
Abstract
As utilization of home care increases across Canada, questions are emerging concerning the extent to which home care expenses, many of which are not publicly covered, are borne by unpaid caregivers of home care recipients. In this systematic review, we review English-language literature published between 2001 and 2022 exploring the magnitude and sources of home care costs incurred by unpaid caregivers in Canada. Of particular interest were empirical, cost-of-illness studies that describe the implications of these costs across domains of financial risk, including caregivers’ income level, employment status, and personal health. Following the screening of 492 studies derived across 6 databases (OVID Medline, CINAHL, PsycINFO, AMED, EconLit, and EMBASE), 24 studies were included in this review. Overall, few studies describe how home care expenses incurred by unpaid caregivers contribute to their financial risk. While some studies characterize the direct costs of caregiving incurred by caregivers, including out-of-pocket expenditure on transportation to medical appointments, respite care, home renovations, supplemental housekeeping, and prescription medications, limited studies attempt to estimate the magnitude of these expenses. Concerning financial risk, the literature is chiefly concerned with indirect costs of caregiving, including consequences on caregivers’ employment (foregone wages). Findings from this literature review suggest further work is needed in Canadian context to document costs associated with unpaid home care provision.
Introduction
In this systematic review, we explore what is known about the magnitude and sources of care-related costs incurred by unpaid caregivers of persons receiving home care in Canada. Similar to facility-based care (eg, care delivered in nursing homes and long-term care home), home care, which is delivered in the community in either individuals’ homes or residential settings (eg, retirement homes), encompasses both formal health care and supportive care. Specifically, home health care includes the provision of upstream services, including nursing care (eg, wound dressing changes, preparing medications, or ventilator use), allied health care (eg, physiotherapy or occupational therapy), and palliative or end-of-life care. Supportive care delivered at home includes downstream services that aid home care recipients in their activities of daily living (eg, bathing, dressing, toileting, feeding), or instrumental activities of daily living (eg, banking, transportation, medication management, use of technology). 1 Collectively, home care may be provided on a long-term basis to individuals with chronic conditions, age-related decline (eg, frailty or dementia), or long-term disability/injury, as well as on a short-term basis for those recovering from an acute medical condition or surgery.
The upstream services that constitute home care are principally provided by formal (paid) healthcare workers. Downstream services may also be provided by paid home care workers such as personal support workers (PSWs) or home health aides; however, in the absence of such support, unpaid caregivers play an important role in the provision of downstream services. An unpaid caregiver (also known as care partner or carer depending on context and preference), may be a family member, friend or neighbor of someone who requires short- or long-term support in due to a health condition, medical procedure, injury, disability, or frailty due to aging.
In Canada, 96% of persons receiving care at home have an unpaid caregiver. 2 The significant role of unpaid caregivers in the provision of home care is, in part, the result of gaps in the availability of publicly funded home care workers who perform downstream care activities. Findings from the 2021 Canadian Community Health Survey (CCHS) show that, of the 6% of all households reporting receipt of home care, almost half (419,800 households) reported needing support from a formal home care worker but not receiving it. 3
Although provincial and territorial health insurance plans subsidize the provision of upstream services when deemed medically necessary per the Canada Health Act, home care is considered an “extended health care service.” 4 Accordingly, there is no obligation for provincial or territorial governments, which are responsible for the delivery of publicly funded health services through Canada’s system of universal health coverage (Medicare), to provide and pay for non-medically necessary home care, including the provision of downstream services. This implicates unpaid caregivers, who may serve as proxy health care decision-makers for their care recipient(s) and, accordingly, may accept responsibility for home care-related expenses. 4
Medicare has been seen as an important policy lever to promote equitable access to healthcare irrespective of individuals’ ability to pay. Accordingly, there are calls to expand public health coverage to include home care. 5 A comprehensive understanding of the costs unpaid caregivers incur in the provision of home care may better inform policy decisions around expanding coverage. To understand the costs incurred by unpaid caregivers, we may be able to turn to cost-of-illness (COI) studies. COI studies aim to identify and measure the costs, including direct and indirect costs, associated with a condition (or set of conditions) or age-related changes, including frailty and limitations in activities of daily living. 6 For this reason, COI studies are particularly useful tools for decision-making when considering public coverage of various health and medical care costs. Historically, published COI studies have demonstrated a bias toward direct medical and other health care costs due to enduring, biomedical conceptions of disease and illness that have long-influenced health economic research around the world. 7 As a result, these studies do not consider non-medical, personal care costs, such as the costs associated with unpaid caregiving.
