
Abstract
To determine whether pandemic-era Medicaid policies to increase postpartum coverage to 1 year were effective in preventing coverage loss into the second-year postpartum. The analytic sample included 7967 cases (N = 4632 in the pandemic era) from the 2019 and 2021–2024 Current Population Survey, Annual Social and Economic Supplement. On multivariable analysis of the entire sample, era was not associated with the type or continuity of insurance coverage. Among families living below 100% Federal Poverty Level, the relative risk of coverage gaps compared with continuous private coverage decreased by 58% (95% confidence interval: 19%, 79%, P = 0.010). Pandemic-era Medicaid policies appeared effective in preventing postpartum coverage loss in the second year after birth, especially among families living below the poverty line.
Interruptions or changes in health insurance coverage (described as insurance “churn”) disproportionately affect Medicaid beneficiaries, who account for 42% of all United States (US) births.1,2 Although Medicaid has historically provided postpartum coverage through at least 60 days, insurance churn after this period is higher among Medicaid beneficiaries than among postpartum patients with other insurance types. 3 Continuous postpartum insurance coverage can support improved maternal mental health, reduce financial burden associated with childbirth, help manage chronic conditions, and potentially prevent late maternal deaths.4–6 For those not qualifying for continued Medicaid coverage outside pregnancy, insurance coverage can be maintained by options offered by the Affordable Care Act of 2014. However, in 2018, nearly 40% of the patients who had enrolled in Medicaid lost coverage in their first year postpartum, with approximately 31% losing coverage in the first 6 months following birth. 3
In response to the COVID-19 pandemic, the American Rescue Plan Act of 2021 gave states an option to extend Medicaid coverage to 12 months postpartum regardless of prior state action on expanding Medicaid eligibility. This option was originally planned to last for 5 years but has now been made permanent as of 2023. As of July 2024, 46 states and the District of Columbia have extended postpartum coverage to 12 months. 7 Additionally, provisions from the Families First Coronavirus Response Act (FFCRA) in effect over 2020–2023 allowed for continuous Medicaid enrollment during this time and was another mechanism to protect against coverage loss. 8 For individuals receiving the 1-year postpartum Medicaid benefit, coverage does not extend beyond the first year. Early studies on the effects of pandemic-era Medicaid extensions for postpartum coverage found that FFCRA had reduced, but did not eliminate, the loss of health insurance coverage within the first year after birth.9,10 However, providing continuous Medicaid eligibility throughout the first postpartum year may not resolve the underlying risk factors for coverage loss, such as unstable employment. Reductions in coverage loss within the first year postpartum due to these pandemic-era and federal policies may just displace the inevitable risk of losing coverage into the second-year postpartum. While the 1-year Medicaid extension improves access to care for these mothers, the question is whether this is enough to improve maternal health care outcomes if many of these recipients lose access to coverage.
This study used population-based repeated cross-sectional data to test changes in the risk of coverage gaps during the second year after the expiration of the Medicaid postpartum coverage extension. This study hypothesizes that pandemic-era policies would protect against coverage loss during the first postpartum year but lead to a higher likelihood of coverage loss during the second postpartum year, compared with the prepandemic era. Although these policies were intended to protect continuity of care within the first year postpartum, their implementation may have unintentionally delayed coverage loss into the second-year postpartum, potentially increasing the risk of coverage loss in the second postpartum year relative to the prepandemic era. This study postulates that after the pandemic-era policy provisions run out, insurance churn would be greater and coverage would not be sustainable. Individuals who would have initially lost coverage 60 days after birth under prepandemic era policies could now be at risk of losing coverage 12 months after birth under pandemic-era policies. Furthermore, the study hypothesized that the increasing risk of coverage loss during the second year would be most evident among low-income families, which would presumably be most likely to experience delayed loss of Medicaid coverage.
