
Abstract
Background:
Lower extremity muscle tears are common sports injuries. The British Athletics Muscle Injury Classification (BAMIC) may provide clinical guidance for tears although its value in American football and college athletes is unknown.
Hypothesis:
Clinical outcomes, specifically time to return to play (RTP) (TRTP), in college American football athletes with activity-related hamstring (HS) and quadriceps (QD) tears will be associated with BAMIC.
Study Design:
Retrospective cohort study.
Level of Evidence:
Level 3.
Methods:
American football college athletes who sustained a HS or QD tear and underwent magnetic resonance imaging within 7 days at 1 institution during the 2023 season were included. TRTP and reinjury rate (RIR) for HS and QD tears classified by BAMIC and injury characteristics were evaluated.
Results:
Of the 24 HS and 10 QD tears in 21 (17.3%) of 121 athletes (20 ± 1.2 years; 100.0% male), most (60.0%) were BAMIC 2a-3b. Most (89.3%) injuries occurred before the season, and all occurred in practice. Overall median TRTP was 26 days (interquartile range, 17.8-33.0), translating to about 4 weeks missed play. The RIR was 19.0% (4/21). Most (75.0%) reinjuries occurred before RTP. There was no significant relationship between BAMIC and TRTP, although TRTP was less for grade 0 injuries and greater TRTP for injury site “c,” albeit with small effect sizes.
Conclusion:
Activity-related HS and QD tears are common in American football college athletes, particularly in preseason and practice. Injured athletes missed about 3 to 4 games, regardless of BAMIC, with 1 in 5 athletes suffering a reinjury. There was no relationship between BAMIC or muscle group and TRTP.
Clinical Relevance:
This appraisal of BAMIC in college and American football athletes highlights the prevalence of muscle tears and the need for prevention. Although BAMIC lacked value in this study, larger studies are needed to evaluate BAMIC in this population.
Keywords
Lower extremity muscle tears are common activity-related injuries and are among the most common injuries responsible for absence from training and competition.7,10,27 Although these injuries are often described as “strains,” some clinicians prefer the term “tear” as it more accurately describes the structural characteristics of the injury. 19 Muscle tears impose a burden in sports requiring acceleration, sprinting, and kicking, including soccer, rugby, track and field, and American football (football).1,3,7,8,15
The muscles most injured among National Football League (NFL) athletes are the hamstring (HS), followed by the quadriceps (QD), with HS injuries ranking as the second most common injury in the NFL and the third most common injury in college football.4,9,14 Despite their frequency, there is limited evidence defining return to play (RTP) times for HS and/or QD tears in college football athletes.5,14,15 Also, the evidence for prognostic guidance for HS and QD injuries is constrained by the heterogeneity of injury grading and classification systems. 14
Muscle injury classification and grading systems may be important because they may provide therapeutic and prognostic guidance. Previous studies using magnetic resonance imaging (MRI) to predict time to return to play (TRTP) in football athletes have demonstrated conflicting results, and some studies have reported that accurate prediction of TRTP is not possible using MRI classifications alone.5,11,14,29
In 2014, the British Athletics Muscle Injury Classification (BAMIC), an MRI-based classification designed to define muscle tears, predict clinical outcomes, and guide rehabilitation, was published (Figure 1). 23 Since its publication, some studies have shown that BAMIC may offer superior therapeutic and prognostic guidance for lower extremity muscle injuries compared with previous classification and grading systems, particularly in predicting TRTP and reinjury rate (RIR).2,13,16-18,20-22,24-26,28,29. Among studies assessing the clinical value of BAMIC, athletes were mostly elite or professional level and played soccer or track and field. Presently, the authors are not aware of studies that appraise the clinical value of activity-related lower extremity muscle tears classified by BAMIC in college athletes or in the context of football. Therefore, the value of BAMIC in college athletes or in the football sport is unknown, but pertinent and further investigation is warranted.
