
Abstract
Objective
To assess the impact of family social support (FSS) on postpartum quality of life (PQOL).
Methods
This analytical cross-sectional study enrolled postpartum women and asked them to complete the PQOL and FSS questionnaire (FSSQ) between October 2021 and February 2022 in three urban health centres in Shiraz, Iran. Pearson correlation coefficient analysis and multiple regression were used to determine the relationship between the FSS and PQOL variables. Structural equation modelling was used to determine the relationship pathways of the impact of FSS on PQOL.
Results
A total of 240 women were enrolled in the study. The mean ± SD scores of PQOL and FSSQ were 61.63 ± 9.59 and 69.80 ± 11.19, respectively. Family support seeking (7.95) and emotional support seeking (−6.80) were two factors affecting PQOL.
Conclusion
Women should be empowered to seek support through education and actions from health workers, especially nurses and midwives, during routine regular prenatal care.
Keywords
Introduction
The postpartum period is a stressful situation for women after childbirth. 1 Along with the presence of a baby and acceptance of a new role as a mother, special physical, physiological and psychological changes occur. These conditions and stressors can lead to a lack of adequate care for women and other family members due to various aspects of their lives and changes in quality of life (QOL).2,3 However, biomedical indicators are still applied in routine prenatal and postnatal care in obstetrics and gynaecology clinics.4,5 Using holistic health indicators, such as QOL, helps in planning holistic care and assessing the effectiveness of care and treatment interventions during the postpartum period.6,7
The World Health Organization defines the QOL as an individual's perception of his/her living situation in terms of culture and value system based on his/her ideals, expectations, standards and interests. 8 Understanding the determinants of QOL is regarded as a prerequisite for its improvement and enhancement. 9 Most studies have focused on biomedical, demographic or socioeconomic determinants.10–16 Social support is among the factors of care and intervention affecting the QOL during the postpartum period. 17
A person's perception of the types and amount of potential and actual support he/she can receive from the social environment plays a significant role in this regard. 18 Thus, social support can be defined, measured and presented from four dimensions including emotional (empathy, love), instrumental (tangible assistance), informational (consulting) and evaluation (constructive feedback). 19 Postpartum social support promotes a healthy lifestyle with buffering effects on stress, healthier nutrition for women, improving their QOL and a higher rate of breastfeeding.20–23 Accordingly, social support is considered an essential element for the physical and mental-emotional health of women, their infants and family, resulting in promoting society and social norms.19,24,25
Therefore, the routine and family social support (FSS) for women during the postpartum period should be evaluated urgently to promote their mental health and familiarize health workers with this concept. Others empower women to mobilize social support from other people, especially their families.26–29
With the emergence of the COVID-19 pandemic in 2019, several studies were conducted on its impact on postpartum social support and QOL, which reported controversial results and did not address this effect.30–32
Generally, shortcomings in the current knowledge and practice in women's healthcare means that there is a need for research on the QOL and its determinants during the postpartum period, especially the amount and dimensions of FSS. Providing evidence for change should impact on healthcare approaches, especially in nursing and midwifery care. In addition, the QOL during the postpartum period has not been examined exclusively and few studies have been conducted on postpartum FSS-related QOL.33,34 Thus, the present study aimed to investigate the status of and relationship between postpartum FSS and QOL in order to determine if FSS and its dimensions are determinants of QOL during this period in Iranian women.
Participants and methods
Study design and sample
This analytical cross-sectional study was conducted using a consecutive sampling method between October 2021 and February 2022 in three urban health centres in Shiraz, Iran. The present study was approved by the Research Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (no. IR.SUMS.REC.1400.223) in 2021. All methods were performed in accordance with the relevant guidelines and regulations. In addition, written informed consent was obtained from all participants for completing the questionnaires used in the study. The reporting of this study conforms to STROBE guidelines. 35 The details of the women were removed to ensure anonymity.
To determine the required sample size at a confidence interval of 95% with an acceptable error of 2% for the mean of postpartum QOL in Iran, 36 207 participants were estimated using the relevant formula. 37 Data from women in the study were used to undertake structural equation modelling (SEM). 38 The inclusion criteria were as follows: (i) no intellectual disability; (ii) no physical disability; (iii) able to read and write; (iv) had a live birth at least 1 month and up to 18 months previously. The exclusion criteria were as follows: (i) gave birth before 37 weeks of gestation; (ii) had a baby with a history of hospitalization in the neonatal intensive care unit; (iii) participant suffered from depression or any other psychiatric diagnosis; (iv) participant had a high-risk pregnancy (such as eclampsia and gestational diabetes). The participants were asked to complete the questionnaires within 30 min after the objectives of the study and the method of completing the questionnaires were explained to them.
