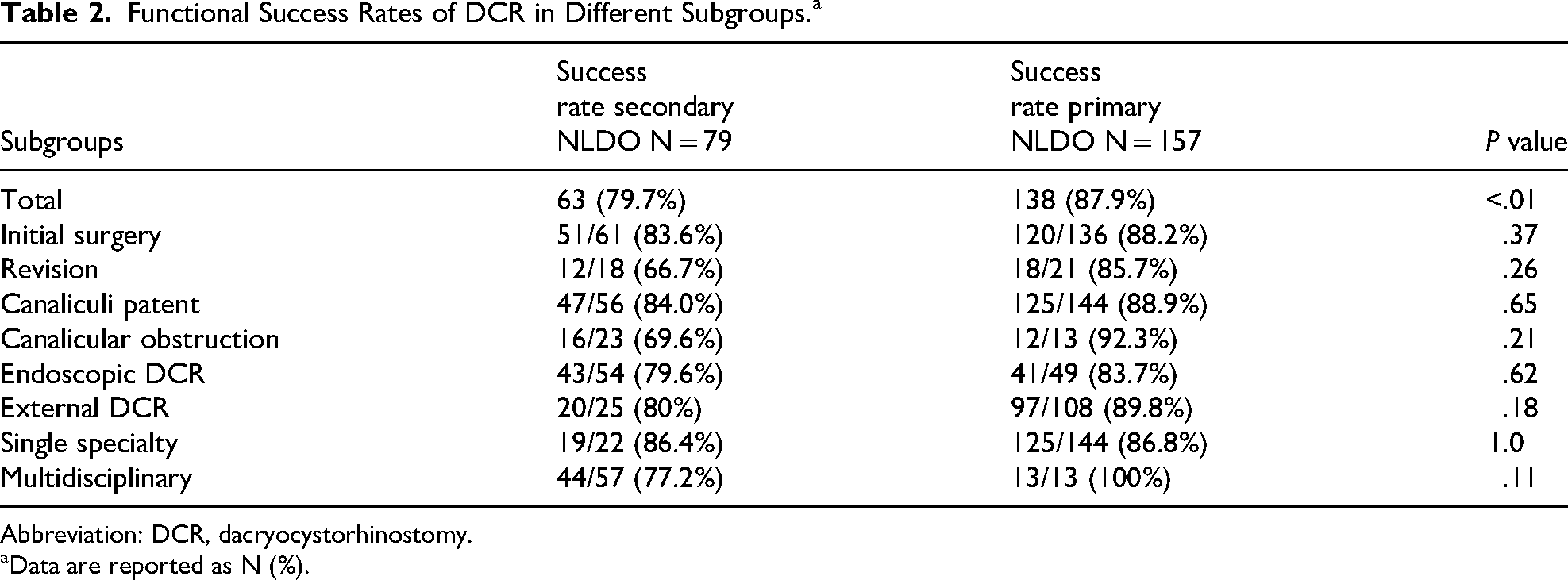
Abbreviation: DCR, dacryocystorhinostomy.
Data are reported as N (%).
Further analysis was performed based on the underlying presumed cause of sNLDO (Table 3). Cases were considered secondary due to history of sinonasal cancer (46.8%), chronic inflammatory disease (24.1%), history of trauma (16.5%), or prior radiation to the relevant anatomical area (31.6%). All cases with radiation exposure also had a history of sinonasal malignancy. Figure 1 demonstrates an example of the anatomical complexity encountered in sNLDO. With a history of radiation and/or sinonasal neoplasm, the success rate of DCR was reduced to 68% and 70.3%, respectively.