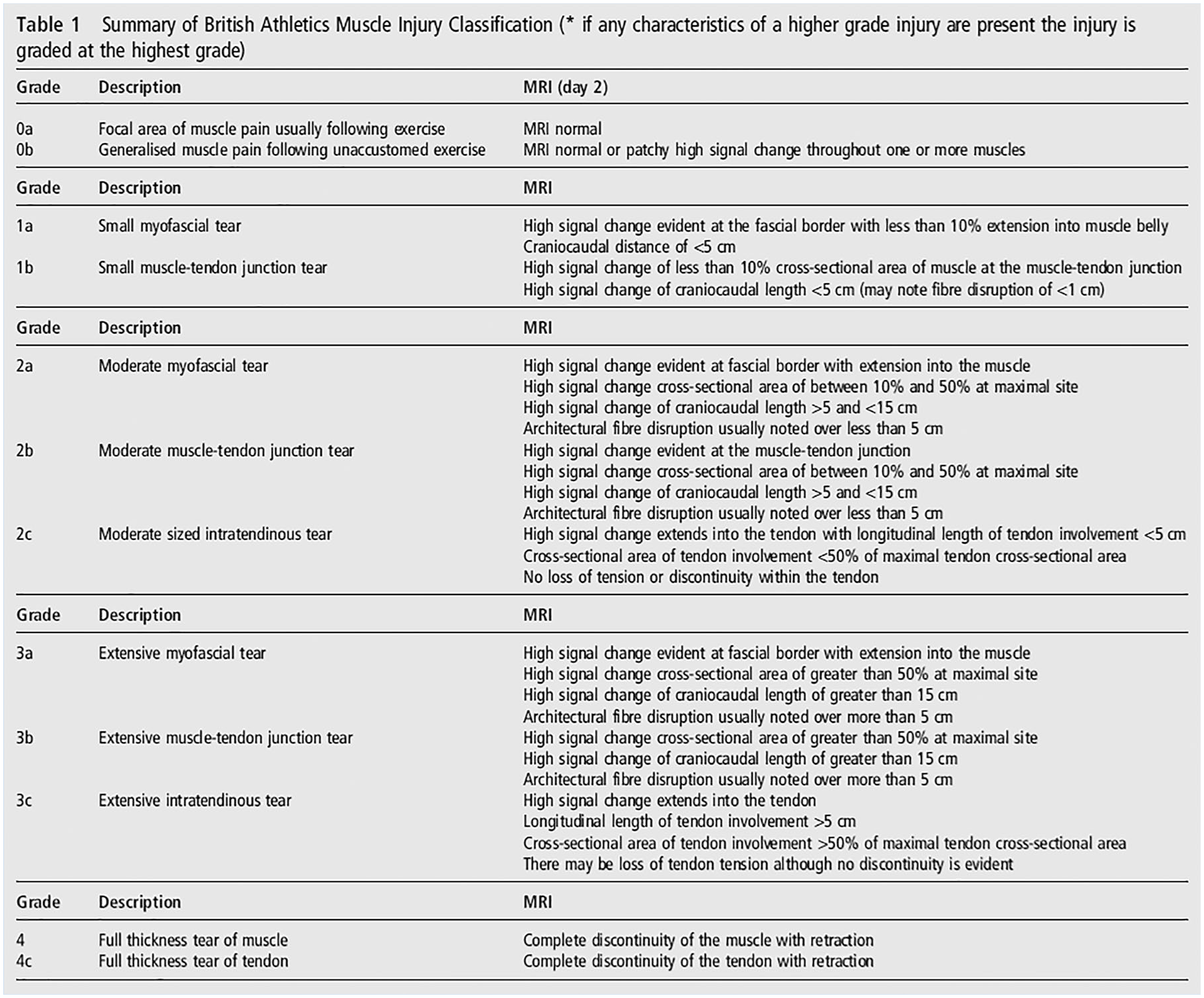
The BAMIC (reproduced from Pollock et al 25 ). BAMIC, British Athletics Muscle Injury Classification.
The aim of this study was to assess clinical outcomes, specifically TRTP and RIR, and injury characteristics of activity-related muscle injuries classified by BAMIC in National Collegiate Athletic Association Division-I (NCAA-DI) football athletes during the 2023 season.
Methods
Study Design and Participants
This study was a retrospective observational cohort study with the aim of evaluating clinical outcomes, particularly TRTP and RIR, and injury characteristics of activity-related HS or QD muscle injuries as classified by BAMIC in NCAA-DI American football college athletes during the 2023 season (spring, preseason, regular season). Injuries were eligible for study inclusion if the injured athlete was an active roster football athlete during the 2023 season at the host institution, experienced an acute-onset football-related lower extremity muscle injury involving the HS and/or QD muscle group(s), received a subsequent diagnosis of a muscle tear by a team physician, underwent an MRI scan without contrast of the affected muscle group within 7 days of the date of index injury, and had the MRI scan interpretation performed by a fellowship-trained, board-certified musculoskeletal radiologist following the BAMIC protocol. 25 HS or QD tears where the RTP date was unknown were excluded from this study.
Data Collection
This study was approved by the host institutional review board. The included athlete’s sex, age, history of previous HS or QD injury (if recorded), date of injury, date of reinjury (if applicable), RTP date, laterality of injury, activity when injury occurred, and return to previous level of play were extracted from the athlete’s electronic medical record (EMR). The EMR of included athletes was reassessed monthly to identify r-injury. MRI scan data obtained included: date of imaging, primary muscle affected, additional HS or QD muscles affected (if applicable), and BAMIC. MRI was performed on either a 1.5- or 3-T MRI scanner at a single imaging center at the host institution. All MRI scans included image sequences used to designate BAMIC. 25
Protocol
The TRTP was calculated as the number of days between the date of index injury and the date that the athlete returned to football (practice, weightlifting, or competition) without any activity limitation enforced by the team medical staff. Day zero was defined as the date of index injury. The RTP date was defined as the date that a team athletic trainer or team physician changed the athlete’s performance status to training and competition without any activity limitation.