COI studies that ignore the various costs caregivers incur on behalf of their care recipient could lead to an underestimation of the full economic and social impact of a specific health issue. This is particularly true of health issues that limit the personal autonomy of those afflicted, for example, persons living with Alzheimer’s disease or a related dementia. We know that these individuals may rely significantly on unpaid caregivers for support in activities of daily living, who may, in turn, incur costs associated with this supportive care. 4
Thus, in this systematic review, we assess how published literature characterizes the magnitude and sources of care-related costs incurred by unpaid caregivers of persons receiving home care in Canada. Additionally, we focus specifically on studies that describe the impact of these costs across various domains of financial risk, including caregivers’ income-generating potential, employment status, and personal health. A more fulsome understanding of both the costs of unpaid caregiving and how they are contributing to caregivers’ financial risk will better inform policy decisions around public coverage of the costs of caregiving, as well as strategies to offset the associated risks.
Methods
Conducted in Fall of 2022 by 2 researchers (HM and AP) at the University of Toronto, this systematic review follows the Cochrane Collaboration’s stepwise approach to conducting systematic reviews: (1) defining a question; (2) searching for relevant data; (3) extracting of relevant data; (4) assessing the quality and relevance of the data; and (5) analyzing and combining the data. 8
A concept table was developed based on the PICo (population, interest, context) framework for descriptive syntheses to operationalize the research question into searchable keywords, 9 including unpaid caregivers (the population), direct costs and indirect costs (the interests), and home care and Canada (the contexts).
For the purpose of this review, we focus on Canadian literature. Under Canada’s publicly funded universal healthcare system, Medicare, care delivered outside of hospitals or care that is provided by clinicians other than doctors, may not be covered. As such, where caregiving takes place, including in the home and residential long-term care or nursing homes, few services are publicly insured. Accordingly, there is reason to believe that unpaid caregivers are experiencing several financial challenges associated with caregiving that may be offset through more targeted public programs. Hence, this review serves as a launching point toward a subsequent review that comparatively explores the monetary costs of unpaid caregiving in other welfare states with systems of national health insurance.
As caregiving is a multidisciplinary field of study and this topic could be captured in a range of subject databases, including medicine, health services research, rehabilitation science, economics, and political science, 5 databases were employed in this search: Ovid MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Allied and Complementary Medicine (AMED), EconLit, and EMBASE. MEDLINE and EMBASE collate life sciences and biomedical information; CINAHL collects nursing and allied health literature; PsycINFO collects literature from the social sciences; AMED focuses on alternative medicine and rehabilitation science; and EconLit primarily collects economic literature.
A language (English) restriction was placed on this search, as well as a date restriction (January 2001-August 2022). We imposed a date restriction to ensure findings of this review reflected the heightened policy attention on unpaid caregiving at this time that may have reshaped the conditions under which caregivers operated, including the corresponding financial risks. Specifically, in June of 2000, the Canadian Senate released its landmark report entitled, “Quality End-of-Life Care: The Right of Every Canadian,” which recommended the federal government implement income security and job protection for family members who care for those who are ill or imminently dying. 10 This spurred the launch of a new federal Employment Insurance (EI) benefit in January 2004 called the Compassionate Care Benefit, which, to this day, provides income security for those taking on such caregiving roles. 10 Around this time, large-scale policy reforms also occurred across provinces/territories in an attempt to shift health service provision from acute-based settings to the community (home). Ontario’s largest such reform was the development of regional health organizations in 2006 called Local Health Integration Networks, which were responsible for overseeing the community-based programming—including enhanced caregiver supports—outlined in the new Aging-at-Home Strategy. 11
Boolean operators, truncation and phrase searches were applied to maximize search results and translate search terms for each database. A combination of these keywords/subject headings were used in each database. In Ovid MEDLINE and AMED, keywords were matched to Medical Subject Headings (MeSH). As an example, Appendix A shows the search schema used in Ovid MEDLINE.
