
Abstract
Context:
Muscle injury classification and grading systems have been reported for >100 years; yet it offer limited evidence relating the clinical or radiological qualities of a muscle injury to the pathology or clinical outcome. The British Athletics Muscle Injury Classification (BAMIC) incorporates recent predictive features of muscle injuries and provides a precise radiographic framework for clinical prediction and management.
Objective:
To investigate clinical outcomes, particularly time to return to play (RTP), reinjury rate (RIR), and prognostic value of specific magnetic resonance imaging (MRI) findings, of activity-related muscle injuries (tears) in athletes after application of the BAMIC.
Data Sources:
A search of PubMed (NLM), EMBASE (Ovid), Web of Science (Clarivate), Cochrane Library (Wiley), and ClinicalTrials.gov from the inception date of each database through August 31, 2022, was conducted. Keywords included the BAMIC.
Study Selection:
All English language studies evaluating clinical outcomes of RTP and RIR after activity-related muscle injuries and where BAMIC was applied were included. A total of 136 articles were identified, and 11 studies met inclusion criteria.
Study Design:
Systematic review (PROSPERO: CRD42022353801).
Level of Evidence:
Level 2.
Data Extraction:
Two reviewers independently screened studies for eligibility and extracted data. Methodological quality of included study was assessed independently by 2 reviewers with the Newcastle-Ottawa Quality Scale (NOS); 11 good quality studies (4 prospective cohort studies, 7 retrospective cohort studies) with 468 athletes (57 female) and 574 muscle injuries were included.
Results:
All studies reported a statistically significant relationship between BAMIC grade, BAMIC injury site, and/or combined BAMIC grade and injury site with RTP. A statistically significant increased RIR was reported by BAMIC grade and BAMIC injury site in 2 of 4 and 3 of 4 studies, respectively. The prognostic value of individual MRI criteria was limited.
Conclusion:
Consistent evidence suggests that BAMIC offers prognostic and therapeutic guidance for clinical outcomes, particularly RTP and RIR, after activity-related muscle injuries in athletes that may be superior to previous muscle injury classification and grading systems.
Keywords
Muscle injuries (tears), also known as “muscle strains,” are common injuries in sports and lead to considerable time lost from participation.14,16,35 Muscle injuries account for approximately 30% of soccer and 48% of track and field activity-related injuries.2,14 Hamstring muscle injuries are the most common muscle injury in soccer athletes and account for approximately 90 days missed per club per season in professional soccer.2,51 Muscle injury classification and grading systems are important because they may provide therapeutic and prognostic guidance for medical providers, coaches, and athletes. The historical 3-grade muscle injury system is the system used most frequently. 18 In this system, a grade 1 or “mild” injury is described as stretching or minimal disruption of muscle fibers with a clinical presentation of minimal, localized pain, and minor disability; a grade 2 or “moderate” injury is described as tearing of a greater number of muscle fibers but without complete rupture with a clinical presentation of moderate, poorly localized pain, and moderate disability; and a grade 3 or “severe” injury is described as a complete muscle rupture with a clinical presentation of severe disability. 18 There are significant limitations to the historical 3-grade muscle injury system as it lacks consistent terminology, has limited ability to correlate magnetic resonance imaging (MRI) findings with prognosis, including return to play (RTP) and reinjury rate (RIR), and it has minimal inclusion of findings that provide prognostic value (ie, cross-sectional area of muscle tear, craniocaudal length of muscle tear, MRI-“negative” injuries, cross-sectional area of edema, tendon involvement and/or retraction).4,9-11,15,17,18,21,31,33,34,36,42,45,47,48
