
Abstract
Background
Priming is a psychological phenomenon where subconscious cues in the environment impact our behavioral responses in certain situations. Well studied in the worlds of business, marketing, and even politics, it is unclear how the priming phenomenon impacts patient perception of their own disease state nor how they report that perception using tools like the Sinonasal Outcomes Test (SNOT-22), used to measure that perception in chronic rhinosinusitis.
Objective
To determine the impact of positive or negative priming on self-reported patient perception of their chronic rhinosinusitis disease using the SNOT-22 disease-specific quality of life instrument.
Methods
Single-blind, randomized, prospective cohort pilot study of 206 consecutive adult patients with a clinical diagnosis of chronic rhinosinusitis presenting to a university rhinology clinic. Patients were randomized to receive “positive priming” (103) or “negative priming” (103) by reading a passage about the positive or negative aspects of chronic sinusitis and its treatment respectively. Patients were then asked to fill out the SNOT-22 and results between the two groups were compared.
Results
The negative priming group had a higher median SNOT-22 score of 49 [IQR = 39] compared to the positive priming groups’ score of 22 [IQR = 27], p < 0.0001), a difference of nearly three times the minimal clinical impactful difference (MCID). This effect was consistent regardless of age or sex of the patient. Subgroup analysis revealed a greater impact when priming was performed by the senior male attending regardless of patient age or sex (p < 0.001), while priming performed by the younger female research fellow had greater impact on older patients (>59 years, p = 0.001) and female patients (p = 0.003).
Conclusions
Priming impacts how patient's perceive their chronic rhinosinusitis as determined by the SNOT-22. It is imperative that the rhinologist understand this when using this instrument in research applications and in clinical decision-making for patients.
Keywords
Introduction
Priming is a psychological phenomenon where exposure to certain concepts or stimuli can influence subsequent judgments or responses.1,2 These phenomena can activate our brain's memory, thereby influencing our subsequent thoughts, feelings, and actions in a subconscious manner. These changes in our perceptions are the result of a three-step process. 3 First involves exposure to a prime stimulus including images, words, or features of the environment. Second, the prime stimulus increases a concept's accessibility in the brain, which increases the likelihood of that concept influencing the encoding of new information. 4 Finally, the newly encoded representations result in perceptual or behavioral changes.
The impact of priming appears to be constant and extensive and is well-known in other disciplines including the world of marketing. The smell of baking bread or cinnamon rolls as a priming stimulus is thought to cause more purchases among customers at bakeries. But priming can have a more profound effect than influencing purchases, such as impacting the interpretation of our senses. An experiment with 40 participants was conducted to explore how wine-tasting preferences could be primed by different genres of musical stimuli. Electroencephalographic measurements were performed to measure participant brainwave activity in two experiments. Significant associations were found between the musical stimulus genre and changes in participant wine selection and their descriptions of the wines. The musical stimuli were administered between two rounds of tasting, resulting in significantly different brainwave activities as participants tasted the same wines. 5
Priming has also been shown to impact behaviors and physical activities. Bargh et al (1996) 2 demonstrated this in an experiment where participants were asked to unscramble sentences that contained words related to either rudeness or politeness. Once participants completed the task, they were told to locate the experimenter to begin the next part of the experiment. However, each time the experimenter would be in a conversation with a confederate. Those who had unscrambled sentences with words related to rudeness interrupted the experimenter much more quickly and frequently than participants exposed to sentences with words related to politeness. 2
While priming has been extensively studied in psychology and sociology,6,7 its impact on subjective health-related quality of life forms in general and rhinology-related questionnaires specifically remains minimally explored. However, it is clear that priming can impact our perceptions of an event or a life experience and how we report it to others on questionnaires. One demonstration of this was seen in an experiment conducted with a group of new M.B.A. students. Some were exposed to a brief, informal talk about the significant stresses and strains typically experienced in their course of study. A control group received no such information and both groups were then asked to complete a questionnaire assessing the degree to which they were experiencing these stresses and strains. Those primed with information about the severity of stressors reported experiencing higher levels of several of these stressors and strains than those who received no information. 8
In this context, we sought to explore the impact of priming on the Sinonasal Outcome Test-22 (SNOT-22). The SNOT-22 is a widely used questionnaire used by rhinologists and designed to assess sinonasal quality of life (QoL) in patients with chronic rhinosinusitis (CRS). 9 While this questionnaire provides valuable insights into the impact of sinonasal conditions on patients’ daily lives, as a subjective questionnaire, we hypothesized that it may be particularly susceptible to priming. Since it is used to assist the rhinologist in making treatment decisions, it is crucial to consider potential factors that may influence responses, such as priming. Understanding and evaluating the potential impact of priming on SNOT-22 scores is crucial for accurate interpretation and assessment of patients’ quality of life. This is the first study to assess the effects of priming on SNOT-22 scores.
