
Abstract
Study Design
Retrospective Observational Study.
Objective
Mandibular condyle fractures are distinctive among maxillofacial injuries in which they disrupt mandibular function in a way that other traumatic injuries do not. Condylar fractures can be treated using either the conservative (closed reduction and immobilisation) or surgical (open reduction and internal fixation) approaches. Both of these modalities of treatment have advantages and disadvantages, as well as indications and contraindications. The purpose of this study is to compile and compare our experience in the management of condylar fractures through open and closed reduction.
Methods
The present retrospective analysis included a total 100 patients of condylar fractures in patients > 18 years of age who were randomly divided into nonsurgical and surgical group based on Edward Ellies criteria. In the present study, the outcomes of conservative vs surgical management of condylar fractures were discussed in terms of seven parameters, including the maximal inter-incisal mouth opening, protrusive and lateral excursive movements of the mandible, status of occlusion, deviation of mandible during mouth opening, temporo-mandibular disorders and facial nerve paralysis which were measured and evaluated pre- and post-operatively at different intervals of time. Follow-up period was for 6 months.
Results
It was noted that the main cause of condylar fracture was trauma with a male predilection with an average age of 32.6 ± 1.2 years. Subcondylar fracture was the commonest type of condylar fracture that we encountered. 33.3% of the patients had restricted mouth opening and 57% of the patients had deranged occlusion. 37% of the patients were treated surgically and 48.6% of these fractures were approached using peri-angular approach. More patients had an increased mouth opening and a stable occlusion at the 6 months follow-up when compared to that of the 2 month follow up.