Treatment and rehabilitation were provided by the team athletic trainers, physical therapists, and sports medicine physicians. Treatment consisted of rest, ice, elevation, pain management, and rehabilitation. BAMIC results were used for information purposes only and were not utilized to guide treatment. Rehabilitation was guided by the philosophy of increasing functional and strength-based recovery incorporating an adaptable return to running progression depending on the athlete’s functional status and pain level. There were no specific criteria used for reintegration into practice, which occurred gradually, starting with individual, sport-specific drills, and slowly increasing exercise volume.
The decision for RTP was made by the team physician and athletic trainers. The decision for return to play was multifaceted and encompassed the athlete’s subjective inclination to RTP, rehabilitation progress and clinical markers including defined parameters for bilateral lower extremity range of motion (ie, symmetric bilateral hip and knee range of motion), strength (ie, within 10% of symmetric knee flexion strength using a force measurement sensor), resolution of pain, and incorporation of continuously assessed variables defined by global position systems (GPS). GPS measuring player load during practice (ie, combined metrics including sprint velocity, accelerations and decelerations, distance covered) were used as part of the clinical markers to determine RTP. Specifically, player load was gradually increased in practice, and, when an athlete’s player load reached the average level for their position group, the athlete was considered healed according to GPS criteria.
A reinjury was recorded if the player sustained an acute, sudden exacerbation of pain in the same muscle and region as the index injury during exercise, followed by worsening of clinical tests including localized tenderness to palpation and changes with manual muscle testing and requiring cessation of current activity of rehabilitation or training for >48 hours. 