Materials and Methods
This study used deidentified data and did not meet criteria for human subjects’ research. Data from the Current Population Survey, Annual Social and Economic Supplement (CPS-ASEC), a monthly survey sponsored by the U.S. Census Bureau and Bureau of Labor Statistics, were used. 11 The survey collects data regarding employment status, household income, and health insurance coverage from participating households, nationally representing insurance status and other demographic factors. 10 Representative information is acquired by sectioning states into primary sampling units that are then stratified based on the following key variables: number of employed males, number of employed females, number of families with female heads of household, and number of households with three or more people. 12
In the original sample, data were collected from female respondents aged 18–44 years living with a child at least 1 year of age but less than 2 years of age. Data from 2019 represented the prepandemic period, and 2021–2024 data represented the pandemic era. Data from 2018 and earlier were not included because the CPS-ASEC did not ask questions regarding current insurance status at the time of the survey. Data from 2020 were omitted from this study to allow sufficient time for pandemic-era policies to affect respondents’ coverage type. Respondents living with children younger than 1 year were excluded to prevent confounding of study findings by maternal coverage eligibility due to a more recent birth. Additionally, respondents with missing data on any study variables were excluded.
The primary outcome of this study was insurance coverage at the time of the survey and in the 12 months leading up to survey participation. Participants were classified as having continuous private coverage, continuous public coverage (without private coverage), continuous lack of coverage, or a coverage gap in the past year. Private coverage was defined as insurance purchased by an individual or through an employer-sponsored program at the time of the survey and without coverage gaps (defined below). Public coverage was defined as insurance provided by a government agency, including Medicaid and Medicare, or any other government insurance at the time of the survey and without private coverage or coverage gaps. Participants were classified as being continuously uninsured if they reported no health insurance coverage in the past year and no coverage at the time of the survey. Participants were classified as experiencing coverage gaps if they currently had health insurance coverage but did not have coverage for the entire previous year or if they currently did not have health insurance coverage but had coverage for part of the previous year. Participants who could not be classified in this schema were considered to have missing data on insurance coverage and were excluded from the analysis.
The primary independent variable was survey year, which was used to identify respondents who may have been eligible for extended Medicaid coverage under pandemic-era policies. In the primary analysis, survey year was analyzed as a dichotomized measure of prepandemic (2019) versus pandemic era (2021–2024) responses. Because Medicaid eligibility redetermination had been paused during the pandemic (which could have suppressed the risk of coverage loss in the second year after birth), sensitivity analysis was conducted comparing 2019 and 2024 data only. Demographic covariates included respondent age at the time of the survey; race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, or none of the above); marital status (currently married, formerly married, or never married); and employment (currently employed, currently self-employed, or not currently employed). Additionally, controlled variables include US citizenship status (citizen vs. noncitizen) and family income as a ratio of the Federal Poverty Level (FPL; 0%−99%, 100%–149%, or 150% and above). The current study also controlled for the presence of older children within the home, as this could represent experience in obtaining postpartum coverage after prior births. Last, the study controlled for whether a respondent was living in a state that had expanded Medicaid before the calendar year of the survey (Supplementary Table A1). 3 As of 2024, most states had expanded Medicaid, making the focus of the analysis more on the effect of pandemic-era policy transitions on insurance gaps.
Data were summarized as weighted means or proportions with 95% confidence intervals (CI) and compared by era (prepandemic vs. pandemic era) using Wald tests. Weights were used to derive nationally representative estimates from the sample. Results were presented as relative risk ratios (RRRs), expressing the likelihood of having each insurance coverage type relative to the reference category of continuous private insurance. The RRR indicates a multiplicative change in the risk of having continuous public, coverage gaps, or continuous uninsurance rather than having continuous private coverage, associated with a one-unit increase in each independent variable. Comparisons between continuous public versus continuous private, coverage gaps versus continuous private, and continuous uninsured versus continuous private were made to describe possible associations of pandemic-era policies with the use of any insurance, continuity of coverage, and source of coverage. In a secondary analysis, the model was refit to the subsample of respondents with household incomes below 100% FPL, as this group would have been most likely to be eligible for postpartum Medicaid coverage. These analyses were repeated in a sensitivity analysis of a subsample of respondents only from 2019 and 2024. All analyses were adjusted for the survey weights and complex sampling design. Data analysis was completed in Stata/SE 18.0 (College Station, TX: StataCorp, LP), and P < 0.05 was considered statistically significant.
