
Abstract
Background:
Hamstring (HS) strength deficits and imbalances have been identified as risk factors for sustaining anterior cruciate ligament (ACL) injuries and muscular strains, with HS injuries being the most prevalent muscle injuries in soccer athletes. The aim of this study was to investigate HS eccentric strength before and after a soccer match in both male and female soccer athletes.
Hypothesis:
Soccer athletes have changes in eccentric HS strength after a soccer game.
Study Design:
Cohort observational study.
Level of Evidence:
Level 3.
Methods:
HS eccentric strength (mean and absolute peak torque and total work) was measured in 64 healthy male and female competitive football athletes (14-25 years) with an automatic device during the execution of the Nordic hamstring exercise (NHE) test before and after a 90-minute soccer match. The anterior-knee laxity (AKL) was quantified with an arthrometer.
Results:
Mean and absolute eccentric HS peak torque decreased by 24.5 N.m (-12.34%; P < 0.01) and 21.9 N.m (-10.08%; P < 0.01) in female athletes, whereas their male peers improved by 19.9 N.m (+9.01%; P = 0.01) and by 20.9 N.m (+8.51%; P = 0.02), respectively. HS total work in female athletes decreased by 831.1 J (P < 0.01) compared with the male athlete reduction of 235.3 J. Both the pre- versus postmatch intersex mean and absolute eccentric HS peak torque changes were significant (P < 0.01), as were the changes in HS total work (P < 0.01). The pre- versus postmatch AKL difference and the dominant versus nondominant limb comparison of the strength parameters were not significantly different. Younger female athletes (14-19 years old) presented a greater decrease in mean and absolute peak HS eccentric strength compared with those in older female athletes and men.
Conclusion:
HS eccentric strength and work differ based on athlete sex, as measured by the NHE test. Mean peak, absolute peak, and total work showed greater reductions in female athletes than those in their male peers. The subgroup of 14- to 19-year-old female athletes experienced the highest reduction in strength parameters.
Anterior cruciate ligament (ACL) tears are very frequently occurring injuries that result in early, mid- and long-term consequences both in terms of symptoms and functional limitations.10,38,51,52 This injury affects both male and female athletes,15,40 with the latter having a significantly higher occurrence rate than that in male athletes practicing the same sport,23,30 especially in children and adolescents.48,60 Therefore, identification of methods to reduce the risk of sustaining such an injury is paramount. 42 A hamstring (HS) strength imbalance has been identified as a risk factor for sustaining an ACL injury in case players perform playing actions with associated reduced neuromuscular HS recruitment. 45 In fact, a HS strength evaluation is crucial to reduce the risk of an ACL tear, as well as to rehabilitate a player after an ACL injury.19,22 In this context, isokinetic devices are used to evaluate thigh muscle function to monitor absolute and side-to-side torque production as well as the HS-to-quadriceps (H/Q) ratio,15,42 even though the latter is not considered an independent risk factor for either HS or ACL injury. 34 Such measurements assist in customizing preventive and rehabilitative programs and in determining return-to-sport readiness.
Unfortunately, the isokinetic device is an expensive tool and presents some limitations. Subjects are tested in a seated position with the hip flexed at approximately 90°, whereas the vast majority of athletic activities are commonly carried out in a standing position, thus reducing the ecological validity of the testing setup. Furthermore, the test is usually performed in a nonfatigued state, but athletes perform in a fatigued state during both training and competition. 50 On the other hand, the Nordic hamstring exercise (NHE) represents an affordable, quick, safe, and effective approach for HS injury prevention and rehabilitation.41,61 The NHE is performed with the subjects’ hips in a neutral position with the HS being increasingly activated in an eccentric fashion. Measuring the HS eccentric strength while executing the NHE test delivers a higher ecological validity, with the alignment of body segments being more similar to the execution of sport-specific tasks. 16 In addition, the NHE test was proven to be reliable and capable of identifying clinically relevant asymmetrical HS strength deficits that are not detected with isokinetic testing.30,44 In this context, NHE testing can be considered a relatively cheap and easy-to-use alternative to isokinetic testing. However, the available evidence in relation to strength measurements obtained with the NHE test after a soccer match is scarce, and does not provide dichotomized results for male and female athletes; thus, sex-specific data in such tasks are not yet available.
The aim of this study was to analyze HS eccentric strength trends before and after a soccer match by performing the NHE test in both male and female soccer athletes. The hypothesis was that the NHE could also detect soccer-specific fatigue-induced changes in HS eccentric torque in women.
Methods
Participants
Our primary outcome was HS eccentric strength, and we based the power analysis to determine the adequate sample size on that variable. Following the methods described in an observational study in which researchers tested whether a 90-minute soccer match induced fatigue effects in HS eccentric strength in male athletes measured while performing NHE, 33 which led to HS eccentric strength pre- and postmatch values (mean ± SD) of 306.91 ± 59.26 and 277.77 ± 60.35 N.m (P < 0.01; Cohen’s d = 0.50), respectively, the delta method based on a Taylor series approximation was applied to determine the mean percentage reduction and the relative standard deviation, which resulted in 9.45% ± 6.85%. 20 Using these data, and following the hypothesis that the difference for female athletes would be equal to 7% with the same standard deviation, an effect size of 1.021 was obtained. With a significance level (alpha) set at 0.05 and a statistical power set at 0.9, the minimum number of study participants per group was 22, for a total of 44. Estimating a potential drop-out rate of 10%, the sample was increased to at least 50 participants (25 per group).