QOL and FSS measures
Data collection instruments included the Persian version of the postpartum quality of life (PQOL) questionnaire 36 and the family social support questionnaire (FSSQ). 39
The Persian version of PQOL had a validity of 0.88 and 0.77 through Cronbach's alpha calculation and Kaiser-Meyer-Olkin (KMO), respectively; and Bartlett's test at the level of P < 0.001. The Persian version of PQOL consisted of 40 questions and four dimensions including childcare, physical function, psychological function and social support with 8, 12, 8 and 12 questions, respectively. The questions were answered on a 5-point Likert scale in the form of intensity (from [1] “not at all” to [5] “extremely”), frequency (from [1] “never” to [5] “always”) and evaluation (from [1] “highly dissatisfied' to [5] “highly satisfied”). The results were scored by the method of the original version between 0–100, in which the lowest and highest scores indicated the inappropriate and appropriate situation, respectively. First, the score of each item was transformed to 0–100 scale using the formula of transformed scale =
In the next step, the social support questionnaire was completed with a validity of 97.0 and 0.921 through Cronbach's alpha calculation and KMO, respectively; and Bartlett's test at the level of P < 0.0001. The FSSQ is regarded as a researcher-made questionnaire that has 79 questions in four dimensions including emotional support (with 25 questions), instrumental support (with nine questions), informational support (with 16 questions) and family support seeking (with 29 questions). The questions were answered in the form of a 4-point Likert scale, including “strongly disagree” [1] to “strongly agree” [4]; the scores were then transformed to a score of 0–100 for better analysis and understanding. 15 Answering these two questionnaires was considered self-reporting.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 and IBM Amos software, Version 24.0 (IBM Corp., Armonk, NY, USA).40,41 Descriptive statistics, such as frequency, mean and SD were used for demographic information after data extraction. Pearson correlation coefficient and multiple regression were utilized to determine the relationship between variables. SEM was applied to pathway mapping and measurement accuracy of the impact of the FSS on PQOL as latent variables. A P-value <0.05 was considered statistically significant.
Results
This analytical cross-sectional study included the data of from 240 women and there were no missing data. The mean ± SD age of the participants was 31.34 ± 5.52 years (range, 16–47 years). Of the 240 women, 131 (54.6%) had a university education and the remaining women had a high school diploma degree or lower. Of the 240 women, 199 (82.9%) were housekeepers and the remaining women were employed.
The mean ± SD PQOL score was 61.63 ± 9.59 (range, 40.00–87.50). Table 1 presents the mean ± SD and range scores of the childcare, physical function, psychological function and social support dimensions. The highest mean ± SD score was observed in the psychological function dimension (83.34 ± 11.76) and the lowest score was observed in the physical function dimension (55.83 ± 12.84).
Scores for the dimensions of the family social support questionnaire (FSSQ) and the Persian version of the postpartum quality of life (PQOL) questionnaire during the postpartum period in a study that investigated the relationship between postpartum family social support and quality of life in Iranian women (n = 240).

The mean ± SD FSS score was 69.80 ± 11.19 (range, 40.00–100.00). Table 1 represents the mean ± SD and range scores of emotional, instrumental, informational and seeking support dimensions and sub-dimensions. As shown, almost all of the dimensions and sub-dimensions scored equally except the emotional support-seeking sub-dimension (67.87 ± 12.67).
Table 2 presents the results of the Pearson correlation coefficient analysis. The results of the multiple regression analysis showed that perceived emotional support (P = 0.01), received emotional support (P = 0.03), emotional support seeking (P < 0.001), informational support seeking (P < 0.001) and family support seeking (P < 0.001) affected the PQOL (Table 3).
Results of the Pearson correlation coefficient analysis undertaken between the variables of the family social support questionnaire (FSSQ) and the Persian version of the Persian version of the postpartum quality of life (PQOL) questionnaire in Iranian women (n = 240) during the postpartum period.

**Correlation was significant at the 0.01 level (2-tailed); *correlation was significant at the 0.05 level (2-tailed).
CC, childcare; PhyF, physical function; PsyF, psychological function; SS, social support; FSS, family social support; FES, family emotional support; PES, perceived emotional support; RES, received emotional support; NES, needed emotional support; NInsS, needed instrumental support; FInfS, family informational support; PInfS, perceived informational support; RInfS, received informational support; FSSe, family support seeking; ESSe, emotional support seeking; InsSSe, instrumental support seeking; InfSSe, informational support seeking.
Results of the multiple regression analysis undertaken between the variables of the family social support questionnaire and the Persian version of the postpartum quality of life questionnaire in Iranian women (n = 240) during the postpartum period.

NS, no significant correlation (P ≥ 0.05).