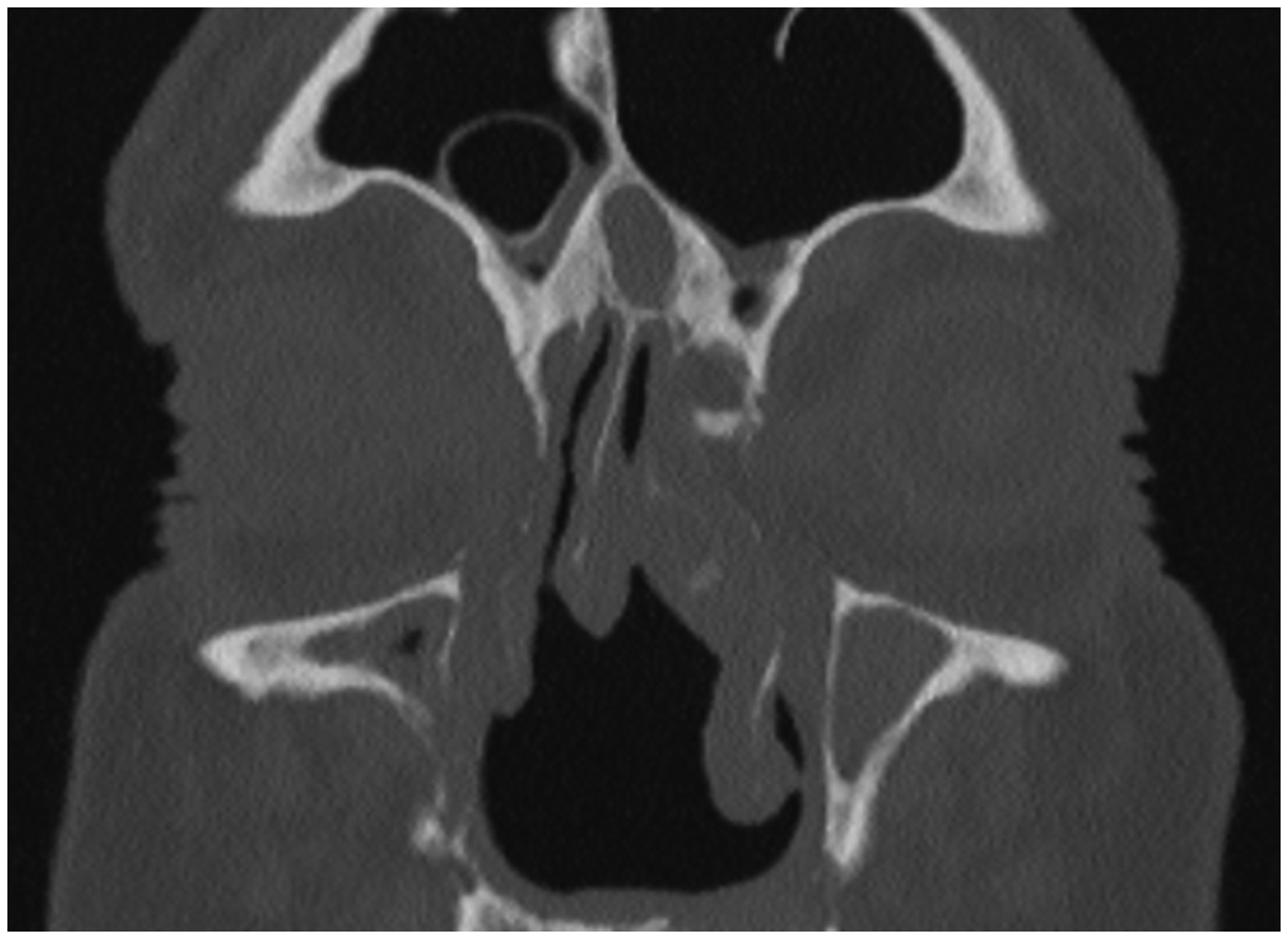
Coronal Computed Tomography (CT) Scan of a Patient with History of Right Maxillary Sinus Squamous Cell Carcinoma Status Post Resection and Adjuvant Radiation Therapy, Radiation-Induced Chronic Rhinosinusitis, and Intranasal Scarring. The Patient was Symptomatic with Right-Sided Epiphora, and Attempted Probing and Irrigation of the Right Lacrimal System in the Office Demonstrated Complete Obstruction with Reflux of Bloody Fluid. Note Loss of Normal Anatomical Landmarks: Partial Septectomy, Right Middle Turbinate Resection, and Evidence of Endoscopic Medial Maxillectomy (Inferior Turbinate Resection with Partially Resected Right Distal Nasolacrimal Duct). The Remaining Superior Septum is Deviated to the Right at the Level of the Lacrimal sac, Limiting Endoscopic Dacryocystorhinostomy (DCR) Access. Broad Adhesions Between the Left Middle Turbinate and Left Nasal Sidewall Resulting in Frontal-Ethmoid Opacification.