Finally, 64 competitive soccer athletes participated in this observational cohort study. Subjects were included if they met the following criteria: male or female; healthy competitive soccer athletes (overall mean Tegner score, 7.84 ± 0.99); training and playing at least 4 times per week; aged from 14 to 25 years (inclusive); not currently injured; without history of HS grade 2 to 3 injury in the previous 3 months; without having undergone ACL surgical reconstruction regardless of the graft type; not pregnant; nonsmokers; played in any position except goalkeeping; starting and completing the entire game. The sample mean age was 19.2 years (± 3.0), comprising 37 female and 27 male athletes, with 55 right (R)-dominant and 9 left (L)-dominant athletes, defined as their preferred kicking leg.
Procedures
The study was carried out in Canton Ticino, Switzerland, in accordance with the Declaration of Helsinki, following the principles of Good Clinical Practice, and the Swiss regulations on human research, and was approved by the local Ethics Committee. The recruitment sites were the playing facilities of local competitive soccer teams in the occasion of official championship matches taking place in the second half of the competitive season, between March and May 2022. The procedures for participant recruitment comprised of a first meeting during a training session to introduce the study characteristics. Candidate participants received an information sheet and a consent form describing the study and providing adequate information to make an informed decision about their participation in the study. The signed informed consent forms were collected on the match day before performing any measurement.
The teams were involved in the prematch measurement procedures, with only the athletes completing the entire game being retested after the end of each match and, therefore, being included in the study. Eccentric HS strength (in terms of mean and absolute torque [N.m] and total work [J]) was assessed on the pitch side through 5 repetitions of the NHE test using 2 units of the N3 device (Easytech Srl) before and after the end of the soccer match. The NHE is an exercise in which the person kneels on a comfortable padded surface while the ankles are either held or secured in place and progressively lowers their trunk toward the ground by extending the knees while maintaining a shoulder-hip-knee alignment (Figure 1). In the process of leaning forward toward a terminal prone position, the athlete uses their HS muscles to lower their descending upper body as slowly as possible. The pregame testing session took place after a light warm-up comprising 5 minutes of jogging, whereas the postmatch measures were performed with the athletes approaching the testing station right after the end of the game. Measuring HS strength while executing the NHE has already been proven to be a reliable method, 9 and the resulting measures are correlated with those of isokinetic dynamometry. 43 The N3 measuring device is connected via Bluetooth with an Android-based tablet on which a dedicated app is installed. The app automatically calculates the HS eccentric absolute peak torque and the total work, while the mean peak torque is calculated by the researchers based on the peak torque of each NHE repetition. Anterior-knee laxity (AKL) was measured concurrently pre- and postmatch with a Rolimeter (Aircast Europe), which is an arthrometer that provides a valid measure of knee laxity that is comparable with that of the KT-1000. 18 This procedure is executed with the tested athlete’s knee flexed at 20° on a support positioned on the back of the distal thigh and the arthrometer fixed to the lower leg with a distally placed adjustable strap. The proximal rounded pad of the arthrometer is positioned on the patella, and an adjustable feeler is positioned on the tibial tuberosity. At this point, the operator executes a Lachman test with maximum manual force, and the anterior tibial translation is quantified automatically by a reader on the sliding feeler of the arthrometer, which indicates the amount of movement in millimeters. On average, the athletes involved began the repetition of the testing procedure within approximately 7.5 minutes (SD 4.3) after the end of the match.

The nordic hamstring exercise (NHE).
To avoid measurement bias and/or interrater discrepancies, automatic devices were used to measure HS strength, whereas AKL measurements were taken by a single researcher. Participants were blinded to the study hypothesis, and no compensation was given to the study participants.
Statistical Analysis
All continuous data are expressed as the means and standard deviations, and categorical variables are expressed as proportions or percentages. The Shapiro-Wilk test was performed to test the normality of continuous variables. The Levene test was used to assess the homoscedasticity of the data. The paired t test was performed to assess pre- and postmatch differences. Two-way analysis of variance was performed to assess differences related to sex and or age. The effect size of the subgroups comparisons was provided and the Sidak post hoc pairwise comparisons test was performed to assess differences between subgroups. The Spearman rank correlation was used to assess correlations between numerical scores and continuous data. Pearson’s chi-square test evaluated using the exact test was performed to investigate relationships between grouping variables. For all tests, P < 0.05 was considered to indicate statistical significance and a threshold of 0.8 was considered relevant for the effect size. All statistical analyses were performed using SPSS Version 19.0 (IBM Corp).
Results
From the initial 83 athletes who participated in prematch testing, 65 who completed a full 90-minute game were eligible to be retested at the end of the match to be included in this study. Of the 18 athletes who did not play the full match, 17 were substituted with backups by their coaches either for technical reasons or turnover purposes, and 1 suffered an injury in the first half and was unable to resume competition. An additional player completed the match but was affected by cramps in the final minutes of the match and was therefore unwilling to undergo the postmatch NHE test. Therefore, 64 athletes were included in this study. To avoid selection bias when enrolling team athletes during the soccer games, all present eligible athletes from the team were recruited, which led to overpassing the sample calculated with the power analysis. The characteristics of the cohort are reported in Table 1.
