
Abstract
We present a case and video of a 31-year-old man with biopsy-confirmed tumefactive demyelination affecting the right internal capsule causing left hemiplegia, excessive yawning, and the curious but well-described phenomenon of parakinesia brachialis oscitans (PBO) with transient tonic elevation of his paralyzed arm while yawning. PBO is most commonly reported in ischemic stroke with internal capsule or pontomedullary brainstem lesions. Our case uniquely demonstrates this phenomenon in the case of tumefactive demyelination. We also highlight excessive yawning which has also been described in multiple sclerosis.
A 31-year-old previously healthy male presented to hospital with five days of progressive left-sided ataxic-hemiparesis two weeks after upper respiratory tract infection. Examination demonstrated left hemiplegia. MRI revealed mass-like abnormality involving deep right subcortical white matter (Figure 1). Lumbar puncture showed lymphocytic pleocytosis (15 cells/uL) with oligoclonal banding. Stereotactic biopsy revealed focal demyelination without histopathological evidence of lymphoproliferation or vasculitis. He initially had frequent yawning with concomitant transient tonic elevation of his paralyzed arm (supplemental video). Parakinesia brachialis oscitans (PBO) is mostly reported in ischemic stroke with internal capsule or pontomedullary brainstem lesions.
1
It is thought to involve release of subcortically regulated automatisms from cortical inhibition.
1
It is proposed that strong contraction of respiratory muscles during yawning generates proprioceptive signals reaching the anterior horn cells of C4-C8, resulting in involuntary movement of the affected upper limb.
2
Cortical release may also lead to excessive yawning seen in patients with multiple sclerosis.
3
Yawning is postulated to modulate cortisol levels, signal brain cooling, and promote clearing of cerebrospinal fluid into central venous structures.
3
Yawning is also thought to be the somatization of a disinterested emotional state, leading to upper limb stretching movements via reticulospinal tracts.
4
Insufficient detection of cortisol levels in stroke may result in the failure of the brainstem to respond to changes in cortisol level, preventing the inhibition of arm movement.
1
This video uniquely demonstrates excessive yawning and PBO in a patient with tumefactive demyelination. Following high-dose intravenous corticosteroids and mitoxantrone, he had complete motor recovery which was sustained at 18-month follow up. Axial T2-FLAIR MRI demonstrating (A) confluent subcortical white matter hyperintensity involving the right corona radiata, centrum semiovale, and deep white matter of the right frontal lobe and corpus callosum; (B) resolved on follow-up 1 year later.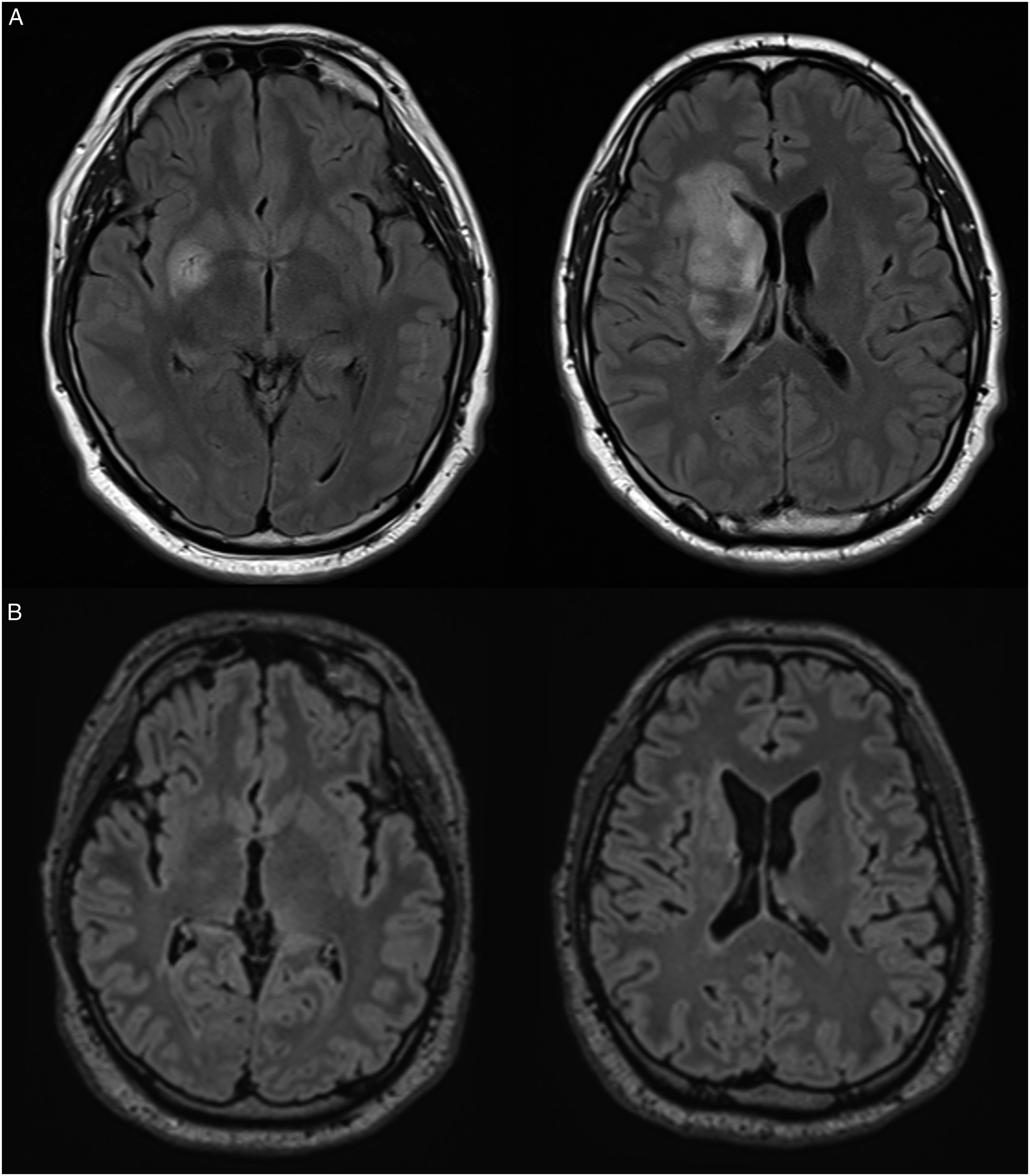
Supplemental Material
Footnotes
Acknowledgements
The authors thank the patient for written consent to publish this case and video. Authors take full responsibility for the data collected, analysis, interpretation, and conduct of this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.