In 2014, the British Athletics Medical Team developed the British Athletics Muscle Injury Classification (BAMIC) based on specific diagnostic MRI criteria to both predict clinical outcomes and guide rehabilitation after an activity-related muscle injury (Figure 1).35,37 Since BAMIC’s publication, studies have shown statistically significant findings for BAMIC and RTP, as well as BAMIC and RIR.7,24,25,27,33,34,36,37,43,46,49 Furthermore, studies have also reported favorable and potentially faster RTP and lower RIR when using BAMIC-guided rehabilitation protocols.23,36 The objective of this systematic review was to assess clinical prognostic outcomes, including RTP, RIR, and prognostic value of specific MRI criteria, of activity-related muscle injuries in athletes after application of BAMIC.
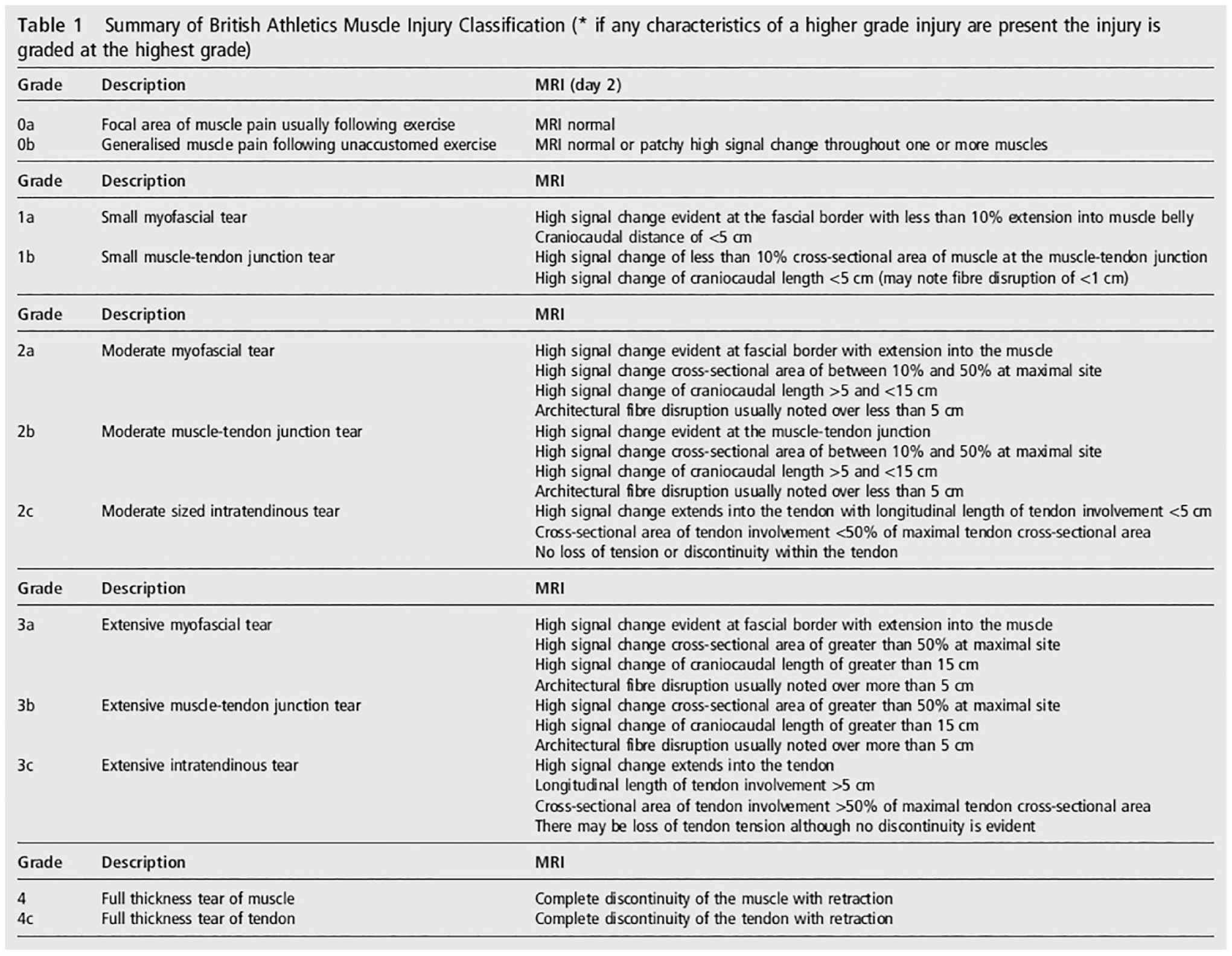
The British Athletics Muscle Injury Classification. Reprinted from Pollock et al. 37
Methods
Information Sources and Search Strategy
This review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and with the implementing PRISMA in Exercise, Rehabilitation, Sport Medicine, and Sports Science (PERSiST) guidelines.3,29 A comprehensive search was conducted in PubMed (NLM), EMBASE (Ovid), Web of Science (Clarivate), Cochrane Library (Wiley), and ClinicalTrials.gov by a health sciences research librarian. The study protocol was prospectively registered at PROSPERO (ID CRD42022353801). Phrase searching was done to find studies that used BAMIC. 35 There were no restrictions on publication date or language applied to the search. The full database search strategies are in Appendix 1 (available in the online version of this article). Database searches were initially conducted on August 9, 2022. Database searches were then repeated after completion of initial title and abstract screening and then again before starting data extraction to find new publications.
Study Selection
Abstract and full-text screening was done using Covidence systematic review software. 1 Two reviewers independently evaluated citations identified using the searches described above. When the title or abstract identified use of BAMIC, it was included and moved onto the second stage of screening. The second stage consisted of both reviewers independently reviewing all full-text articles meeting initial screening for inclusion and selecting articles that met all study inclusion criteria. Disagreements between team members were resolved by a senior author independent of initial review until consensus was met on all article exclusions and inclusions.
Articles were included if all the following conditions were met: (1) activity-related muscle injury, (2) BAMIC applied to the muscle injury, and (3) clinical outcomes were evaluated after application of BAMIC. Articles were excluded if any of the following conditions were met: (1) nonactivity-related muscle injury (tear); (2) BAMIC was not applied; (3) studies were basic science, biomechanical, or descriptive anatomy/cadaveric; (4) abstract and/or full text had insufficient methodological or results reporting; or (5) non-English publication language. See Figure 2 for the study flowchart showing the stages of identification to final inclusion.
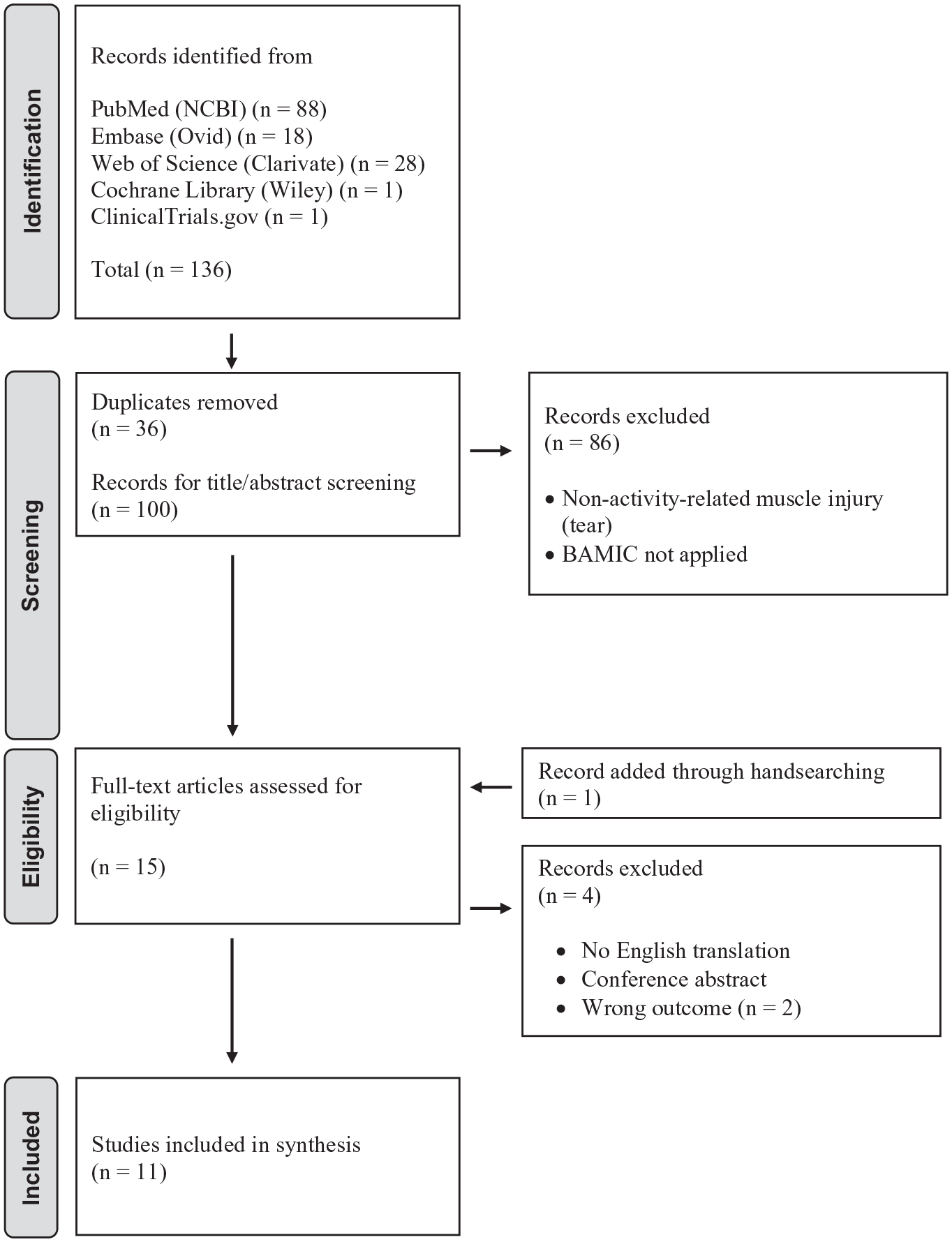
Flowchart for systematic review using PRISMA guidelines. 29 BAMIC, British Athletics Muscle Injury Classification; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Collection and Synthesis
Data extraction for the full text of articles that met inclusion criteria was performed independently by 2 reviewers to limit bias; and afterward the reviewers compared all data extracted for uniformity. Data extraction was completed using a specifically designed and standardized data extraction form (see study protocol) in Covidence systematic review software. 1 Consensus was then reached through discussion between those doing the extraction for all final data to be used in synthesis.
