
Abstract
Concurrent cardio-cerebral infarction (CCI) describes the simultaneous occurrence of an acute myocardial infarction and an acute ischemic stroke. It is a rare phenomenon, and no consensus yet exists on how to best treat it. CCI patients present with variable clinical scenarios and complications which makes the establishment of a treatment guideline difficult. We present here a case of a 67-year-old male with concurrent acute ST-elevation myocardial infarction and acute ischemic stroke due to right middle cerebral artery occlusion who was successfully treated with Tenecteplase and mechanical thrombectomy. A literature review was also conducted in search of potential reasonable management strategies of CCI.
Introduction
Concurrent cardio-cerebral infarction (CCI) refers to a rare event when an acute myocardial infarction (MI) and an acute ischemic stroke (AIS) occur simultaneously. It has posed immense challenges for physicians as delaying treatment of either condition may lead to devastating outcomes. However, no consensus has been made on how to best manage CCI, and the available case reports have suggested different treatment strategies which are often limited by circumstances in which those patients present. In many cases, mechanical thrombectomy (MT) or percutaneous coronary intervention (PCI) are not possible due to the clinical presentation, and even when these procedures are possible, opinions differ on the order in which they should be performed. Here, we report a 67-year-old man who presented with a simultaneous acute ST-elevation MI (STEMI) and acute right hemisphere stroke. He was treated with Tenecteplase (TNK) followed by mechanical thrombectomy (MT) and was discharged with good clinical outcome 5 days later. We also review previous reports of CCI in the literature and discuss its management strategies.
Case Report
A 67-year-old man with a history of hyperlipidemia, paroxysmal atrial fibrillation (AF) not on anticoagulation, chronic obstructive pulmonary disease, tobacco abuse, and obstructive sleep apnea complained of sudden onset chest pain at home. On the arrival of the Emergency Medical Service, the patient began to develop left-sided hemiplegia and neglect. In the emergency room, his NIH stroke score (NIHSS) was 15 and CT of the head showed no hemorrhage but hyperdense sign of the right middle cerebral artery (MCA) M1 segment. He was also found to have an anterior STEMI on EKG (Figure 1(a)) and high-sensitive troponin-I level >24,000. Both cardiology and neurology services were involved. Thrombolytic therapy with TNK was given at the dose for cerebral infarction (0.25 mg/kg). CT angiogram of the head and neck showed distal right M1 occlusion (Figure 1(b)) as well as high-grade stenosis of right proximal internal carotid artery (ICA). Although the patient was also experiencing a STEMI, he was hemodynamically stable without sign of cardiogenic shock or high-risk arrhythmia. In addition, the cardiologist was concerned about the