The reciprocal impacts of the variables were investigated using SEM. Fit indices of the model included the root mean square error of approximation (0.100), the relative fit index (0.975), the incremental fit index (0.996), the comparative fit index (0.996), the Tucker-Lewis index (0.982) and the normed fit index (0.995). The structural equation showed an ideal fit (χ2/df = 3.554, P = 0.02). The factor load between PQOL and family support seeking and emotional support seeking were 7.95 and −6.80, respectively. Figure 1 shows the relationships between FSS and PQOL.
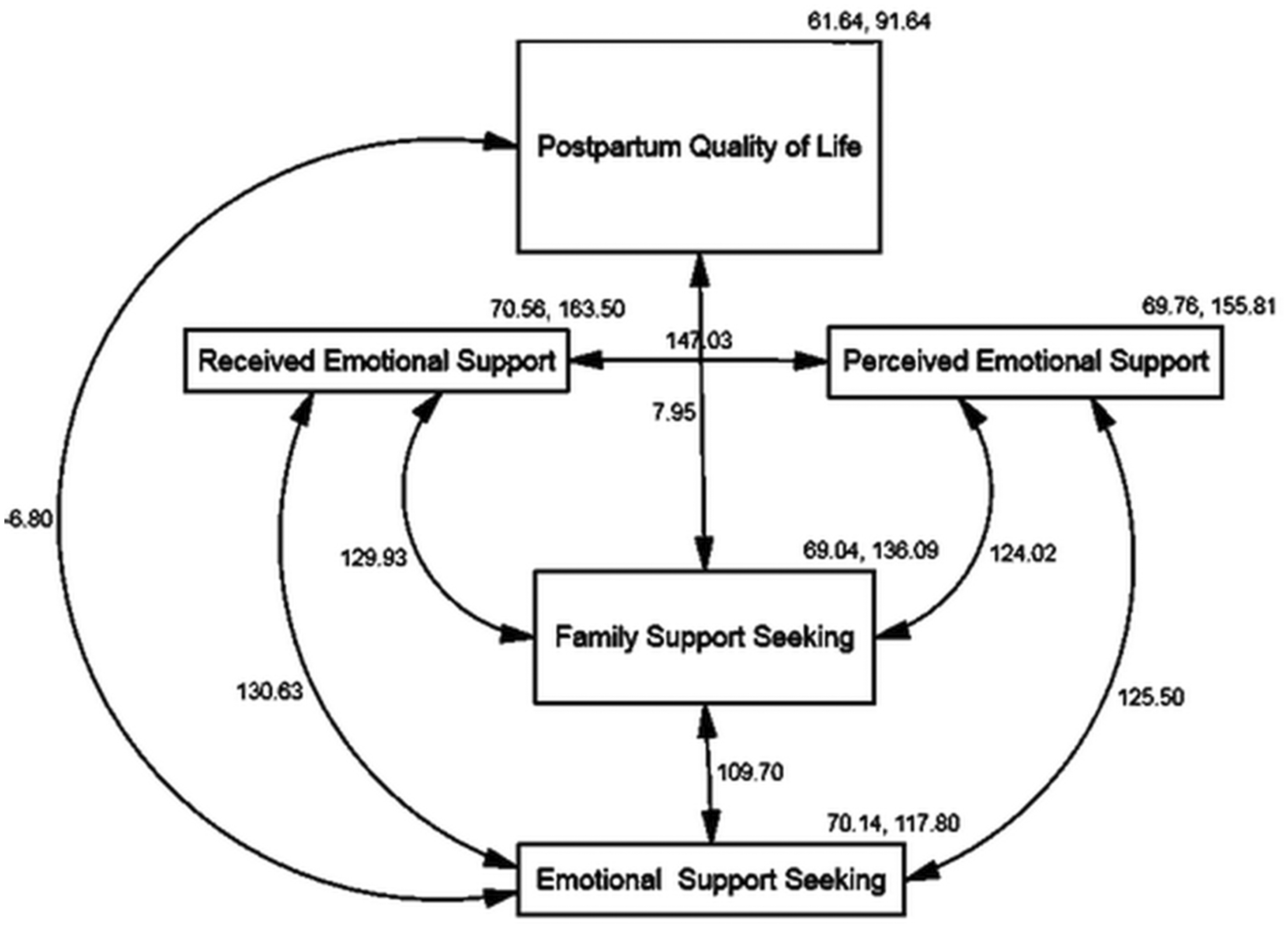
The relationship pathway between family social support and postpartum quality of life in Iranian women (n = 240). Covariance was used to measure the relationship between variables. Positive values indicate the same direction relationship and negative values indicate an inverse relationship between the variables. Family support seeking (7.95) and emotional support seeking (–6.80) were two factors affecting postpartum quality of life. In addition, perceived (124.02) and received (129.93) emotional support affected family support seeking.