When available, we extracted general study information, number of participants, age, sex, sport, level of competition, muscle injured, hamstring muscle(s) affected, quadriceps muscle affected, injured during training or competition, activity during which injury occurred, location of injury (proximal/central/distal), length of muscle edema on MRI scan, cross-sectional area of muscle edema on MRI scan, length of architecture fiber disruption on MRI scan, cross-sectional area of tendon injury on MRI scan, longitudinal length of tendon injury on MRI scan, loss of tendon tension on MRI scan, BAMIC grade (0-4), BAMIC injury site (a-c), RTP in days, RIR number and/or in days, the number of athletes who sustained a reinjury, and ability to return to previous level of play (see Online Appendix 2 for data extraction form). If authors did not report relevant data in the text, we extracted data from tables when present. When data were not reported in text or table format, authors were contacted. No additional data were received from contacted authors.
Due to study, BAMIC criteria, and outcome heterogeneity, meta-analysis of data and subsequent formal certainty assessments were not performed. Summary data from individual studies were analyzed qualitatively and reported.
Quality Assessments
The quality of studies was independently assessed by 2 reviewers using the Newcastle-Ottawa Quality Scale (NOS), which is a validated scale used to assess the quality of nonrandomized studies. 50 The NOS consists of 3 domains: (1) the selection of study groups, (2) the comparability of study groups, and (3) the assessment of exposure or outcomes. 50 We assigned points if the studies met related criteria. Studies with total scores of 0 to 3, 4 to 6, and 7 to 9 were considered as poor, fair, and good quality, respectively. 50
Results
Study Selection
The flow of studies through the search and selection process is presented in Figure 2. A total of 136 articles were initially identified. Based on the title and abstract screening, 122 articles were excluded due to duplication, nonactivity related muscle injury, or lack of BAMIC application. One article was identified to meet inclusion criteria by hand-searching. Of the 15 full-text articles assessed for eligibility, 2 studies were excluded due to assessing the wrong outcome, 1 study for non-English language, and 1 study for lack of full text (unable to be obtained by a medical librarian).6,23,40,41 A total of 11 studies ultimately met the inclusion criteria for this systematic review (n = 136).7,24,25,27,33,34,36,37,43,46,49
General Characteristics of Included Studies
The main characteristics of the included studies are summarized in Table 1. Of the 11 included studies, there were 4 prospective cohort studies and 7 retrospective cohort studies. Studies were from the United Kingdom (7), Italy (2), Spain (1), and Norway (1). The minimum mean athlete age was 23.8 years, and the maximum mean athlete age was 27.4 years. Three studies included female participants. Nine studies included soccer athletes and 3 studies included track and field athletes. Analyses of BAMIC grade, injury site, and/or combined grade and injury site, and clinical outcomes were assessed in a variety of ways including correlation, multivariable regression, t tests, and analysis of variance across all studies.
Main characteristics of the included studies
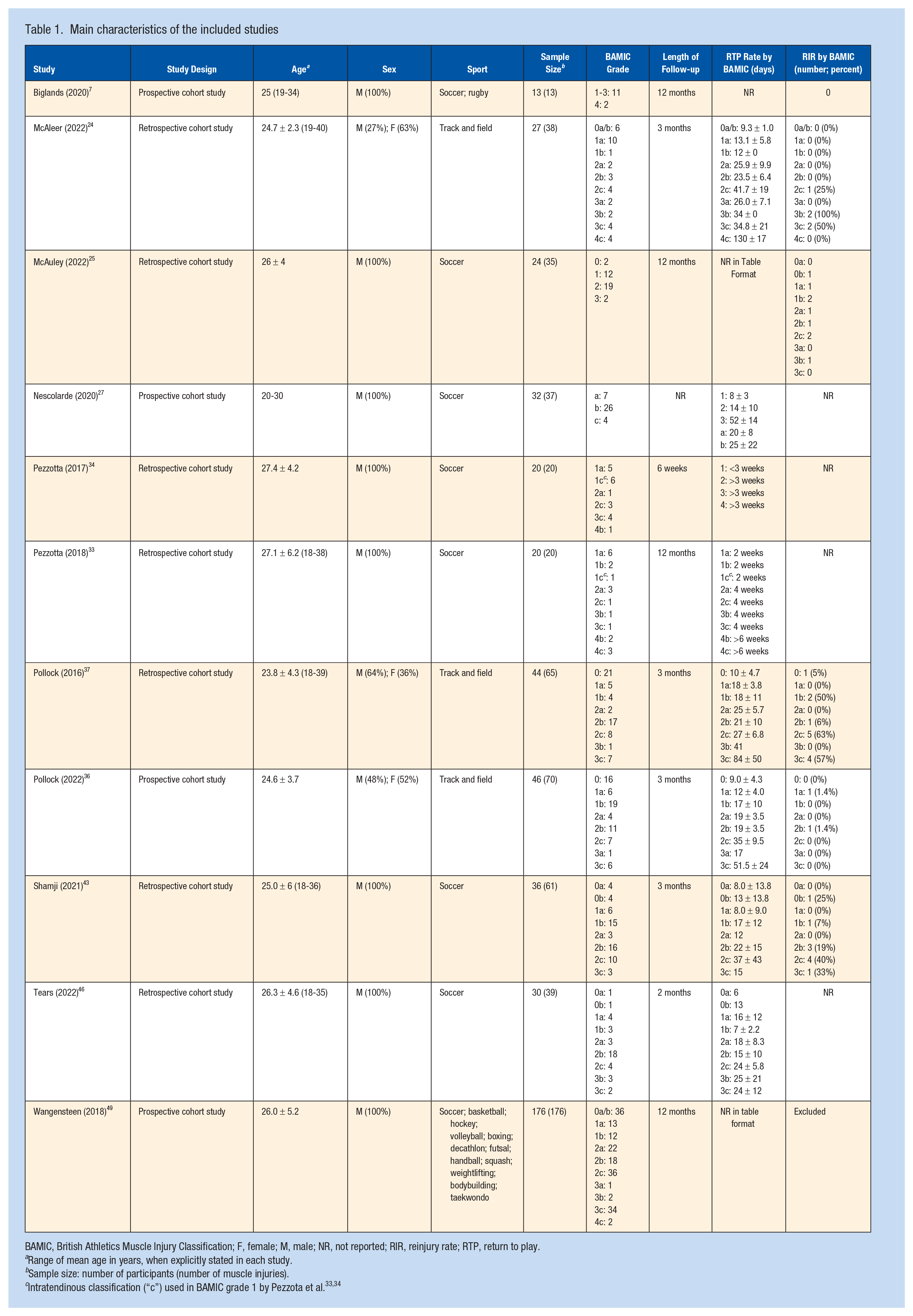
BAMIC, British Athletics Muscle Injury Classification; F, female; M, male; NR, not reported; RIR, reinjury rate; RTP, return to play.