Methods
Study Population
This pilot study was an IRB-approved, single-site, prospective, single-blinded, randomized controlled trial including patients with CRS presenting at a rhinology clinic. As we sought to evaluate the susceptibility of the SNOT-22 to priming, we included all adult patients with all phenotypes of CRS, including those who had been operated on and those who had not, as well as new patients and returns. As a preliminary pilot study, we did not seek to determine if patients with certain diagnoses were more susceptible to priming, but our primary objective was to assess whether the SNOT-22 was susceptible at all using a large group of “all comers” and to determine if an effect was seen if an effect size could be discerned. We thereby hope to use this knowledge in subsequent studies of different phenotypes of CRS.
Patients were randomized into negative or positive priming groups using a sealed envelope technique, where researchers were given randomly generated treatment allocations within sealed opaque envelopes. Researchers employed masked priming, 7 which involves the presentation of a brief stimulus that is not consciously perceived. Researchers delivered the SNOT-22 questionnaire using a standardized script based on the assigned priming group. Two researchers were involved in recruitment for this study: Researcher 1 was the senior attending who was the primary physician with whom the patients were most familiar; Researcher 2 was a research fellow who was meeting the patients for the first time.
Patients who received positive priming were given the following script to read prior to filling out the SNOT-22:
Important Things to Know About Chronic Sinusitis and Nasal Polyps:
Treatment methods for chronic sinusitis and nasal polyps have improved dramatically over the last 20 years with decreased risk of side effects, and rapid recoveries, getting you back to your life sooner! Optimal treatments can result in significant improvements in symptoms of chronic sinusitis and nasal polyps including nasal congestion, sinus drainage, and headaches. Optimal treatments can improve the quality of your sleep helping you to get you back to normal activities quickly New office-based procedures for many with chronic sinusitis can get you back to your life the next day! New medications taken on an intermittent basis can cause polyps to disappear with little side effect and without steroids! Important Things to Know About Chronic Sinusitis and Nasal Polyps:
Untreated chronic sinusitis and nasal polyps can cause significant side effects in some people including rarely spread of infection into the eyes and the brain Individuals with chronic sinusitis and nasal polyps suffer from worse vitality and social functioning than those with other diseases including congestive heart failure and COPD People with chronic sinusitis can suffer with more bodily pain than those with chronic lower back pain Chronic sinusitis and nasal polyps are a chronic disease analogous to asthma or rheumatoid arthritis, frequently requiring treatment throughout a person's life to keep it under control Untreated forms of nasal polyps can cause deformity of the face and eyes in some rare cases
Patients who received negative priming were given the following script to read prior to filling out the SNOT-22:
Sino-Nasal Outcome Test-22
The SNOT-22 is a 22-item questionnaire that measures the impact of chronic rhinosinusitis (CRS) on quality of life. Patients rate the severity of CRS symptoms on a 0-5 scale. The total score ranges from 0-110, with higher scores indicating a more significant symptom burden and reduced quality of life. 9
Statistical Analysis
Data normality was assessed using the Shapiro-Wilk test. Values were reported as median and Interquartile Range (IQR) (continuous) and absolute counts (n) and relative frequencies (%) (categorical). Fischer's exact test was utilized for categorical variables. Comparisons of SNOT-22 scores were made using the Wilcoxon test. Subgroup analysis by sex, age, and researcher was performed. All statistical tests were two-sided with a significance level (α) of 0.05. Data analysis was performed using RStudio Version 2023.06.0 + 421 (RStudio Inc., Boston, MA).