Causes of Secondary NLDO and Associated Success Rates.
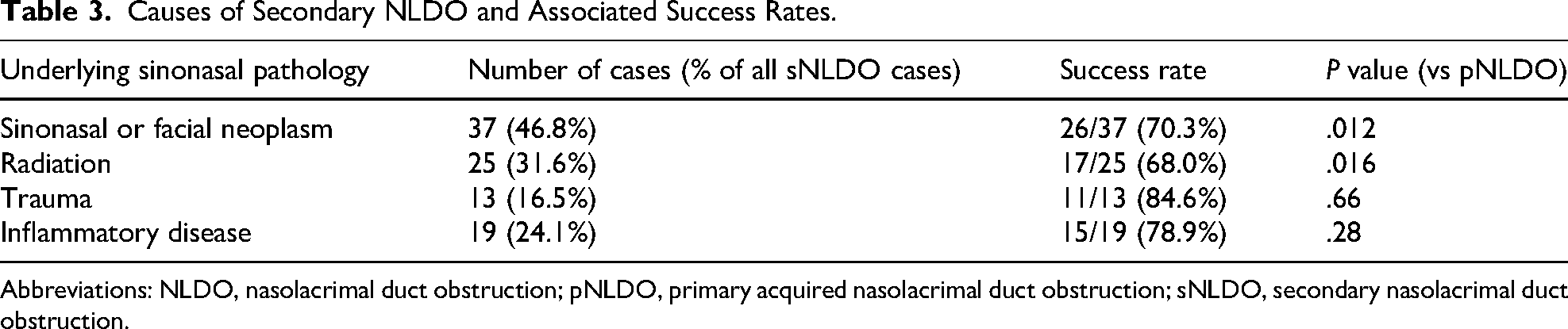
Abbreviations: NLDO, nasolacrimal duct obstruction; pNLDO, primary acquired nasolacrimal duct obstruction; sNLDO, secondary nasolacrimal duct obstruction.
Discussion
The incidence of primary acquired NLDO is estimated at 20.24 per 100,000 individuals, with chronic epiphora and dacryocystitis as the main clinical manifestations. 10 Dacryocystorhinostomy, the definitive surgical intervention for NLDO, has an excellent prognosis with success rates over 90% reported in the literature. 2 However, many studies on DCR outcomes specifically exclude patients with sinonasal comorbidity, such as history of malignancy or radiation therapy, which we will refer to as complex DCR in the discussion, as opposed to simple DCR for pNLDO.
Traditionally, DCR has been performed through an external approach without visualization of endonasal structures. More recently, endoscopic DCR has gained popularity among both oculoplastic surgeons and rhinologists. Multiple studies found that external and endoscopic techniques have comparable outcomes.2,11,12 An endoscopic approach may be favorable in complex DCR for sNLDO associated with sinonasal pathology in order to address endonasal anatomical abnormalities or scar tissue seen after surgery or radiation, and with chronic inflammatory disease.7,8,13 Prior studies that analyzed sNLDO outcomes reported either an external or an endoscopic approach, but no comparison of the two. In our study, an endonasal approach and multidisciplinary collaboration were utilized at a much higher rate in complex DCR cases (Table 1). We did not see a difference in DCR success rates between the endoscopic and external groups (79.6% vs 80%; P = 1.0), or between multidisciplinary and ophthalmology-only DCRs (77.2% vs 86.4%; P = .53) for sNLDO (Table 2). However, when looking at case details, the multidisciplinary group contained more cases at high risk of failure, such as patients with history of radiation or revision surgery. This uneven distribution is likely due to referral patterns at our institution, with rhinologists being mainly involved in lacrimal cases that are perceived to be more challenging from an endonasal standpoint.