Conclusions
From the above study we can conclude that the treatment plan should be patient specific and follow the algorithm for a particular type of fracture. We endorse the same based on our experience in treating condylar fractures over the last 5 years. The art of decision making solely depends on the surgeon’s expertise in managing condylar fractures.
Introduction
Condylar fractures are extremely common in oral and maxillofacial traumatology and account for 19–52% of mandibular fractures due to trauma. 1 Among paediatric facial fractures, mandibular fracture accounts for 20 to 50% and condyle is the most commonly injured area within the paediatric mandible and is considered a primary growth centre in children. 2
The pattern of injury in paediatric condyle differs from the adult condyle due to the relative development of mandible when compared to cranium and midface, as the neurocranium develops around 5 years of age to reach 85% of the adult size, followed by the development of maxilla and midface skeleton around 7–9 years, while mandibular growth attaining the adult size usually happens between 14–16 in girls and 18–20 in boys. 3 The morphology of paediatric condyle lacks the development in condylar base/subcondylar region often appearing as a weak stout/stump bearing the oval/bulbous condylar head which is in contrast with an adult condyle with a well demarcated condylar neck and base. 3
Static and dynamic transmission of forces in paediatric condyle often results in condylar head fracture with or without comminution and displacement. According to A.Ghasemzadeh in et al, in his 20 years study in managing the paediatric condylar fracture, the most commonly observed fracture pattern in paediatric population is dicapitular fracture. 2 Mode of injury to paediatric condyle can only be hypothesized to static and dynamic transmission of force to condylar head leading to comminution, displacement or dislocation determined by morphology and velocity of injury. 4
Moore determined the orientation of grain pattern causing fracture line propagation in ascending ramus region. In adult mandibular condyle, the mode of injury is kinetic energy generated by a subject falling on a static object and a moving object against a static subject or its combination. 5
Paediatric condylar fractures are rarely displaced and almost treated by observational or functional therapy due to their elastic bony composition, high vascularity and high remodelling capacity. 6 On the other hand, geriatric patients have brittle bony structure with high incidence of atrophy and reduced vascularity making healing and condylar adaptation quite difficult often healing happens by pseudoarthrosis. 7
The outline of the treatment protocol may include one or all of three things.
8
1) A fixed period of inter-maxillary fixation followed by functional therapy. 2) Observation/Functional therapy without inter-maxillary fixation and 3) Open reduction with internal fixation.
Multiple factors are taken into consideration when deciding a treatment plan like malocclusion, degree of displacement, angulation of condylar fracture segment, shortening of vertical ramus height, role of masticatory muscle pull and influence of fracture on TM joint function. 