Two authors (HM and AP) engaged in the process of screening articles using Covidence, a primary screening and data extraction tool used in the conduct of literature reviews. 12 Two stages of screening were conducted—a title/abstract screening for relevance and a full-text screening. At both stages, articles were excluded based on the following criteria: article was not based in Canada; was not an empirical COI study that presented any research results (eg, article was a commentary, proposal or literature review); the article focused on public health costs only (eg, based on administrative datasets), and the study was not explicitly about patients or caregivers. Articles were also excluded following title/abstract screening if the full-text was unavailable after contacting study authors. Disagreement between screeners concerning articles that should be included was reconciled through a collaborative discussion until consensus was reached.
Using the Quality Assessment Tool for Studies with Diverse Designs (QATSDD), 13 authors (HM and AP) independently conducted a quality assessment of all research articles included in this review, resolving disagreement through discussion. Due to the heterogeneity of study types, statistical analyses (eg, quantitative synthesis or meta-analysis) was not possible. Hence, descriptive synthesis was used to summarize the categories of costs identified in these papers and qualitative thematic analysis was used to describe the impacts across domains of financial risk, including income, employment and overall health. 14 Descriptive synthesis (whether numeric or thematic) enables readers to survey the pattern of characteristics found in the studies.15,16
Results
Reporting of the database search follow recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on reporting systematic reviews. 16 Appendix B shows the PRISMA flow diagram for article selection. In total, 492 articles were yielded from all databases. Of those, 193 studies were excluded because they were screened by Covidence as duplicates. Of the remainder (n = 299), a further 247 were excluded following a title/abstract screening, rendering a total of 52 articles for full-text screening. After full-text screening, 28 studies were excluded yielding 24 for analysis. Following quality assessment by authors (HM and AP), no additional articles were excluded from this review.
Summarized in Appendix C, the 24 included articles represent a mix of quantitative studies (eg, analyses of self-reported surveys and questionnaires [n = 13], secondary analyses of national datasets [n = 3], a randomized control trial [n = 1], and a longitudinal, microsimulation model [n=1]), and qualitative studies (eg, analyses of semi-structured interviews or focus groups [n = 5] and a document review [n = 1]). Studies were conducted across Canada, or within specific provinces, namely Ontario, British Columbia or Alberta. Studies largely focused on costs incurred by patient and caregiver dyads, with few studies focusing specifically on caregivers. Studies focus on different conditions, with a great emphasis on Alzheimer’s Disease and related dementias.
Descriptive Synthesis of Sources and Magnitude of Care-related Costs
Specific elements were extracted from included articles to be consistent with the research aims to (1) characterize the costs associated with unpaid care provision; and (2) understand how expenditure associated with caregiving impacts unpaid caregivers across domains of financial risk. Table 1 summarizes cost categories and specific estimates (where applicable) derived from empirical investigation. For the purpose of this table, the terms and labels used to categorize costs is based on the language used in the articles. Only 2 articles17,18 do not identify cost categories, but present aggregate cost expenditure associated with caregiving among unpaid caregivers, which we discuss further below.
Categories and Estimates of Care-Related Costs.