Range of mean age in years, when explicitly stated in each study.
Sample size: number of participants (number of muscle injuries).
Risk of Bias Within Studies
Evaluation of manuscript quality was conducted on the 11 studies that satisfied the study inclusion criteria. Based on quality assessment of NOS performed independently by 2 reviewers, all 11 studies were good quality.7,24,25,27,33,34,36,37,43,46,49 Zero studies were rated poor or fair quality.
Description of Muscle Injuries
The description of muscle injuries is summarized in Table 2. All 11 studies included professional athletes. There were 468 total athletes (57 female) and 574 total muscle injuries. The number of athletes per study and number of muscle injuries per study both ranged from 13 to 176. As reported, total number of muscle injuries included in this systematic review: BAMIC grade (0a: 5, 0b: 7, 1a: 55, 1b: 56, 1c: 7, 2a: 40, 2b: 82, 2c: 73, 3a: 4, 3b: 9, 3c: 61, 4a: 0, 4b: 3, 4c: 9), grade (0: 91, 1: 141, 2: 263, 3: 84, 4: 14), and injury site (a: 151, b: 182, c: 151). Length of follow-up after initial activity-related muscle injury ranged from 6 weeks to 12 months.
Main characteristics of the BAMIC injury data
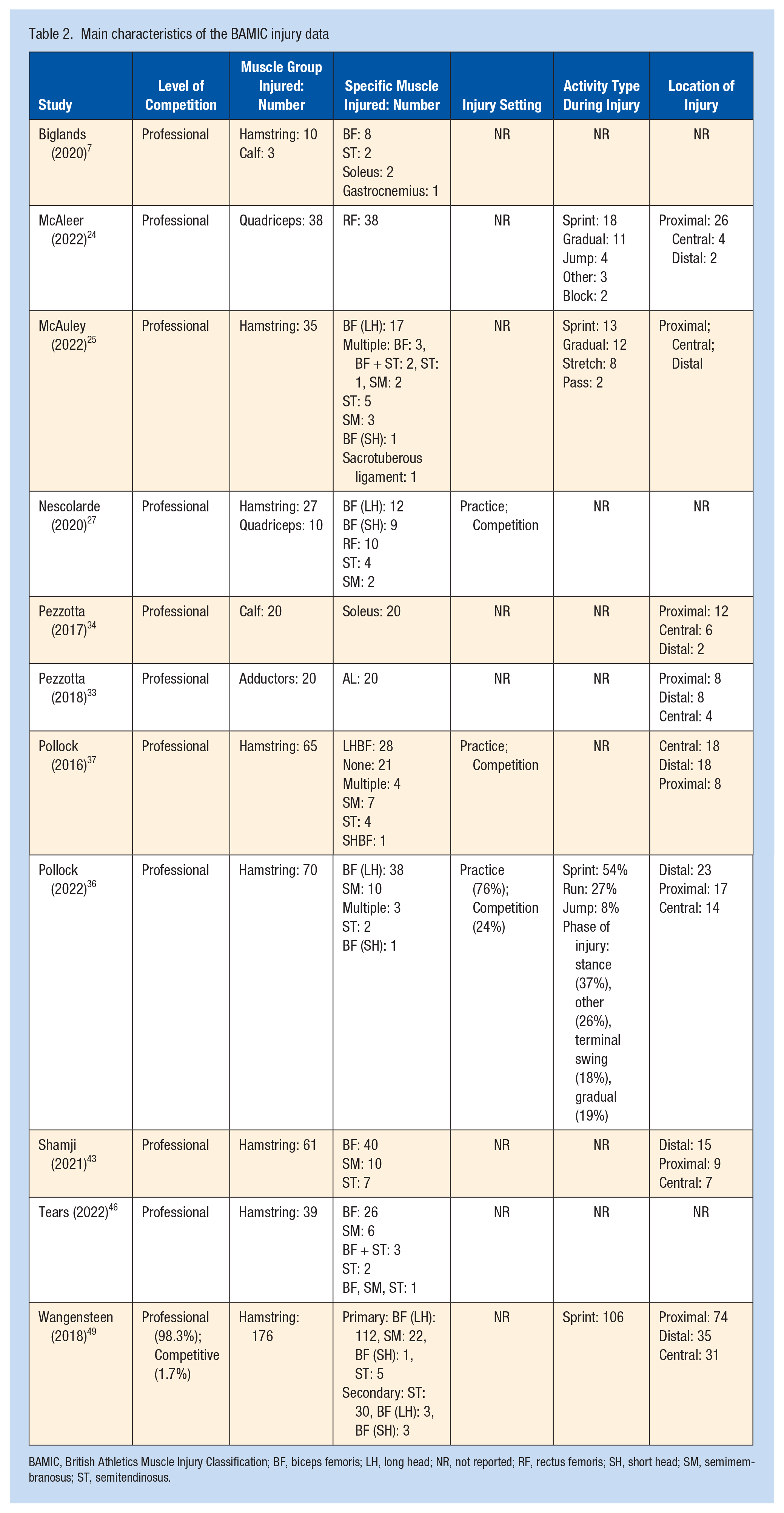
BAMIC, British Athletics Muscle Injury Classification; BF, biceps femoris; LH, long head; NR, not reported; RF, rectus femoris; SH, short head; SM, semimembranosus; ST, semitendinosus.