Discussion
A previous study that determined the validity and reliability of the PQOL questionnaire in Iranian women was used to determine the sample size for this current study. 36 The results of the current study demonstrated a moderate PQOL among Iranian postpartum women, which was similar to the findings of the previous study. 36 In addition, the scores of the dimensions except social support were higher than those in the reference study, which could have occurred due to the inclusion criteria. 36 The history of childbirth in the current and reference studies was between 1–18 months and 60–67 days, respectively, during which the mother observed the most attention and had the least adaptation to new conditions. In another study undertaken in Iran, the mean ± SD PQOL of women using the Short-Form Health Survey questionnaire was 74.18 ± 12.65. 42 The difference in the QOL measured by the two studies could be attributed to the differences between the two questionnaires in terms of the number of questions asked and the range of dimensions covered.36,42 The mean ± SD QOL measured in postpartum women in other countries ranged from 45.15 ± 10.50 to 83.00 ± 8.13;15,43,44 and the differences observed could be attributed to applying different questionnaires with general questions or cultural, social and economic factors affecting the QOL.
In the present study, the mean score of FSS for postpartum Iranian women was moderate (69.80 ± 11.19). No study in Iran has reviewed FSS during the postpartum period. Most studies have focused on the social support from family, friends and significant others.38,45–47 The mean scores for the family support subscale in previous studies ranged from 21.52 to 22.39 on a 4–28 scale.38,47 Based on these previous results, the level of family support was regarded as appropriate.38,47 These previous findings were not consistent with the results of the present study due to the differences in the number of questions affecting the different aspects of the issue, along with the transparency and accuracy of the results. In other countries, the family support subscale was considered appropriate.34,48,49 Such discrepancies could be attributed to a lack of questions and ignoring the various aspects of the issue, leading to wrong and unclear results.
Results of the present study showed that family support seeking and emotional support seeking were two factors affecting PQOL. The effects of FSS on PQOL were not exclusively analysed and further studies should be conducted in this regard. Although the accuracy of this relationship cannot be shown in an evidence-based manner, it can be stated that in traditional societies seeking support from others is likely to be rewarded and the person that receives the support is not ashamed. 19 Thus, people are assured of family support seeking and having perceived supporters. Therefore, this finding may lead to the revision of perinatal and postpartum care with the target of paying special attention to developing and improving the status of women's support from the family to improve their QOL. In addition, it may guide other studies to further investigate the determinants of family support on QOL.
The strengths of the present study include the use of subject-specific tools to measure variables and the hierarchical use of analytical statistics to investigate the relationship between variables. The current study had several limitations including the self-reported data collection, which will need to be verified by further studies. In addition, women were not eager to participate in the study during the COVID-19 pandemic, since they wanted to spend less time in public centres and were not willing to complete the questionnaires. Thus, it took a long time for the researchers to convince them to participate in the study.
In conclusion, the present study showed that FSS was associated with QOL in the postpartum period in Iranian women. Seeking family support, especially emotional support, is among the most critical QOL-related factors. Improvement of women's QOL by identifying the above-mentioned factors and taking necessary actions by healthcare, especially nurses and midwives, strengthen women's physical, mental and childcare performance, plays a significant role in overcoming challenging situations and ensures their health worldwide. Therefore, women should be empowered to seek family support to improve postpartum QOL. Health workers are obligated to provide this empowerment, especially nurses and midwives. Thus, it is recommended to assess the status of family support and their ability to seek family support as routine prenatal care. Since the family members are the closest individuals to the postpartum woman. Additionally, few studies have been conducted on the relationship between FSS and QOL of postpartum women. Therefore, it is suggested that the present study can pave the way for further studies in Iran and other countries to identify the family support dimensions affecting women’s QOL.
Research Data
Research Data for The impact of family social support on postpartum quality of life among Iranian women: structural equation modelling
Research Data for The impact of family social support on postpartum quality of life among Iranian women: structural equation modelling by Khadijeh Khademi, Mohammad Hossein Kaveh, Leila Ghahremani, Mahin Nazari and Masoud Karimi in Journal of International Medical Research
Footnotes
Author contributions
Khadijeh Khademi collected and analysed the data and wrote the manuscript. Mahin Nazari participated in choosing the QOL instrument and conducting the study as an advisor. Leila Ghahremani participated in presenting the proposal and expressing the method of writing the manuscript. Masoud Karimi advised on the statistical analysis and method of reporting. Mohammad Hossein Kaveh supervised all of the processes from registering the project proposal until final editing of the manuscript as a supervisor. All of the authors read and approved the final version of the manuscript.
Acknowledgement
The authors acknowledge the support of Shiraz University of Medical Sciences to conduct this study in its affiliated health centres and the cooperation of the personnel of these centres with the researchers of this study.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.