Results
The CPS-ASEC initially included 138,269 female participants aged 18–44 in the 2019 and 2021–2024. 130,247 participants, who did not have a child at least 1 year of age but less than 2 years of age and who had children younger than 1 year, were excluded and 46 had missing data on study variables, leaving 7976 cases for analysis. Based on this sample, 65% (95% CI: 64, 67) of this population had continuous private coverage, 22% (95% CI: 21, 23) had continuous public coverage, 4% (95% CI: 3, 4) experienced part-year uninsurance, and 9% (95% CI: 8, 9) were continuously uninsured. Insurance coverage and study variables are compared by era in Table 1. There was no significant difference between era and insurance status on this bivariate analysis. Compared with the prepandemic era, respondents in the pandemic era were slightly older and more likely to live in a Medicaid-expansion state, which may be related to a larger number of states’ enacting Medicaid expansion in recent years.
Study Outcomes and Characteristics of Patients Age 18–44 Years by Prepandemic Versus Pandemic Era
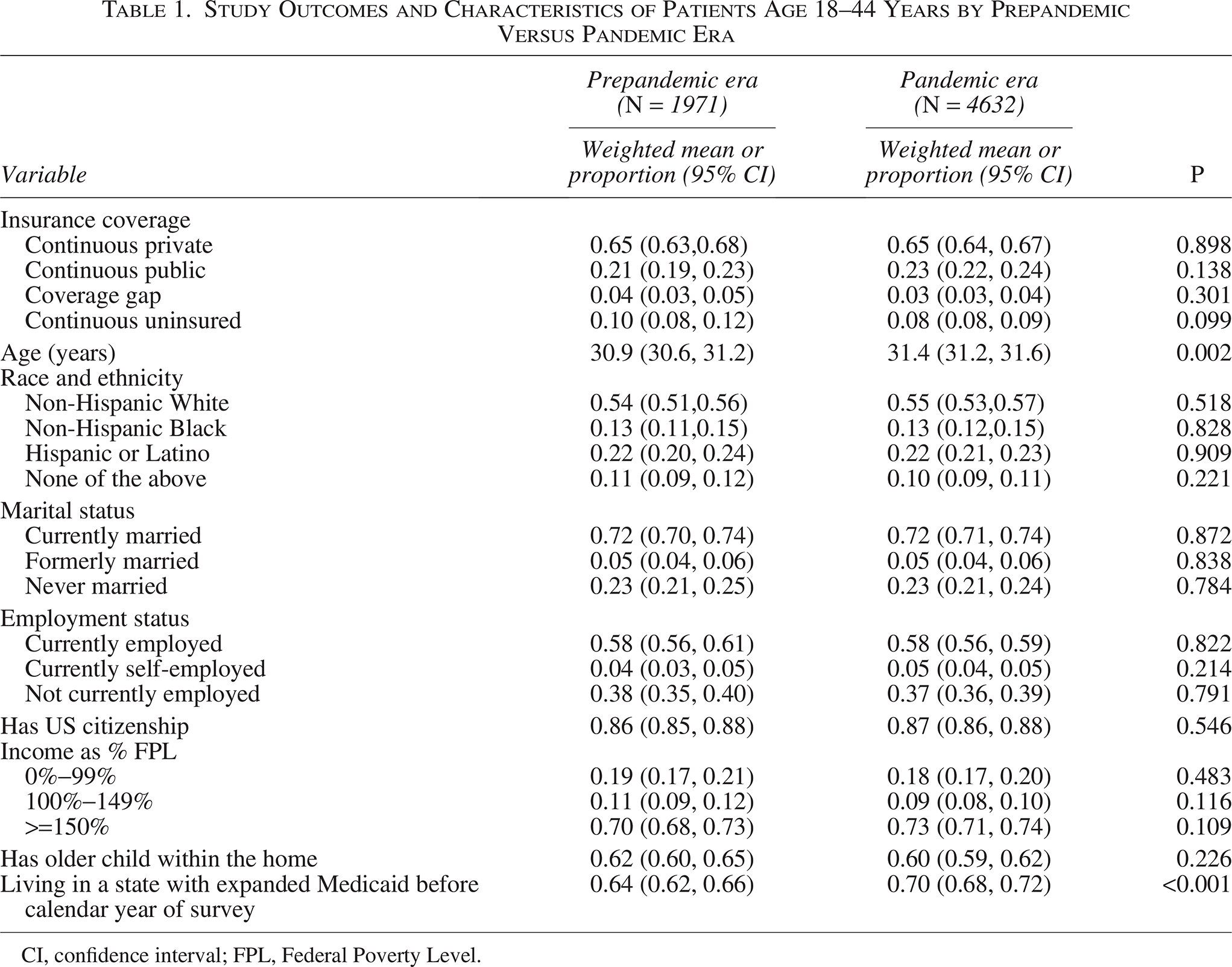
CI, confidence interval; FPL, Federal Poverty Level.