Eight studies reported hamstring injuries, 2 reported calf injuries, 2 reported quadricep injuries, and 1 reported adductor injuries. Hamstring injuries were reported in the semimembranosus (n = 63), semitendinosus (n = 68), and biceps femoris (n = 297). When reported for injuries of the BF, injuries occurred in the short head of the BF (n = 16) and long head of the BF (n = 200). Quadriceps injuries were reported in the rectus femorus is (n = 48), and calf injuries were reported in the gastrocnemius (n = 1) and soleus (n = 22). While injuries occurred during both practice and competition, most injuries occurred either during sprinting/running or had a gradual onset. When cranial-caudal location of injury was reported, injuries occurred in central (n = 82), distal (n = 103), and proximal (n = 154) muscle bellies.
BAMIC MRI Description of Muscle Injury and Prognostic Value
The MRI descriptions of muscle injuries and prognostic variables are summarized in Table 3. Most studies did not evaluate specific BAMIC MRI criteria for RTP. No studies reported analysis of specific BAMIC MRI criteria for RIR. MRI scan features associated with RTP included length of muscle fiber disruption or gap,33,34 cross-sectional area of tendon injury, 36 and loss of tendon tension. 36 While 2 studies reported that the length of muscle edema was associated with RTP,34,36 2 studies reported that it was not.33,46 While 1 study reported that the cross-sectional area of muscle edema was associated with RTP, 36 1 study reported that it was not. 46 Moreover, 1 study reported that longitudinal length of tendon injury was not associated with RTP. 36
Prognostic value of specific BAMIC MRI criteria and RTP
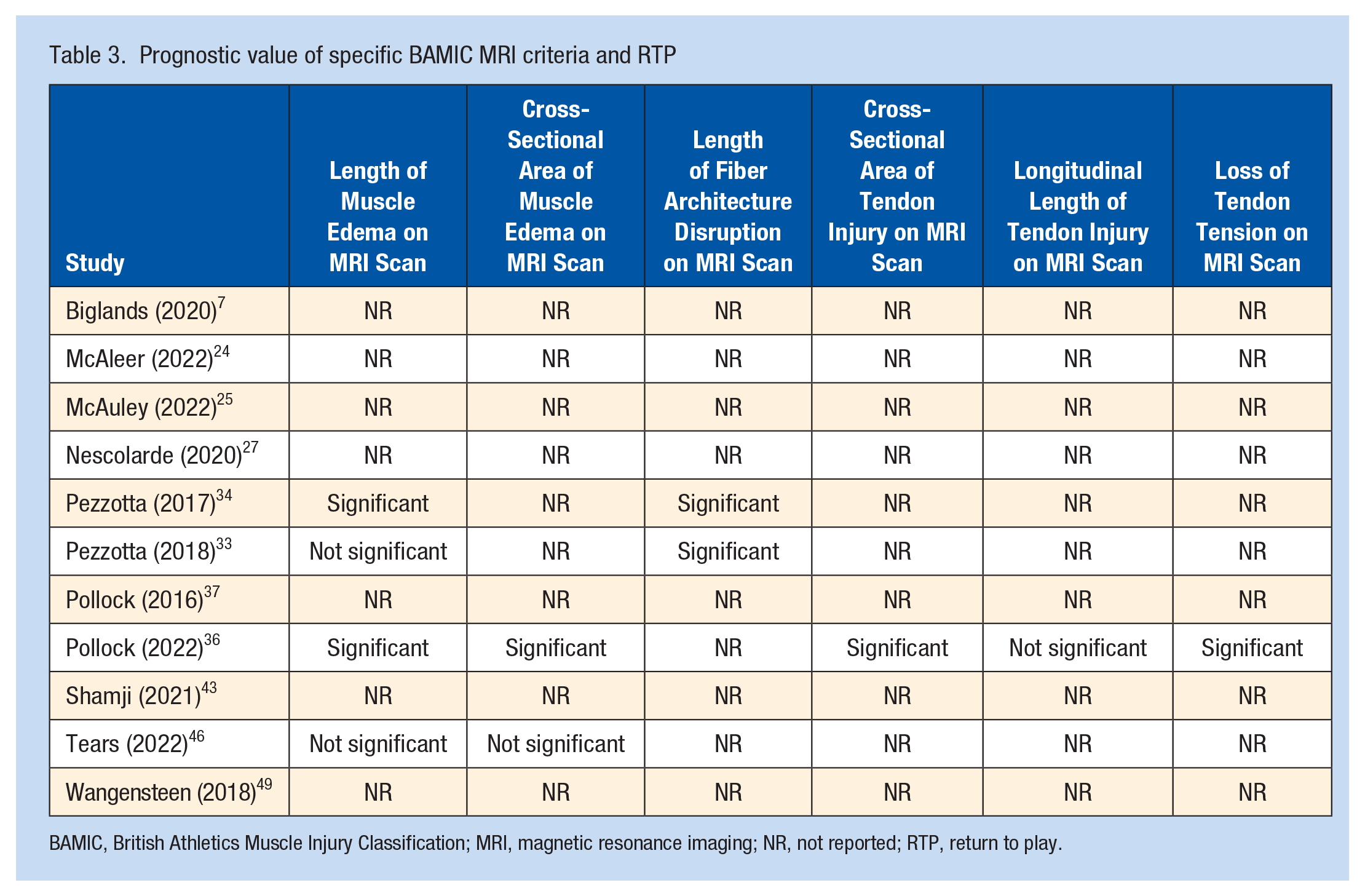
BAMIC, British Athletics Muscle Injury Classification; MRI, magnetic resonance imaging; NR, not reported; RTP, return to play.
BAMIC Grade/Injury Site RTP, RIR, and Return to Previous Level of Play
Evidence for the BAMIC grade and injury site for RTP, RIR, and return to previous level of play are summarized in Table 4.
