
Abstract
Unpaid caregiving is associated with significant burdens, including financial strain, time constraints, diminished quality of life, and elevated stress levels. Despite these challenges, existing literature on disease burdens devotes limited attention to caregiver experiences. The aim of this scoping literature review was to identify instruments used to measure caregiver burden to better inform future studies of caregiver costs. This study included articles that estimated the costs or burdens associated with unpaid caregiving to patients in the United States and used a survey or cohort study design to conduct primary or secondary quantitative data analysis. Across the 46 articles abstracted, 27 unique survey instruments were identified; 23 (89%) instruments were validated, 12 (46%) were publicly available, and 14 (54%) were designed for or validated among caregivers. Among studies included in this review, 18 (39%) studies designed their own questionnaires to assess caregiver burden. This review additionally identified six nonsurvey data sources, such as medical claims data, used to estimate caregiver costs. The heterogeneity across measurement tools limits comparability across studies. Standardized, validated, and accessible instruments are essential for understanding caregiver burdens and advancing research to improve outcomes for patients and their caregivers.
Unpaid care plays a crucial and indispensable role in the health care, economic, and social landscape of the United States. An estimated 21% of US adults provide unpaid care to family members or friends, often stepping in as an extension of the health care system. 1 These unpaid caregivers—typically family members, partners, or close friends—offer nonprofessional, unpaid support to individuals with chronic illnesses, disabilities, or age-related conditions to help them maintain daily function and quality of life.2,3 Their responsibilities span a wide range of tasks, including personal hygiene assistance, managing medications, providing meals, helping with mobility, and facilitating transportation to health care appointments.
Reliance on unpaid caregivers is becoming increasingly critical as the US health care system confronts an aging population with complex medical needs, including multiple chronic conditions and cognitive impairments such as Alzheimer’s disease. A report by the Assistant Secretary for Planning and Evaluation found that by 2040, the number of adults who need regular caregiving services will grow by 30%. 4 However, the United States is facing significant shortages in the direct care workforce. 5 Direct care workers—including home health aides, personal care aides, and nursing assistants—are in short supply due to low wages, high turnover, limited training opportunities, and challenging work conditions.6,7 Many long-term care facilities and home care agencies are unable to recruit and retain sufficient staff to meet demand, particularly in rural or underserved areas.8–10 This structural inadequacy in the formal care sector has placed an even greater burden on families to fill in the gaps through unpaid care.
Despite the critical value of unpaid caregiving, caregivers often face substantial personal and financial burdens. Specifically, caregivers frequently incur work-related opportunity costs such as missed workdays, reduced work hours, career disruptions, or early retirement. 11 Many caregivers also need to modify their living arrangements or household routines to accommodate the care recipients’ needs, leading to feelings of stress and anxiety for the caregiver.12,13 Caregivers may also expend as much as 26% of their annual income on caregiving-related activities, including out-of-pocket medical expenses, medication costs, and assisted living facilities, contributing to feelings of financial strain and diminished household wealth. 14
Current literature on disease burdens patients and their families experience focuses on the patient perspectives, often neglecting the unique and additional challenges caregivers face.15–17 Two recent systematic reviews of out-of-pocket costs and indirect burdens borne by patients and families or caregivers found that only 20% of studies (n = 100) incorporated the caregiver perspective.16,17 This omission is significant, as the burdens caregivers experience may be different from and additional to those patients experience, potentially leading to an underestimation of the overall impact of a disease. Furthermore, among the limited studies that do address caregiver burdens, definitions and methodologies are often inconsistent. 15 These discrepancies hinder meaningful comparisons of burdens across studies and complicate efforts to monitor changes over time.
The goal of this review was to assess the methods and instruments used to collect caregiver burdens and identify the instruments that have been validated to better inform future studies of caregiver costs. This work builds on prior systematic reviews that identified patient and caregiver burdens.
Materials and Methods
Search and data sources
The authors of the current study identified a recent systematic review by Schmidt et al. 17 that focused on burdens accrued by patients or unpaid caregivers, including direct medical costs, direct nonmedical costs, and indirect impacts. As Schmidt et al. 17 included multiple categories of caregiver costs, the authors obtained and screened the list of citations included in Schmidt et al. 17 as a starting point for this review.
Schmidt et al. 17 searched PubMed, Embase, and Cochrane for English-language articles published between April 2017 and March 2022. The review included quantitative and qualitative studies of patient or caregiver burdens but excluded studies without patient or caregiver burdens; studies for which reported burdens could not be differentiated into categories; estimates for economic analyses, such as cost-of-illness studies and cost-effectiveness analyses; and policy analysis predicting future impacts.
In addition to screening the studies in Schmidt et al., 17 the authors searched PubMed for articles published between April 2022 and August 2024 using the search terms in Schmidt et al. 17 The goal of this additional search was to expand the timeline of this scoping review and capture more recent publications. However, in this expanded PubMed search, the authors excluded terms relating to patients, including patient, beneficiary, and enrollee, because caregivers are the focus of this review. The authors also did not use the same list of exclusion terms from Schmidt et al. 17 and instead opted to manually screen these exclusions out given that the search time frame of this study was shorter, and the inclusion criteria was expected to yield a manageable number of citations. See Appendix A for the detailed search strategy for Schmidt et al. 17 and this review.
Study selection and data abstraction
The Preferred Reporting Items for Systematic reviews and Meta-Analyses and Joanna Briggs Institute guidance for scoping reviews was used to guide the screening and abstraction processes.18,19 This study used a two-stage screening process to identify relevant studies. For the title/abstract and full-text review stages, the authors conducted a dual independent review of each article. A third reviewer was consulted to resolve disagreements at each stage. Studies were excluded if the full-text article was unavailable.
This review was limited to peer-reviewed research that (1) estimated the costs or burdens associated with unpaid caregiving (eg, care provided by family or friends) to patients, (2) focused on a US population, (3) was published in English, and (4) used a survey or cohort study design to conduct primary or secondary quantitative data analysis. This reviewed included studies whose data collection included the United States but also spanned other countries. Outcomes included any burden experienced by caregivers while providing care related to a medical need to a patient, such as work-related absenteeism or lost wages, presenteeism, transportation or travel, reductions in quality of life, and stress or anxiety resulting from caregiving. The authors excluded studies whose focus was on caregiving for nonmedical conditions, such as parental caregiving in absence of a medical need. Appendix B details the study inclusion criteria.