Characteristics of included participants
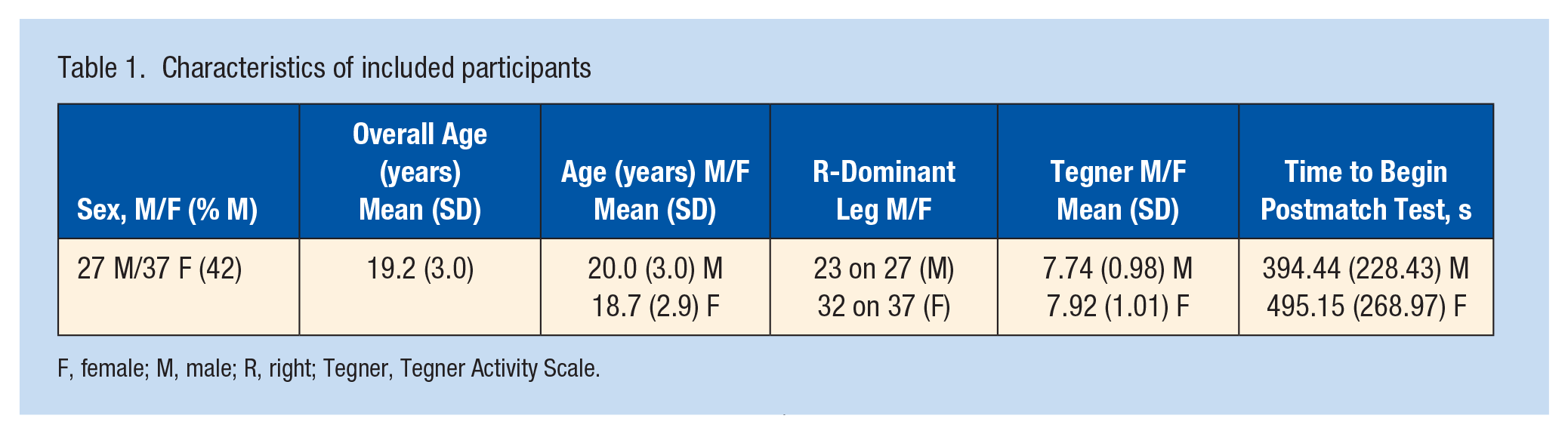
F, female; M, male; R, right; Tegner, Tegner Activity Scale.
Primary Outcome
During the execution of the NHE tests, the variable of primary interest was the pre- and postmatch between-sex difference in the mean eccentric HS peak torque. This difference emerged as highly statistically significant (P < 0.01), with female athletes showing a significant decrease of 24.5 ± 49.1 N.m (effect size [ES], 0.5; P < 0.01) equal to -12.34%, whereas their male peers improved significantly by 19.9 ± 40.5 N.m (ES, 0.5; P = 0.01) corresponding to +9.01%.
Secondary Outcome
The secondary outcome was the intersex pre-post change in absolute eccentric HS peak torque. Such a difference was highly statistically significant for both limbs (P < 0.01). Female athletes showed a significant decline of 21.9 N.m ± 49.2 N.m (ES, 0.44; P < 0.01), which is -10.08%; in contrast, an improvement of 20.9 ± 46.1 N.m (ES, 0.45; P = 0.02), equivalent to +8.51%, was revealed for the male athletes. A further secondary outcome was the difference between sexes for total HS work recorded pre- versus postmatch. This delta-change score was significantly different (P = 0.01), with female athletes experiencing a highly significant decrease of 831.1 ± 1149.6 J (ES, 0.72; P < 0.01) and male athletes experiencing a nonsignificant decrease of 235.3 ± 1471.2 J (ES, 0.16). In the end, the between-sex pre-post AKL difference was nonsignificant. In fact, this measurement increased in a highly significant manner (P < 0.01) regardless of sex, with female athletes showing an increase of 1.8 ± 1.3 mm and males increasing by 1.6 ± 1.3 mm.