Summary findings of individual studies on the relationship between RTP, RIR, and BAMIC grade and injury site
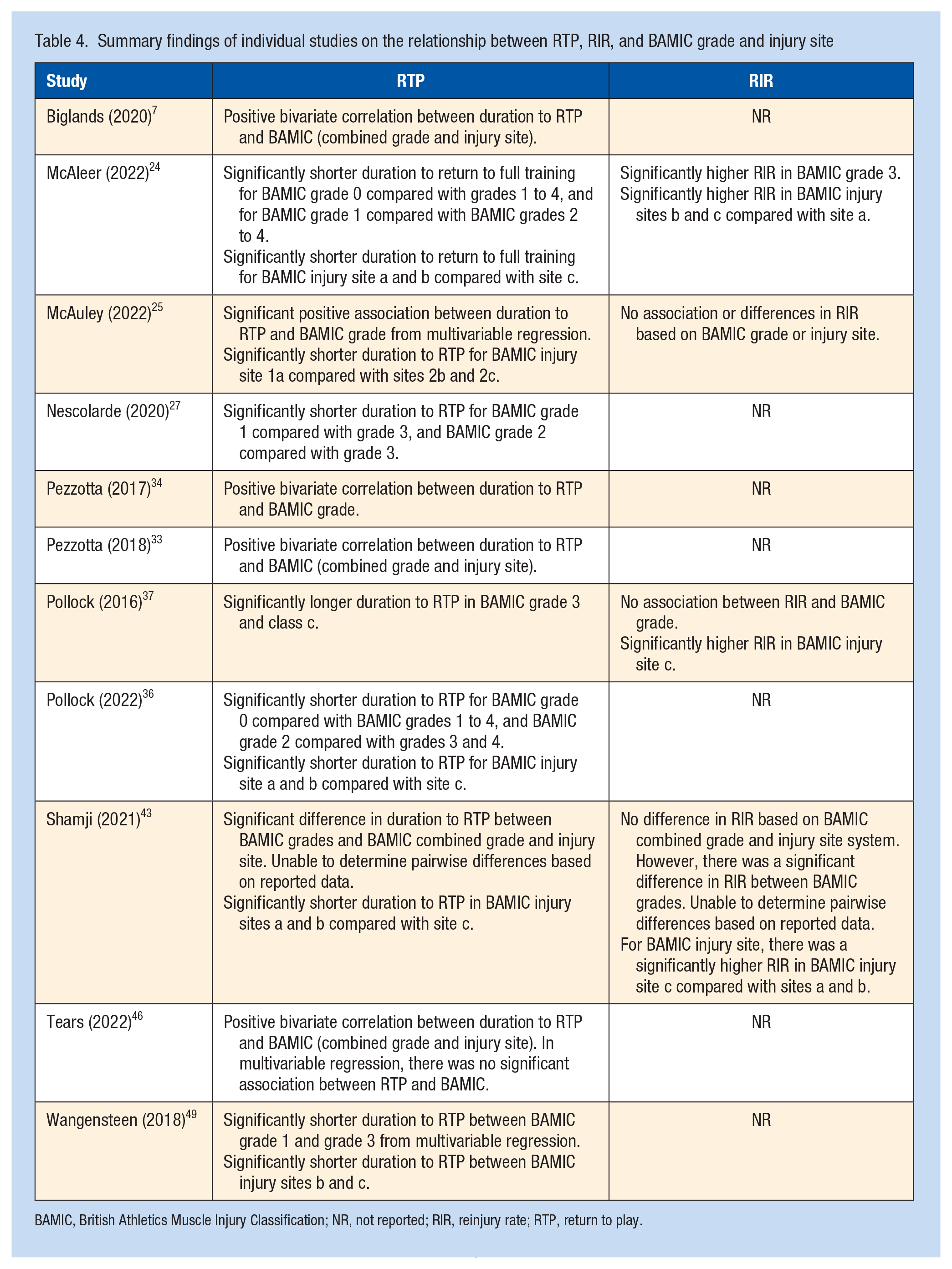
BAMIC, British Athletics Muscle Injury Classification; NR, not reported; RIR, reinjury rate; RTP, return to play.
BAMIC and RTP
All studies reported RTP. While all studies analyzed RTP by BAMIC grade, 3 studies combined BAMIC grade and injury site when reporting RTP outcomes. A significant relationship between BAMIC grade and RTP was found in all studies that analyzed RTP by BAMIC grade or by combined BAMIC grade and injury site. While 1 study revealed a positive bivariate correlation between RTP and BAMIC (combined grade and injury site), multivariable regression displayed no relationship between RTP and BAMIC grade. 46 Moreover, 9 studies analyzed RTP by BAMIC injury site, and 3 of these studies combined BAMIC grade and injury site when reporting RTP. A significant relationship between BAMIC injury site and RTP was found in all studies that analyzed RTP by BAMIC injury site or combined BAMIC grade and injury site.
Although BAMIC grade demonstrated a significant relationship with RTP, individual studies reported variation in RTP significance by BAMIC grade. One study reported that while BAMIC grade 3 injuries had statistically significant longer RTP, there was no difference in RTP between grade 1 and 2 injuries. 37 Another study reported that, whereas there was a statistically significant shorter RTP for BAMIC grade 0 injuries versus grades 1, 2, or 3 injuries, and for BAMIC grade 1 injuries versus grades 2 or 3 injuries, there was no statistically significant difference for RTP between BAMIC grade 2 and 3 injuries. 36 In addition, another study reported that while there was a statistically significant shorter RTP for BAMIC grade 1 versus 3 injuries, there was no statistically significant difference for RTP between BAMIC grade 1 versus 2 or grade 2 versus 3 injuries. 49 Lastly, 1 study reported statistically significant longer RTP with BAMIC grade 1b versus 3b injuries and BAMIC grade 2b versus 3b injuries. 27
For BAMIC injury site, 1 study reported no difference in RTP between muscle tears with and without intratendinous involvement of the same size, ie, “b” versus “c” injuries. 25 All additional studies that individually analyzed BAMIC injury site identified a statistically significant increased RTP for “c” injuries and no statistically significant difference in RTP for “a” versus “b” injuries.36,37,43,49
Overall, consistent evidence suggests that BAMIC grade and injury site may better guide sports medicine clinicians regarding RTP prognosis and potentially therapeutic management of activity-related muscle injuries compared with previously published muscle injury classifications.