25 All suspected reinjuries were evaluated by a team physician, who confirmed the diagnosis of reinjury. Reinjuries were included if the injury occurred during the index injury rehabilitation process or within 3 months of the day of an injured athlete was designated “as tolerated.”
Statistical Analysis
Frequencies, mean, median, standard deviation, and interquartile range were used to describe participant/injury characteristics, TRTP, and RIR. Participant and injury characteristics were described for all 34 injuries among the 21 participants. However, as in Pollock et al, 25 an injury was excluded if the participant had a reinjury before returning to play for TRTP analysis. To assess differences in TRPT by BAMIC (0a-3b), grade (0-3), injury site (a-c), and muscle group, Kruskal-Wallis H and Mann-Whitney U tests were used where appropriate. For these analyses, repeat participants were excluded by selecting primary injury based on having a higher BAMIC. If 2 cases had the same BAMIC, then the injury to the long head of the bicep femoris was included. Median and interquartile range of TRTP were plotted by BAMIC, grade, injury site, and reinjury status. Separate linear regressions assessing TRTP by grade and injury site were conducted controlling for age and then for muscle group. All analyses were conducted using IBM SPSS Statistics (Version 29.0).
Results
Study Participants and Injury Characteristics
The study participant and injured muscle characteristics are described in Table 1. Athletes were excluded if there was no identifiable RTP date (n = 3), if an MRI scan was not obtained (n = 2), and due to incorrect diagnosis (ie, femoral diaphyseal stress fracture, n = 1). A total of 11 (52.0%) of the athletes suffered ≥2 separate muscle injuries during the index injury. One athlete suffered an index injury involving both his HS and QD. Most (89.3%) tears occurred before the season and all tears occurred in practice. All injured athletes returned to previous level of play.