Results
A total of 206 participants were randomized into positive (n = 103) and negative (n = 103) priming groups. Patient characteristics, including age and sex, did not differ between the priming groups (Table 1). The negative priming group had a higher median SNOT-22 score of 49 [IQR = 39] compared to the positive priming groups’ score of 22 [IQR = 27], p < 0.0001) (Figure 1). Multiple linear regression models revealed that male sex was negatively associated with SNOT-22 scores (B = -9.74, p = 0.007).
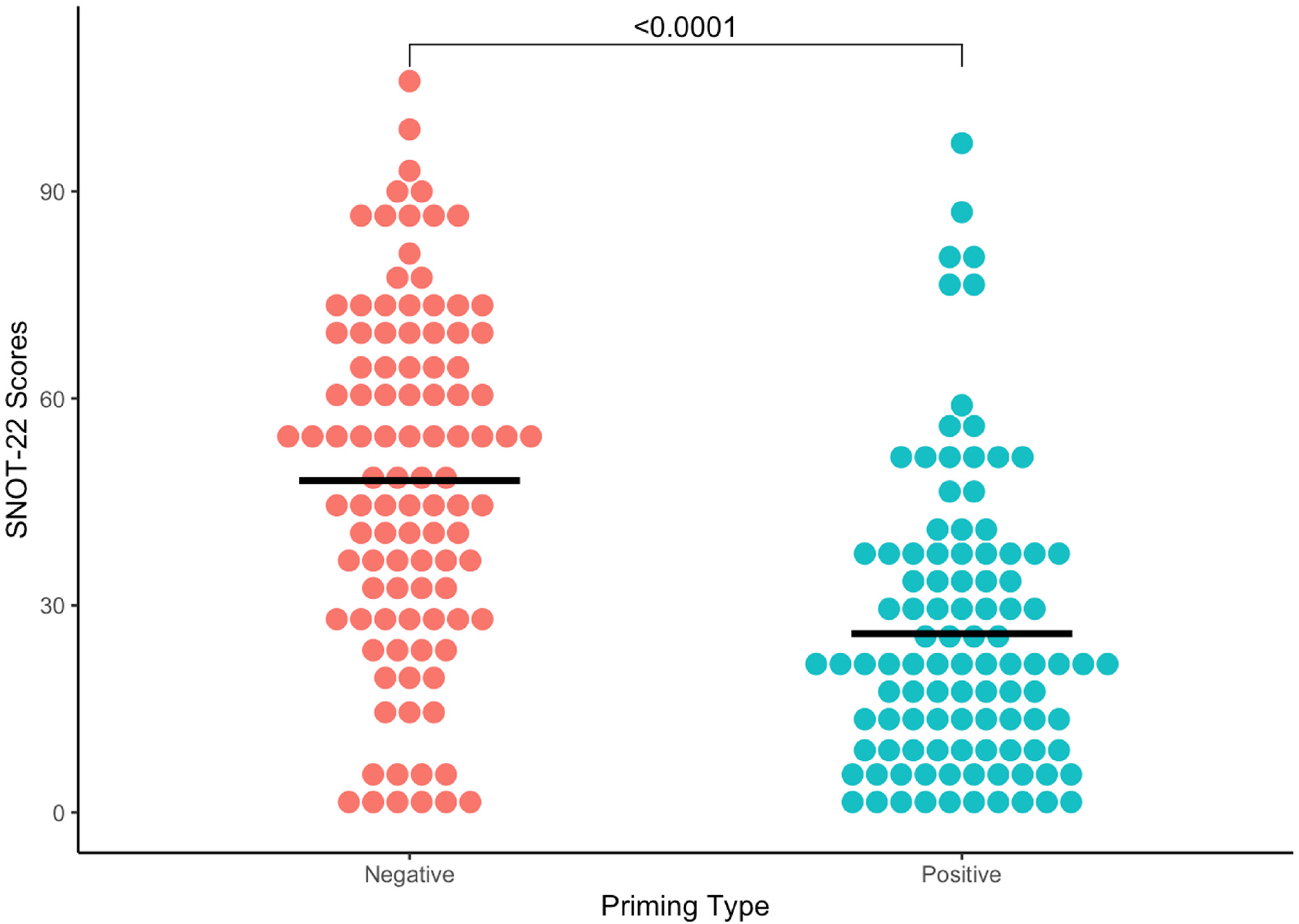
SNOT-22 scores, plotted by negative versus positive priming. Median scores, denoted by the black crossbar, were 22 (IQR = 27) for positive priming and 49 (IQR = 39) for negative priming. Median SNOT-22 scores were higher in the negative priming group, with a p-value of <0.0001.