The authors used DistillerSR to abstract the study’s purpose, country, disease or treatment, sample size, caregiver burden categories, study survey instrument or secondary data sources, and frequency of data collection. The authors abstracted caregiver burden and study survey instrument information for direct medical costs, direct nonmedical costs, and indirect impacts because Schmidt et al. 17 collected these categories. Although Schmidt et al. 17 did not explicitly search for intangible burdens, the authors of this study also collected these data points for any intangible burden studies meeting the inclusion criteria that reported them. A single reviewer abstracted each study, whereas a second reviewer verified the abstracted elements.
Data synthesis
For each survey instrument identified in the data abstraction, the authors reviewed the instrument’s website (if available), the peer-reviewed literature, and the gray literature to identify burdens that are collectible in the instrument, the number of items included in the instrument, and whether the instrument was publicly available. The authors also conducted a search of the peer-reviewed literature to determine whether the instrument had been validated.
Instruments were categorized by the overarching type of burden collected, including direct medical, direct nonmedical, indirect, and intangible burden. This categorization is consistent with prior literature reviews on patient and caregiver burdens.16,17,20 Direct medical costs include costs caregivers spend for health care services, such as copays, home health care costs, and medication costs. These may include costs for health care services for the patient or costs for health care services for the caregiver for conditions resulting from caregiving. Direct nonmedical costs include all other out-of-pocket spending attributable to managing or treating the patient (but not directly for medical services). Indirect impacts include measurable nonmonetary outlays that affect caregiver well-being and can be quantified, including caregiver productivity, financial impacts, and time impacts. Intangible burdens are also impacts to caregiver well-being, but intangible burdens represent qualitative experiences and feelings that are challenging to quantify, including psychological burdens and coping behaviors. 20 The authors identified burden categories using the reported elements in the instrument. The authors categorized instruments that collected elements from only one type of burden as one-dimensional survey instruments and instruments that collected elements across multiple burden categories (eg, direct medical and indirect elements) as multidimensional.
Results
Overview
The search strategy returned 952 records; 815 of these records were identified from Schmidt et al., 17 and the expanded search in PubMed identified 137 records (Fig. 1). Among these citations, 85 of these records were included for full-text review; however, the full texts for four records were unable to be located and these four records were excluded from further review. Of the 81 records screened during the full-text review, 46 studies were abstracted in this review. Most records were excluded for focusing on a non-US caregiver population (n = 860, 94%). A subset of records used only qualitative methods and were ineligible for this review (n = 42, 4%).
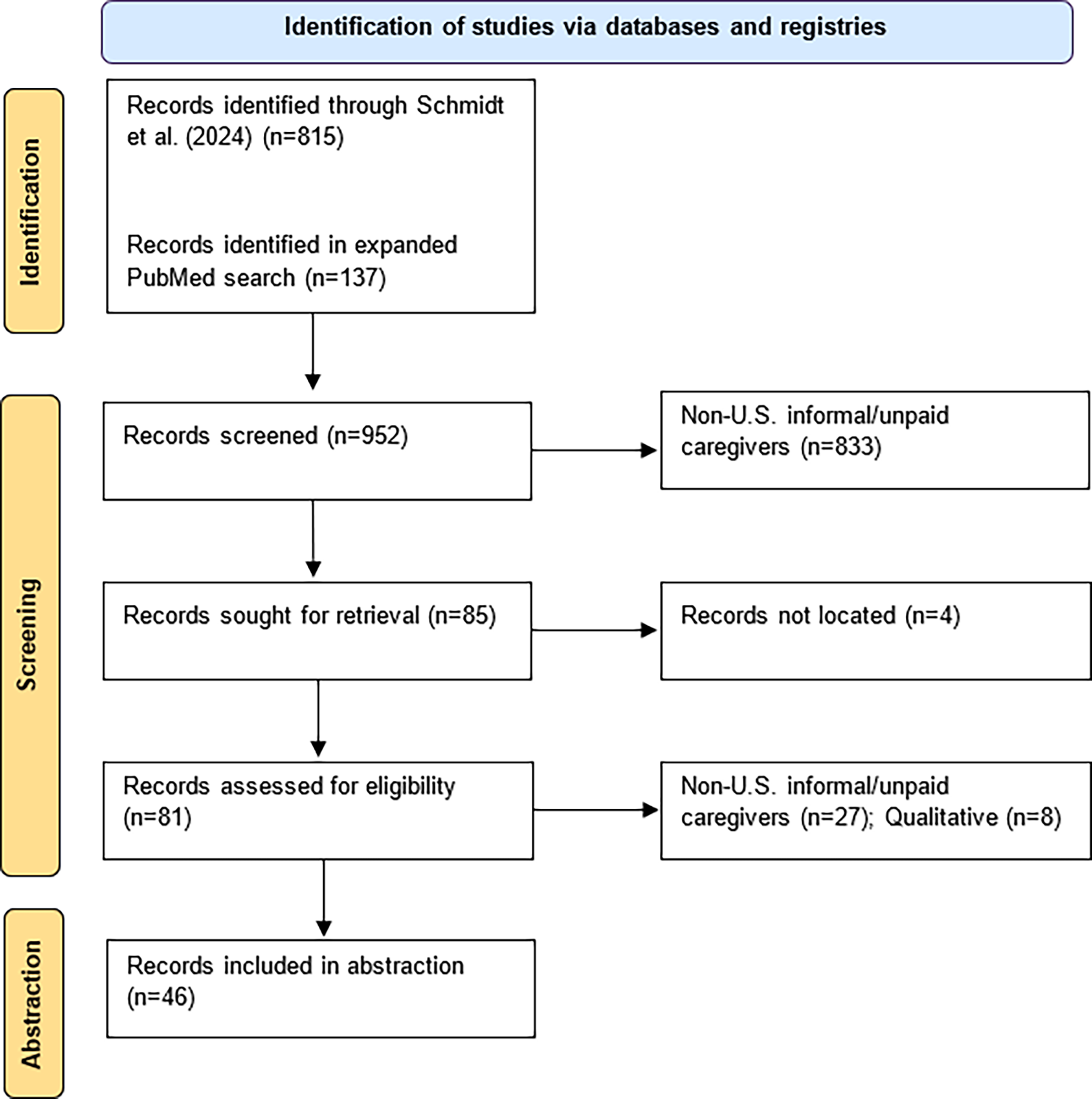
PRISMA diagram. A search of PubMed and a prior systematic review identified 952 articles. After abstract and full-text review, 46 articles met the inclusion criteria and were included for further analysis. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Table 1 describes the studies included in this review. Slightly more than half of studies (n = 24, 52%) focused on caregiver and patient burdens, whereas the remaining half focused on caregiver burdens alone (n = 22, 48%). More than half of all studies (n = 24, 52%) examined data on a national level, whereas fewer studies looked at multiple sites (n = 9, 20%) and single institutions (n = 10, 22%). Three studies (7%) examined data across multiple countries, including the United States. Surveys were the most common instrument for quantitative data collection (n = 41, 89%). Two studies used medical records, and five studies used medical claims. Only two studies used qualitative interviews in addition to their quantitative data collection. Other data sources included telemedicine appointment records and employee absenteeism data from integrated employer databases. Nine studies used a combination of data sources, including medical claims and employee absenteeism data (n = 4, 8%), survey and medical records (n = 1, 2%), survey and medical claims (n = 1, 2%), survey and telemedicine appointment records (n = 1, 2%), and surveys and interviews (n = 2, 4%). The majority of studies in this review were cross-sectional studies (n = 32, 70%), followed by retrospective cohort studies (n = 7, 15%), prospective cohort studies (n = 5, 11%), case–control (n = 1, 2%), and randomized controlled trials (n = 1, 2%).