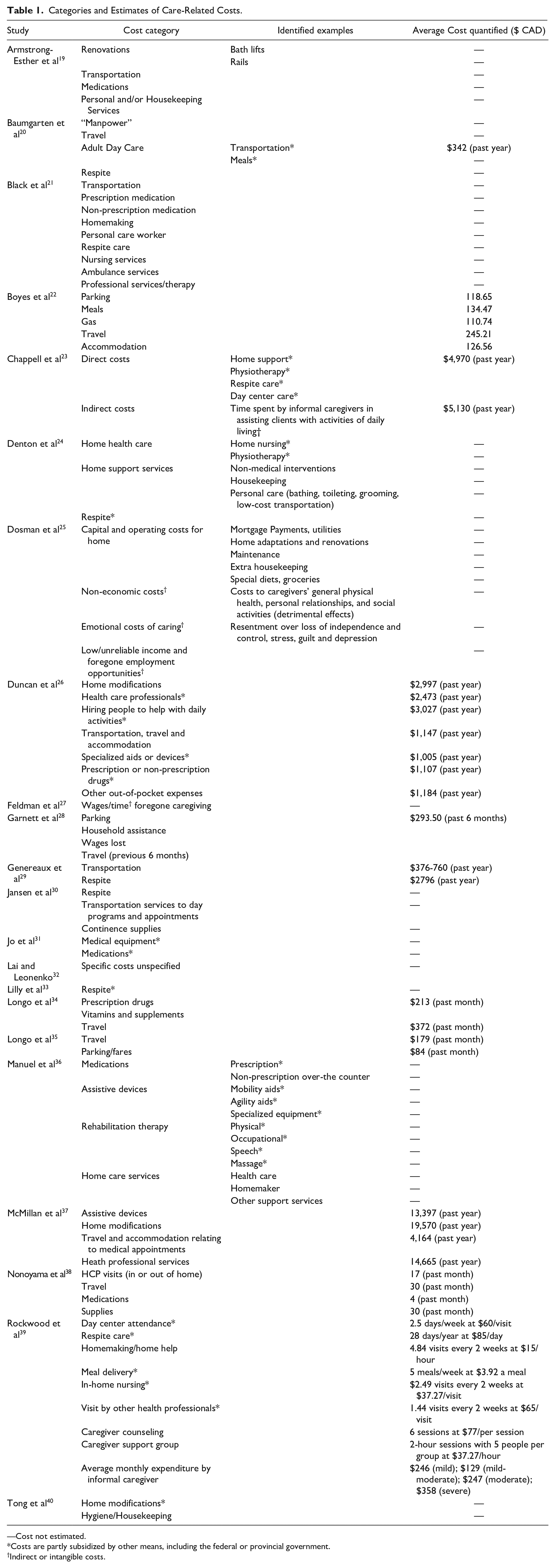
—Cost not estimated.
Costs are partly subsidized by other means, including the federal or provincial government.
Indirect or intangible costs.
Average estimates are derived from the previous month, 6 months, or year. Costs ending with (*) are those that are partly subsidized by other means, including the federal or provincial government (eg, through Medicare) or credits/grants. Costs ending with (†) refer to indirect or intangible costs. Where costs are reported, several studies do not distinguish which costs are specifically or wholly incurred by caregivers versus care recipients/patients.35,37 Further, some studies report aggregate estimates of total private (out-of-pocket) expenditure across multiple cost categories.23,28,34
In summary, the most commonly noted cost categories were respite, extra housekeeping, transportation, home renovations and/or modification, and time spent caregiving/forgone wage†. Less frequently mentioned, but noteworthy, categories of costs include adult day care, rehabilitation (physiotherapy), and assistive devices.
Financial Risk: Key Themes
The literature presents a number of themes concerning how the costs of caregiving impact caregivers, which are summarized as follows.