Overall SNOT-22 Scores and Patient Characteristics.
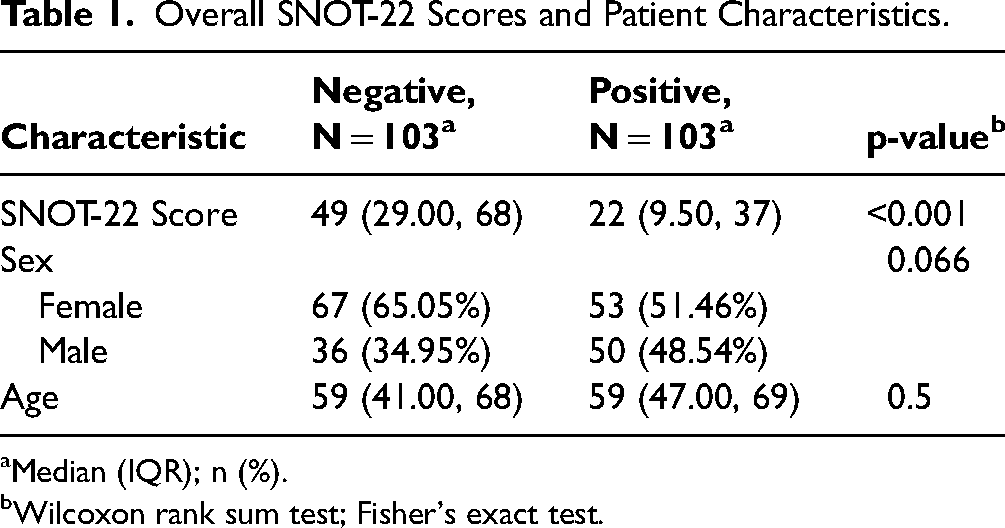
Median (IQR); n (%).
Wilcoxon rank sum test; Fisher's exact test.
Subgroup analyses based on age and sex were consistent with overall results, with negative priming having higher SNOT-22 scores (Composite, Table 2). Subgroups were further stratified by which researcher recruited each subject. Recruitment by researcher 1 versus researcher 2 showed a trend but did not yield significant differing overall SNOT-22 scores (37 [IQR = 37.25] vs 28 [IQR = 35.75], p = 0.14); however, subgroup analysis elucidated subtle SNOT-22 differences between the two researchers (Table 1B). Recruitment by researcher 1 (male senior attending) yielded statistically significant (p < 0.001) higher scores in all negatively primed subgroups of age and sex. On the other hand, recruitment by Researcher 2 (female research fellow) resulted in statistically significant differences only in the female subgroup (p = 0.003) and those over 59 years of age (p = 0.001). Patient characteristics were not statistically different when comparing groups recruited by researcher 1 versus researcher 2 (Table 3).
Subgroup Analysis Based on age (>59 or <59) and sex.