Caregiver-Only and Caregiver/Patient-Focused Studies
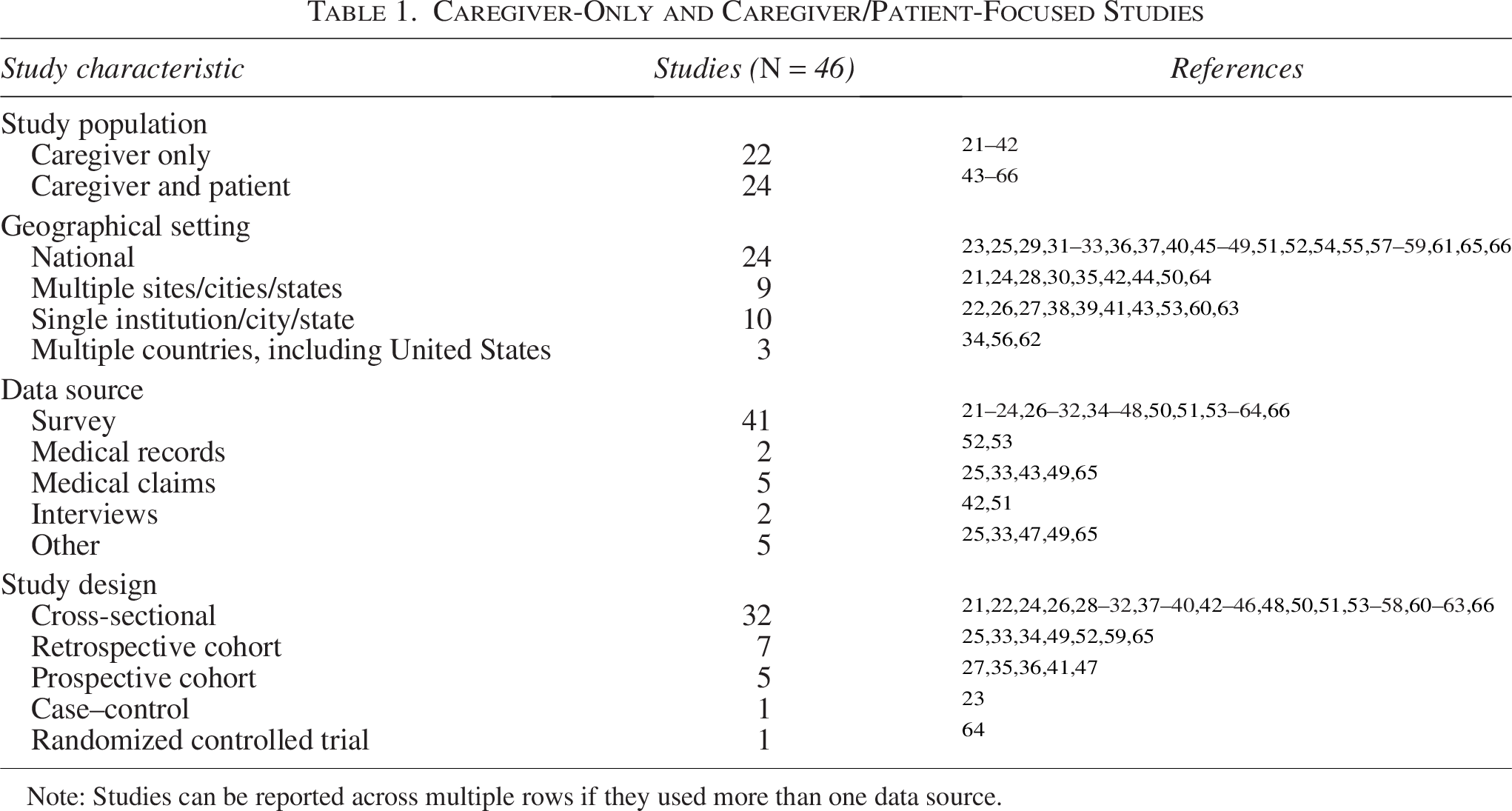
Note: Studies can be reported across multiple rows if they used more than one data source.
Nearly half of the studies in this review used an existing survey instrument (n = 21, 46%), whereas 18 studies (39%) designed one or more of their own questionnaires, and 8 studies (17%) did not report any information on their survey tool. In addition, 13 studies (28%) used other, nonsurvey data sources as their sole data source or in combination with a survey.
Caregiver burdens
Table 2 lists the four caregiver burden categories: direct medical, direct nonmedical, indirect and intangible, and corresponding subcategories identified by studies in this review. Among studies reporting direct medical costs, most studies did not indicate a subcategory (n = 19). The next most common direct medical cost subcategories were diagnosis/treatment/management costs (n = 7) and medical supply costs (n = 5). Only one study each estimated dental costs, hospice care costs, and long-term care facility costs.