The comparison between dominant and nondominant limbs for the primary and secondary outcomes showed no significant difference. Further data about the measurements are provided in Figure 2.
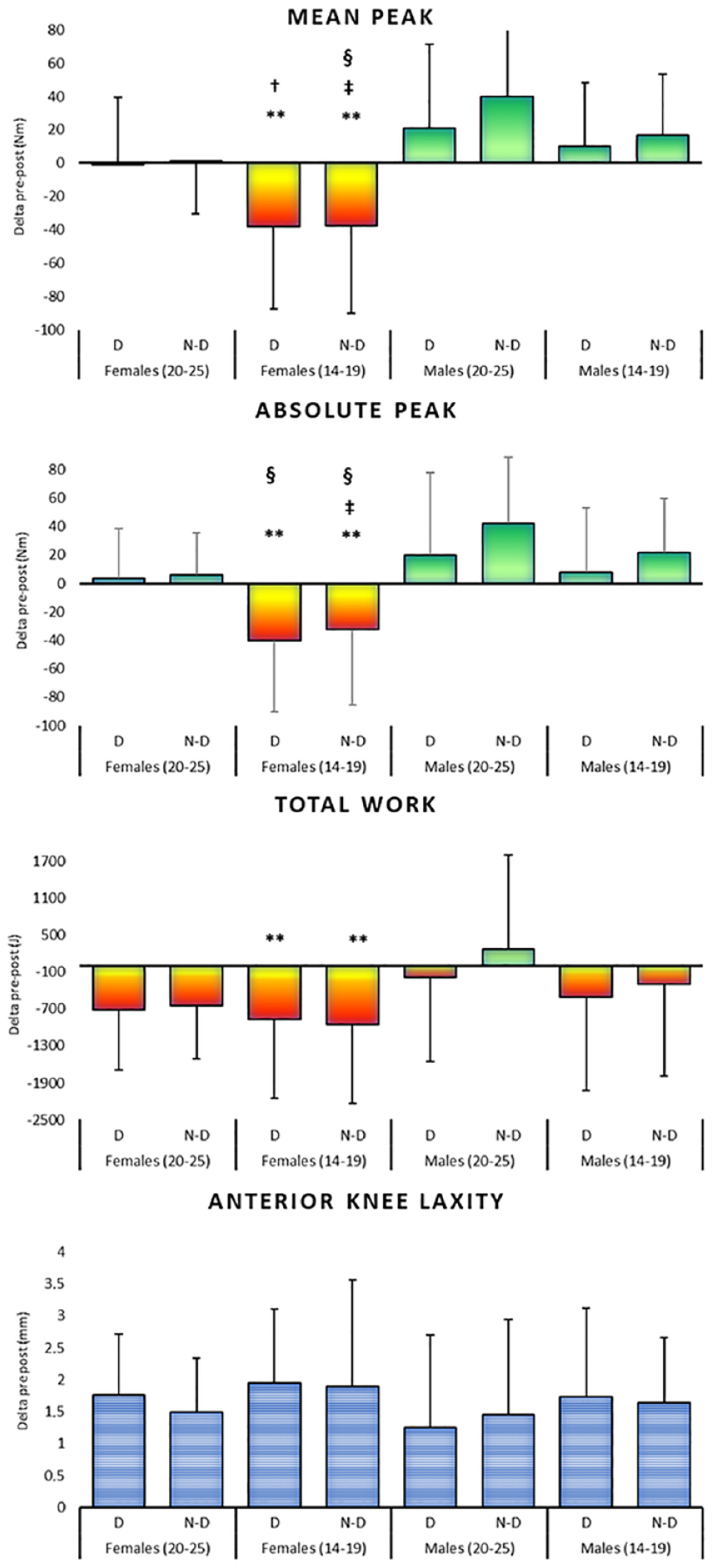
Depiction of mean peak, absolute peak, total work, and AKL in female and male subjects for right and left lower limb. *P < 0.05 (significantly different from male athletes aged 14-19 years, **P < 0.01 (significantly different from male athletes aged 14-19 years, †P < 0.05 (significantly different from male athletes aged 20-25, ‡P < 0.01 (significantly different from male athletes aged 20-25 years), §P < 0.05 (significantly different from female athletes aged 20-25 years). AKL, anterior-knee laxity.
Subgroup Analyses for Sex and Age
Filtering the collected data by sex and subgrouping by age (14-19 years and 20-25 years), the younger female athletes (14-19 years) experienced a significant pre- versus postgame reduction in both mean and absolute eccentric HS peak torque compared with males regardless of the age of the latter (P < 0.01 for both parameters). The connection between pre-/postmatch differences in mean eccentric HS peak torque and participants’ age is represented in the scatter plot in Figure 3. There was no difference for pre- versus postgame total HS work and AKL considering sex and age. Details are reported in Tables 2-4.
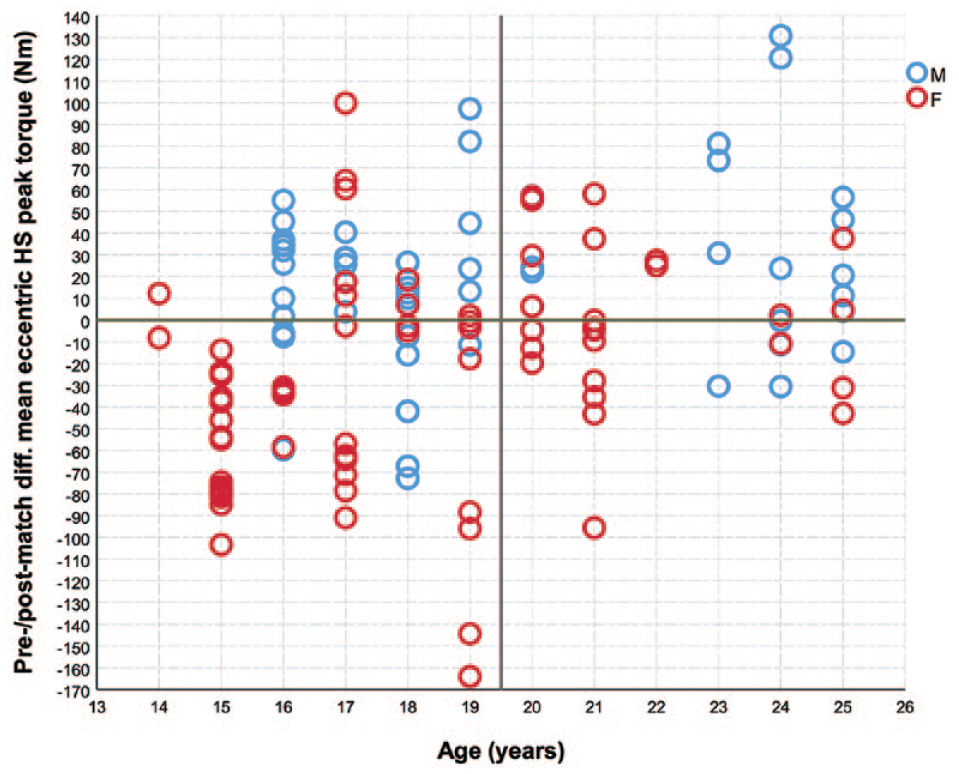
Pre-/postmatch differences in the mean eccentric HS peak torque of the lower limb and the participants’ age. F, female athletes; HS, hamstring; M, male athletes.