Characteristics of study participants and HS and QD injuries
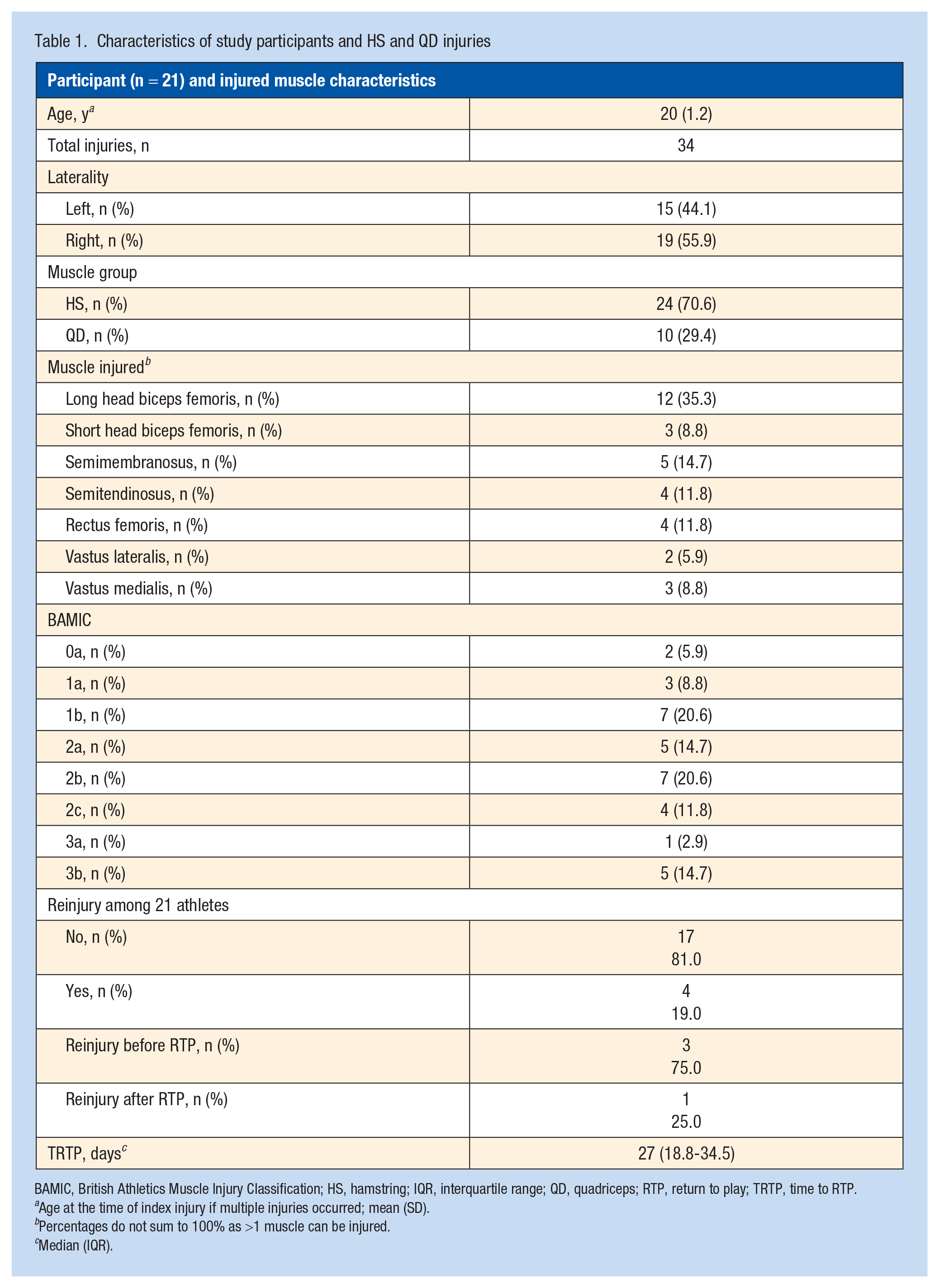
BAMIC, British Athletics Muscle Injury Classification; HS, hamstring; IQR, interquartile range; QD, quadriceps; RTP, return to play; TRTP, time to RTP.
Age at the time of index injury if multiple injuries occurred; mean (SD).
Percentages do not sum to 100% as >1 muscle can be injured.
Median (IQR).
Association Between TRTP, BAMIC, and Muscle Group
The median TRTP and number of injuries by BAMIC are presented in Table 2. Most injuries were classified as BAMIC 2a-3b (60.0%) and 2 injuries (<0.1%) were 0a. The median TRTP for muscle injuries according to BAMIC, grade, and injury site are presented in Figure 2. The median TRTP was 26 days (interquartile range [IQR], 17.8-33.0) with BAMIC 0a included and 29 days (IQR, 23.3-35.5) with BAMIC 0a excluded, which translates to approximately 4 weeks of missed play due to injury.
TRTP and RIR of HS and QD injuries according to BAMIC (n = 30)
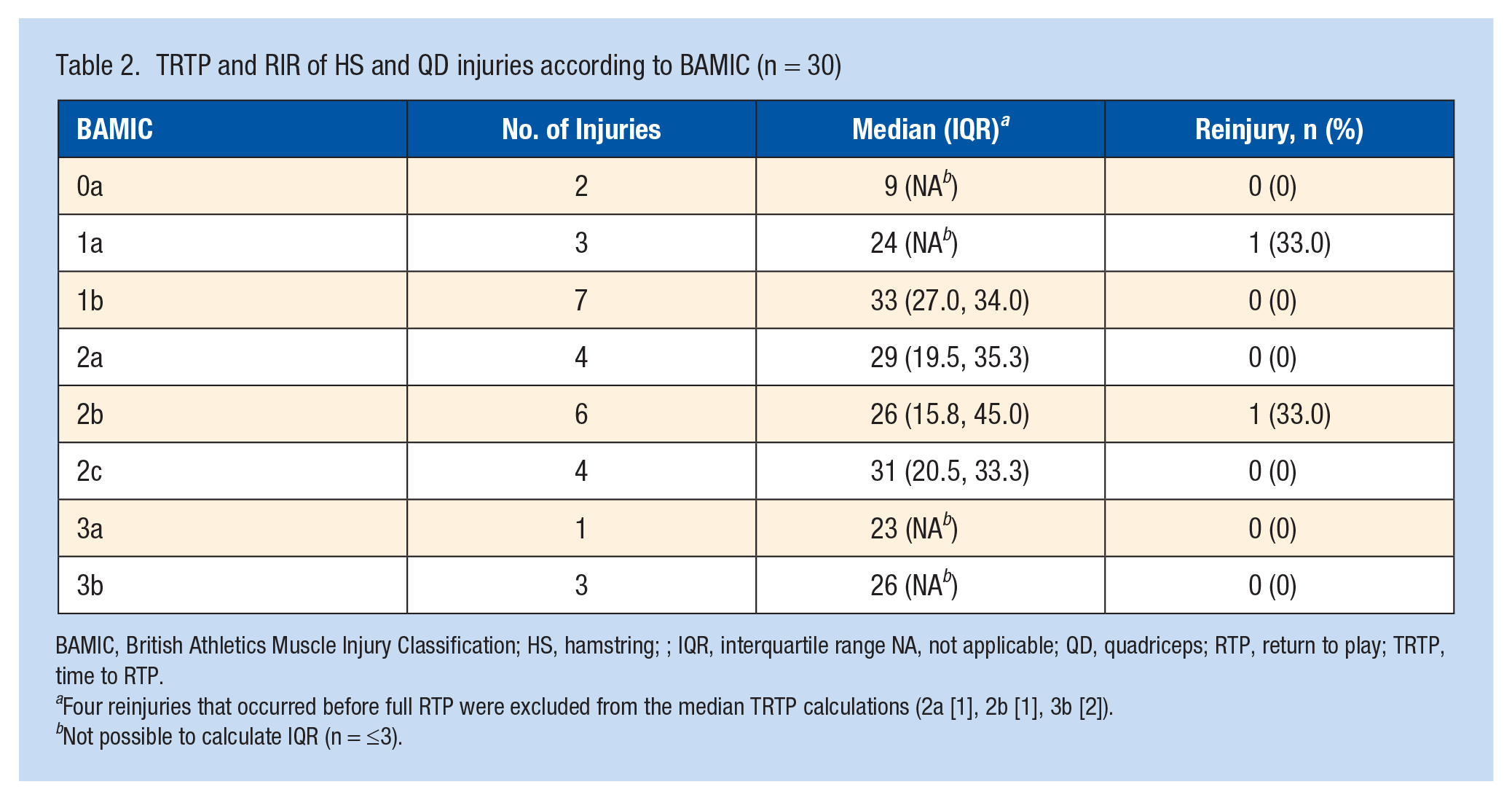
BAMIC, British Athletics Muscle Injury Classification; HS, hamstring; ; IQR, interquartile range NA, not applicable; QD, quadriceps; RTP, return to play; TRTP, time to RTP.
Four reinjuries that occurred before full RTP were excluded from the median TRTP calculations (2a [1], 2b [1], 3b [2]).
Not possible to calculate IQR (n = ≤3).
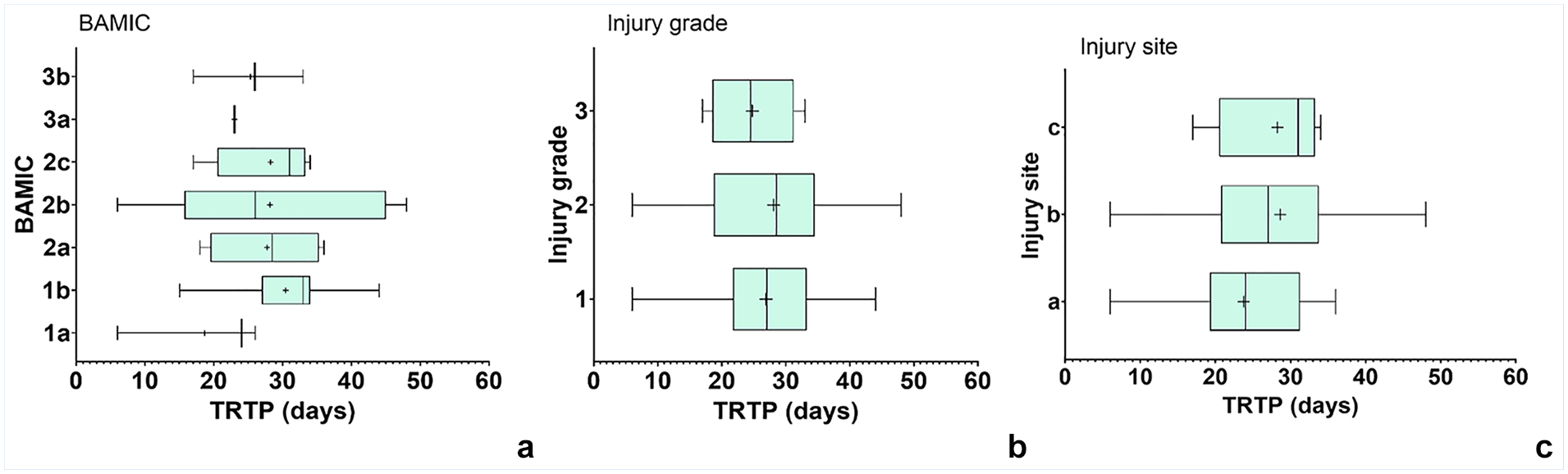
(a) BAMIC and subclassifications of muscle injuries by (b) injury grade and (c) injury site. Data are shown as median (IQR, range) TRTP (days).
Kruskal-Wallis H tests of unique patients showed no statistically significant relationship between TRTP by BAMIC (H = 0.9; P = 0.99; n = 18; ε2 = 0.055), grade (H = 0.6; P = 0.76; n = 18; ε2 = 0.032), or injury site (H = 0.1; P = 0.94; n = 18 ε2 = 0.008) (Table 3). However, TRTP for grade 0 injuries was less compared with grade 1 to 3 injuries, and TRTP was greater for injury site “c” or intratendinous injuries compared with “a” and “b” site injuries (Figure 2).