Caregiver Burden Categories Estimated by Studies Included in this Review (N = 46)
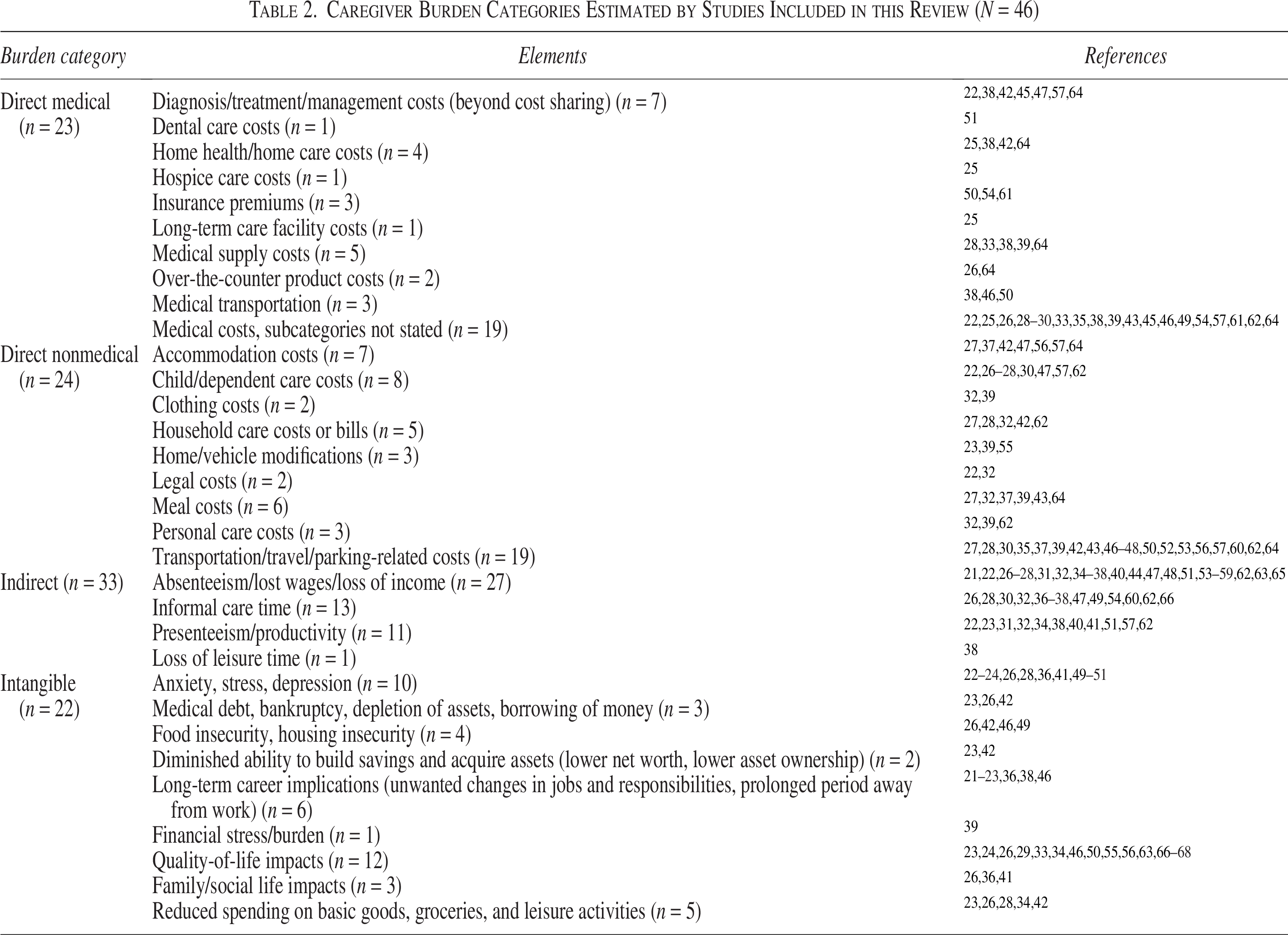
Among studies reporting direct nonmedical costs, transportation/parking costs were most frequently estimated (n = 19), followed by child/dependent costs (n = 8) and accommodation costs (n = 7). Among studies reporting indirect impacts, studies most commonly estimated absenteeism/work loss (n = 26), time spent caregiving (n = 12), and presenteeism (n = 10). One study also collected data on lost leisure time among caregivers.
Among studies estimating intangible burdens, quality of life was the most commonly estimated subcategory (n = 12), followed by long-term career implications (n = 6) and reduced spending on basic goods, groceries, and leisure activities (n = 5).
One-dimensional survey instruments, by burden category
This study identified 19 unique one-dimensional survey instruments; these instruments collected direct medical, indirect, and intangible burdens among unpaid caregivers across 20 studies (Table 3).
Only one study used a one-dimensional existing survey instrument for direct medical costs, the CommonWealth Fund Biennial Health Insurance Survey (Table 3). This questionnaire is publicly available and includes questions on health insurance coverage and out-of-pocket medical costs. The study that employed the CommonWealth Fund questionnaire used a subset of questions from the survey on unexpected costs, increased out-of-pocket expenses, and financial worry.
Instruments Used to Collect Direct Medical Costs
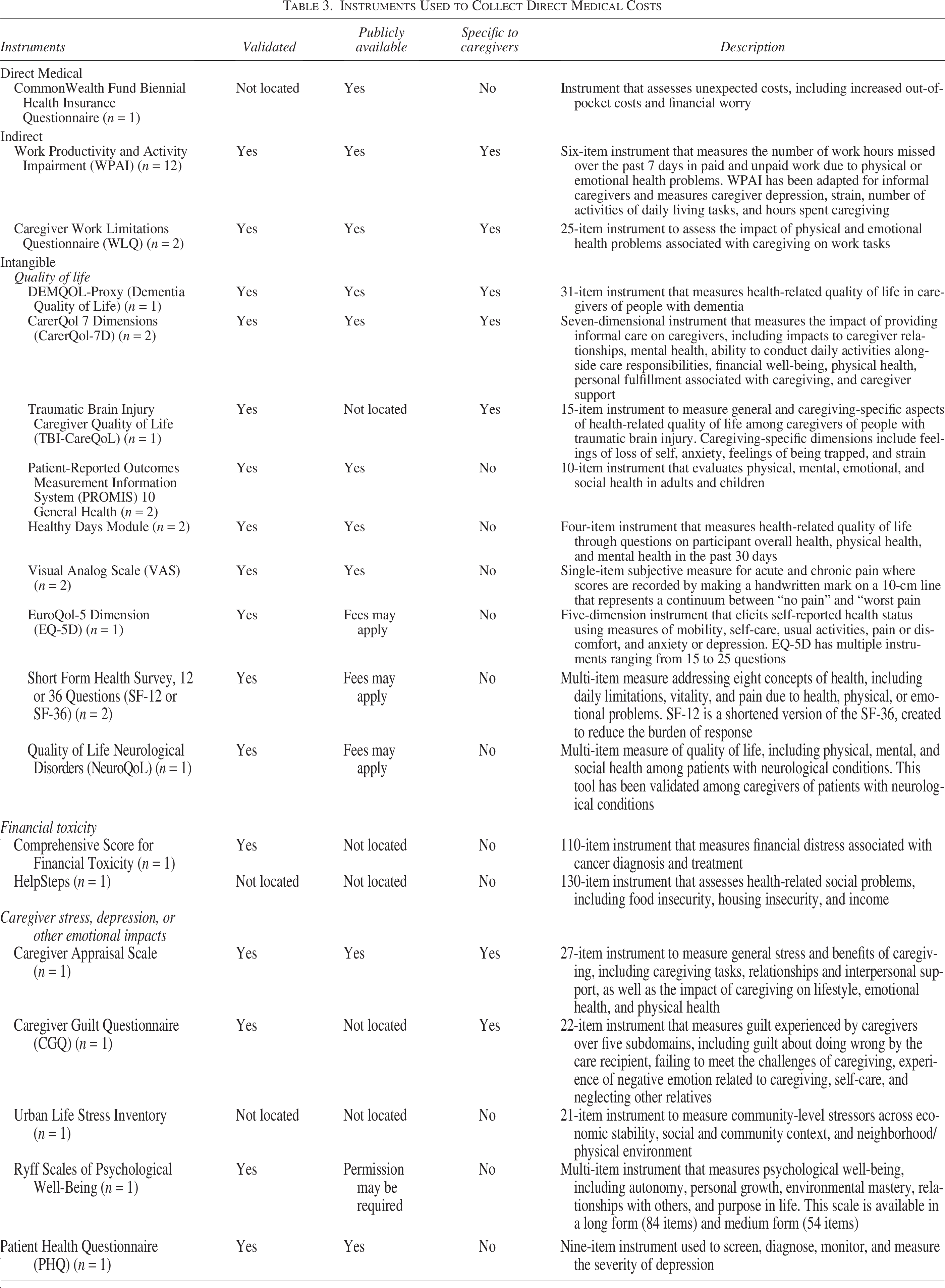
Studies measuring indirect impacts from providing caregiving services (n = 14) used two existing instruments: the Work Productivity and Activity Impairment (WPAI) survey and Caregiver Work Limitations Questionnaire (WLQ; Table 3). WPAI was the most frequently used instrument (n = 12 studies) across studies measuring indirect impacts in this review; only two studies used WLQ. Both the WPAI and WLQ, which measure the impact of caregiving on productivity and impacts to work, are publicly available and validated. Notably, WPAI is a shorter measure of work impairment with 6 items, whereas WLQ is a 25-item instrument, which may have contributed to WPAI’s popularity.