Pre-post differences (delta) in mean and absolute eccentric peak torque and total work main and interaction effects by age and sex
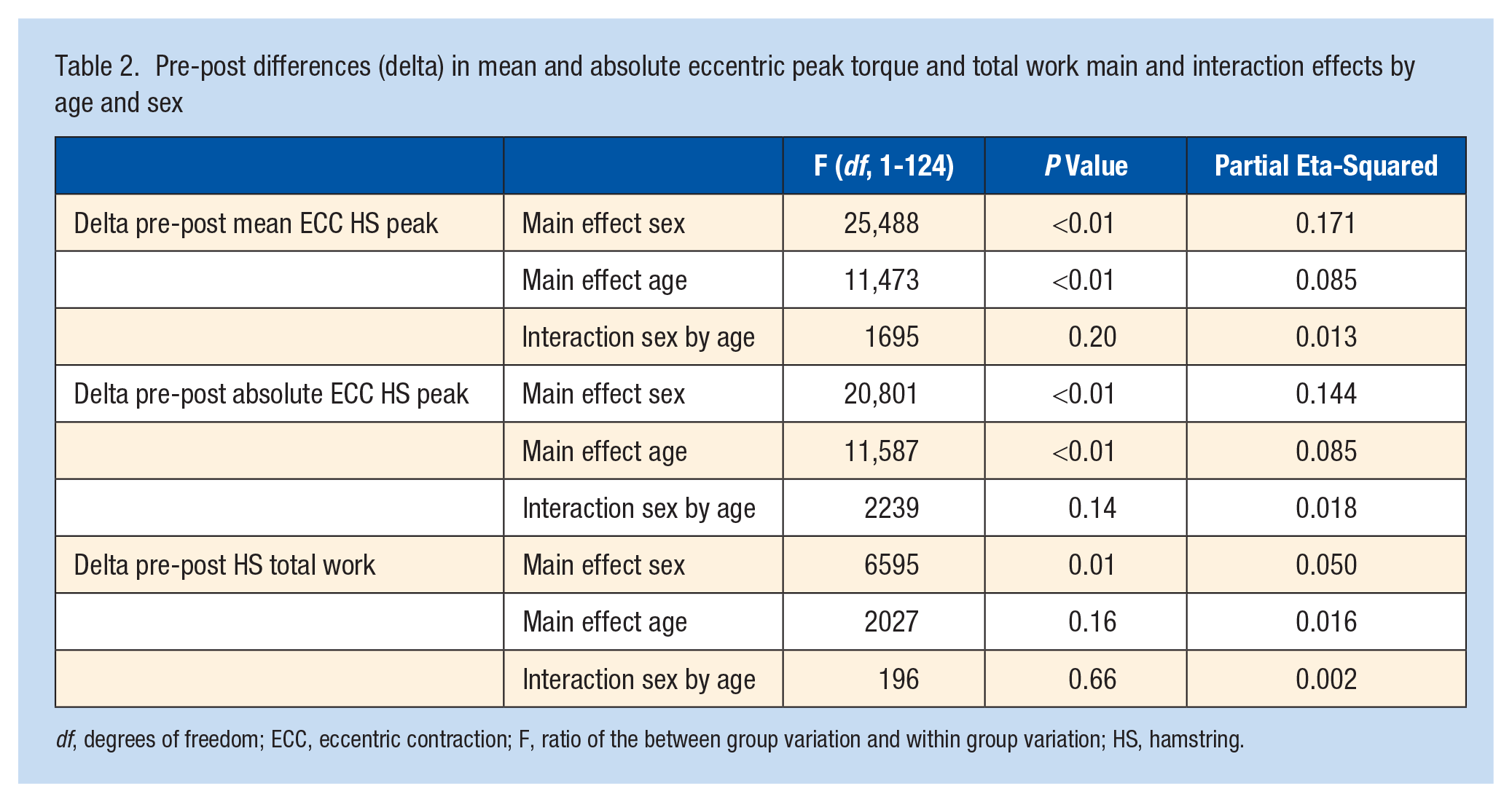
df, degrees of freedom; ECC, eccentric contraction; F, ratio of the between group variation and within group variation; HS, hamstring.