9 Up until the 1960’s, authors like Edward Ellis preferred closed reduction due to the surgical complications listed above but an article given by Zide and Kent in 1983 clearly listed the indications for open reduction and internal fixation and closed reduction, it was further modified in 1990 opening a gateway into the ease and superiority of ORIF. 10 More recently the guidelines from ASIF/AO, AACOMS and AAOMS all emphasize on ORIF after clinical & radiographic evaluations. 11
The purpose of this study is to compile and compare our experience in the management of condylar fractures over the last 5 years in addressing condylar fracture through open and closed reduction. To the best of the author’s knowledge, there aren’t many studies in the literature to address all the parameters and controversies surrounding condylar fractures.
Materials and Methodology
A retrospective analysis of 100 cases of condylar fracture treated in the Department of Oral and Maxillofacial Surgery from January 1, 2016 to December 31, 2021 was done. Prior to the start of the study, an ethical clearance was obtained from the Institutional Review Board strictly adhering to Helsinki declaration. All participants gave their written consent for their participation in the current study and the usage of any of their photograph(s) that was taken during the study that was related to the study procedure, for all possible publication related to the study. The inclusion criteria for the study include patients who had a condylar fracture and who come under ASA guidelines I, II and III. The exclusion criteria for the study were patient not willing to participate. The demographic, clinical and radiographic data were collected for each patient. The criteria for deciding open vs closed reduction was based on chair side drop back test suggested by Edward Ellis III, premature occlusal contacts due to shortening posterior ramus height and radiographic angulations of the condyle. Patients falling under this