Studies measuring intangible burdens (n = 21) employed 16 unique instruments that focused on 3 unique categories of intangible burdens: quality-of-life, emotional impacts, and financial toxicity (Table 3). Nine instruments measured caregiver quality of life. While three of the quality-of-life instruments specifically address caregiving populations, six were designed for general or patient populations but were administered to the caregiver populations. All quality-of-life instruments were validated in the peer-reviewed literature, and the majority (n = 5, 56%) are publicly available. Five instruments measured emotional impacts to caregivers, including caregiver depression, stress, and guilt. Only two of these instruments, the Caregiver Appraisal Scale and the Caregiver Guilt Questionnaire, were specifically designed to estimate emotional impacts of caregiving, whereas the remaining three instruments were designed for general or patient populations. An additional two instruments were used to measure financial toxicity among caregivers; however, neither instrument was specifically designed for caregivers.
Multidimensional survey instruments
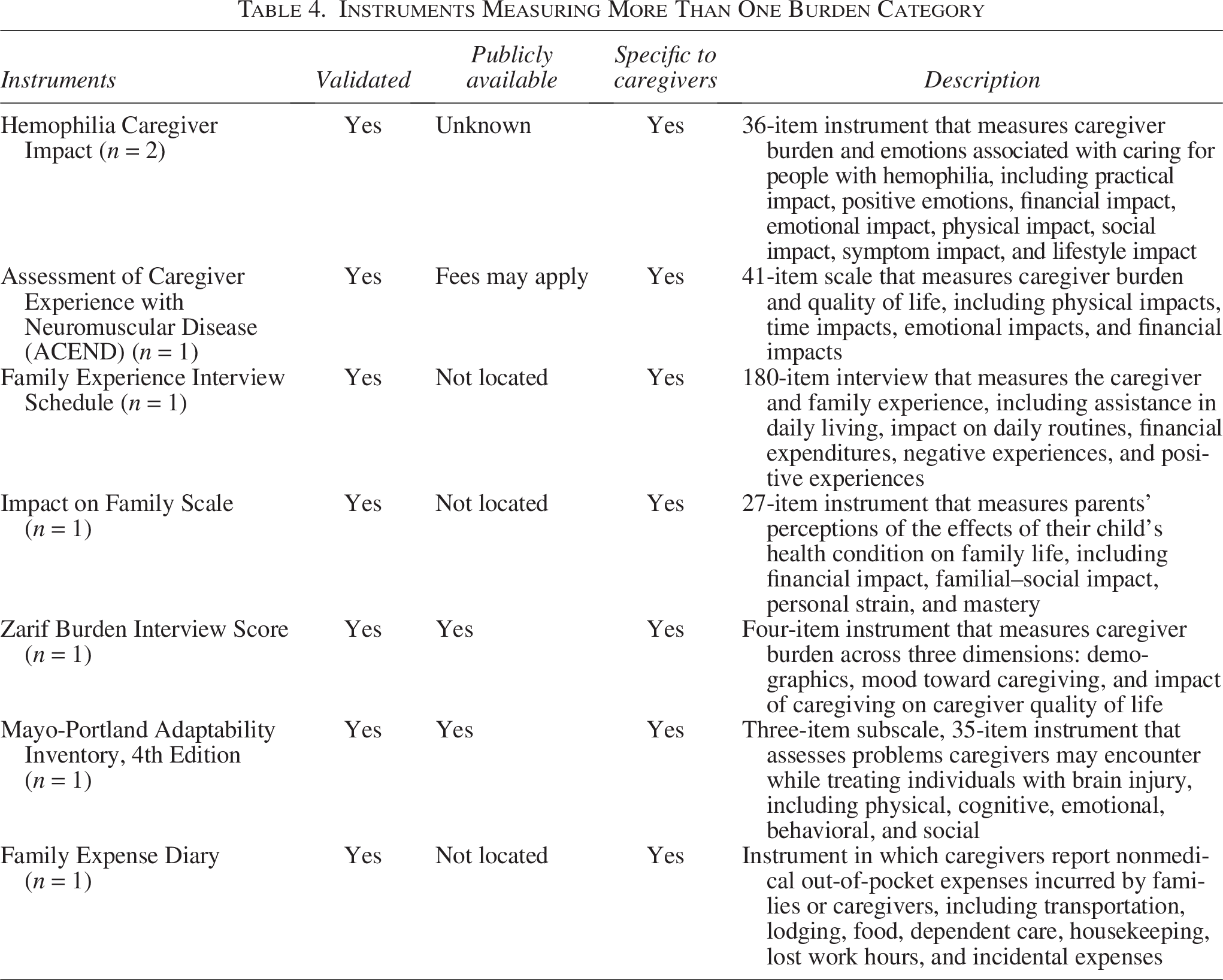
Eight studies (17%) used an instrument that assessed a combination of burden categories (Table 4). Among these, this study identified seven unique instruments that investigated multiple burden categories associated with the costs of caregiving, including emotional, physical, financial, and quality-of-life impacts. The Hemophilia Caregiver Impact instrument was the only instrument used by two studies to assess caregiving burden, whereas the rest were employed by one study each. Dimensions assessed by the various instruments include emotional, physical, financial, social, and cognitive burdens. Although all instruments were validated, only two of them were confirmed to be available publicly. The length of these instruments varied substantially, from 4-item measures (the Zarit Burden Interview score) to the 180-item Family Experience Interview Schedule.