BAMIC and RIR
Seven of the included studies reported RIR,7,24,25,34,36,37,43 and 4 studies (4 retrospective cohort studies) analyzed RIR by BAMIC.24,25,37,43 Overall, RIR was 13.5% (38 of 282 muscle injuries). RIR by BAMIC grade and injury site was variable and study dependent. An increased RIR was found for higher BAMIC grade injuries (2 of 4 studies), and by BAMIC injury site, ie, highest RIR reported in “c,” “b,” and “a” injuries (3 of 4 studies), respectively.24,25,37,43 Furthermore, 1 study reported that BAMIC grade 0 to 1 reflected 89% of the RIR and most RIR occurred <2 months after RTP. 25 The same study also reported that, whereas BAMIC grade and injury site did not influence RIR, there was a higher adjusted odds ratio (OR) of RIR for previous hamstring injury (OR, 1.16), experiencing the hamstring injury during sprinting (OR, 31.1), during a pass (OR, 5.38) or stretching (OR, 1.96), and number of days of pain during ambulation (OR, 2.18). 25 Another study reported that, whereas there was a statistically significant increase in RIR for increasing BAMIC grade, there was no difference in RIR based on combined BAMIC grade and injury site. 43 Lastly, 1 study reported that BAMIC grade 1 injuries are without any reinjury risk. 34
Overall, limited evidence suggests that BAMIC grade, injury site, and/or combined grade and injury site may guide sports medicine clinicians regarding prognostic risk of reinjury and potentially therapeutic management to reduce the RIR of activity-related muscle injuries compared with previously published muscle injury classifications.
BAMIC and Return to Previous Level of Play
Of the 8 studies that reported return to previous level of competition, 98.7% (224 of 227) of athletes were able to return to previous level of competition. For the 1.1% (3 of 267) of athletes who did not return to previous level of competition, association with BAMIC grade was not analyzed.
Discussion
Summary of Evidence/Principal Findings
This systematic review assessed the clinical outcomes, particularly RTP and RIR, of activity-related muscle injuries in athletes after application of BAMIC across the entire peer-reviewed literature through August 31, 2022. This systematic review was performed using a reproducible search strategy and a validated tool for methodological quality evaluation. 50 PRISMA and PERSiST guidelines were utilized, and 2 reviewers independently completed study selection, data extraction, and quality assessment.3,29 To the best of our knowledge, no studies have systematically reviewed the emerging volume of literature reporting clinical outcomes of activity-related muscle injuries after application of BAMIC. While most preceding muscle injury classification and grading systems that incorporate clinical and/or radiographic criteria offer limited prognostic validity, the current systematic review suggests that application of BAMIC to activity-related muscle injuries may provide key prognostic value to sports medicine clinicians, particularly regarding both RTP and RIR. 19
Appraisal of Study Methods
The 11 studies that met inclusion criteria in this systematic review are Level of Evidence 1 and 2 for Prognostic Studies and the methodological quality of the included studies as evaluated through the NOS were all rated as good quality.7,24,25,27,33,34,36,37,43,46,49,50 Meta-analysis and subsequent certainty assessment were not performed due to the heterogeneity of both BAMIC data and data analysis methods between studies. Specifically, there were several methods of data investigation across studies including how BAMIC was examined (ie, by BAMIC grade, injury site, or combined grade/injury site) and whether the full range of BAMIC was examined, which limited the ability to effectively compare studies. In addition, the types of analysis differed between studies (ie, univariable versus multivariable, t test versus correlation) which further limited effectively study comparison.
Comparison With Previous Classifications
For prognostic value, medical teams use MRI for muscle injury diagnosis and grading. Although MRI is likely the most sensitive and precise modality to assess muscle injury, initial evidence reported the limited role of MRI in prediction of RTP.11,38 Although muscle injuries were traditionally graded with MRI using the classical 3-grade system, this scale has been disparaged for simplifying muscle injury characteristics,10,15,32,35,49 and its overall prognostic value including RTP is disputed.38,39,49 Newer muscle injury classifications have been proposed that integrate a thorough classification of injury characteristics, such as the Munich Muscle Classification (MMC) and the system proposed by Chan et al.8,26 However, the MMC does not incorporate recent evidence supporting the prognostic value of specific muscle injury MRI findings and it also includes problematic terminology as it divides muscle injuries into “structural” versus “functional” categories.4,10,11,20,21,44 Although the “structural” category has been shown to offer some prognostic benefit, the lack of incorporation of recent MRI evidence suggests that the “structural” category of the MMC does not offer considerable additional benefit than the modified Peetron’s classification.13,26,32 In addition, Chan et al 8 reported an image-based classification defined by the location and type of tissue injury. Admittedly, this classification has numerous limitations as it does not clearly define the limits of each grade nor does it does include MRI scan-“negative” injuries. 8 Contrarily, BAMIC offers a clear diagnostic framework and incorporates recent evidence of the prognostic value for muscle injury site, length, cross-section size, tendon involvement, and “MRI-negative” presentations.4,10,11,20,21,44 Since its description, numerous studies have reported BAMIC’s prognostic value.7,24,25,27,33,34,36,37,43,46,49
BAMIC and RTP
While muscle injury classifications have existed for over 100 years, current classifications offer the sports medicine clinician minimal improvement in prognostic and therapeutic guidance when compared with initial classifications. 19 Furthermore, when specifically evaluating radiographic classification systems other than BAMIC, there is limited evidence to support their prognostic validity. 19 Contrarily, all studies included in this systematic review reported a statistically significant relationship between BAMIC and RTP. The most consistent findings from our review indicate that RTP timing increases as BAMIC grade increases and for injury site “c” injuries compared with “a” or “b” injuries. Specifically, BAMIC grade 0 injuries, also known as MRI- “negative” injuries, are associated with shorter RTP and lower RIR, while BAMIC injury site “c” injuries are associated with longer RTP and higher RIR. Pertinently, tissue healing time estimates for BAMIC injury site “a” injuries have been reported to be up to 3 weeks, with 4 to 8 weeks for “b” injuries and 2 to 4 months for “c” injuries. 23 This invaluable prognostic information can guide sports medicine clinicians with evidence-based data to accurately advise both athletes and athletic staff regarding injury prognosis and prediction of RTP. Furthermore, structured rehabilitation guidelines directed by BAMIC grade and injury site are published. 23 The implementation of these rehabilitation guidelines compared with non-BAMIC-guided RTP timelines has been shown to have favorable and shorter RTP for some hamstring injuries.23,36 Compared with previously published muscle injury classifications, consistent evidence suggests that BAMIC grade and injury site may best guide sports medicine clinicians regarding RTP prognosis and potentially therapeutic management of activity-related muscle injuries.