Theme 1: Unpaid caregiving costs are the largest component of care costs
Unpaid caregiving costs accounted for the largest portion of direct care costs. For example, in the context of palliative care at home, private (out-of-pocket) care expenditure accounted for 76.7% of total care costs, with publicly subsidized care associated with 21% of direct costs on average. 17 Highest expenditures were on costs related to transportation (travel) to medical facilities 20 and both prescription and non-prescription medication, 21 as well as accommodation during long stays in hospital. 22
In addition to out-of-pocket care expenditure, several studies noted significant indirect costs associated with caregiving, including imputed value of caregivers’ unpaid labor, or time spent caregiving. Time spent caregiving was a major indirect cost for caregivers taking care of persons with intellectual disabilities, 29 those on mechanical ventilators, 38 and octogenarians in intensive care units. 22
Theme 2: Caregiver and caregiving characteristics may predict extent of care-related costs
Three characteristics of caregivers and the nature of caregivers’ care activities may predict care-related costs. First, specific caregiver groups experience high indirect costs through lost wages from taking time off work, including (1) caregivers who provide assistance with activities of daily living (ADLs) for care recipients in an advanced stage of a condition (eg, dementia or intellectual disability); (2) caregivers who provide end-of-life (EOL) care; and (3) caregivers who provide palliative care.17,18,29,32,36,39 Second, caregivers with higher household incomes and/or those working full-time reported being able to afford expenses associated with caregiving. Authors note that is because they were likely to have financial resources to alleviate the financial challenges associated with caregiving.18,32 By contrast, greater cost burdens were experienced among caregivers who had to take time off work. 34 Although not explicitly attributable to the costs of caregiving, caregivers who reported a high household income were more likely to be willing to miss full days of work while caregiving. However, caregivers residing in middle-income households were more likely to quit their job. 18 Lastly, one study observed gender-related patterns in the direct costs of caregiving (out-of-pocket care expenditure), with men caregivers reporting out-of-pocket costs that were 1.93 times higher than those of women caregivers. 22
Theme 3: Forgone employment income makes paying for care-related expenses more challenging
For working caregivers, the indirect costs associated with time spent caregiving (unpaid labor) may be framed as lost or forgone employment income attributable to caregiving, which is projected to increase over time as unpaid caregivers take on greater homecare responsibilities.25,36Although foregone income depends on illness severity, with some caregivers reporting less time off work for care recipients who’s illness was less severe, the majority of caregivers (over 50%) reported high average monthly forgone income (lost wages), including $4860 (CAD) in caring for octogenarians in intensive care, 22 $2000 in caring for older adults at home, 32 and $700 34 and $2402 35 in the context of cancer caregiving. Lost wages, an indirect cost of caregiving, exacerbated the perceived financial burden of direct care costs (namely out-of-pocket caregiving expenditure). In other words, deficits in employment income made it challenging to pay for care-related expenses.18,22,34
Caregivers also modified their employment to better manage caregiving responsibilities, including quitting work, changing jobs, taking an unpaid or paid leave of absence, and modifying work hours.18,21,26,37,32 These modifications were common among caregivers taking care of someone at end-of-life or advanced in their illness (eg, dementia) trajectory.18,21
Theme 4: Paying for caregivers’ own health-related expenses is challenging due to the costs attributable to caregiving borne by caregivers
Across studies, the direct, private (out-of-pocket) costs of medical equipment and prescription medication were difficult to cope with compromised physical and mental well-being.21,31 While few studies explicitly describe the health-related impacts associated with caregiving expenditure, one study notes that 65.2% of caregivers reported some degree of anxiety or depression due to their caregiving responsibilities, with 31.1% consequently having to pay for medication for these care-related mental health challenges, 45.7% seeking respite for their exhaustion, and 45.7% paying for physiotherapy for an injury related to caregiving (eg, lifting or transferring their care recipient). 37 In the context of caregiving for someone living with dementia, while the cost of medication was a significant expense, it reduced hospitalizations likely related to the role of being a caregiver and lowered the time spent caregiving overall relative to those whose care recipients were not on any medication for dementia. 27
Caregiver respite—or time off from caregiving during which time a care recipient is either being taken care of by a PSW or at an adult day-program—is particularly important in preserving overall health and well-being of caregivers given the stressors associated with full-time caregiving. 18 Articles point to the need for improved subsidies for unpaid caregiver respite. For example, one study notes that respite was prohibitive for unpaid caregivers of persons living with dementia as these caregivers are often older, retired spouses who have a fixed income. 33 Challenges paying for respite were exacerbated due to caps on the number of days per week caregivers could access subsidized respite. This study also notes that there is still a clinical/medical orientation toward unpaid caregiver protection. 33 In the Canadian context, caregivers can only access services when they are at an immediate risk of becoming patients themselves. Authors suggest rather than offering costly care for these individuals after they have become patients of the health system, these caregivers should be viewed as a valuable health human resource, and should have access to services before they need to ask.