Instruments Measuring More Than One Burden Category
Other, not stated instruments
Over 30% of studies used researcher-designed questionnaires (n = 18) to explore burdens associated with caregiving; most of these studies used researcher-designed questions in collaboration with an established survey instrument (n = 12, 67%). Although some studies indicated that they conducted internal validation on the researcher-designed questions, many did not specify validation efforts for the researcher-designed questions. Example questions included free responses such as “costs of hepatocyte transplantation,” 43 as well as yes/no questions, such as “has your child ever been evaluated or re-evaluated for special education services.” 21
Nonsurvey data sources
Thirteen studies (28%) collected data from nonsurvey data sources (see Table 5). The nonsurvey data sources captured direct medical, direct nonmedical, and indirect impacts but did not include data for intangible burdens. The most commonly used nonsurvey data source was medical claims databases (n = 5). All five studies using claims data accessed the data from employer-sponsored repositories, including Merative MarketScan data and OptumHealth Care Solutions. In four of the studies, researchers linked claims data to integrated employer databases with information on employee absences, income, and disability payments. These studies identified patient–caregiver pairs using the primary plan holder identifier in the data and assumed the primary plan holder was a caregiver to the patient. Researchers then used information on the primary plan holders’ workplace absences and disability pay to estimate caregiver absences. One study also used historical income data to estimate the lost income progression of caregivers associated with their caregiving duties.
Additional Data Sources Used for Assessing Caregiver Burdens
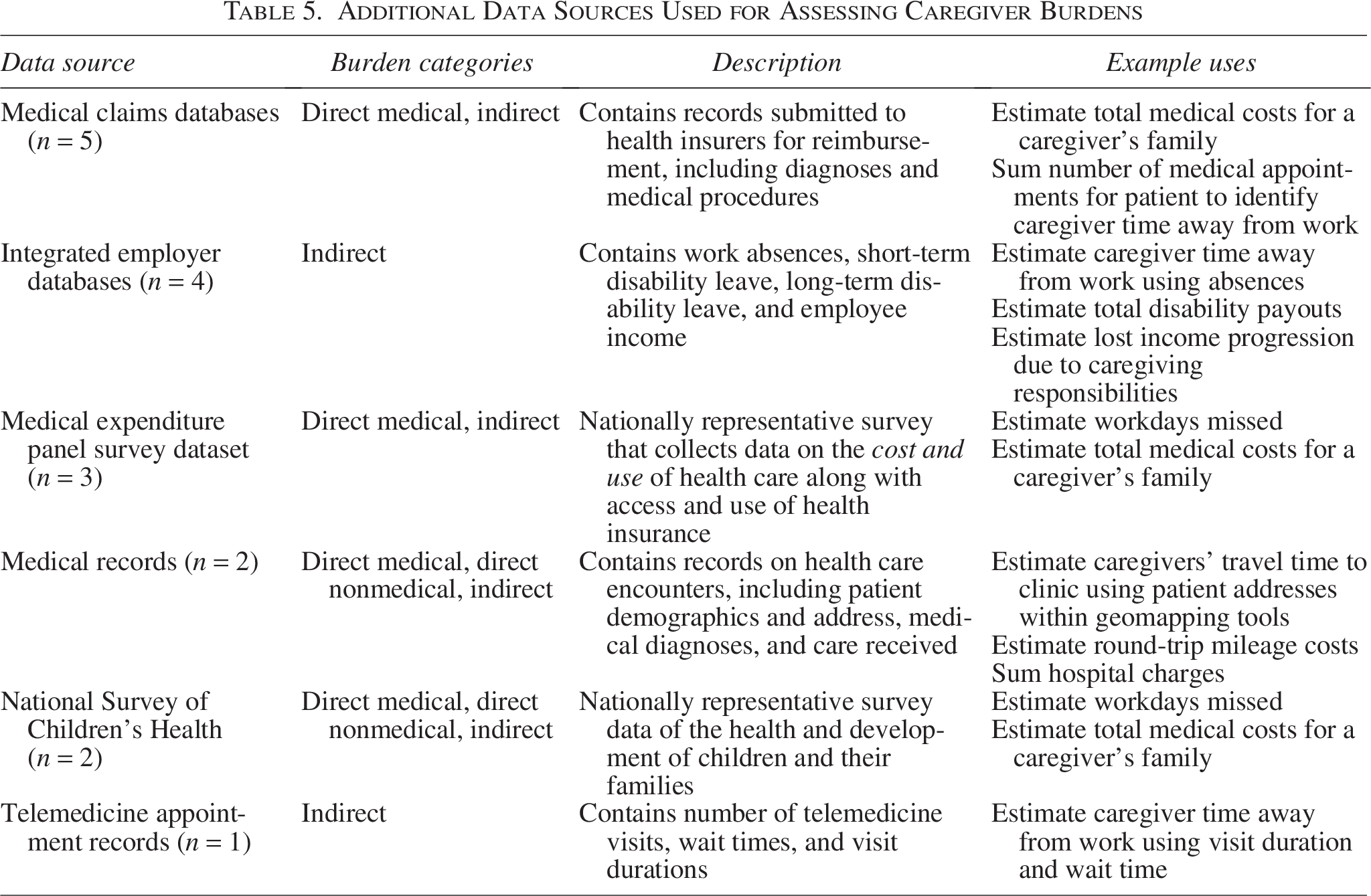
Five studies (11%) used data from two nationally representative survey: Medical Expenditure Survey (MEPS) and National Survey of Children’s Health (NSCH) to estimate direct medical, direct nonmedical, and indirect burdens to caregivers. Three studies analyzed data from the MEPS, a nationally representative, publicly available dataset sponsored by the Agency for Healthcare Research and Quality. MEPS collects data on families’ health care utilization and costs. Two studies analyzed data from NSCH, sponsored by the Health Resources and Services Administration. NSCH is publicly available and collects information related to the health and well-being of children, including access to and use of health care, family interactions, parental health, school and after-school experiences, and neighborhood characteristics.