BAMIC and RIR
RIR is a frequent complication of muscle injury in athletes, with significant performance implications. RIR is common, with previous studies reporting RIR for hamstring injuries ranging from 14% to 63%.12,28,37 Evidence-based tools for clinical prediction of RIR for activity-related muscle injuries are lacking, as clinical examination and previous radiographic muscle injury classifications have provided insufficient prediction of RIR.22,48 Although only 4 studies from this systematic review analyzed BAMIC and RIR, most studies reported a significant relationship. Increasing BAMIC grade was associated with increased RIR in 2 out of 4 studies. BAMIC injury site “c” injuries were associated with increased RIR compared with “a” or “b” injuries in 3 out of 4 studies. The most consistent findings from our review indicate that RIR increases as BAMIC grade increases and for injury site “c” injuries compared with “a” or “b” injuries. Yet, confidence in these results should be tempered because all 4 studies analyzing BAMIC and RIR were retrospective cohort studies. Importantly, structured rehabilitation guidelines directed by BAMIC grade and injury site have resulted in a significantly lower hamstring RIR of 2.9% compared with previously published RIR. Compared with previously published muscle injury classifications, limited evidence suggests that BAMIC grade and injury site may guide sports medicine clinicians regarding prognostic risk of reinjury and potentially therapeutic management to reduce the RIR of activity-related muscle injuries.
BAMIC MRI Features and Value
BAMIC grade is defined by specific MRI scan criteria, including cross-sectional area of muscle edema, craniocaudal length of muscle edema, muscle architecture fiber disruption, longitudinal length of tendon involvement, cross-sectional area of tendon involvement, loss of tendon tension, and complete discontinuity of muscle or tendon with retraction. There is mixed but emerging evidence to support the prognostic value of isolated MRI scan abnormalities in activity-related muscle injuries.19,35,46 In general, “MRI-positive injuries” correlate with longer RTP compared with “MRI-negative” injuries. 13 In addition, previous studies have reported specific MRI abnormalities identified in activity-related muscle injuries that are suggestive of prognostic value, including cross-sectional area of muscle edema, craniocaudal length of muscle edema, tendon involvement, tendon retraction, distance from muscle origin, and estimated muscle volume injured have in limited studies predicted RTP.4,9-11,17,21,31,33,34,36,42,45,47,48 Contrarily, numerous previous studies have reported that specific MRI scan abnormalities do not correlate with RTP.4,5,11,33,36,46
The result of this systematic review offers varied prognostic value of specific MRI abnormalities for RTP, particularly those included in BAMIC. While most studies included in this systematic review did not analyze specific BAMIC MRI abnormality criteria and RTP, the results of studies that did were variable. MRI features associated with RTP included length of muscle fiber disruption or gap,33,34 cross-sectional area of tendon injury, 36 and loss of tendon tension. 36 While 2 studies reported that the length of muscle edema was associated with RTP,34,36 2 studies reported that it was not.33,46 While 1 study reported that the cross-sectional area of muscle edema was associated with RTP, 36 1 study reported that it was not. 46 Moreover, 1 study reported that longitudinal length of tendon injury was not associated with RTP. 36
The primary aim of BAMIC was to develop a muscle injury classification system with prognostic and therapeutic value that incorporates an evidence-based MRI-based precise diagnostic framework. Aptly, a recent study also demonstrated BAMIC’s reliability through intra-rater and inter-rater kappa values with at least substantial agreement in all groups. 30 Our results suggest that, whereas individual MRI abnormalities may provide limited prognostic value, the combination and severity of specific MRI abnormalities characterized by a reliable and precise muscle injury classification system like BAMIC provides increased prognostic value for the sports medicine clinician as compared with previous activity-related muscle injury classification systems.
Limitations
A meta-analysis was not performed due to the heterogeneity of both data and data analysis methods between studies. Future studies are necessary reporting clinical outcomes of BAMIC with a standardized method of analysis of BAMIC grade, injury site, and clinical outcomes. There was also large variation in the patient inclusion criteria between studies. While most participants were professional male athletes, there was a considerable variation of athletic disciplines, predominantly track and field and football, and multiple injured muscle groups, including hamstring, quadriceps, calf, and adductors. Notably, BAMIC was designed initially for hamstring injuries. The limited number of included studies and the heterogeneity of data presentation and investigation in each study in this systematic review may lead to reporting bias. BAMIC recommends that the MRI scan is obtained 24 to 48 hours after the injury occurs. While this time frame is typical for professional athletes, many youth and collegiate athletes often do not undergo an MRI scan until weeks after the injury occurs. Therefore, BAMIC’s external validity and applicability across a broad spectrum of athletes of all levels may be limited to those athletes who undergo MRI in the suggested time frame.
Future Implications
Future studies should investigate the clinical outcomes of activity-related muscle injuries in athletes after application of BAMIC, particularly further definition of the prognostic value of BAMIC grade and injury site. Additional studies are also needed to define the prognostic value of the presence, and severity, of specific MRI abnormalities in muscle injuries. Moreover, standardizing the method of analysis of BAMIC grade, injury site, and clinical outcomes would allow for effective comparison between studies and completion of meta-analysis.
Conclusion
All studies included in this systematic review reported a statistically significant relationship between BAMIC and RTP. When evaluated, most studies reported a statistically significant relationship between BAMIC and RIR. Prognostic value of isolated MRI scan criteria was variable and limited. Consistent evidence suggests that BAMIC may offer the clinician guidance for therapeutic and prognostic management of activity-related muscle injuries in athletes that may be superior to previous muscle injury classifications and grading systems. Future studies should investigate the clinical outcomes of activity-related muscle injuries after application of BAMIC.
Supplemental Material
sj-docx-1-sph-10.1177_19417381231195529 – Supplemental material for Outcomes of Activity-Related Lower Extremity Muscle Tears After Application of the British Athletics Muscle Injury Classification: A Systematic Review
Supplemental material, sj-docx-1-sph-10.1177_19417381231195529 for Outcomes of Activity-Related Lower Extremity Muscle Tears After Application of the British Athletics Muscle Injury Classification: A Systematic Review by William L. Hollabaugh, Alexander Sin, Rachel Lane Walden, Jennifer S. Weaver, Lauren P. Porras, Lance E. LeClere, Ashley R. Karpinos, Rogelio A. Coronado, Andrew J. Gregory and Jaron P. Sullivan in Sports Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.