risk of hemorrhagic conversion after TNK with concomitant use of dual antiplatelet therapy if PCI were performed, so the STEMI was managed medically with intravenous (IV) heparin and clopidogrel 24h post TNK administration. The patient had severe neurologic deficits with a proximal large vessel occlusion (LVO) and within early treatment window, MT was then given priority. Subsequent cerebral angiogram confirmed right M1 occlusion and right ICA high-grade stenosis (Figure 1(c)). He underwent successful MT with complete revascularization of right M1 (Figure 1(d)). Post procedure, his stroke symptoms and chest pain were much improved the following day and NIHSS was down to 5. MRI brain showed scattered patchy acute cerebral infarcts at the right MCA territory (Figure 1(e)). Echocardiogram demonstrated septal and anterior segment akinesis with left ventricle ejection fraction of 20-25% compared with 60-65% one year prior. The patient received a right ICA stent 3 days after his stroke. His IV heparin was transitioned to apixaban for paroxysmal AF and cardiomyopathy, and he was discharged home with minimal residual left hemiparesis at day 5. Other medications on discharge included clopidogrel, atorvastatin, metoprolol, sacubitril-valsartan, and spironolactone. At follow-up in 3 months, he only had mild left hand residue dexterity difficulty. (a) Electrocardiogram on presentation showing ST elevation in anteroseptal leads and T wave inversion in anterolateral leads, consistent with acute anterior STEMI. (b) CT angiogram of the head showing right MCA M1 segment occlusion (arrow). Cerebral angiogram showing (c) proximal right internal carotid artery high-grade stenosis (arrow) and (d) successful mechanical thrombectomy with complete revascularization of right MCA. (e) MRI brain showing patchy acute infarction at the right MCA territory.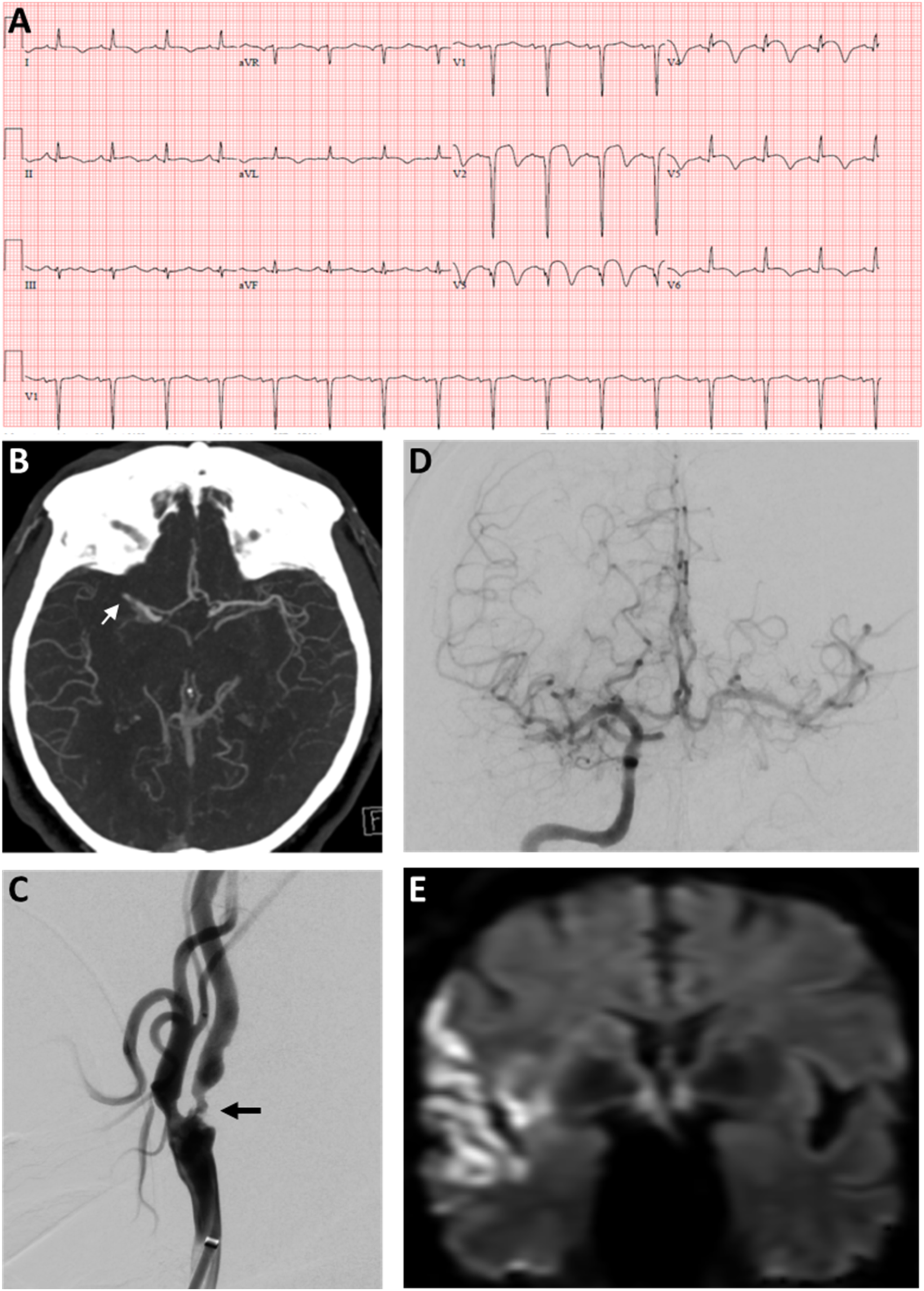
Discussion
The mechanism for CCI is not quite clear, but several possible explanations exist. It has long been postulated that the development of a mural thrombus in a patient suffering an acute MI with myocardial dysfunction may give rise to emboli which then cause acute ischemic stroke.1,2 Another possibility would be the paradoxical embolus from a right ventricular thrombus in the setting of patent foramen ovale. 3 Thrombus from AF is also considered a common source of CCI.4,5 In addition, MI induced hypoperfusion may induce watershed cerebral infarcts in the vascular border zones. 1 Rarely, aortic dissection extending to coronary ostia as well as the carotid or vertebral artery can be the culprit. 3 Hypercoagulable state from advanced malignancy or essential thrombocytosis has been associated with CCI.6,7 Lately, during the COVID pandemic, hypercoagulability from COVID infection has also been speculated to play a role in the pathogenesis of CCI.8,9 In our case, AF not on anticoagulation and acute cardiomyopathy associated with anterior STEMI are likely the possible causes of his CCI.