Three studies used medical records and telemedicine appointment records to estimate indirect impacts to caregivers. Two studies extracted patient home addresses from medical records and used these addresses to estimate caregiver travel time for clinic visits using geomapping tools. One study used telemedicine appointment records to identify the amount of time a caregiver may have spent away from work for the appointment.
Discussion
This study identified 46 studies that estimated direct medical, direct nonmedical, indirect, and intangible burdens among caregivers. To the authors’ knowledge, this study is the first review to identify survey instruments that measure unpaid caregiver burden. This study identified 27 survey instruments and 6 nonsurvey data sources that were used in the literature to quantitatively estimate caregiver burden.
Most of the survey instruments in this review were validated in the peer-reviewed literature. However, only half of the instruments were publicly available and approximately one third of the studies in this review developed their own questionnaires. The cost and application process barriers to accessing validated instruments may lead researchers to design their own research questions. Use of researcher-designed questionnaires can hinder comparability across studies, as each set of questions may be unique. The validation of the researcher-designed questionnaires also varied, with several studies not reporting their validation approaches. Validation ensures that the instruments have face and content validity for their target populations and adequately capture what the instrument is intending to measure. Without validation, instruments may produce unreliable data that limit the generalizability of results.
Use of existing instruments varied by burden category, with direct medical cost studies being least likely to use existing survey instruments. Of the 23 identified studies estimating direct medical costs, most (n = 22, 96%) did not report using a survey instrument, opting to design their own questionnaire (44%) or use secondary data sources (26%) or did not report the instrument (26%). Although secondary data sources, such as medical claims and medical records, were used in some studies to approximate caregiver direct medical costs, these data sources may not be accessible to all researchers due to their high cost, restricted access, and use requirements. Further, these claims data covered only a subset of individuals with employer-sponsored private health insurance and thereby may not be representative of the caregiving population. For example, these databases would be unable to detect caregiving for elderly patients covered by Medicare. These studies also assumed that the policy holder was a caregiver to the patient and were unable to account for other paid or unpaid caregivers on the policy. Given that claims databases were more frequently used to estimate direct medical costs than survey instruments, these limitations could lead to misestimation of caregiver direct medical costs. Studies also used publicly available MEPS and NSCH data to assess direct medical and direct nonmedical costs; however, these datasets may not provide sufficient sample sizes for certain patient populations.
The variation in questions across survey instruments and infrequent use of each survey instrument may also limit comparability across studies. Only one instrument, the WPAI, was used in more than two studies. Further, burden definitions may vary across instruments, which complicate any summarization or meta-analyses of caregiver burdens. For example, nine different instruments measured health-related quality of life. In addition, only half of studies used an instrument designed specifically for caregivers. The burdens caregivers experience may differ from patient experiences, and instruments used in the caregiver population should also be designed to capture their needs and experiences. Using a patient-centered instrument could omit key caregiver-only categories, such as funeral costs and respite care.
Further, although studies estimated indirect impacts more frequently than other burden categories, the instruments used had a narrow scope. For example, WPAI estimates only missed workdays, so this instrument does not capture other indirect subcategories, such as travel time and lost leisure time. Although some of the indirect burdens may have been captured in multidimensional instruments, these multidimensional instruments were used by only eight studies.
Implications for future research
This study identified the instruments and other data sources used to collect caregiver burdens, along with gaps that could provide a starting point for further investigation. The authors recommend several areas for future research.
First, given that only half of studies used an instrument designed for caregivers, future work should (1) explore whether existing instruments for patients can be validated within a caregiver population and (2) identify any barriers to using these instruments among caregivers. This review found several instances where an instrument specifically designed for one medical condition was adapted to another condition or an instrument designed for a patient population was adapted to a caregiver population. For example, Schwartz et al. adapted the Hemophilia Caregiver Impact instrument to measure quality of life among caregivers of patients with Duchenne muscular dystrophy. 23 Future work should also explore whether existing patient instruments or disease-specific instruments could be adapted to a caregiver population.
Second, prior meta-analyses of caregiver burdens highlight wide variation in the instruments researchers use, within and across diseases. 15 Most studies in this review employed unique instruments used by only one study, which complicates the interpretation and comparison of caregiver burdens across studies. Further, approximately 30% (n = 18) of the studies in this review used questions designed by researchers rather than existing questionnaires. The range of instruments used to measure caregiver burdens may be one of the major drivers of high variation in estimates of caregiver costs; each study is capturing a unique variant of the caregiver experience. To facilitate comparisons across measures of caregiver burdens, future research should consider an in-depth analysis of existing caregiver instruments to assess comparability of question domains across instruments and evaluate the appropriateness of each tool for evaluating caregiver burdens. Further, evaluations of caregiver support initiatives often use different instruments to measure caregiver burden, which also hinders comparability of results across evaluation efforts.69,70 Understanding which instruments are most appropriate for measuring the caregiver burdens is important for identifying support types that most meaningfully alleviate caregiver burden and for tailoring these programs to the diverse needs of caregivers.
In addition to assessing comparability of tools, future work should also consider developing standards for collecting caregiver burdens. Standards have been established for other areas of patient-centered and health economics research, such as the Panel on Cost-Effectiveness in Health and Medicine. 71 However, work to establish standards for caregiver burdens would first need to harmonize the definition of each burden, as prior research has found substantial variation in how caregiver burdens are defined.15,20
Third, it was unclear if the use of researcher-developed questions was driven by need for flexible questions, barriers to access and use of existing instruments (eg, cost or length), unawareness of existing instruments, or another reason. Future research should consider identifying the rationale for use of researcher-developed questions because this could identify avenues to improve uptake of existing instruments.
Limitations
This study had several limitations. The authors based the search strategy on Schmidt et al. 17 which did not include search terms for intangible burdens. This may have led to incomplete assessment of intangible survey instruments and data sources. Schmidt et al. 17 also excluded cost estimates for economic analyses, and this review thereby does not include instruments and data sources potentially used in cost-of-illness studies estimating costs of unpaid caregiving.