The multivariable model of insurance coverage is reported in Table 2. There was no significant difference in change in relative risks between pandemic era and continuous public coverage (RRR: 1.14; 95% CI: 0.97, 1.34; P = 0.102), part-year uninsurance (RRR: 1.07; 95% CI: 0.78, 1.47; P = 0.665), or continuous uninsurance (RRR: 0.89; 95% CI: 0.70, 1.15; P = 0.376) compared with having continuous private coverage. The relative risk of continuous public rather than continuous private coverage was higher among younger respondents, Black respondents, Hispanic respondents, unmarried respondents, self-employed or unemployed respondents, non-US citizens, respondents with lower household income, respondents with older children in the home, and respondents living in states that expanded Medicaid eligibility. Relative risks of coverage gaps or year-round uninsurance (compared with continuous private coverage) were higher among younger respondents, Hispanic respondents, unmarried respondents, unemployed respondents, non-US citizens, and respondents with lower income. However, respondents in Medicaid expansion states had lower relative risks of both coverage gaps and year-round uninsurance.
Multinomial Logistic Regression of Health Insurance Coverage (N = 6603)
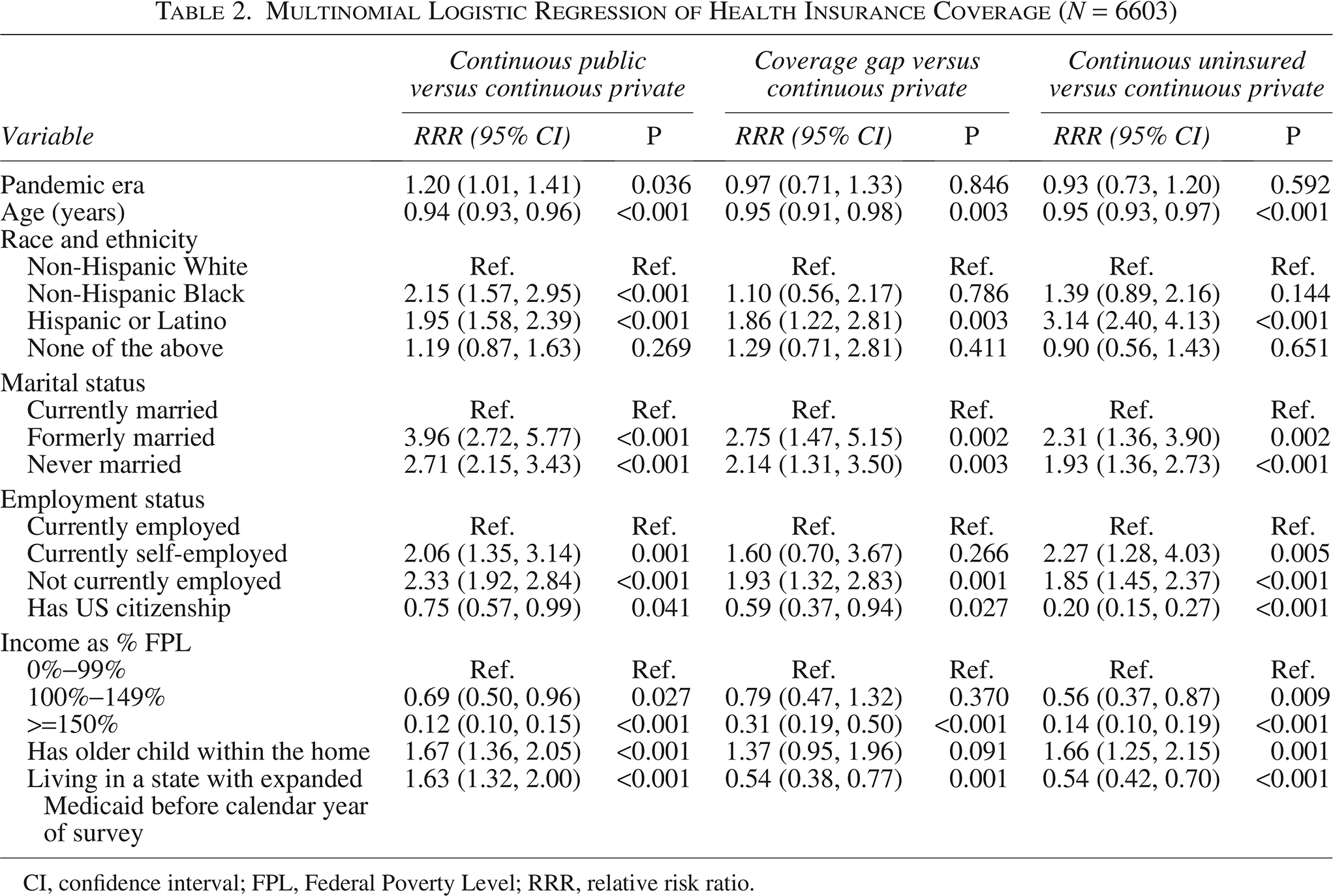
CI, confidence interval; FPL, Federal Poverty Level; RRR, relative risk ratio.