Comparison of BAMIC and TRTP (n = 18)
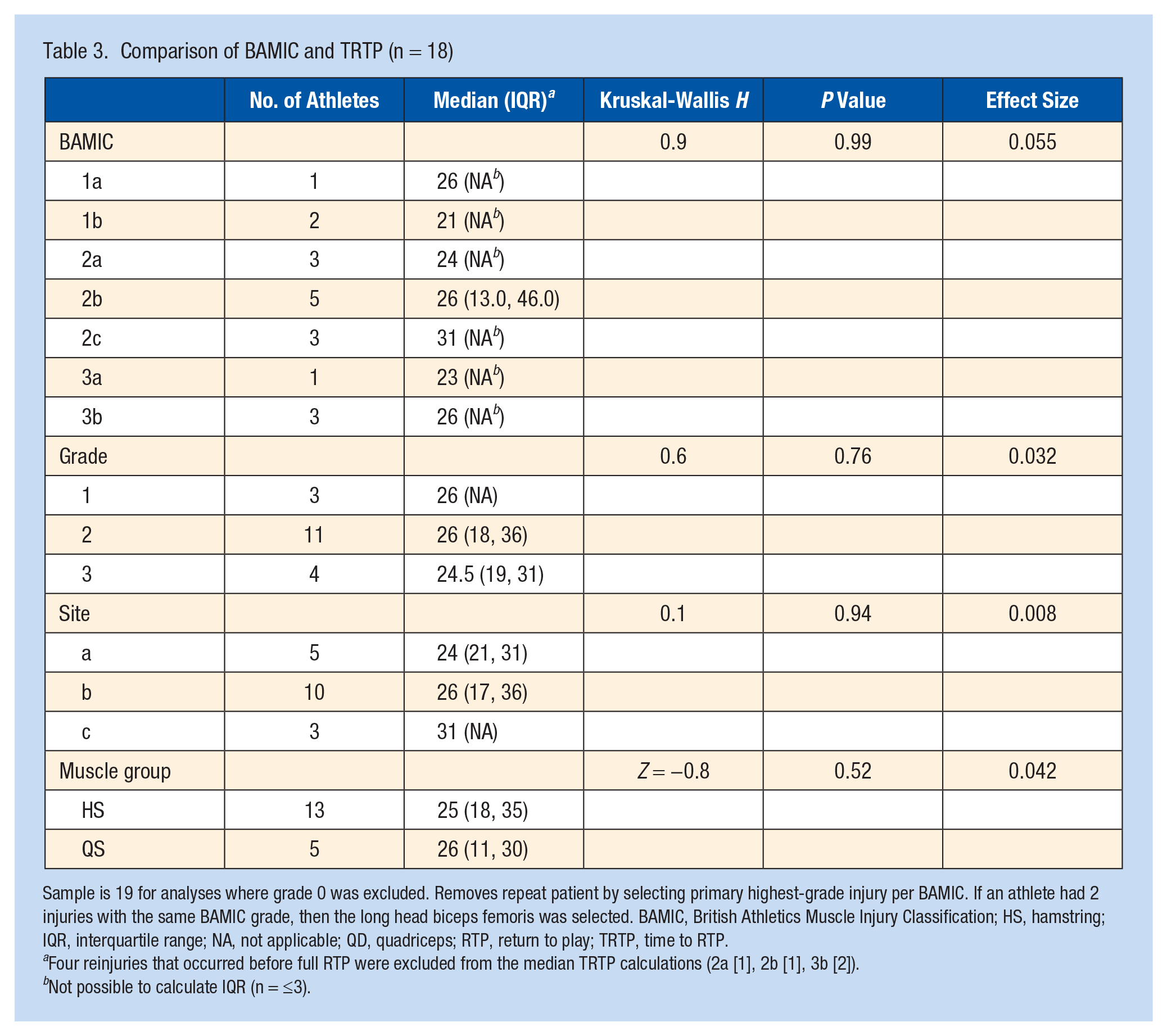
Sample is 19 for analyses where grade 0 was excluded. Removes repeat patient by selecting primary highest-grade injury per BAMIC. If an athlete had 2 injuries with the same BAMIC grade, then the long head biceps femoris was selected. BAMIC, British Athletics Muscle Injury Classification; HS, hamstring; IQR, interquartile range; NA, not applicable; QD, quadriceps; RTP, return to play; TRTP, time to RTP.
Four reinjuries that occurred before full RTP were excluded from the median TRTP calculations (2a [1], 2b [1], 3b [2]).
Not possible to calculate IQR (n = ≤3).