Broadly speaking, CCI can be further divided into synchronous (thrombosis of two vessels at the same time) or metachronous (thrombosis of one vessel precedes the other) events.10,11 For metachronous CCI, the priority of care will be directed without delay towards the initial event, according to the standard guidelines of each. Here we will focus on synchronized or nearly synchronized CCI, which is a rare event with an estimated incidence of 0.53%-0.9% in stroke patients.10,11 Due to a narrow treatment window, delayed therapy of either MI or AIS can cause severe consequences including long-term disability and death. Timely and appropriate decisions must be made in terms of the candidacy of thrombolysis, priority of available intervention modalities, and the balance between potential ischemic and hemorrhagic complications. However, no consensus on the management of CCI currently exists given the rarity of the situation and the lack of clinical trials.
Characteristics, Decision-making and Outcomes of reported Synchronous CCI Cases in the Literature.
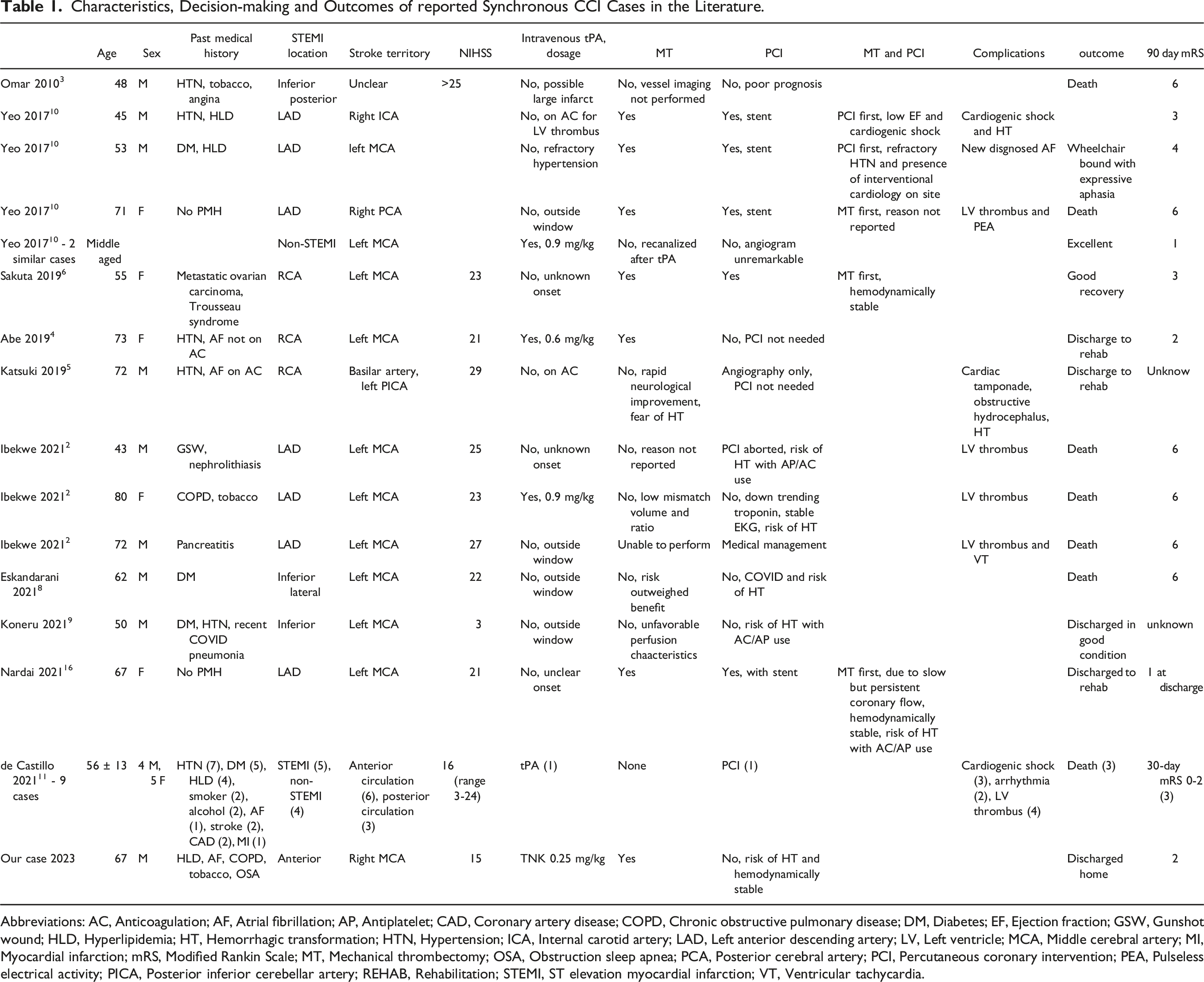
Abbreviations: AC, Anticoagulation; AF, Atrial fibrillation; AP, Antiplatelet; CAD, Coronary artery disease; COPD, Chronic obstructive pulmonary disease; DM, Diabetes; EF, Ejection fraction; GSW, Gunshot wound; HLD, Hyperlipidemia; HT, Hemorrhagic transformation; HTN, Hypertension; ICA, Internal carotid artery; LAD, Left anterior descending artery; LV, Left ventricle; MCA, Middle cerebral artery; MI, Myocardial infarction; mRS, Modified Rankin Scale; MT, Mechanical thrombectomy; OSA, Obstruction sleep apnea; PCA, Posterior cerebral artery; PCI, Percutaneous coronary intervention; PEA, Pulseless electrical activity; PICA, Posterior inferior cerebellar artery; REHAB, Rehabilitation; STEMI, ST elevation myocardial infarction; VT, Ventricular tachycardia.