The secondary analysis of households with incomes below 100% FPL is reported in Table 3. In this subgroup, the pandemic era was associated with a lower relative risk of part-year uninsurance (RRR: 0.49; 95% CI: 0.27, 0.89; P = 0.020) but no significant changes in the relative risks of continuous public coverage (RRR: 0.76; 95% CI: 0.52, 1.12; P = 0.171) or continuous uninsurance (RRR: 0.69; 95% CI: 0.42, 1.11; P = 0.129) compared with having continuous private coverage.
Multinomial Logistic Regression of Prepandemic Versus Pandemic Era in a Subsample of Respondents with Household Incomes Below 100% FPL (N = 1162)
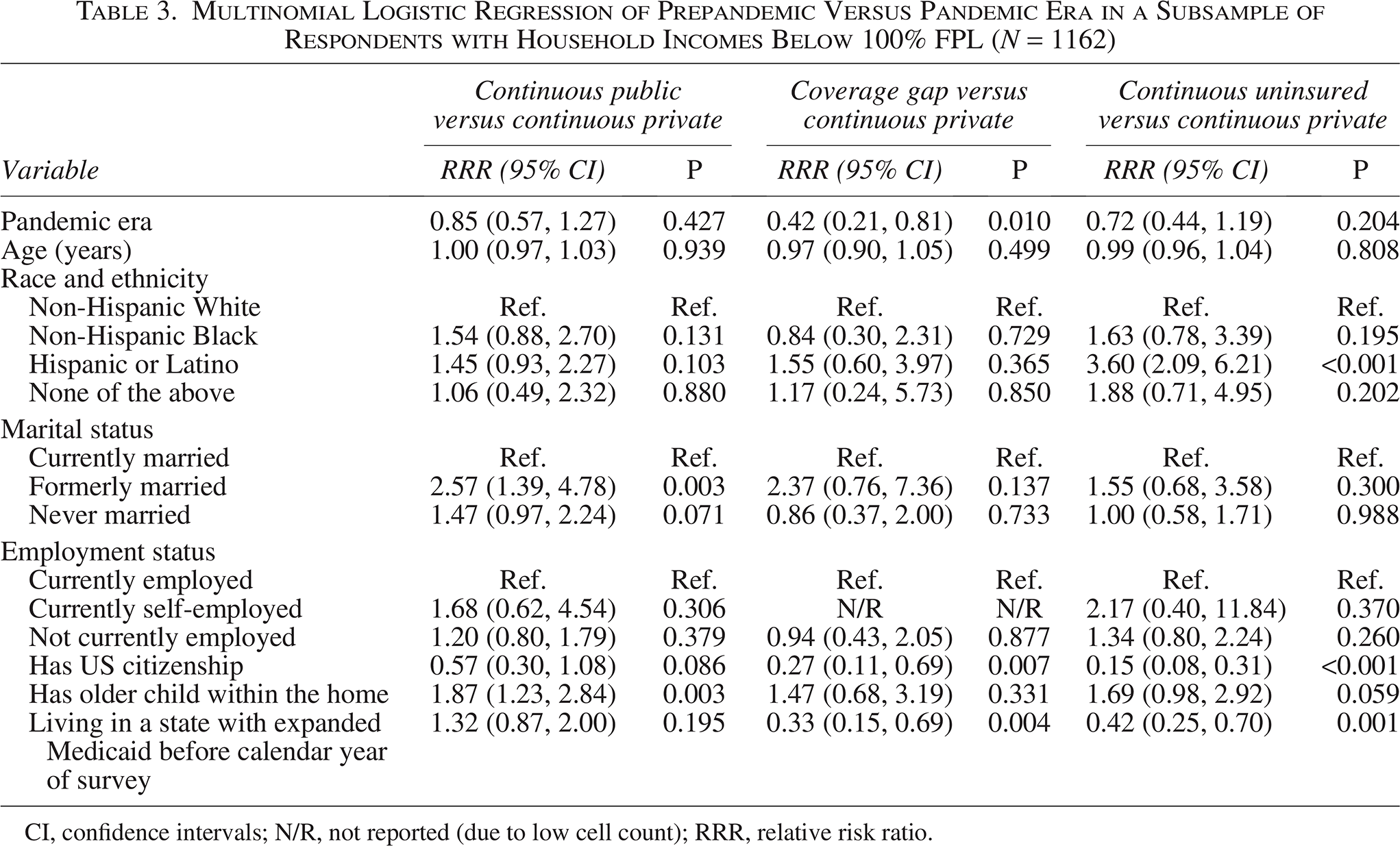
CI, confidence intervals; N/R, not reported (due to low cell count); RRR, relative risk ratio.
The sensitivity analysis of only 2019 and 2024 is reported in Supplementary Table A2. In this subgroup, the pandemic era was not associated with changes in relative risks of continuous public coverage (RRR: 0.997; 95% CI: 0.77, 1.29; P = 0.981), part-year uninsurance (RRR: 1.41; 95% CI: 0.89, 2.22; P = 0.141), or continuous uninsurance (RRR: 0.78; 95% CI: 0.55, 1.10; P = 0.156), compared with having continuous private coverage. The sensitivity analysis of households with incomes below 100% FPL for only 2019 and 2024 is reported in Supplementary Table A3. In this subgroup, the pandemic era was associated with a lower relative risk of continuous public coverage (RRR: 0.51; 95% CI: 0.29, 0.90; P = 0.021), but not associated with part-year uninsurance (RRR: 0.72; 95% CI: 0.31, 1.68; P = 0.454) or continuous uninsurance (RRR: 0.59; 95% CI: 0.30, 1.17; P = 0.129), compared with having continuous private coverage.
Discussion