Pre-post differences (delta) in mean and absolute eccentric peak torque and total work stratified by age and sex
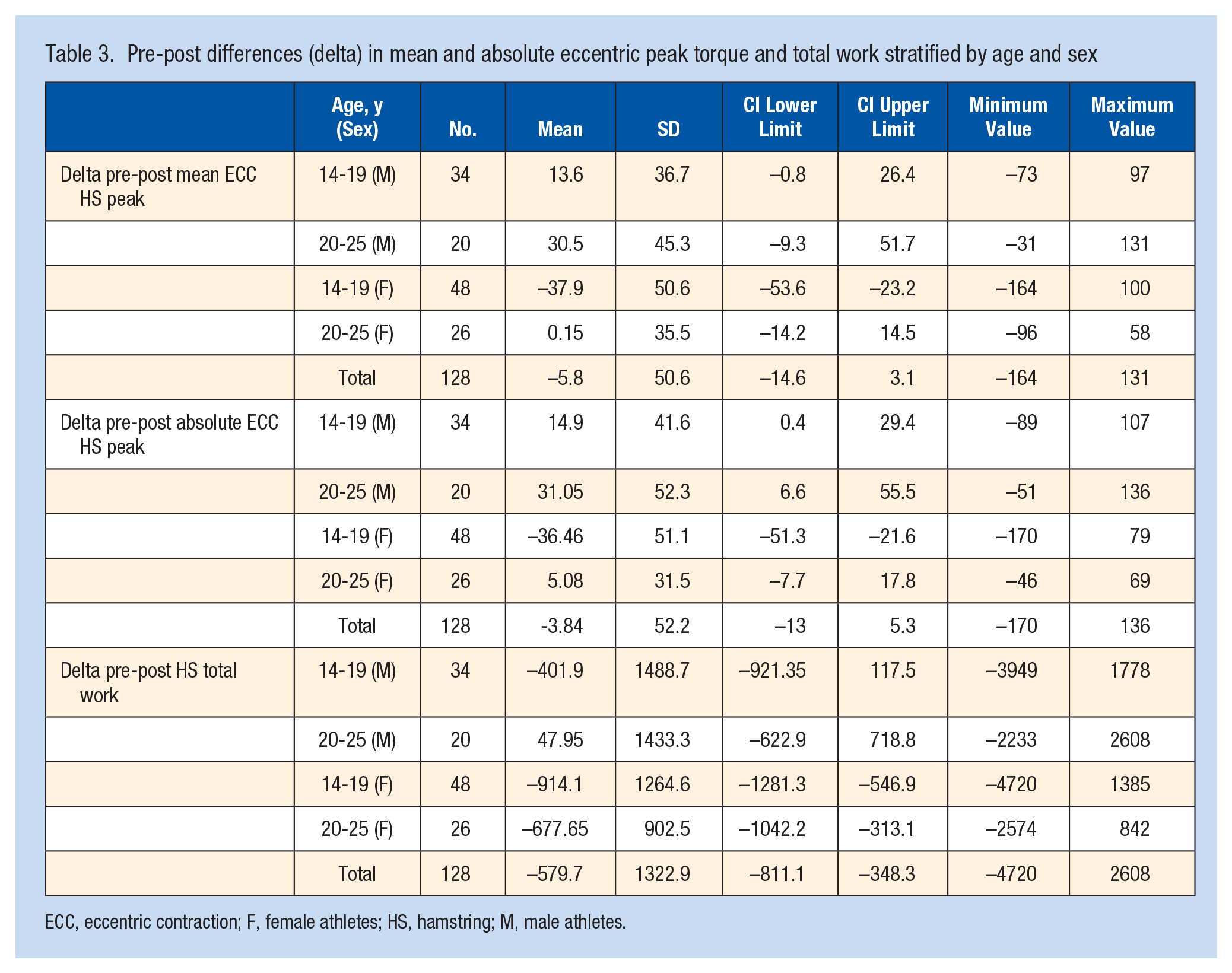
ECC, eccentric contraction; F, female athletes; HS, hamstring; M, male athletes.
Post hoc pairwise comparison (differences between the means of each subgroup with reported level of significance) a
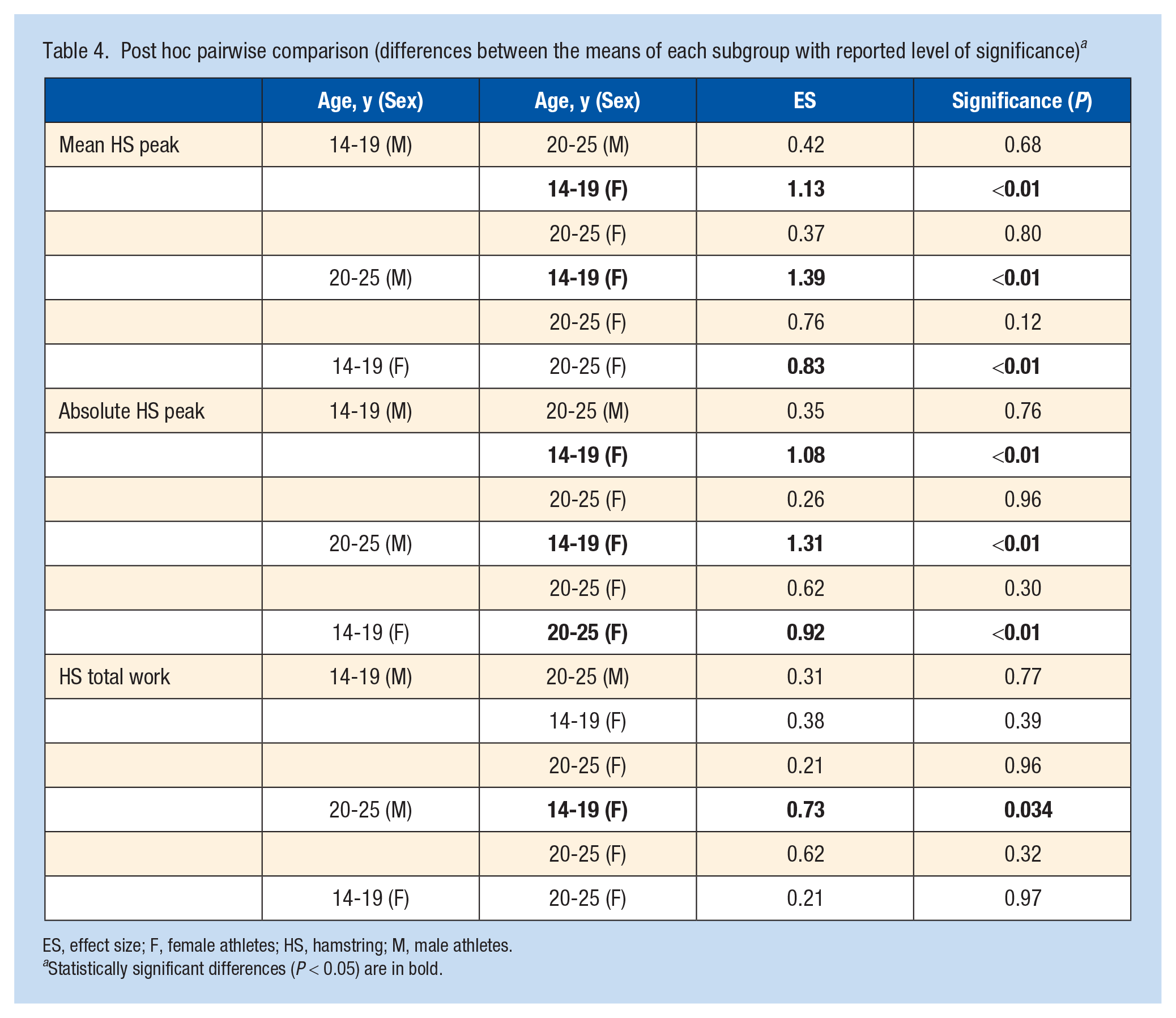
ES, effect size; F, female athletes; HS, hamstring; M, male athletes.