A few patients without contraindications received thrombolysis with IV alteplase (Table 1), which was thought to benefit both MI and AIS.2,4,10,12,13 However, the dosage of IV alteplase in CCI has been a topic of debate as a higher dose is recommended in MI alone 14 as compared to AIS alone. 15 While most reported CCI cases received the 0.9 mg/kg regular IV tPA dose for AIS,2,10,13 some were given lower doses at 0.6 mg/kg 4 or 0.5 mg/kg 12 to mitigate the risk of hemorrhagic conversion. According to the latest acute stroke guideline, “for patients presenting with concurrent AIS and acute MI, treatment with IV alteplase at the dose appropriate for cerebral ischemia, followed by percutaneous coronary angioplasty and stenting if indicated, is reasonable (COR IIa; LOE C-EO)”. 15 Without significantly increasing the risk of hemorrhagic conversion, stroke dose of alteplase has been accepted by most clinicians in the setting of CCI.
As far as we know, our patient presented here is the first case received TNK in the setting of CCI. Of note, the stroke dose of TNK (0.25 mg/kg with maximum 25 mg) is significantly lower than the cardiac dose.14,15 Combined with the higher affinity to fibrin than alteplase, TNK may render a lower risk of hemorrhagic conversion when used in CCI.
Among the reported cases, only a handful of patients received MT, PCI or both (Table 1).4,6,10,16 When both interventions were available, the order in which they were performed was variable. Sakuta et al. reported a patient with ovarian cancer and Trousseau syndrome was admitted with left MCA occlusion and occurring at the same time an inferior MI. 6 She underwent MT of the left MCA first and then PCI of her right coronary artery. She had a modified Rankin Score (mRS) of 3 on follow-up 3 months later. Another case with a left MCA stroke and anterior STEMI presented outside of the window for thrombolytics and was treated with MT first, followed by coronary revascularization. 16 This case was unique as both procedures were performed by a single operator. Yeo et al. also discussed 3 cases of both MT and PCI, with 2 of them having PCI first and then MT and the other MT first followed by PCI. 10 One patient achieved 90-day mRS of 3, one mRS of 4 and the other died during hospitalization.
Most physicians recommend the combined approach in managing CCI. A feasible combined option is to administer the stroke dose of thrombolytics first when there are no contraindications, and then proceed to endovascular approaches including PCI, MT or both whichever is appropriate.1,2,10,16 When both MT and PCI are possible, treating the stroke first if the NIHSS score is high, the mismatch profile is favorable, the collaterals are poor, or a proximal LVO is present. However, treating the MI first if the patient develops cardiogenic shock, hemodynamic instability, severe cardiomyopathy or high-risk arrhythmia.10,16 Nonetheless, the final decision-making should be individualized, and based on the cardiac and cerebral conditions at the presentation. Our case underwent MT without PCI because of stable vital signs and EKG changes. He was discharged home with 90-day mRS at 2.
The prognosis of CCI is generally poor (Table 1). On reviewing 25 previously reported cases, Ibekwe et al. stated that about 4 (16%) and 6 (24%) having mRS ≤ 3 at 1 and 3 months, respectively. Approximately 20% expired during hospitalization. 2 de Castillo et al. pooled cases from the literature and their own data and reported CCI mortality rate of 28%. 11 The relatively poor outcome likely reflects the serious clinical profiles of both MI and AIS, but also the inconsistent clinical practice without clear consensus. Combined approach mentioned above may provide a reasonable guideline to improve the prognosis.
Conclusions
CCI is a clinically very challenging situation. Although occurs rather seldom, it renders high likelihood of poor outcome. The presentation is so variable that reaching consensus for an optimal treatment is probably difficult. However, as the management of both MI and AIS advances and our experience of treating CCI accumulates, a combination of interventional approaches based on patient cardiac and cerebral conditions may be most reasonable and acceptable.
Footnotes
Acknowledgments
An informed consent for publication was obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.