The findings indicate that policies expanding Medicaid coverage through 1-year postpartum were not associated with increased risk of losing insurance coverage in the second-year postpartum. These results could be due to steady demand for private coverage and the transition of Medicaid beneficiaries to private insurance in the second-year postpartum. Extending the amount of time for postpartum individuals to select the right form of coverage or return to work and resume coverage by employer-sponsored insurance may help minimize coverage loss beyond the first postpartum year.
Approximately one-third of postpartum individuals experience insurance changes or loss.9,13 Americans living in states that have not expanded Medicaid are more likely to experience coverage loss. 14 While policy and research efforts have focused on the expansion of Medicaid coverage in the first year postpartum, there have been limited studies on whether this expansion has translated into sustainable insurance coverage beyond this initial period. Concerns about the sustainability of coverage were renewed when Medicaid redetermination came back into effect in April 2023. 15 As of September 2024, over 25 million original Medicaid enrollees have been disenrolled, with rates varying across states based on the policy promoting continuous coverage. 16 Difficulties with Medicaid renewal particularly affected families where at least one person in the family was ineligible, 15 and most Medicaid enrollees were unaware of their state’s ability to end their Medicaid coverage. 17 However, the secondary analysis shows that even after Medicaid redetermination (comparing 2024 with 2019), patterns of health insurance coverage in the second-year postpartum were generally comparable with prepandemic data.