Statistically significant differences (P < 0.05) are in bold.
Discussion
The main finding of this study is that HS eccentric strength and work at the end of a soccer match, as measured by performing the NHE test, present differences based on the sex of the athlete. Specifically, mean peak, absolute peak, and total work showed greater reductions in female athletes than in their male peers.
The results of the current study build upon the results previously provided by the observational study published by Kakavas et al, 33 which investigated the potential effect of fatigue in reducing the peak eccentric strength of the HS muscles as well as in generating a between-limb eccentric strength imbalance of the HS muscle group after a soccer match. A total of 22 male professional soccer athletes participated in that previous study during a single match. The eccentric strength of the HS muscles was determined using the NHE test before and after full participation in an entire soccer match. The findings highlighted a significant decrease in eccentric strength after the match, whereas the imbalance in eccentric HS muscle strength between the dominant and nondominant limbs that was observed before the match remained unchanged after it ended. The present study revisits those previous findings by showing how the reported decrease in eccentric HS after a soccer match emerges following a sex-related trend, with only female athletes being significantly affected in this series, whereas male athletes showed a significant improvement in both HS eccentric peak and absolute torque.
Such intersex postmatch outcome differences showed that male athletes were possibly subject to soccer-specific postactivation potentiation (PAP), whereas female athletes were not. 29 PAP refers to an acute increase in muscle force parameters (eg, peak torque) after voluntary maximal or near-maximal intensity muscle contractions. At the same time, this physiological phenomenon happens to be fatigue-modulated depending on the resting time between muscle activation and the subsequent measurements associated with muscular activity and by several variables that leave the PAP-fatigue relationship not yet fully elucidated. 59 Further studies should investigate whether these aspects could play a role in explaining the higher incidence of ACL injuries in female athletes compared with male athletes performing the same sport.40,48
The stratification for age in this study also showed that younger female athletes (14-19 years) showed a greater decrease in HS eccentric strength (both mean and absolute peak) and work compared with those in older women and men, respectively. Such a result could help in understanding the underlying causes of the increased risk of sustaining an ACL tear in children and adolescents presented in previous studies.3,57 Adolescent female athletes who participate in jumping and pivoting sports appear to be at elevated risk of sustaining noncontact ACL injury, even more so if they are aged 14 to 19 years. 47 The age of onset of ACL injury claims in female athletes is close to that of menses, 54 and a particular increase in injury rate is reached during midcycle (high estrogen levels) in normally menstruating women. 65 When landing, decelerating, and pivoting, women have a decreased ability to dynamically control the knee joint,26,27 and other etiological factors for a female predisposition to ACL injury, including HS performance, have been discussed in this regard, especially in younger female athletes.
Puberty is accompanied by hormonal changes and a growth spurt that increases adolescents’ height and weight dramatically without corresponding changes in strength and neuromuscular adaptations, and the presence of specific receptors makes skeletal muscle sensitive to estrogens and progesterone fluctuations.36,37,63 An increased body mass index during adolescence has been reported as a possible risk factor for ACL injuries, especially among adolescent female soccer athletes. 25 HS flexibility decreases with age and maturation in boys, whereas girls show an increase after puberty. 8 This causes a compromised capacity for resisting changes in length associated with joint perturbation in girls compared with boys. 7 The increase in estrogen levels impairs muscular stiffness and laxity of the HS myotendinous unit as well as the entire lower limb.5,12
However, although the role that female hormones play in different anatomic structures appears supported scientifically, the causal relationship between hormone fluctuations and the higher rate of specific musculoskeletal injuries in female athletes is far from being established. 35 Many factors interact, and the research is still conflicting. It has been demonstrated that female athletes who incur more injuries are subjected to menstrual hormonal irregularities, the impact of which is often overlooked in the literature. 58 In a study performed on collegiate female athletes with regular menses, regardless of the observed fluctuations in relaxin levels over a span of 1 month, there were no significant differences in AKL, and no differences were observed in mean relaxin levels compared with those of male controls. 2 Furthermore, different studies highlighted a higher injury frequency occurring from the premenstrual phase, characterized by the lowest hormonal levels, through later phases, in which estrogen rises to the highest levels, up to the postovulatory phase, when estrogen levels rapidly drop, hence failing to correlate the occurrence of the majority of injuries with estrogen peaks. To complete the complex scenario, the use of oral contraceptives increases H/Q strength ratios, increases stability on 1 leg, and decreases knee laxity, 24 offering up to a 20% reduction in ACL injury secondary to hormonal changes during the menstrual cycle. 23 After puberty, female athletes tend to increase their quadriceps strength more than their HS strength, thereby becoming “quadriceps dominant.”1,32,56 This deficit in HS strength is particularly pronounced at the higher angular velocities typical of sports participation. 13 In contrast, male athletes are more HS dominant, which contributes to stabilization of the knee.25,48 On the one hand, this can protect men from ACL injuries, whereas on the other, it can contribute to the documented higher risk of HS injuries in men.4,53 Fatigue produced after a professional 90-minute football match significantly impacts the ability of athletes to produce high-speed eccentric strength in the HS muscle groups, 33 causing a greater loss of HS strength than quadriceps strength in female athletes.21,47,55 Female athletes generally have smaller muscles, including HS and quadriceps, than male athletes. 4 A disproportionately small HS muscle in girls might represent an anatomic sex-related difference that can contribute to a low H/Q strength ratio. 14 This can also alter dynamic control ratios, which indicates an impaired HS capacity to absorb ground-reaction force and counterforce in female athletes predisposed to ACL injury.11,62