Existing literature on DCR outcomes for sNLDO reports overall success rates ranging from 68% to 90%; because of small case numbers, there is often no subgroup comparison.7–9,13,14 Sweeney et al were able to identify a history of radioactive iodine or external beam radiation treatment as risk factors for DCR failure. 7 Similarly, we found a lower overall success rate of DCR for sNLDO at 79.7%, compared to 87.9% for pNLDO. Subgroups with history of sinonasal neoplasm and radiation had lower success rates than those with history of trauma or chronic inflammatory disease (Table 3). This should be recognized when counseling patients on expected outcomes, and adjunct treatments such as Mitomycin C, postoperative endonasal debridement, or anti-inflammatory nasal rinses may be considered. 15
We found that proximal lacrimal system obstruction, including stenosis or complete blockage of the puncta or canaliculi, was more than three times as common in sNLDO compared to pNLDO patients (29% vs 8.3%). The issue of coexisting proximal lacrimal obstruction was not addressed in prior studies on sNLDO. Bothra et al reported on radiation-associated lacrimal obstruction at various levels of the drainage system and found poor outcomes in patients with canalicular involvement. 16 In line with these findings, we saw a trend for increased failure rate among sNLDO patients who also had canalicular pathology, compared to those who did not (69.6% vs 84%, P = .22). The combination of canalicular obstruction and sNLDO with sinonasal pathology needs to be considered in surgical planning and is best managed by a multidisciplinary team of oculoplastic surgeons and rhinologists.
Silicone stents were placed in virtually all cases in our series, and stent removal time was significantly longer for complex cases compared to simple cases. Although silicone stent placement has not been shown to increase DCR success in the cited meta-analyses, the authors feel that this should be included for all cases of sNLDO, due to both the high rate of coexisting canalicular stenosis and propensity for endonasal scarring. 2 Although some literature advocates for the use of mitomycin C intraoperatively to improve function and anatomical outcomes in DCR, high-level evidence to support its use is lacking. 7 Mitomycin C application was infrequent in our patient cohort, with only 7 cases in the sNLDO and 2 cases in the pNLDO cohort, precluding statistical analysis.
This study has several limitations that must be acknowledged. The surgical procedures were performed by multiple ophthalmologists and ENT surgeons, which may have resulted in variability in surgical technique, perioperative care, and postoperative follow-up. There may also be referral bias, with cases that are deemed more complex from an endonasal perspective being routed to rhinologists. While this reflects real-world practice at a tertiary academic center, it may impact the generalizability of results. Additionally, anatomical success was not consistently documented across all cases, limiting our ability to compare functional and anatomical outcomes systematically. Finally, although a minimum follow-up of 3 months was required, longer-term outcomes beyond that point were not uniformly available and may have affected the reported success rates.
Conclusions
In this large series of 79 sNLDO cases associated with sinonasal pathology, endoscopic technique and a multidisciplinary approach were commonly utilized. The more challenging anatomical and tissue conditions are reflected in a lower success rate of DCR for sNLDO. History of sinonasal neoplasm and radiation was associated with higher failure rates, and coexisting canalicular obstruction was frequently encountered. The findings from this study can support surgeons in planning complex DCR cases, setting expectations for sNLDO patients, and informing future research studies to optimize outcomes.
Footnotes
Authors’ Contributions
The initial study conception and design were completed by Lilly Wagner, with contribution by Janalee Stokken, Andrea Tooley, and Elizabeth Bradley. Material preparation, data collection, and analysis were performed by Lily Farrell, Piotr Kopinski, Mohamad Rani, Hassoun and Jeffrey Graves. The first draft of the manuscript was written by Lily Farrell, edited by Lilly Wagner, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This study was deemed exempt by the Mayo Clinic Institutional Review Board and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki. Written consent for data contained in the medical chart to be used for retrospective research is on file from all included patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.