In prior studies, major risk factors for coverage loss within the first postpartum year included Medicaid coverage at delivery (compared with private or other insurance), not speaking English at home, being unmarried, living in the South (compared with the Northeast, West, or Midwest), being >35 years old (compared with those younger than 20 years), lower educational attainment, and lower family income.18,19 The results further confirmed that being married and having a higher income were protective factors for retaining insurance coverage in the second-year postpartum. This is likely because having additional domestic and financial support facilitates mothers’ access to care by increasing their likelihood of having insurance and having additional childcare assistance. Employment status was also found to be consistently protective against coverage loss, which was likely related to access to employer-sponsored insurance. 20 Having additional children was associated with lower risk of coverage gaps, but was not associated with lower risk of being continuously uninsured. This could be due to familiarity with the process of Medicaid enrollment based on prior pregnancies.
This analysis shares limitations with prior research using CPS-ASEC data in studying postpartum health insurance coverage, including potential misreporting of insurance coverage and the lack of data on the type of coverage during pregnancy. 9 Insurance coverage sources were classified (public vs. private) based on coverage at the time of the survey, which prevented the inclusion of years before 2019 in the analysis. Furthermore, the measurement of coverage in the second postpartum year was based on reported child age in years, meaning the 12-month look-back period of the survey questions may have also captured episodes of uninsurance experienced during the first postpartum year. It is a known limitation that CPS-ASEC data does not record insurance coverage status at the time of delivery, and this study used the FPL as a proxy for likely Medicaid eligibility at the time of birth. Other limitations include the lack of data on potential chronic conditions present within the postpartum patient population, the inability to specifically identify biological children in the home, and the lack of data on respondents who gained coverage due to pregnancy in the second-year postpartum.
The American College of Obstetricians and Gynecologists advocated for bipartisan legislation to extend postpartum Medicaid coverage to improve maternal outcomes. 21 As many as 60,000 women in the US experience severe maternal morbidity every year. 22 These conditions include cardiomyopathy, diabetes, hypertension, anxiety, and depression, all of which require management during and after childbirth. Postpartum care is associated with improved maternal morbidity, although only 40% of Medicaid enrollees attend a postpartum visit. 23 The reasons for this are not clear, but women in Medicaid expansion states utilized postpartum outpatient services more than those in nonexpansion states, especially during the time frame in which the risk of coverage loss is the highest. 23 Sustained coverage in the postpartum period allows for chronic health conditions to be managed, and protecting the stability of health insurance coverage in the first postpartum year and beyond may help improve long-term health outcomes due to insured patients’ increased use of preventive services.18,24
Conclusions
Apart from Medicaid eligibility expansion, access and continuity of health insurance after birth can be enhanced by testing alternative payment models and marketplace reforms. 25 However, for people with significant health needs (like postpartum women), out-of-pocket premium and cost-sharing costs are higher with private insurance coverage compared with Medicaid. 26 High uninsurance rates both prenatally and postpartum suggest that low-income women face significant barriers in marketplace enrollment, highlighting the importance of reducing financial barriers for this population. 27 These findings have clarified and added nuance to risk factors for postpartum coverage loss, specifically beyond the first year postpartum. Ultimately, the pandemic-era policy to extend postpartum coverage to 1 year does not appear to have postponed loss of coverage, but may have contributed to decreasing part-year uninsurance among low-income families.
Authors’ Contributions
M.M.: Writing—original draft; writing—review and editing; visualization; investigation. Nupur.J.: Writing—original draft; writing—review and editing; visualization; investigation. Neha.J.: Writing—original draft; writing—review and editing; visualization; investigation; conceptualization. E.L.M.: Writing—review and editing; methodology; software; formal analysis; data curation. J.L.W.: Writing—review and editing; supervision; investigation; conceptualization. D.T.: Writing—review and editing; supervision; methodology; project administration; conceptualization.
Footnotes
Author Disclosure Statement
Dr. Tumin discloses salary support from Kate B. Reynolds Charitable Trust and Lilly Grant Office for research and quality improvement projects unrelated to this work. All remaining authors also report no conflict of interest.
Funding Information
No funding was received for this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.