criteria were treated surgically whereas patients with stable to minimally deranged occlusion, without shortening of posterior ramus height and radio-graphically minimal displacement were treated either with closed reduction with functional guiding elastics, inter-maxillary fixation and observation. All the relevant data such as including the maximal inter-incisal mouth opening, protrusive and lateral excursive movements of the mandible, status of occlusion, deviation of mandible during mouth opening, temporo-mandibular disorders, facial nerve paralysis and pain which were analysed from records and evaluated pre- and post-operatively. All the collected data were then complied and assessed.
Results
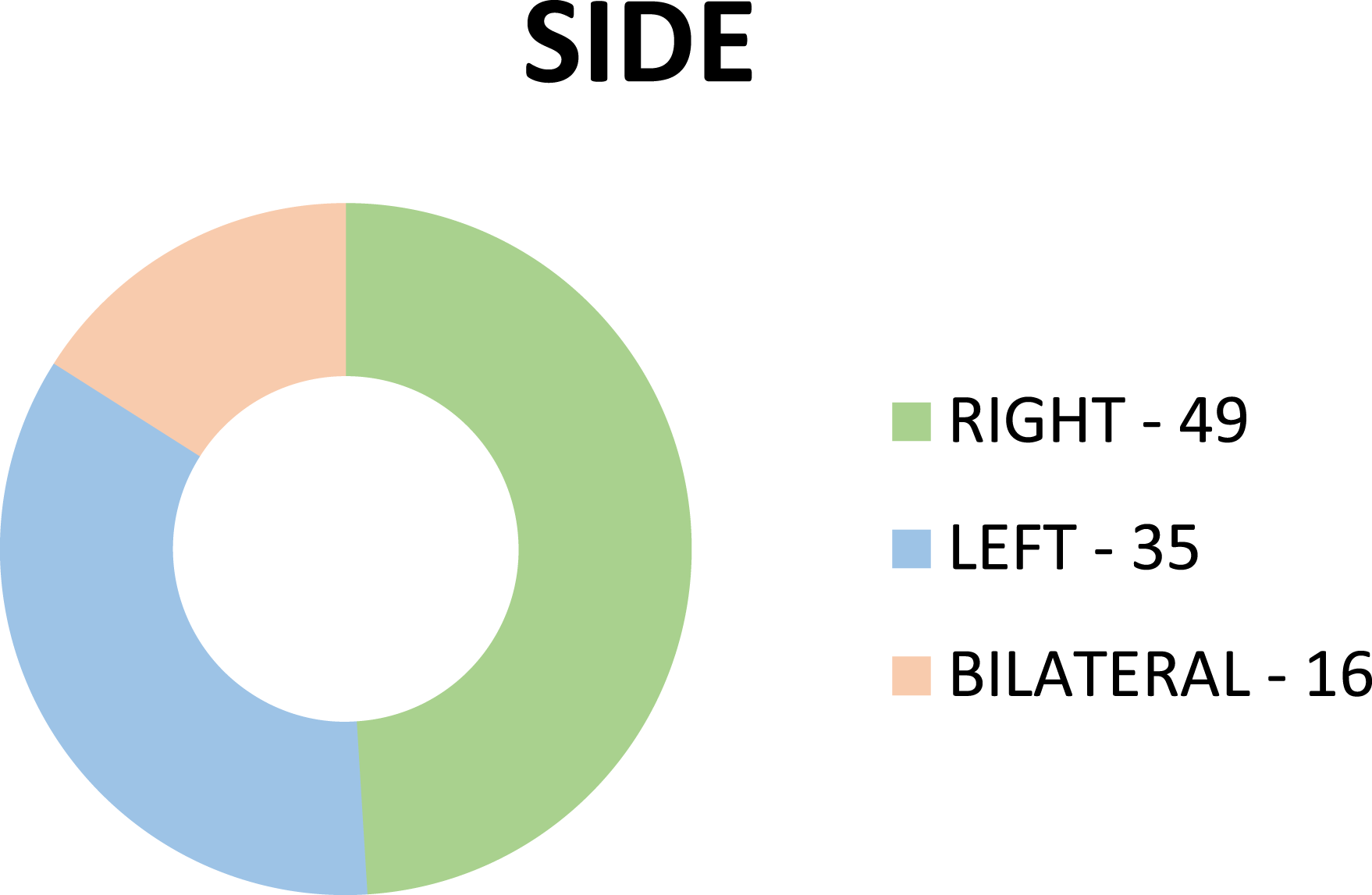
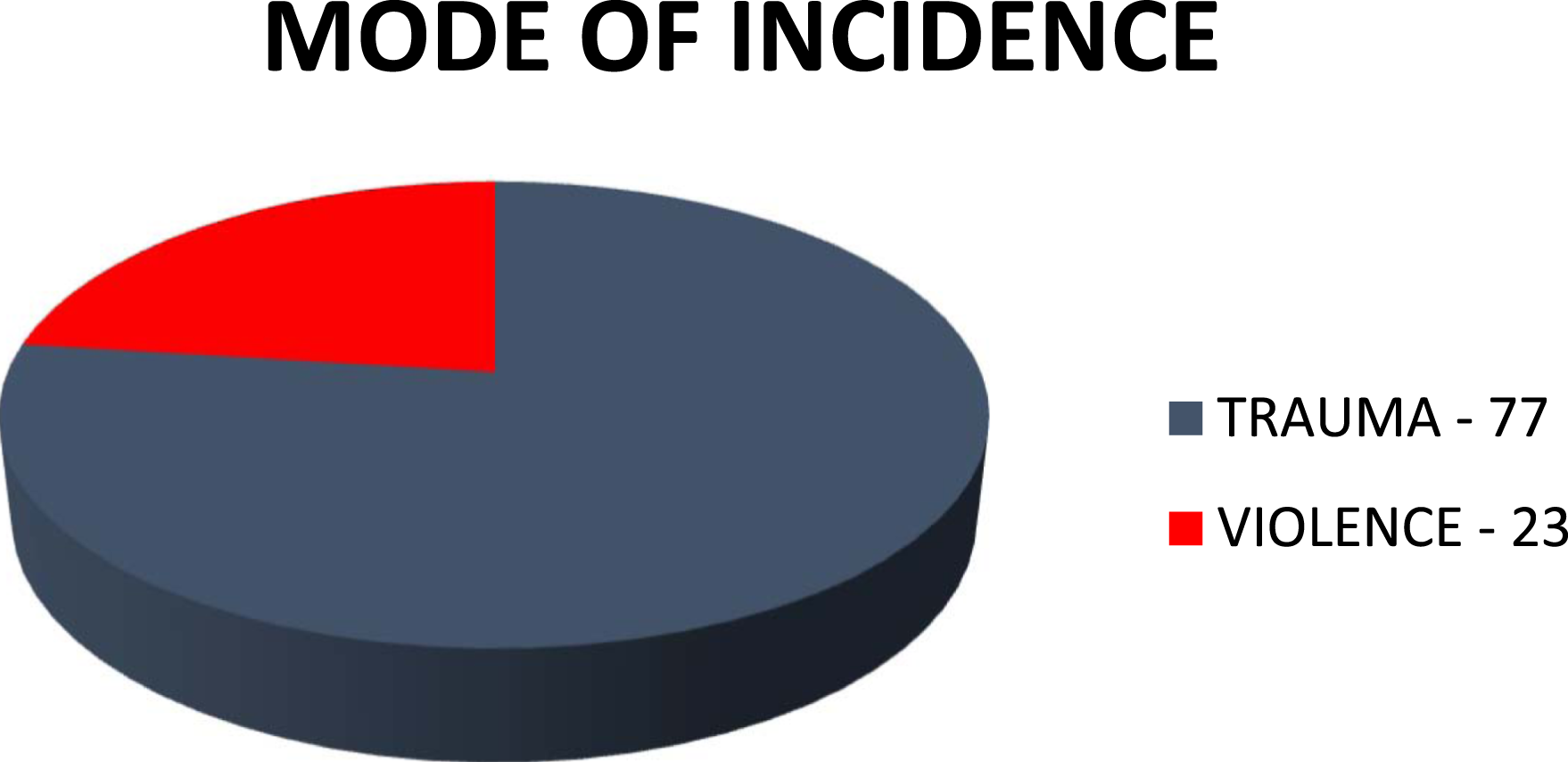
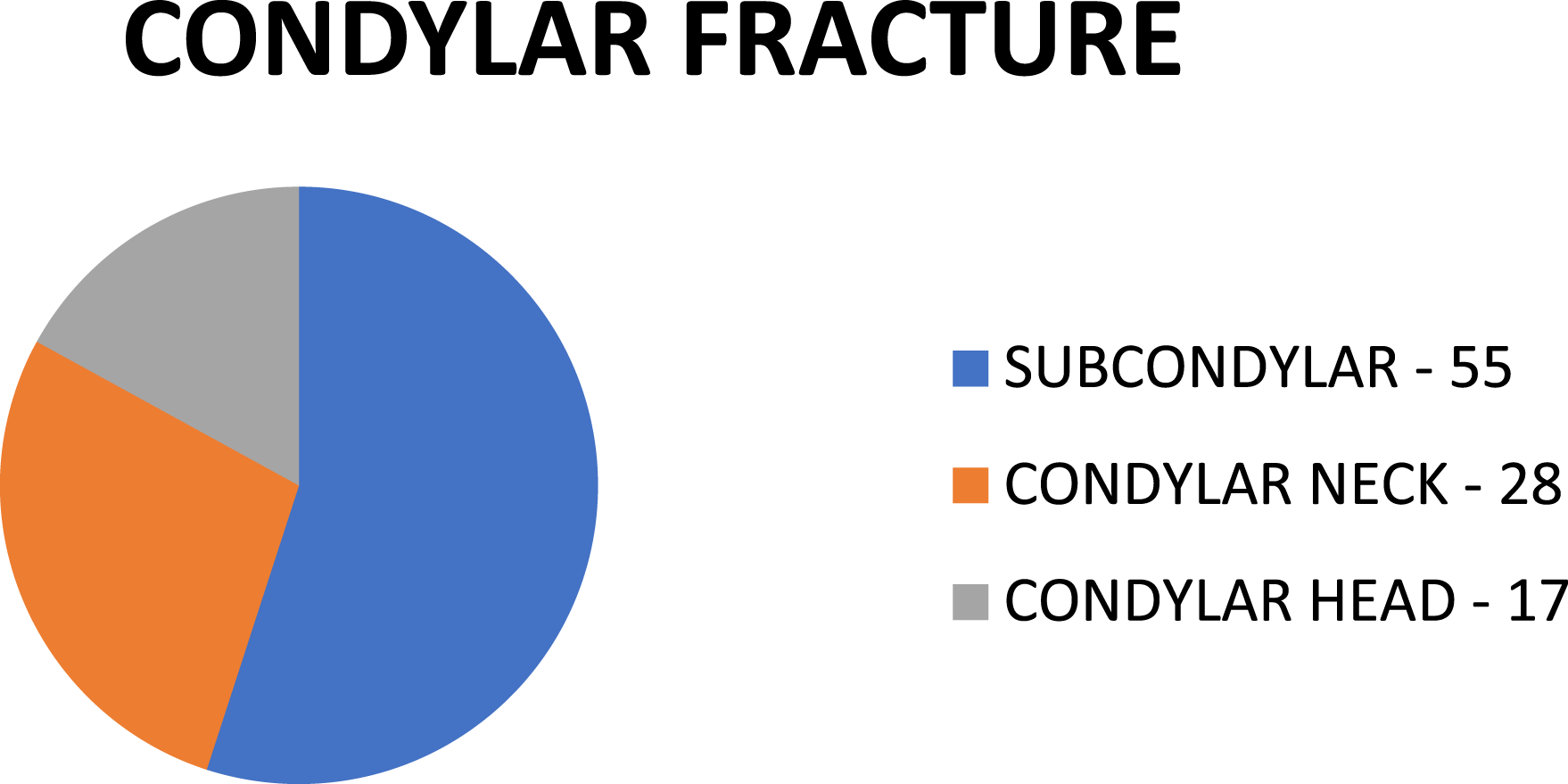
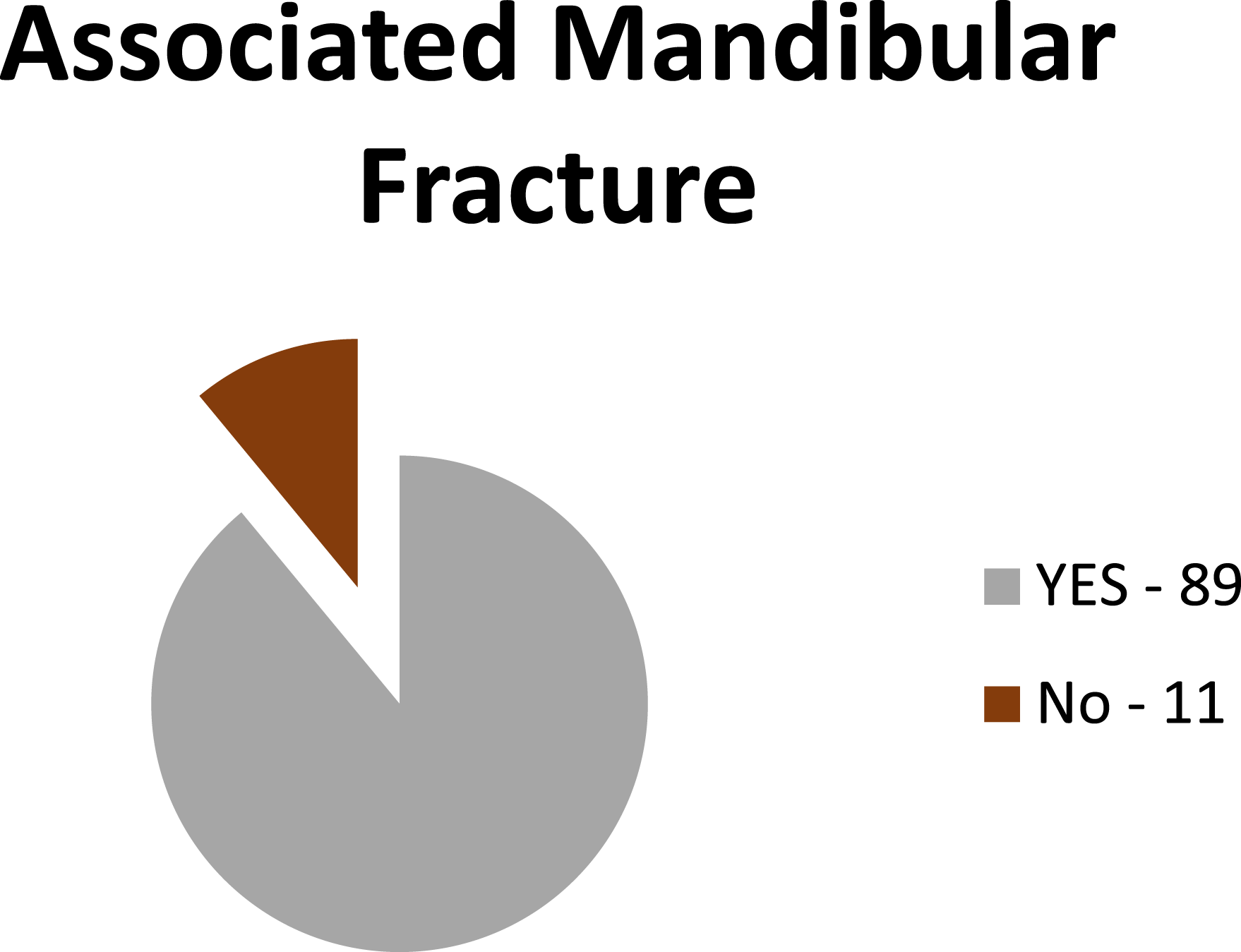
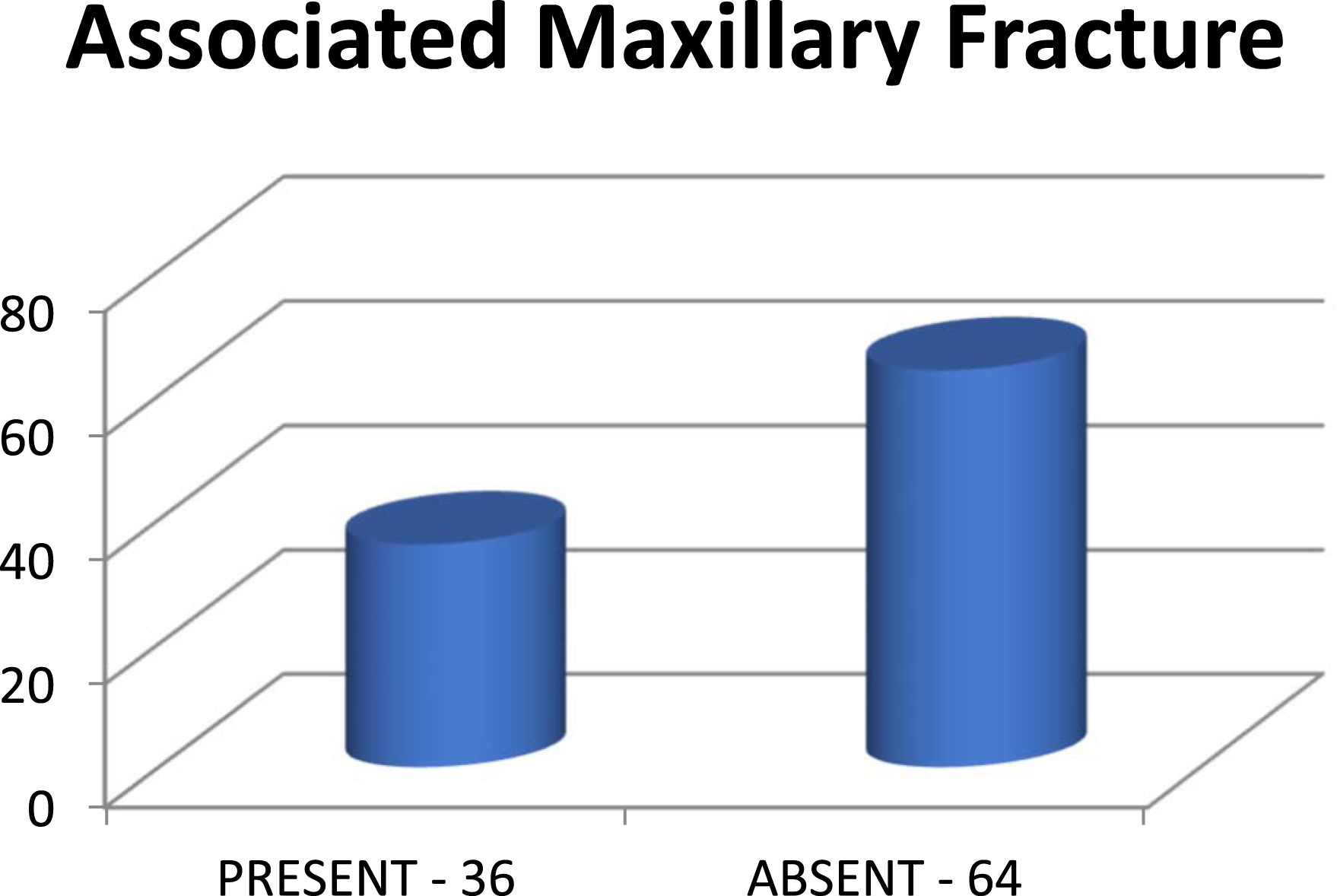
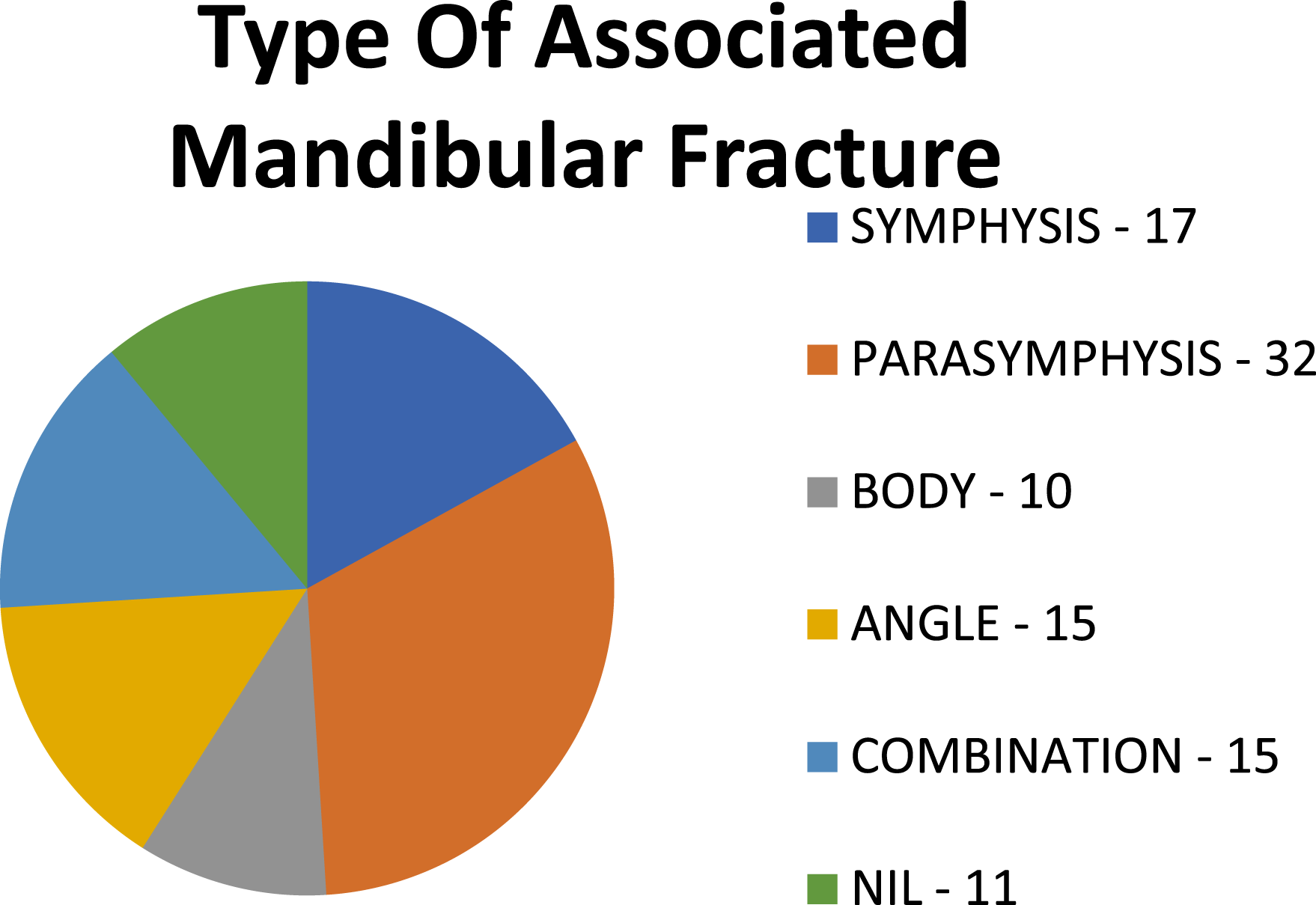
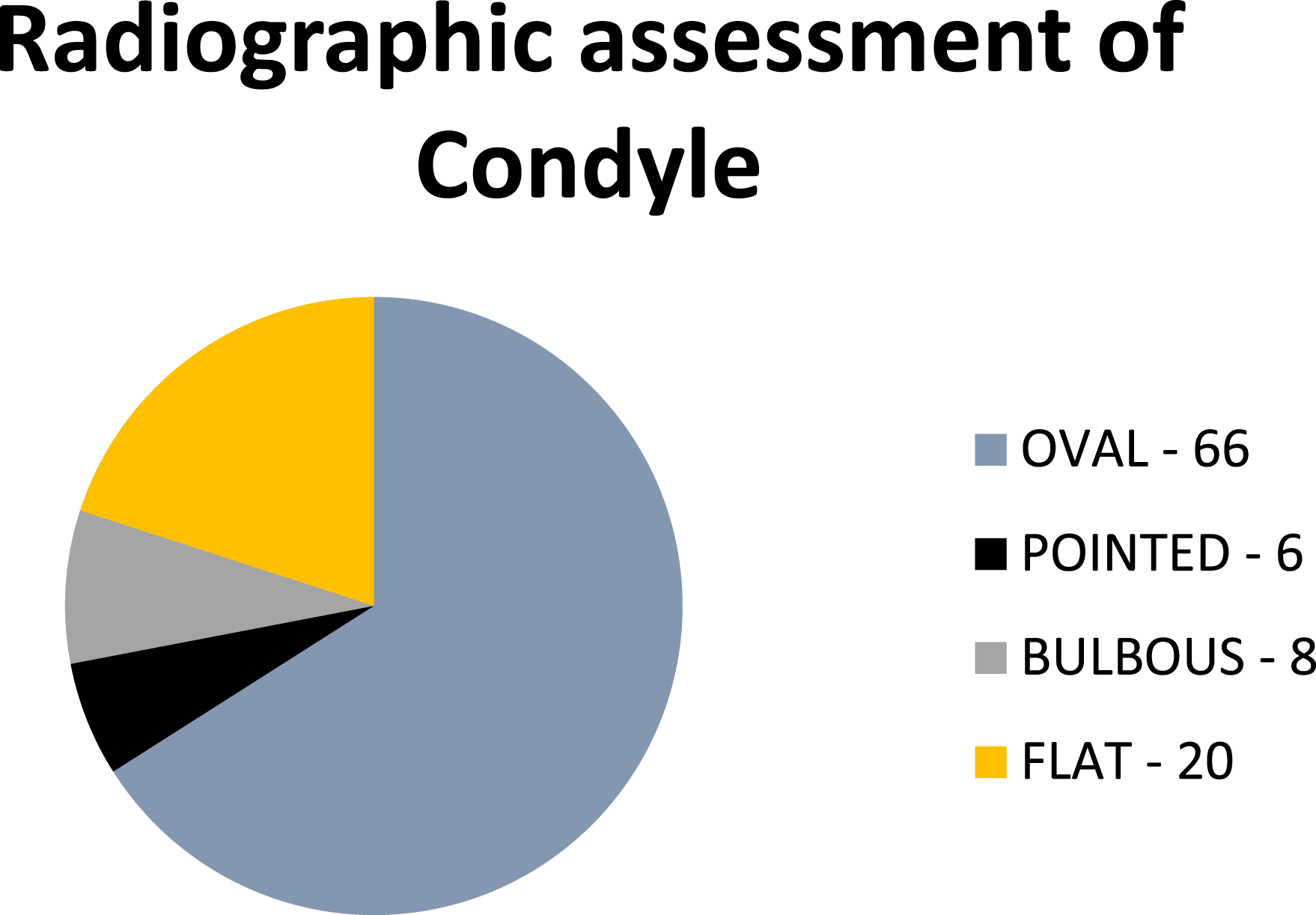
A total of 100 participants with condylar fracture participated in this study with 84% of the participants as males (Figure 1) and an average age of 32.6 ± 1.2 years. The fracture mostly occurred on the right side (Figure 2) and the commonest cause for the fracture was trauma or accident (Figure 3). Subcondylar fracture was seen mostly (55%) when compared to condylar neck and head fracture (Figure 4). 89% of the cases were associated with other mandibular fracture (Figure 5), whereas on 36.2% of the cases were associated with any maxillary fractures (Figure 6). The most common type of mandibular fracture seen was the parasymphysis fracture of the mandible comprising 32.2% of the study (Figure 7). Radiographic assessment of the condylar shaped revealed 66.6% to be oval in shape (Figure 8). Gender