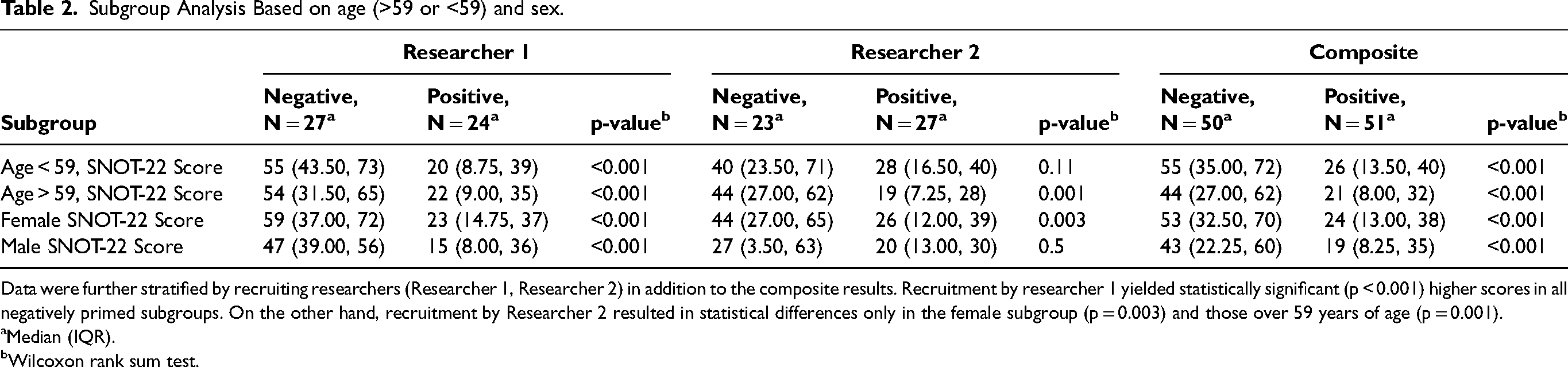
Data were further stratified by recruiting researchers (Researcher 1, Researcher 2) in addition to the composite results. Recruitment by researcher 1 yielded statistically significant (p < 0.001) higher scores in all negatively primed subgroups. On the other hand, recruitment by Researcher 2 resulted in statistical differences only in the female subgroup (p = 0.003) and those over 59 years of age (p = 0.001).
Median (IQR).
Wilcoxon rank sum test.
Neither SNOT-22 Scores Nor Patient Characteristics (Sex/Age) Differed When Stratified by Researcher.
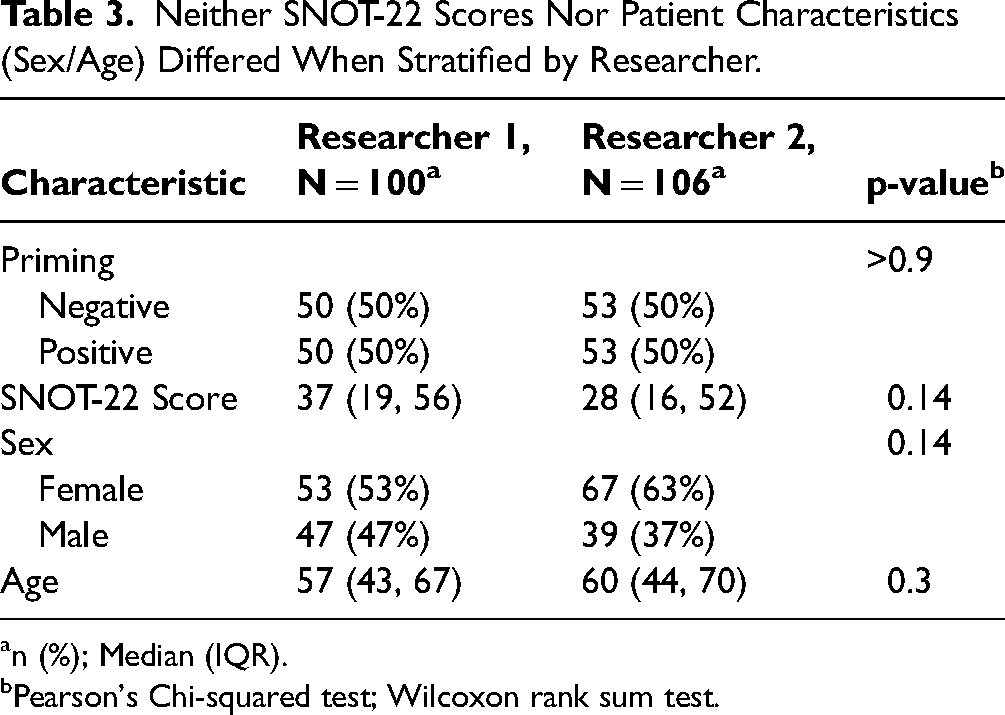
n (%); Median (IQR).