There was no association between median TRTP for HS (n = 15) versus QD injuries (n = 5) (Z = −0.7; P = 0.48; ε2 = 0.042) (Table 3). Separate linear regression analyses revealed no significant association between injury site (B = 1.3, confidence interval [CI], –7.1 to 9.7; P = 0.75; β = 0.083) or grade (B = 0.3; CI, –8.6 to 9.2; P = 0.95; β = 0.017) and TRTP when controlling for age. Likewise, there was no significant association between injury site (B = 1.4; CI, –6.7 to 9.6; P = 0.72; β = 0.091) or grade (B = 0.4; CI, –8.2 to 9.1; P = 0.91; β = 0.027) and TRTP when controlling for muscle group.
Association Between RIR, BAMIC, and Muscle Group
The summary of reinjuries is reported in Figure 3. Most (75.0%) reinjuries occurred before RTP, were grade 2, and were “b” site injuries. The median number of days between the index injury and the reinjury for athletes who suffered a reinjury before returning to play was 25 days (range, 20-46 days) and for athletes who suffered a reinjury after returning to play was 120 days. The median TRTP for reinjury status are presented in Figure 4. We were unable to assess the statistical significance between BAMIC, grade, or injury site and RIR due to the low number of reinjuries.
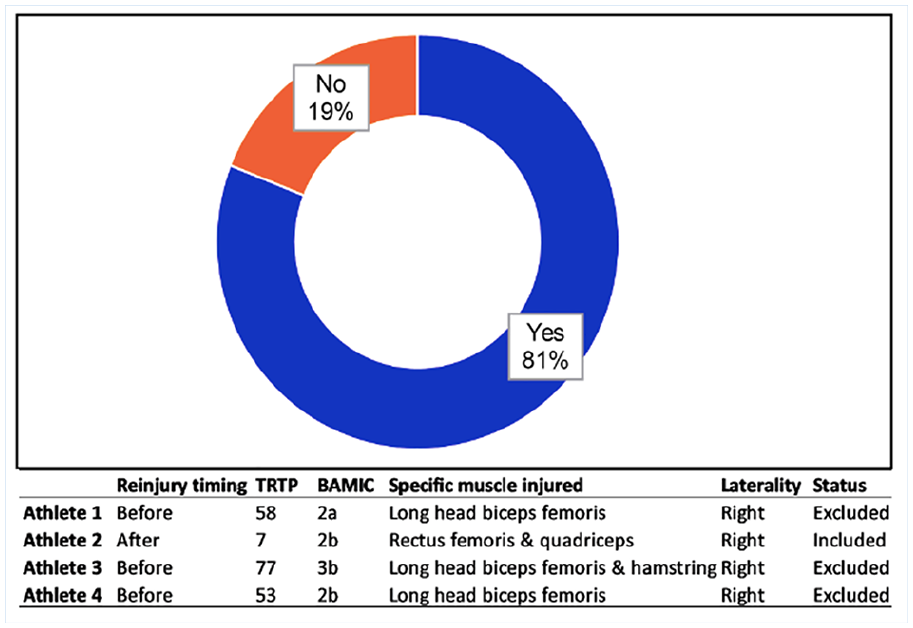
Summary of reinjuries among athletes.
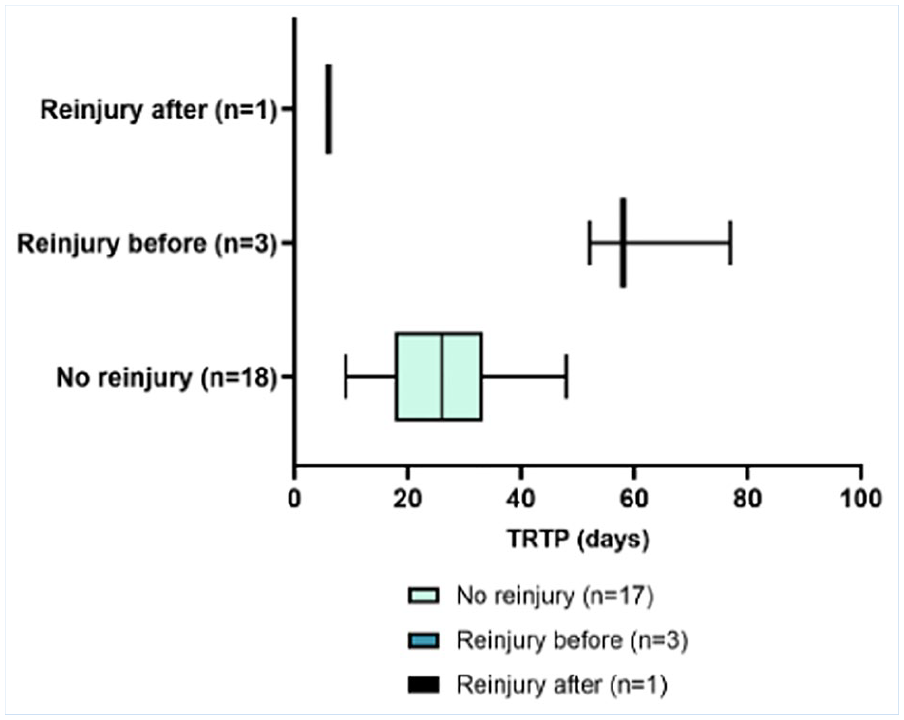
Median (IQR, range) TRTP (days) to return to play by reinjury status.