distribution. SITE distribution. Mode of incidence. Type of condylar fracture. Distribution of associated mandibular fracture. Distribution of associated maxillary fracture. Distribution of type of associated mandibular fracture. Distribution of radiographic assessment shape of condyle.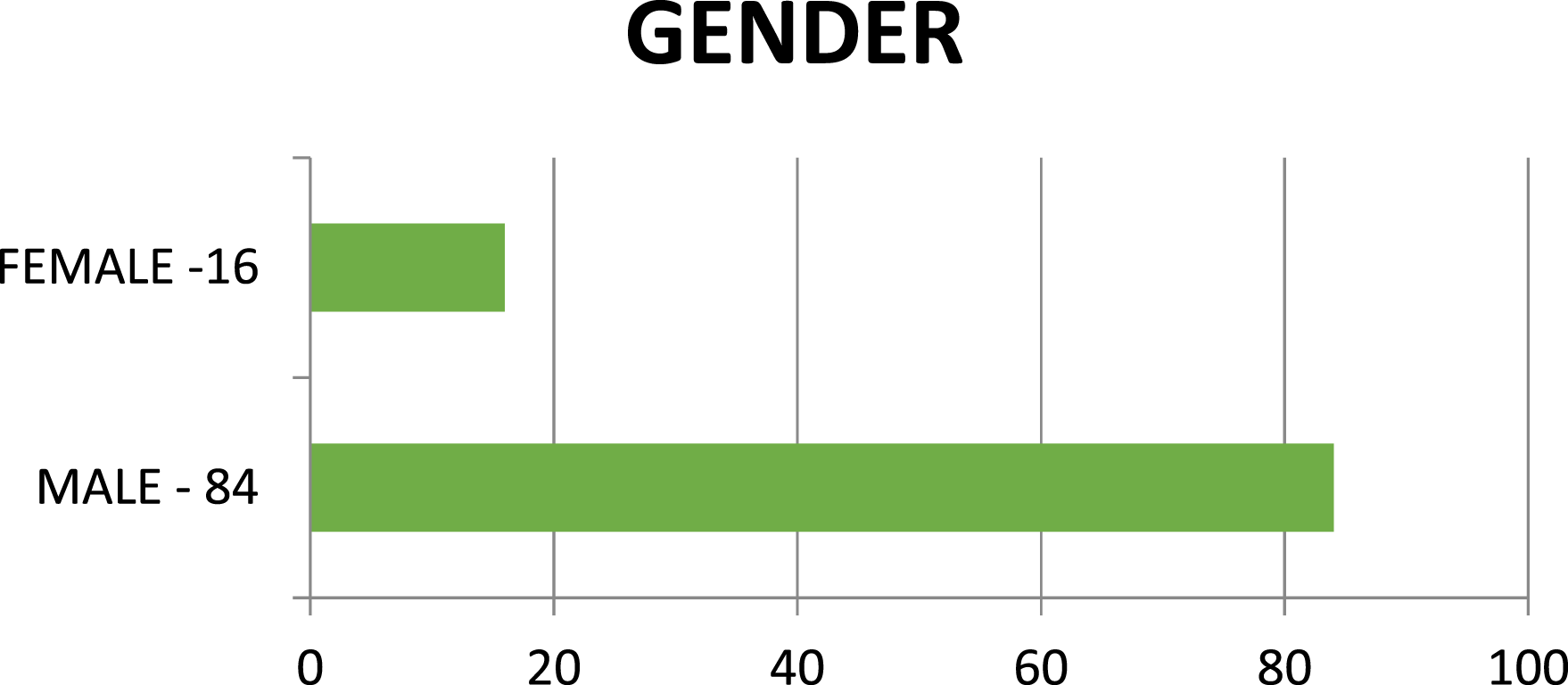
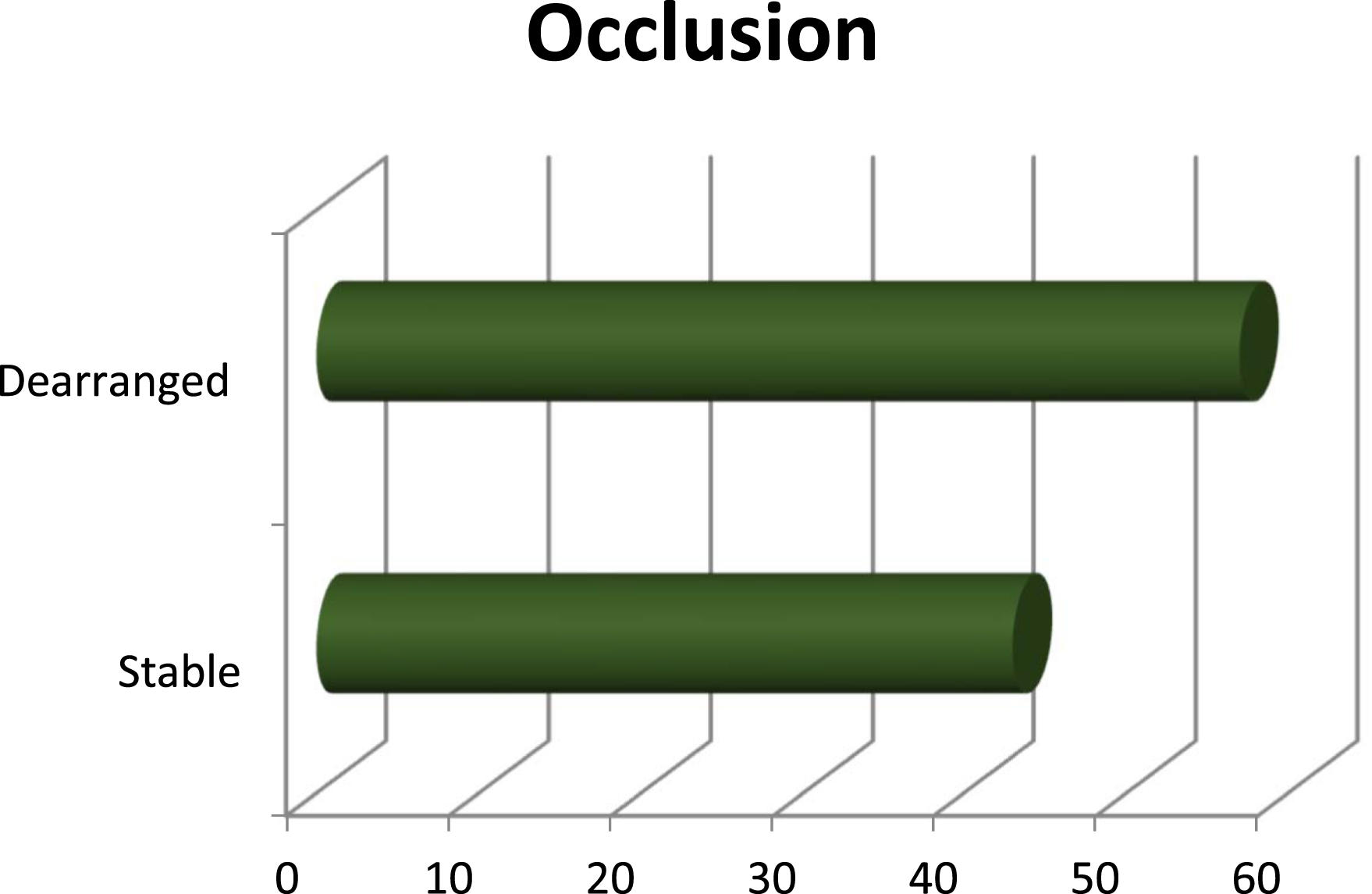
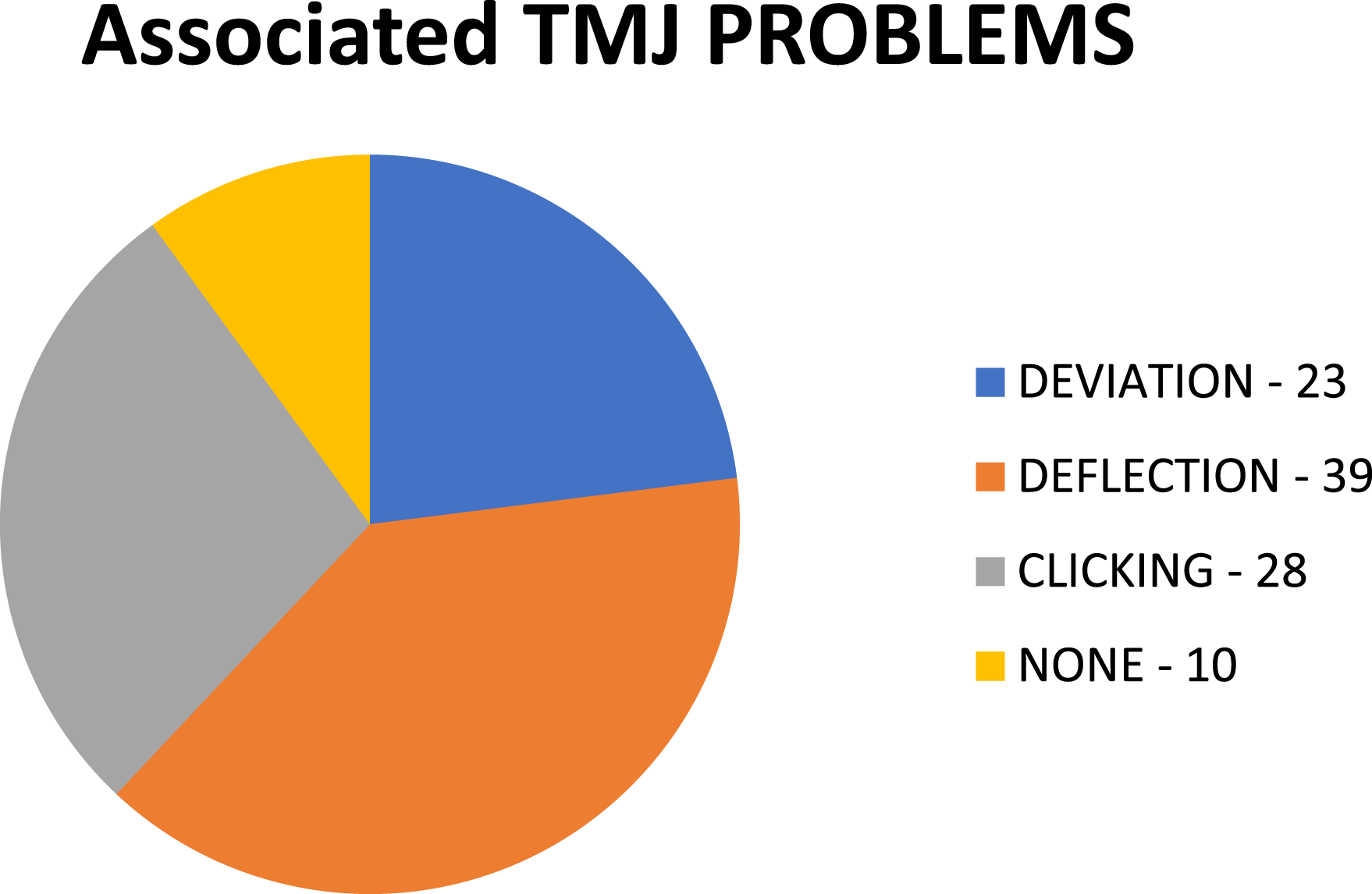
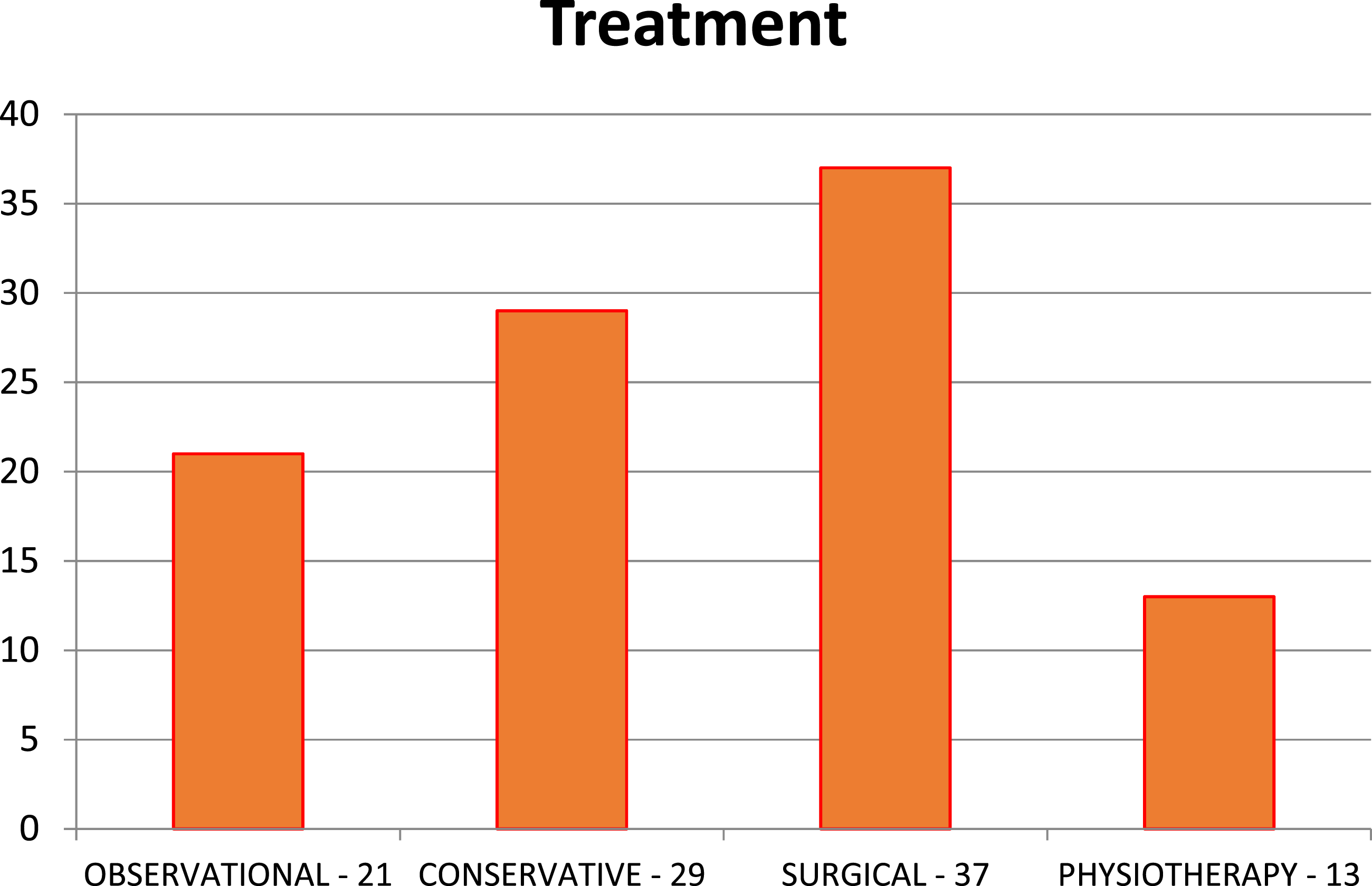
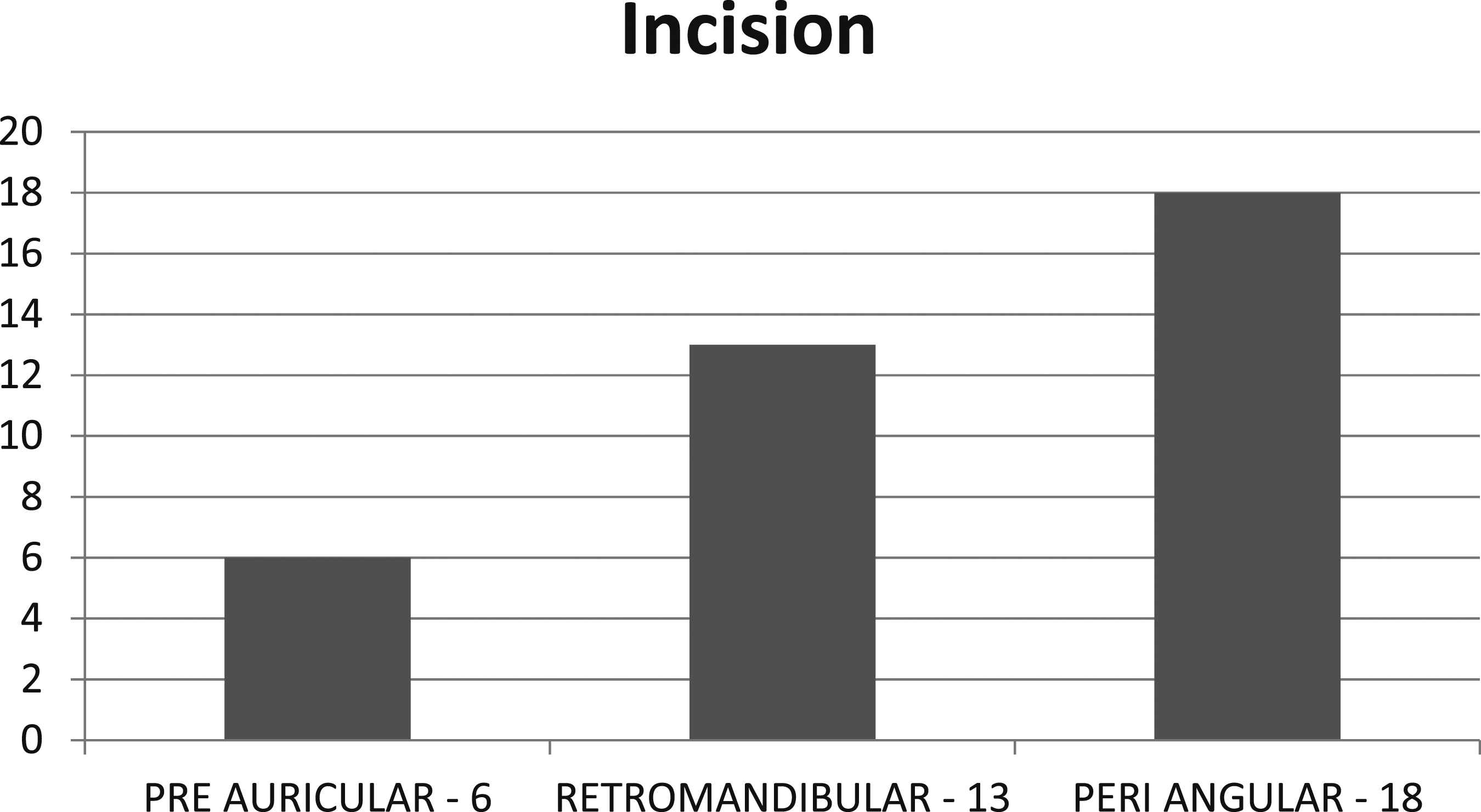
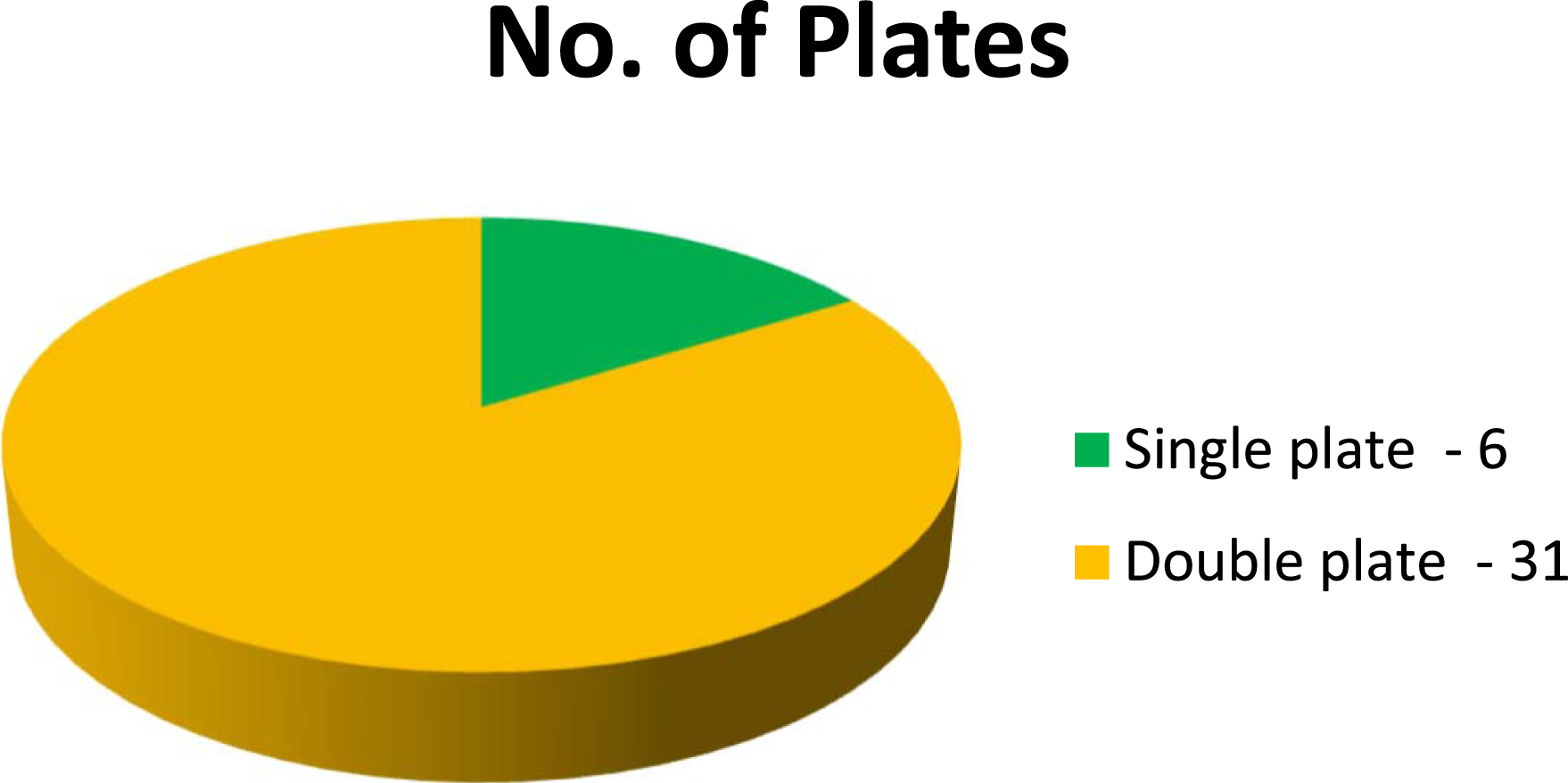
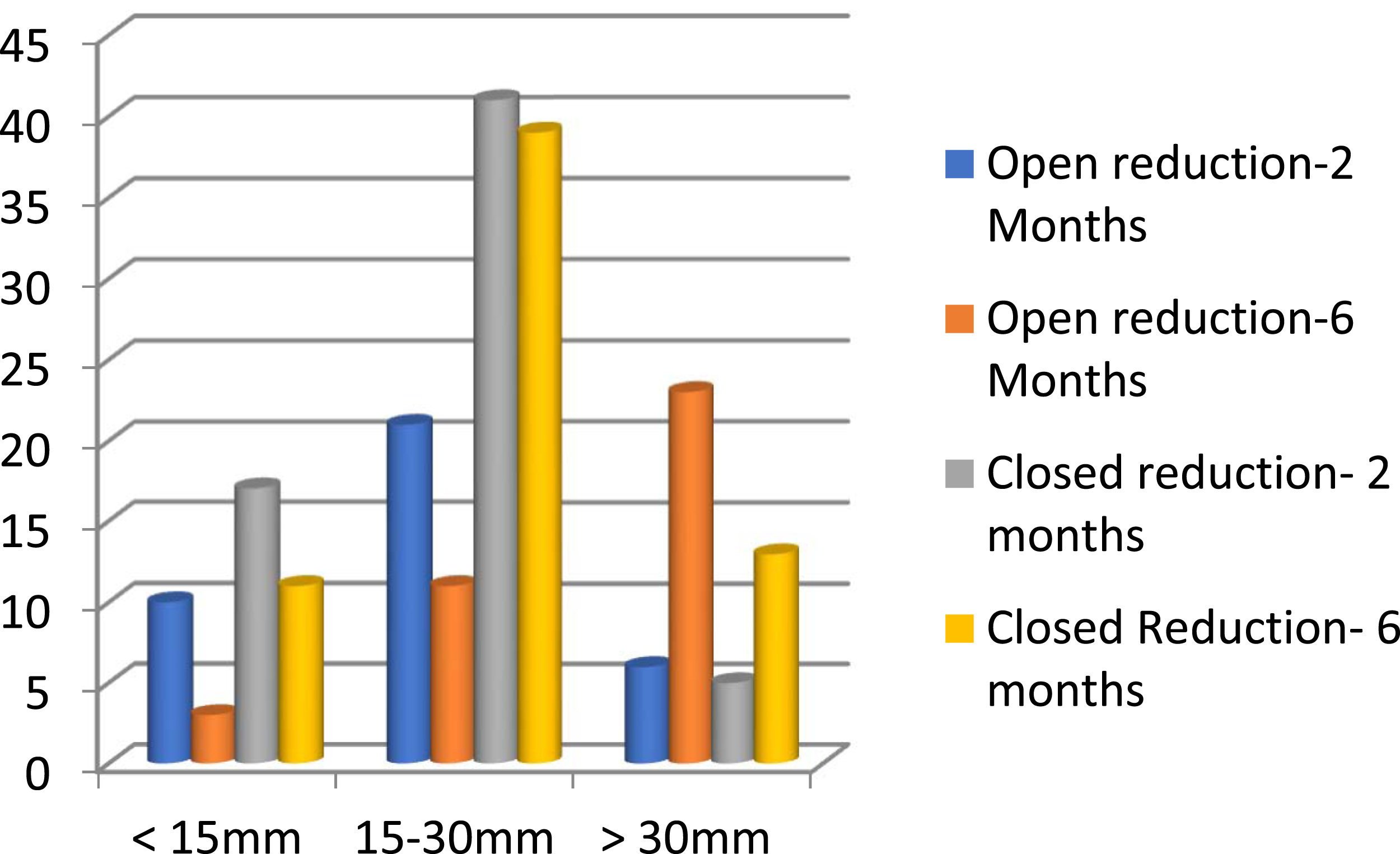
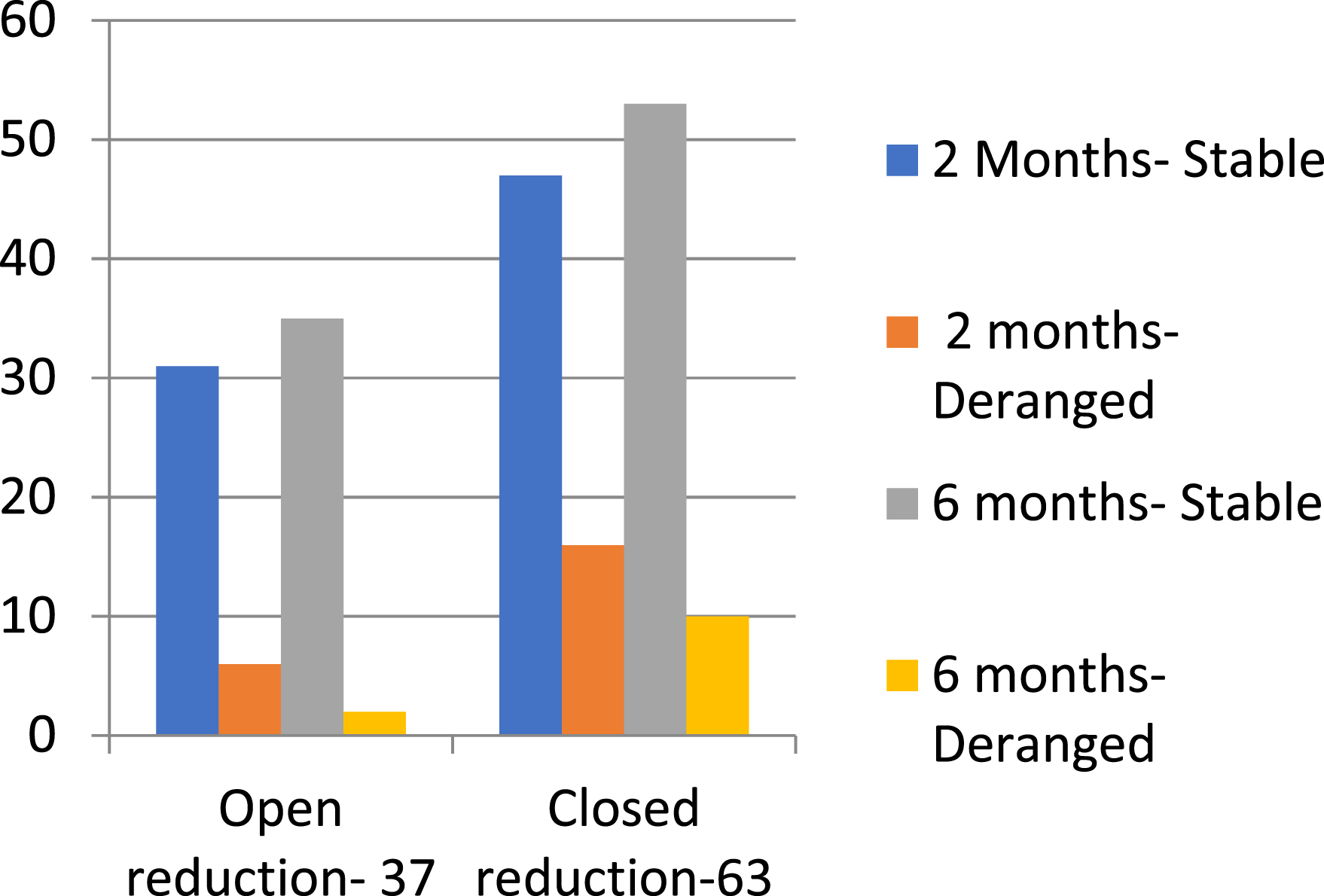
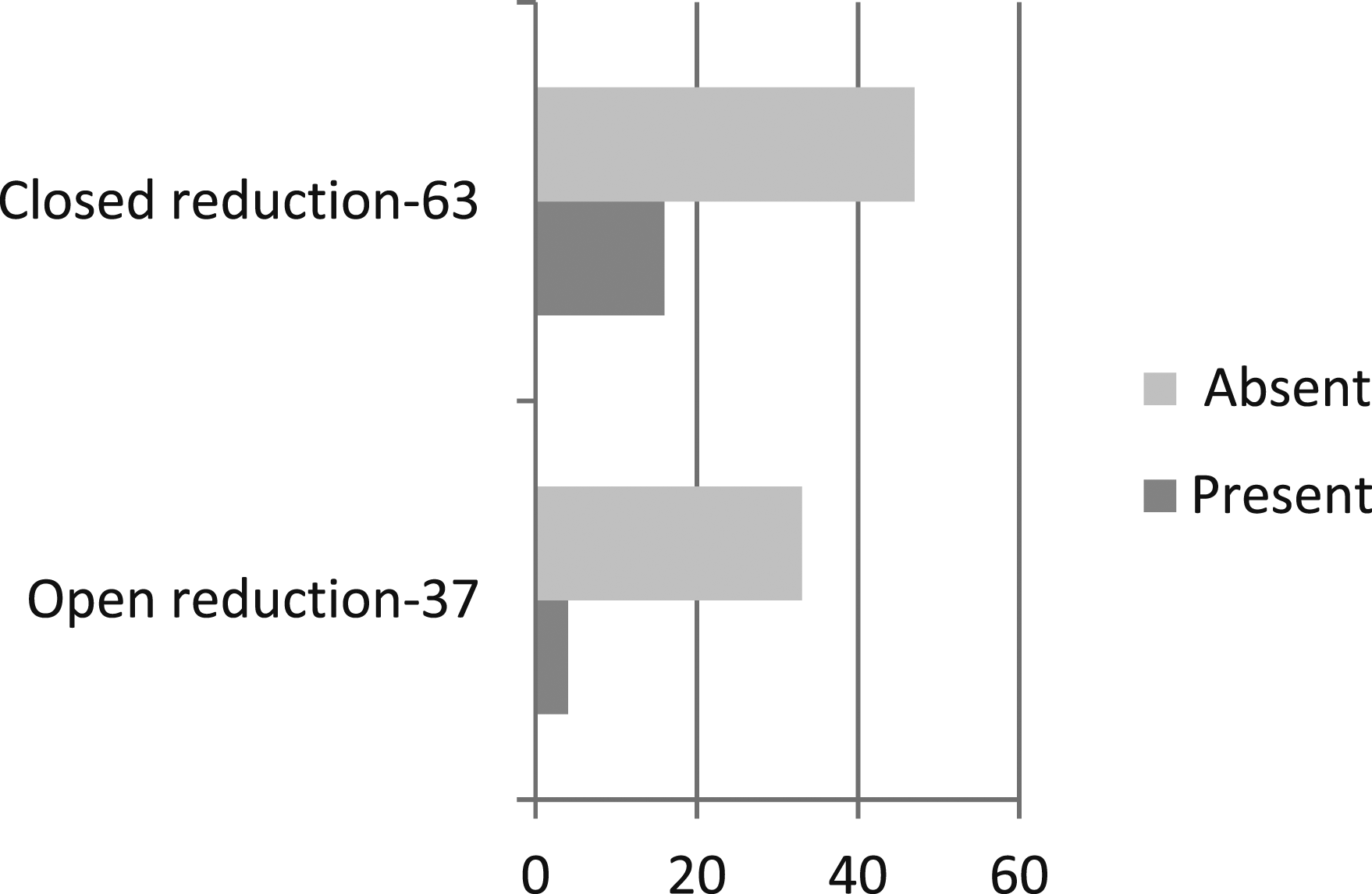
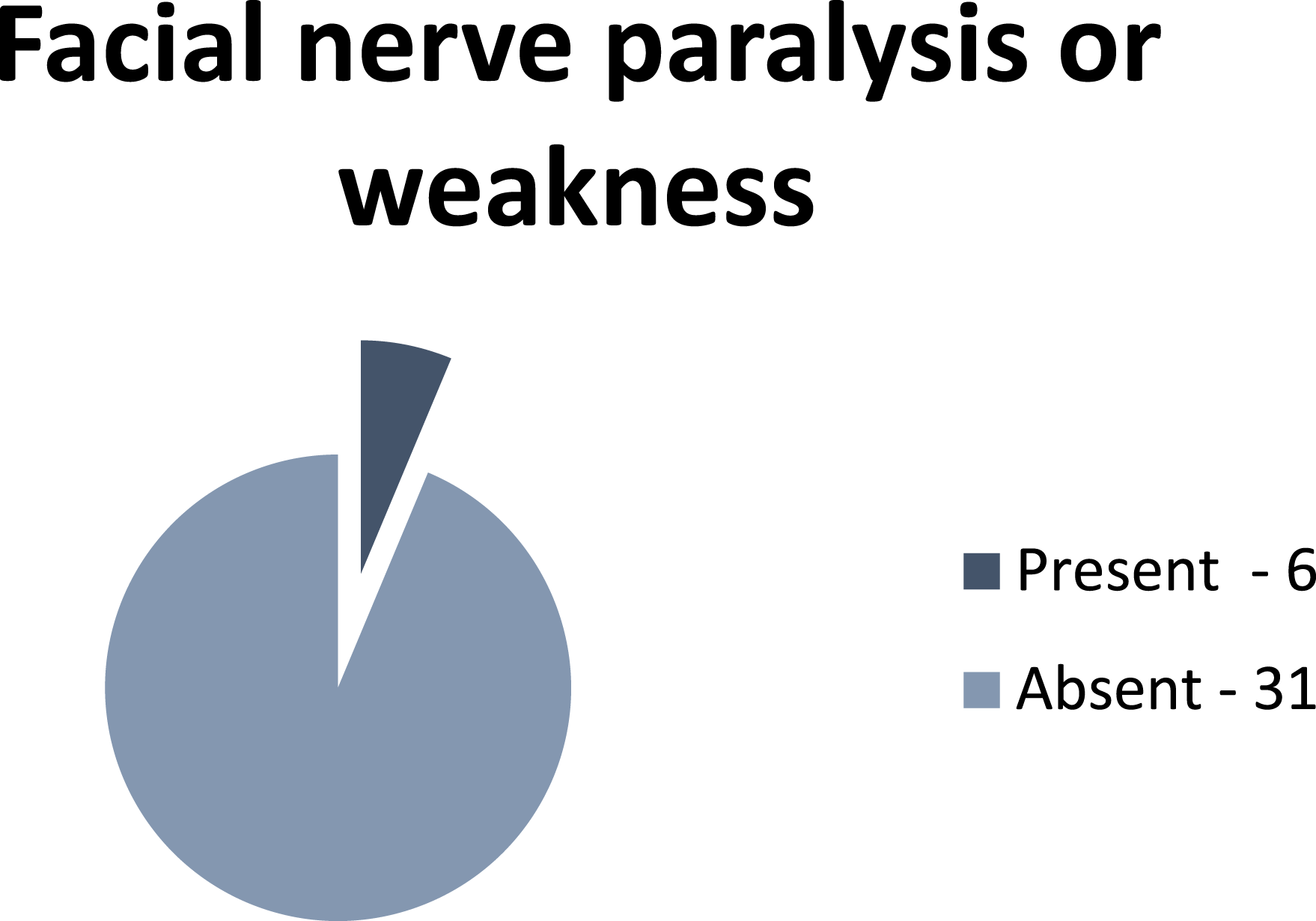
Pre-operatively 33.3% patients had a mouth opening of less than 15 mm (Figure 9), 57% of the patients had deranged occlusion (Figure 10) and only 10% of the patients did not show any associated Temporo-mandibular joint problems (Figure 11). Surgically 37% of the patients were treated whereas 29.7% patients were treated conservatively and 21.7% were just observed (Figure 12). Peri-angluar incision was mostly used (Figure 13) and 83.7% of cases treated surgically were fixed using double plates (Figure 14). Mouth opening when assessed at 6 months post-operatively revealed that only 62.1% of cases had a mouth opening of more than 30 mm when compared to mouth opening assessed at 2 months post-operatively which was 16.2% after open reduction of the condyle; whereas, mouth opening when assessed at 6 months post-operatively revealed that only 20.6% of cases had a mouth opening of more than 30 mm when compared to mouth opening assessed at 2 months post-operatively which was 7.9% after closed reduction of the condyle (Figure.15). Occlusion when assessed at 6 months post-operatively revealed that