Pearson's Chi-squared test; Wilcoxon rank sum test.
Discussion
The SNOT-22 is a valuable tool providing insights into the impact of CRS on patients’ quality of life. However various factors can influence SNOT-22 scores, including psychological aspects such as priming. Understanding the interplay between priming and SNOT-22 scores is vital for accurately interpreting and utilizing these scores.
Our data demonstrate that negative priming of patients with CRS resulted in significantly higher SNOT-22 scores compared to those who received positive priming, a finding similar to that reported by Yang et al.10 In both male and female subgroups, negative priming led to significantly higher SNOT-22 scores than positive priming. These results suggest that the psychological effects of priming are consistent across different demographics, including sex and age, reinforcing the generalizability of the findings. Further subgroup analyses revealed that researchers involved in participant recruitment can influence subjective data with a significant impact seen in all patients primed by the male senior attending while only in older patients and female patients by patients primed by the female research fellow.
Since SNOT-22 is considered validated and reliable tool, it can be surprising that a simple paragraph providing brief clinical information about rhinological diseases could have such a significant impact on participants’ responses. We interpret this result as a crucial finding, suggesting that SNOT-22, like other clinical assessment tools, requires specific parameters for accurate application, similar to how other clinical tests are conducted. For instance, blood pressure is typically measured from the upper arm of a resting patient, serum cortisol levels are measured in the morning, and lipid panels are conducted on an empty stomach. Similarly, we believe that PROMs need a standardized clinical context to resist external influences and factors such as manipulation/priming, ensuring consistent, reliable, and robust results, We suggest that the completion of the SNOT-22 form at home prior to the visit could help mitigate factors of both feasible positive and negative manipulation in the clinical setting.
Further, our study emphasizes the need for careful standardization of recruitment to minimize potential bias and ensure the reliability and validity of study outcomes in which SNOT-22 score is an important criterion. Similarly, treatment decisions in which SNOT-22 score is a significant feature must be carefully considered.
Our study is limited by being a single-site study and may be limited based on the geographic location of our patient population. Further, as a pilot study, this study is also limited by a lack of granularity of patient information, such as cultural background, medical and surgical history, severity of CRS, and psychosocial factors. Now that we have confirmed that priming impacts the SNOT-22 scores of patients with CRS, we will use this information to study further susceptibility of specific subgroups of patients, including new patients versus returning patients, operated patients versus non-operated, and different phenotypes of CRS.
Conclusion
Priming is a powerful force impacting how patients report their CRS QOL on disease specific instruments like the SNOT-22. Our findings emphasize the importance for rhinologists to consider the influence of the clinic environment, patient interactions, and how medical information is conveyed on the assessment of sinonasal symptoms. By recognizing the impact of priming on patients’ SNOT-22 scores, rhinologists can better understand the complex interplay between psychological factors and sinonasal symptoms. This knowledge can inform clinical decision-making and enhance the holistic approach to patient care, reinforcing the need for a multidimensional approach when evaluating patients with sinus disease.
Ethical approval for this study was obtained from Institutional Review Board of the University of North Carolina School of Medicine: 22-2772.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by NIH grant KL2TR002490 to AJK. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. No authors have any financial conflicts of interest.
Presentation
Presented at the Meeting of the European Rhinologic Society, Sofia, Bulgaria, June 19, 2023.