Among the included studies, not all studies directly stated the survey instruments used and the populations taking the surveys. For example, the authors were unable to distinguish between studies that administered the patient version of WPAI versus those that administered the caregiver version of WPAI. In addition, for studies that surveyed caregivers and patients, the population on which the survey instruments were used was not always clear. This study cautiously included the instrument when the surveyed population was unclear, and the results may include some instruments focused on only patient burdens.
Consistent with guidelines for scoping reviews, this study did not conduct a formal assessment of quality for the studies or survey instruments identified in the review. Thus, the results cannot draw conclusions about the strength of the body of evidence or quality of the survey instruments. To increase the applicability of findings, this study limited the review to studies published in English from the United States.
Conclusions
Unpaid caregivers incur significant financial and nonfinancial burdens attributable to their caregiving duties. Given the increasing need for unpaid and family caregivers, it is imperative to understand the daily burdens these individuals face. However, the large number of instruments used to measure caregiver burdens may limit the ability to compare estimates of caregiver burden across studies. Continued assessments of existing instruments and identifying avenues to harmonize burden measures are critical to improving the outcomes and experiences of those patients and their caregivers.
Authors’ Contributions
D.P.: Writing—original draft (lead), writing—review and editing (equal), conceptualization (equal), formal analysis (lead), and methodology (lead). K.G.: Writing—review and editing (equal), funding acquisition (equal), conceptualization (equal), and writing (supporting). E.S.: Writing—original draft (supporting), formal analysis (supporting), investigation (supporting), and writing—review and editing (supporting). Z.T.: Formal analysis (supporting) and investigation (supporting). M.D.: Formal analysis (supporting) and investigation (supporting). O.K.: Writing—review and editing (equal), conceptualization (equal), and funding acquisition (equal).
Footnotes
Acknowledgments
The authors would like to acknowledge the editorial support for this article by Margaret Johnson from RTI International and acknowledge the help of Theresa Schmidt, who provided the review team with a list of citations from her review, Expanding the Catalog of Out-of-Pocket Costs.
Author Disclosure Statement
The authors did not have any conflicts of interest.
Funding Information
This literature review was supported by Patient-Centered Outcomes Research Institute (PCORI).
Disclaimer
All statements, findings, and conclusions presented in this publication are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute® (PCORI®). This publication was developed from materials originally created through a PCORI® contract [IDIQ-TO#05-RTI-ENG-AOSEPP-09-20-2021] to support PCORI’s work. Questions or comments may be sent to PCORI at info@pcori.org.
Appendix
Selection Criteria
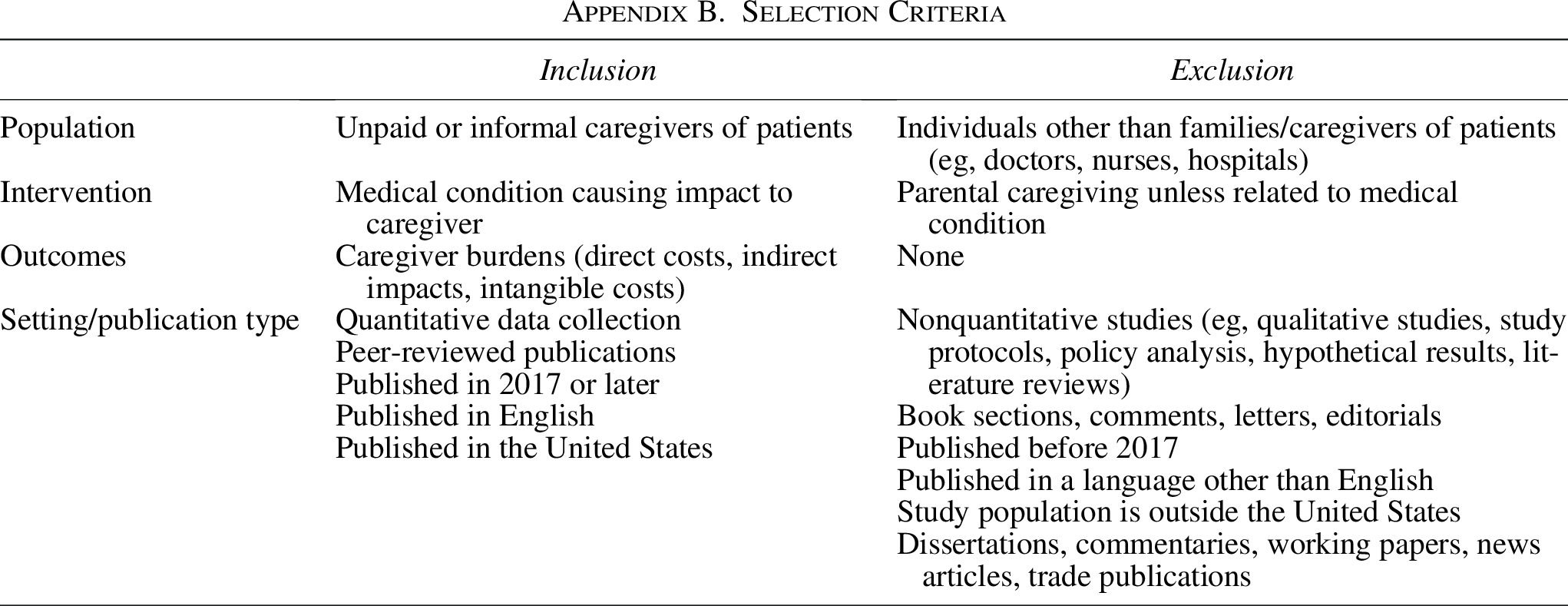
| Inclusion | Exclusion | |
|---|---|---|
| Population | Unpaid or informal caregivers of patients | Individuals other than families/caregivers of patients (eg, doctors, nurses, hospitals) |
| Intervention | Medical condition causing impact to caregiver | Parental caregiving unless related to medical condition |
| Outcomes | Caregiver burdens (direct costs, indirect impacts, intangible costs) | None |
| Setting/publication type | Quantitative data collection Peer-reviewed publications Published in 2017 or later Published in English Published in the United States |
Nonquantitative studies (eg, qualitative studies, study protocols, policy analysis, hypothetical results, literature reviews) Book sections, comments, letters, editorials Published before 2017 Published in a language other than English Study population is outside the United States Dissertations, commentaries, working papers, news articles, trade publications |