only 94.5% of cases had a stable occlusion when compared to occlusion assessed at 2 months post-operatively which was 83.7% after open reduction of the condyle; whereas, occlusion when assessed at 6 months post-operatively revealed that only 84.1% of cases had a stable occlusion when compared to occlusion assessed at 2 months post-operatively which was 74.6% after closed reduction of the condyle (Figure 16). Post-operative temporo-mandibular joint pain was seen in 25.3% and 10.8% of the cases that were treated using closed and open reduction, respectively (Figure 17). Facial nerve weakness was seen in 16.2% of the cases post-operatively which resolved within 6 months (Figure 18). Distribution of mouth opening pre-operatively. Distribution of occlusion pre-operatively. Distribution of associated TMJ problems. Distribution of treatment done. Distribution of incisions placed in the surgical treatment of condylar fracture. Distribution of number of plates used. Distribution of assessment of mouth opening post-operatively at 2 months and 6 months intervals. Distribution of assessment of occlusion post-operatively at 2 months and 6 months. Distribution of assessment of TMJ pain post-operatively. Distribution of facial nerve paralysis or weakness.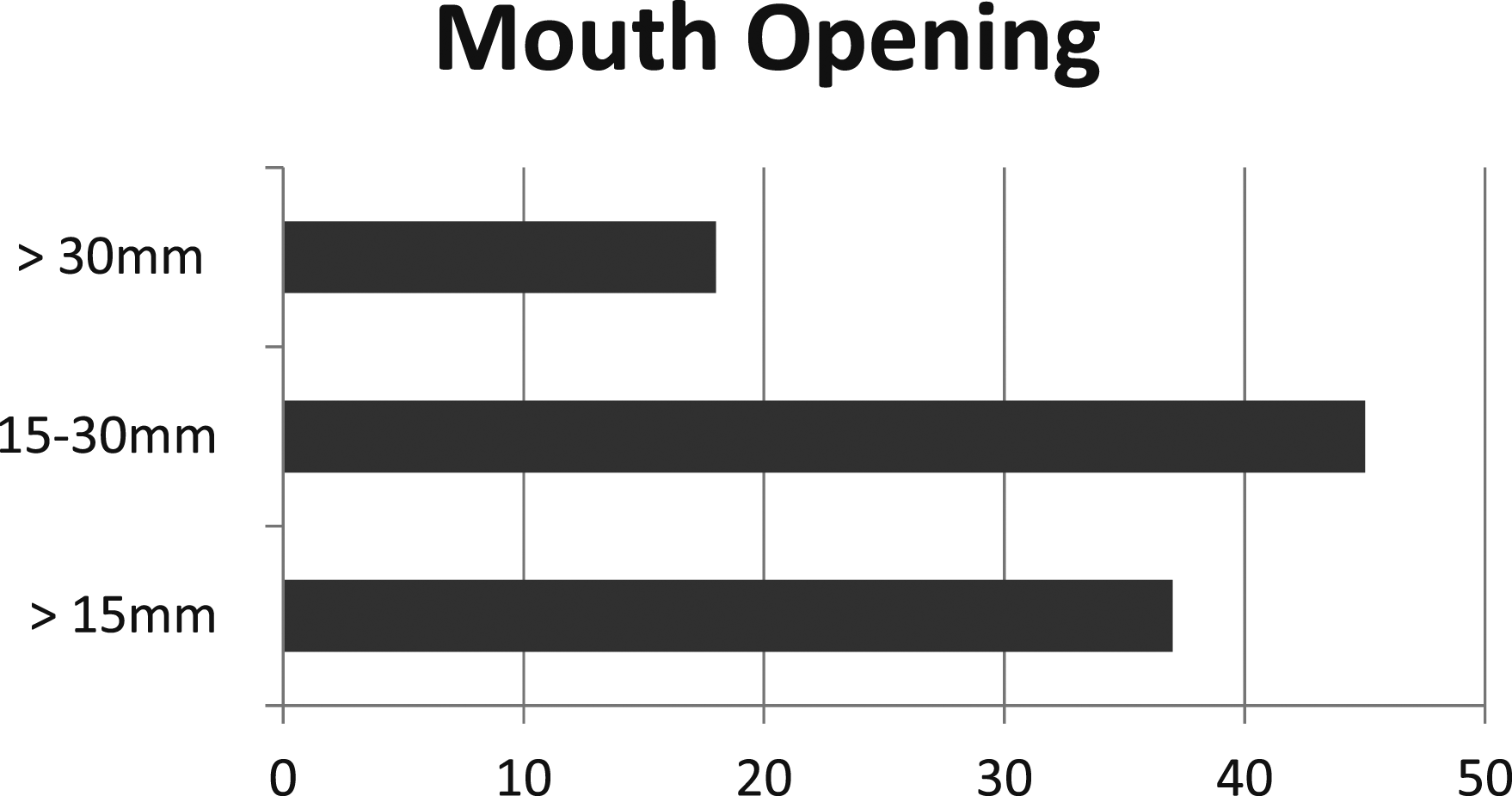
Discussion
Treatment of mandibular condylar fracture has always been in the limelight of maxillofacial traumatology, owing to its intrinsic anatomic configuration, biological healing mechanism and perplexed biomechanics involved. The clinical relevance of condylar fracture managed by closed reduction with or without functional treatment goes undisputed owing to its potential impact on the TM joint function, posttraumatic malocclusion, chronic facial pain and facial asymmetry associated (Figure 19).