Sex-related differences have also been observed in HS muscle activation patterns, with lower HS preactivation reported in female athletes.6,31 Girls also exhibit a more valgus knee under static and dynamic conditions, likely related to anatomic constraints and aspects of neuromuscular control. This pattern among girls, which is even more pronounced in earlier puberty, generates high frontal-plane shear stress on the ACL that, together with an altered H/Q ratio and a delayed HS activation timing, resulting in “valgus collapse” being the most common female pathomechanic injury. 17
The reduced HS activity during soccer sport-specific movements can be detrimental from the ACL and HS injury perspective. Hewett et al 28 showed how HS contribution in the H/Q ratio diverges between sexes, with a significant decrease in female subjects associated with increasing angular velocity. The results of this study further support such information by investigating the execution of a different task–the NHE. The decrease in eccentric HS strength documented immediately after a soccer match may be explained by the fatigue experienced by female athletes (especially those aged 14-19 years) created by soccer-specific demands. Such effort seems to be significantly impactful in this population with respect to the other subgroups, thus extending the results of Hewett et al 28 in a setting with higher ecological validity.
NHE presents several advantages compared with classic isokinetic testing. It is fast and straightforward to execute, involving a cheap and portable device while providing higher ecological validity, which is pivotal for the translation of research findings. Isokinetic normative and protective values have emerged from the literature in recent decades.46,49 It has been shown how they change with increasing angular velocity (similar to those occurring during sports activities), mainly affecting the ability of female athletes to maintain HS strength, consequently leading to a markedly decreased H/Q ratio. 28 However, the intrinsic characteristics of isokinetic testing, requiring a nonportable and expensive device, make it difficult to extend and apply these findings to a broad population. This further highlights the relevance of the current study findings, which are based on NHE testing – a method widely available in the field. The possibility of evaluating athletes with NHE testing empowers clinicians and strength and conditioning coaches with the possibility of screening healthy athletes to identify subjects at higher risk of injury and to implement specific prevention programs to reduce muscle imbalances.9,61
This study adds important normative data on NHE-tested HS strength in the field and provides key information on sex-related changes with fatigue. Comprehensively, the results of this study provide more insights into the behavior of HS strength before and after a soccer match, highlighting how, in young female athletes, HS strength shows a higher and statistically significant decline. This information may help understand the higher ACL injury and reinjury rates in this population, and could be used in prevention and rehabilitation situations. Preventing HS strength impairment is crucial as a primary prevention intervention to lower the overall (ACL and HS) injury risk. In addition, testing HS strength and function along a rehabilitation process, for instance, after an HS injury or an ACL-R with HS autograft, is a vital secondary prevention approach to ensure a normative data-based recovery, which would apply to all ages and sexes. Although future studies should confirm these findings in different study settings investigating different soccer ability levels, different sports, and different training conditions, this study sets the base for the routine use of NHE testing to investigate HS eccentric strength.
This study presents many limitations. Although it was adequately powered to investigate the primary study outcome, the sample size was insufficient to properly perform subanalyses. The match intensity and/or the subjective physical demand on the tested athletes was not monitored with a specific device (eg, heart rate monitor, GPS, etc), which could constitute a confounding factor. Moreover, players were evaluated within approximately 7.5 minutes of the match ending. While we organized the athletes immediately after the end of each game with 2 devices/testing stations to reduce the postgame waiting time before testing as much as possible, we cannot exclude the possible influence of PAP.39,64 Nevertheless, this possible influencing factor could not counteract the fatigue effect observed in younger women, which further strengthens our conclusions. Concurrently, we speculated the role of a soccer-specific PAP as a possible explanation of the study outcomes. Furthermore, including movement quality evaluation linked directly to the ACL injury mechanism might strengthen the relationship between a postmatch HS strength reduction and the actual risk of sustaining an ACL tear. Lastly, no measurements of hormonal levels were carried out concurrently to investigate a possible link between sex-related hormonal fluctuations and exercise physiology and fatigue tolerance, which should be explored in future studies.
Conclusion
HS eccentric strength and work, as measured by performing the NHE test, differ based on athlete sex. Specifically, mean peak, absolute peak, and total work showed greater reductions in female athletes than in their male peers. Moreover, younger female athletes (14-19 years old) showed a statistically significant greater decrease in HS eccentric strength at the end of a soccer match, both in terms of mean and absolute peak, compared with older female athletes and male athletes. These results may help clinicians and trainers develop customized rehabilitation and training programs while considering sex-specific characteristics with the aim of reducing the risk of sustaining ACL and HS injuries.