Theme 5: Access to public (government) support to offset financial insecurities varies
Unpaid caregivers experienced difficulties coping with care costs. Estimates of the proportion of unpaid caregivers who experienced financial insecurity as a result of the direct costs of caring vary, though there is agreement that these challenges need to be offset by greater public support. One study estimates that 20% of unpaid caregivers desire better financial protection, for example, through an attendance allowance, a mandated leave of absence from work, or paid leave of absence from work. 19 While financial risk protection schemes exist across Canada (eg, the Canada Caregiver Credit and employment insurance-based care benefits), these schemes target younger, working caregivers, thereby excluding a sizable majority of unpaid caregivers, who are often retired spouses. 24 This is consistent with empirical findings showing that retired caregivers were less likely to have access to financial support from government, or to access tax benefits, and that caregivers with a higher household income were better able to access tax benefits for care-related expenses. 18
Authors of one study argue that public support for unpaid caregivers is inadequate. 25 This compromises available financial resources for other important care-related expenses, including transportation, home renovation, and personal respite care, which other articles demonstrate are the largest out-of-pocket expenses categories. For example, transportation costs to day programs and appointments often prevented access to out-of-home services. 30 Further, the costs of implementing safety solutions for homebased persons living with dementia was prohibitive as well. 40 While federal grants, provincial grants (eg, British Columbia’s Home Adaptations for Independence Program) and non-profit organizations (eg, the Red Cross) provide some financial support, it often does not cover the full cost of recommended or required modifications or equipment. Financial support to create safe living conditions at home has the potential to prevent costly injuries, with some studies emphasizing that community and home care services ought to be “medically necessary,” and therefore publicly covered to curtail the growing trend toward the privatization of home care services (eg, purchasing personal and/or housekeeping services).19,39
Discussion
This review reveals a number of direct costs of caregiving, including for prescription medication and travel to and from medical appointments, that caregivers incur out-of-pocket. Caregivers also experienced indirect costs such as lost wages due to caregiving. However, gaps remain in our understanding of the costs of caregiving and how they contribute to financial risk. For example, while some studies report specific cost estimates, the costs are reported as being incurred by both care recipients/patients and their caregivers: the magnitude of expenditure incurred specifically by caregivers is not entirely clear. As well, studies were largely based on specific conditions making it challenging to draw general assessments about the costs of caregiving across the broad population of caregivers. Further, although we see categories of costs described in recent literature, there is still paucity of data estimating the magnitude of expenditure across these categories. Without specific estimates, we cannot make meaningful assessments about if and how these expenses are contributing to financial risk, and accordingly, how public (government) intervention may be able to offset these expenses and corresponding risks. Lastly, only a few studies that estimate how much caregivers are paying out of their own pocket across different cost categories are based on self-reported data. Previous scholarship note this as a limitation of studies that explore the costs of home care: the cost of homebased services is likely underestimated because reliable information on direct, non-medical care expenses is unavailable in publicly administered datasets.20,41 This is also highlighted in previous scoping reviews of literature on out-of-pocket costs in dementia care, which observed deficiencies in accurately calculating the full costs of dementia care on society (including out-of-pocket care expenditure by caregivers).42,43 These deficiencies in data capture undermine the full financial impact of these costs on caregivers, and mask the economic and societal impact at large.