12
(A) Occlusion immediately after arch bar placement. (B) Occlusion with elastics. (C) Occlusion with IMF. (D) OPG. (A) Pre op occlusion. (B) Pre op OPG. (C) Fracture site exposure. (D) Fixation with mini-plates. (E) Post op OPG. (F) Post op Occlusion.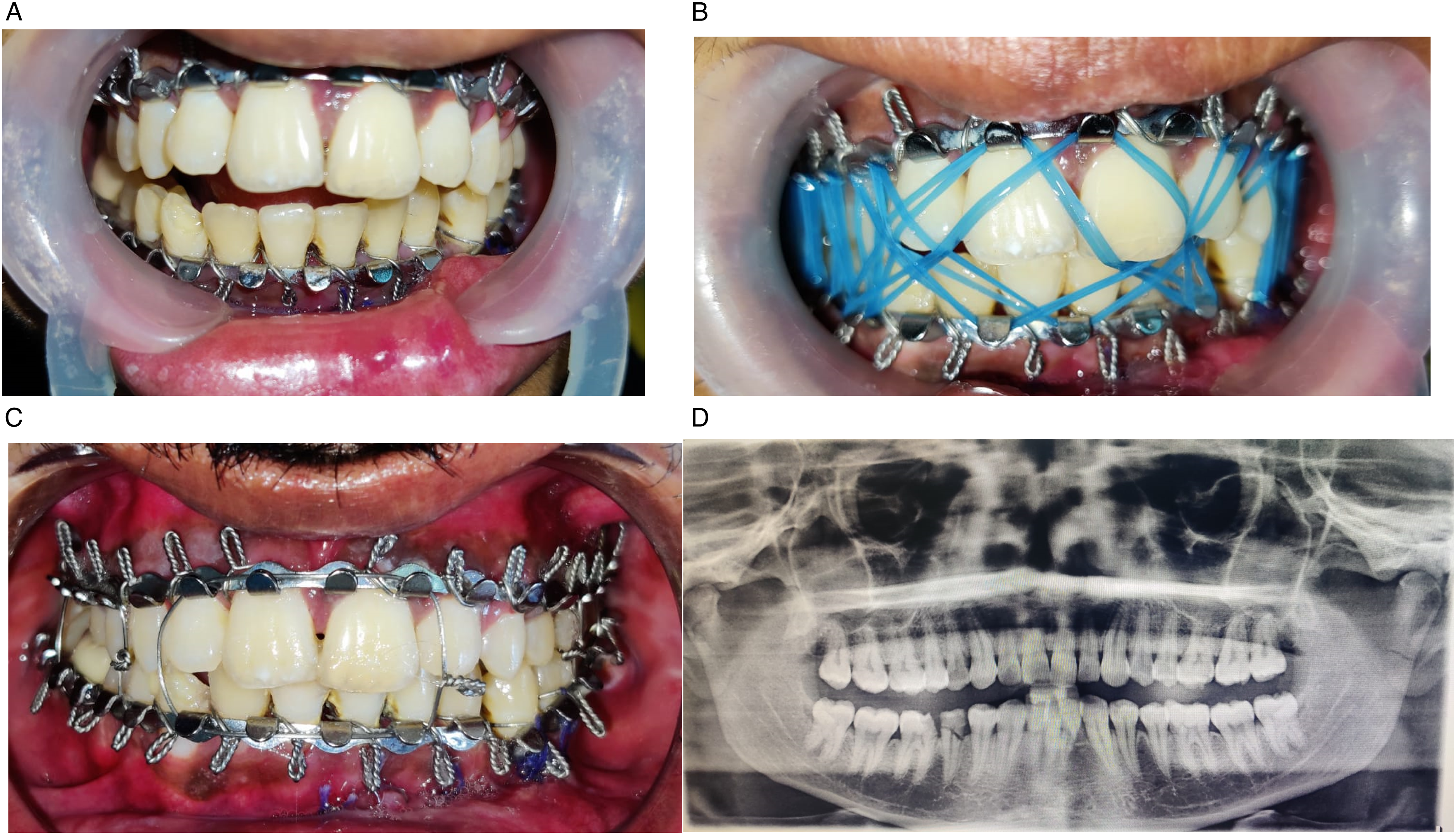
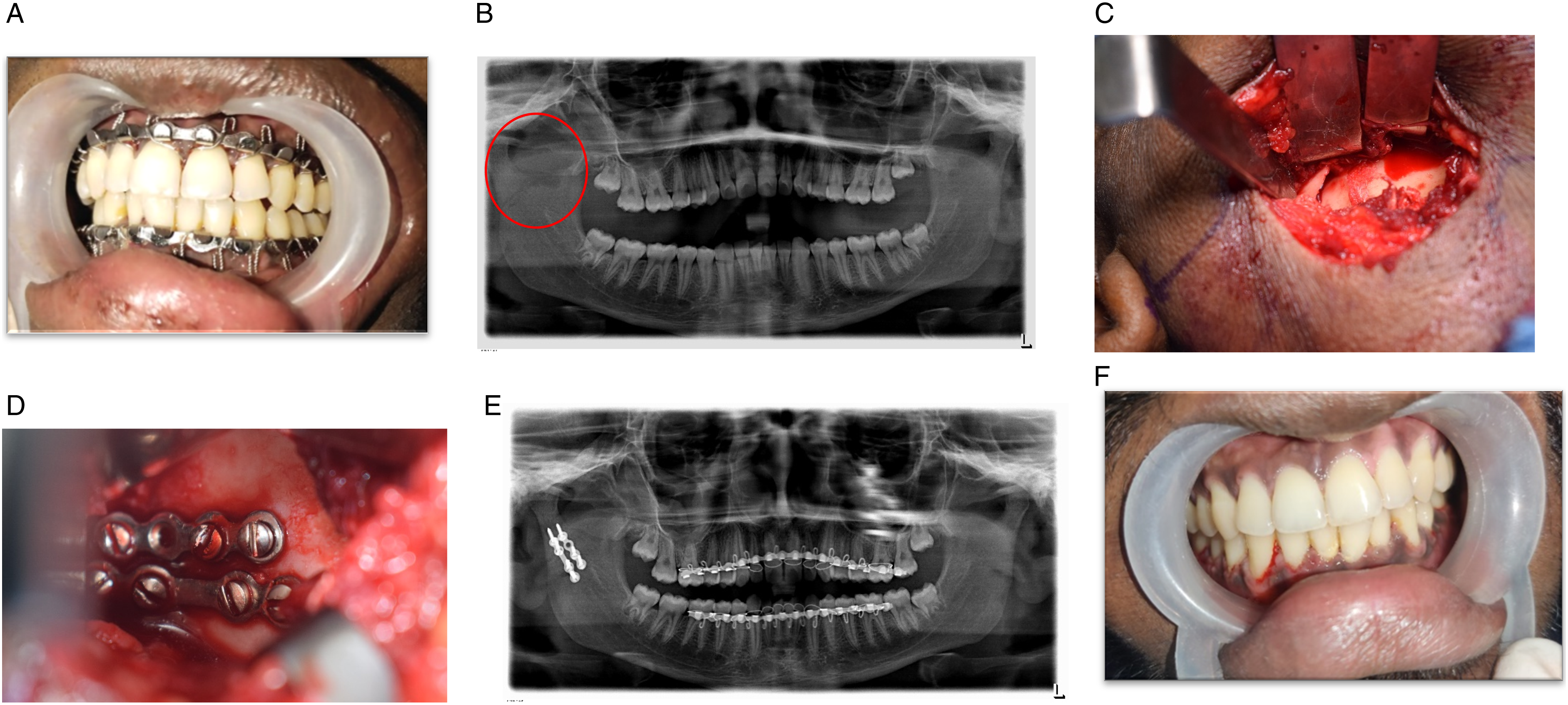
Surgical reduction and fixation on the other hand leads to facial nerve paresis due to inadvertent damage to the any of the branches or facial nerve per se especially when transparotid approach is employed and less importantly the facial scar associated with surgery. 13 Inadequately fixed condylar fracture segment carries the same drawbacks as that of closed reduction primarily due to the direction of pull by lateral pterygoid muscles, and pterygomasseteric sling contraction (Figure 20). 14
Due to this above mentioned adverse effects surgeons opted for the closed reduction protocol of the mandibular condyle as the results obtained with closed reduction was surprisingly of clinical relevance in terms of achievable pre-traumatic occlusion with eccentric mandibular movements through guiding elastics as extensively advocated by Edward Ellis in early 1970s; however, in cases of bilateral subcondylar and neck fracture with severe dislocation and shortening of the ramus height achieving all these clinical parameters wasn’t feasible which lead to the paradigm of shift of the century in sporadic management of condylar fractures surgically. 15
Closed Reduction
Haug and Assael reported that no statistically significant difference between closed and open reduction in achieving occlusion. 16 Jeter et al reported that relatively satisfactory outcomes were obtained from closed reduction for condyle fracture, but that this method could cause mouth opening disorder, mandibular setback, temporo-mandibular pain and functional disorders after long period after injured. 8
Ellis et al 17 reported that complications such as intra-operative bleeding and postoperative infection, facial nerve paralysis, functional disorder of the auriculotemporal nerve and condyle growth disorder significantly increased when open reduction was conducted to treat condylar head and neck fractures, and that closed reduction was more advantageous than open reduction. 17
In our institute, observational treatment with or without inter-maxillary fixation and soft diet was advocated for undisplaced fracture of the condylar head and neck.
Paediatric condylar fractures, condylar head fractures and minimally displaced condylar neck fracture were managed through closed reduction, based on the status of occlusion, deviation during mouth opening, mandibular movements and a negative Ellis drop back test.
Class II guiding elastics based on Edward Ellis protocol was used for achieving occlusion depending on the derangement with a brief period of inter-maxillary fixation not exceeding 2 weeks in adults and 7–10 days in paediatric cases.
Occlusion was almost achieved in all patients, and chronic TMJ pain was noted in some cases usually with associated fracture of the squamous part of the temporal bone. One of the major drawbacks we encountered is patient compliance to a brief period of IMF.
Open Reduction
The shift towards surgical management mainly happened during the 1980s through the introduction of functionally stable osteosynthesis concept for the first time enabling both anatomical repositioning of condylar segments and also achieving early mobilization, TM joint functions. 18
In the study conducted by Ellis et al to compare the occlusal relationships after open and closed reductions for unilateral condylar fractures, the authors concluded that patients treated by closed reduction had a significantly greater percentage of malocclusion compared with those treated by open reduction, inspite of initial displacement of fractures greater in open reduction. 19
Zide and Kent reported the relative and absolute indications for condylar fractures in 1983, management became controversial and new approaches of surgical reduction and fixation were introduced and developed. 10 In the same year, Mathes (1983) mentioned that angulation between the fractured fragments, lateral override and lack of contact of fracture segments should be considered before open reduction and this was also suggested by Klotch and Lundy. 8
In 2003, American Association of Oral and Maxillofacial Surgeons suggested an international guideline on treatment of condylar fractures according to which open reduction was recommended to prevent complications of growth and functional disorder. 20 AAOMS in 2014 and ASIF in 2017 proposed guidelines where in open reduction was considered superior in achieving desirable treatment outcomes. 8
The findings of our study was also consistent with the literature, malocclusion was observed in patients with bilateral condylar fracture and subcondylar fracture with anteromedial/posterolateral displacement most probably due to interference of fracture segments during mandibular movements, majority of our cases also showed varying degree of shortening of posterior ramus height. Hence, cases with bilateral condylar fractures, condylar fractures with more than 10 degree of displacement, shortening of vertical ramus height and positive Ellis drop back test, open reduction and internal fixation was done.
Inadvertent damage to the facial nerve or its branches was seen when transparotid approach was employed one of the main complications associated with open reduction. Even we had cases with transient facial parasthesia. However, it resolved within 3–6 months.
In our institute, we followed plating the proximal and distal ends of fracture segments using 2 mm mini-plates. Though cases of stress shielding are reported by authors in literature, we haven’t encountered it in our experience.
IMF was not required in majority of our patients treated with open reduction and internal fixation. In cases where there is deranged occlusion guiding elastics with a brief period of IMF for a week was done. Patient compliance was excellent towards open reduction compared to closed reduction.
Our study entails the protocol we followed in our institute. We observed and reported multiple parameters to be considered in treating condylar fracture. Based on Ellis drop back test, AAOMS and ASIF guidelines clinical decision was made for closed and open reduction, both producing promising results with its own merits and demerits. Closed reduction stands out exceptionally in treating paediatric condylar fractures. However, it has its own limitations in efficiently addressing bilateral displaced subcondylar fractures with loss of posterior ramus height.
Conclusion
The extensive debate of closed vs open reduction of condylar fracture over 30 years of scientific literature still continues without any final consensus yet more in favour towards the surgical reduction and fixation of condylar fracture. At the same time, the traditional time tested treatment option through closed reduction and observation also holds equally good. We endorse the same based on our experience in treating condylar fractures over the last 5 years. The art of decision making solely depends on the surgeon’s expertise in managing condylar fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.