Discussion
Summary of Principal Findings
This study substantiated that activity-related HS and QD tears are common in American football college athletes, particularly in practice and preseason, and lead to considerable time lost to participation. There was no statistically significant relationship or meaningful effect sizes between BAMIC or muscle group and TRTP. Similarly, BAMIC grade and injury site lacked significance and meaningful effect sizes. However, upon visual inspection, there was greater TRTP for injury site “c” or intratendinous injuries compared with “a” and “b” injuries and TRTP was less for grade 0 injuries compared with grade 1 to 3 injuries. Most athletes missed about 4 weeks of play, irrespective of BAMIC, albeit with nearly 1 in 5 athletes suffering a reinjury. The low number of reinjuries precluded assessment for a relationship between BAMIC and RIR. Next, we will discuss the findings related to BAMIC, including TRTP, RIR, and muscle characteristics identified in this study in further detail.
BAMIC and TRTP
A significant relationship has been identified between BAMIC grade and TRTP, indicating that injuries of increasing grade have longer TRTP.20,24,25,29 Specifically, BAMIC grade 0 injuries, also considered MRI “negative” injuries, are associated with shorter TRTP.6,17,24 The athlete in this study who sustained a grade 0 injury had a TRTP of 9 days, aligning with previous data and clinically resulting in significantly fewer missed games than the TRTP for the remaining athletes in this study. Yet, there was no statistically significant relationship between BAMIC and TRTP in this study.
Compared with muscle belly/myotendinous junction injuries (BAMIC injury site “b”), myofascial injuries (BAMIC injury site “a”) have demonstrated the shortest TRTP, whereas intratendinous injuries (BAMIC injury site “c”) have shown the longest TRTP.17,24-26 This study revealed greater TRTP for injury site “c” injuries, with a mean TRTP of 31 days (range, 21-33 days), compared with shorter TRTP for injury site “a” injuries, with a mean TRTP of 24 days (range, 19-31 days). Clinically, this difference in TRTP between injury site “a” and “c” injuries in this study represents the variance of missing an additional game. However, the practical significance of these findings is limited due to the small effect sizes in this study.
BAMIC and RIR
Due to the low number of reinjuries in this study, the sample size precluded assessment of the relationship between BAMIC and RIR. For the athletes who suffered a reinjury after returning to play, the injury involved the QD and were classified as 1a and 2b. For the athletes who experienced a reinjury before returning to play, all involved the HS and were classified as 2a (n = 1), 2b (n = 1), and 3b (n = 2). However, previous studies suggest a relationship between BAMIC and RIR, ie, that increasing BAMIC grade and injury site “c” injuries have been associated with a greater risk of reinjury.18,25,28
Muscle Injury Characteristics
There was no difference in TRTP for HS and QD injuries in this study (P = 0.48). Comparably, a study of HS injuries and QD injuries in NFL athletes found similar recovery times, 12 although the median TRTP for BAMIC grade 1 to 3 injuries in this study was approximately twice that reported by Herzog et al, 12 possibly due to the low number of BAMIC grade 0 injuries in this study. Also, when controlling for age or muscle group (ie, HS or QD), there was no association between BAMIC and TRTP. Although these findings may have been expected due to the lack of overall significance for BAMIC and TRTP, the potential difference in TRTP between HS and QD injuries as predicted by BAMIC remains relevant given the prevalence of HS and QD injures in football.
Limitations
Our study cohort represented a small number of HS and QD injuries in 1 NCAA-DI college football team. A limitation to this study is the sample size and inherent underpowering, particularly the lack of a sufficient number of injuries in each BAMIC category, which limits the definitive ability to establish conclusions. Primarily, there was 1 grade 0 injury and zero grade 4 injuries. In addition, there were an insufficient number of reinjuries to assess for significance between BAMIC and RIR. Due to the significant burden of lower extremity muscle injuries and the limited ability of current muscle injury classification and grading systems to accurately predict clinical outcomes including TRTP and RIR, further studies with larger sample sizes are necessitated. Previous authors have called for a multiteam, multileague approach to increase the sample size of studies evaluating lower extremity muscle injuries in athletes.18,28 Given the frequency of lower extremity muscle injuries in football and college athletes, a similar approach in these populations could be considered. Because the team medical staff was not blinded to the BAMIC of an athlete’s injury when making rehabilitation and RTP decisions, this presents a potential source of bias. Finally, patient care is not based solely on imaging. Although this study describes the prognostic value of an imaging classification, it is important to recognize that a patient’s physical examination is equally crucial in the overall clinical decision-making process.
Conclusion
This is the first appraisal of BAMIC in college and American football athletes. The notable prevalence of muscle tears in our cohort highlights the need for prevention, particularly in the preseason and early in the regular season. Although BAMIC lacked clinical value in this study, the lack of enough injuries in each category limits our findings. Future studies are needed to assess the value of BAMIC in college and football athletes.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Accessibility Statement
All data are available as requested through the study principal investigator.