Findings from this review, particularly about the direct, private (out-of-pocket) costs of caregiving are consistent with another literature review exploring global out-of-pocket expenditure in the context of aging at home. 44 This study emphasized the importance of developing standardizing approaches to valuating out-of-pocket spending as a percentage of family income for older adults living at home, which informed the focus on home care in our review. Several studies suggest that that home care is not as cost-effective as policymakers had hoped, as the care and cost burden has effectively been transferred from the system to caregivers themselves, thereby increasing societal costs, defined as direct costs and the imputed value of caregivers’ unpaid labor. 39 Previous scholarship from Québec notes that home care is less expensive than institutional care when only public costs are taken into account, but more expensive when unpaid care costs are considered. 23 This is as a result of unpaid caregivers’ contribution of both their time and out-of-pocket funds. Accordingly, the financial responsibilities imposed on unpaid caregivers should be understood by health care providers, who should, accordingly, be aware of local policies and resources to support caregivers in mitigating out-of-pocket spending associated with homebased care. 23 It has been suggested that implementing a community-based surveillance strategy, such as the Canadian Institute for Health Information Minimum Data-Set for Community Care, is essential to ensure we are fully aware of the outcomes of home care strategies on caregivers. 45 This is particularly relevant today given ongoing investment in strategies that promote aging at home across Canada.11,46
Limitations
This review attempted to explore the costs of unpaid, homebased caregiving in Canada, and their respective impacts across various domains of financial risk. Themes around indirect costs, including lost wages, were discussed if relevant to the impact of the costs of caregiving on domains of financial risk. Accordingly, this study may have excluded articles on financial risk if they did not measure direct costs, and only focused on indirect or opportunity costs. Furthermore, our focus on articles published since 2001 may have compromised the scope of our findings. Lastly, this review focuses narrowly on the Canadian context given the design of its healthcare system which emphasizes public provision. Excluding analyses on the monetary costs of unpaid caregiving across other comparable jurisdictions may compromise the generalizability of our findings, but we do acknowledge a growing body of research from high-income countries on unpaid care costs, including the United States,47,48 and the United Kingdom. 49 We hope in the future to leverage approaches used in this review to conduct a broader review of literature on the costs of unpaid caregiving across comparable jurisdictions.
Conclusion
Findings from this review suggest that the financial risks of caregiving may be significant, but the magnitude of care-related expenditure incurred by caregivers specifically are not wholly quantified or documented. These results provide fodder for future research—both locally and in other jurisdictions where home care utilization is increasing—that explores the magnitude of home care expenditure among unpaid caregivers, and the corresponding impacts across domains of financial risk.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223231169504 – Supplemental material for Unpaid Caregiver Costs in Canada: A Systematic Review
Supplemental material, sj-docx-1-hhc-10.1177_10848223231169504 for Unpaid Caregiver Costs in Canada: A Systematic Review by Husayn Marani and Allie Peckham in Home Health Care Management & Practice
Supplemental Material
sj-docx-2-hhc-10.1177_10848223231169504 – Supplemental material for Unpaid Caregiver Costs in Canada: A Systematic Review
Supplemental material, sj-docx-2-hhc-10.1177_10848223231169504 for Unpaid Caregiver Costs in Canada: A Systematic Review by Husayn Marani and Allie Peckham in Home Health Care Management & Practice
Supplemental Material
sj-docx-3-hhc-10.1177_10848223231169504 – Supplemental material for Unpaid Caregiver Costs in Canada: A Systematic Review
Supplemental material, sj-docx-3-hhc-10.1177_10848223231169504 for Unpaid Caregiver Costs in Canada: A Systematic Review by Husayn Marani and Allie Peckham in Home Health Care Management & Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.