
Abstract
Background:
Altered reorganization of the sensorimotor system after an initial lateral ankle sprain may lead to a chronic neuromuscular maladaptation in multiple body locations. Specifically, decreased diaphragm contractility has been observed in patients with chronic ankle instability (CAI). The diaphragm has an essential role in postural control. Decreased diaphragm contractility could associate with diminished postural control commonly observed in patients with CAI. However, no study has determined if diaphragm contractility contributes to postural control in a CAI population.
Hypothesis:
Decreased diaphragm contractility would be negatively associated with static postural control in patients with CAI.
Study Design:
Cross-sectional study design.
Level of Evidence:
Level 4.
Methods:
A total of 15 participants with CAI participated voluntarily. An ultrasonography assessment was performed to quantify the right and left hemidiaphragm thickness at the end of resting inspiration and expiration in supine while breathing quietly. The degree of diaphragm contractility was calculated from the diaphragm thickness. Participants performed 3 eyes-open trials of a 20-second single-leg balance task on the involved limb. Static postural control measures included the center of pressure velocity (COPV) and mean of time-to-boundary (TTB) minima in the anteroposterior (AP) and mediolateral directions.
Results:
Moderate correlations of the right hemidiaphragm contractility were observed with COPV (ρ = -0.54) and TTB mean minima (ρ = 0.56) (P < 0.05) in the AP direction. The left hemidiaphragm contractility was moderately correlated with COPV (ρ = −0.56) and TTB mean minima (ρ = 0.60) (P < 0.05) in the AP direction.
Conclusion:
Lower diaphragm contractility may be associated with diminished static postural control in the AP direction in patients with CAI.
Clinical Relevance:
This study highlights diaphragm contractility could be a potential connection with diminished static postural control in patients with CAI. Our data raise new avenues for future exploration including potential beneficial effects of implementation of diaphragm breathing exercises and techniques for restoring static postural control in patients with CAI.
A lateral ankle sprain is among the most prevalent musculoskeletal injuries, with high rates of recurrent incident and significant healthcare costs.11,14,31 At least 40% of the patients who experience an initial lateral ankle sprain fail to recover fully and subsequently develop chronic ankle instability (CAI).10,37 Patients with CAI frequently have episodes or perceptions of the ankle giving way, typically experience lifelong residual symptoms, and/or repeatedly resprain their ankle. 17 The current literature has reported that CAI is associated with diminished health-related quality of life, 29 decreased physical and occupational activities,30,61 and increased likelihood of progression to posttraumatic ankle osteoarthritis. 58 The negative health consequences of CAI after a first-time lateral ankle sprain highlight the need for continued research focused on further understanding of the underlying impairments associated with CAI.
Various motor-behavioral impairments have been observed in patients with CAI. 20 However, a large body of literature has consistently documented static postural control deficits in CAI populations.40,41 Recently, a patient-oriented study has reported that diminished static postural control may be a potential factor that reduces patient-generated function and diminishes health-related quality of life among patients with CAI. 28 Thus, poor static postural control is a prominent motor-behavioral impairment that is a potential target for interventions to produce optimal outcomes in patients with CAI. While clinicians and researchers have focused on identifying postural control impairments,34,38 it is important to identify what clinically modifiable factors to static postural control may provide direction for targeted interventions.
Researchers have suggested that altered reorganization of the sensorimotor system after an initial lateral ankle sprain may lead to a chronic neuromuscular maladaptation in multiple body locations.19,45 Specifically, previous work has identified altered diaphragm contractility in patients with CAI. 54 The diaphragm has multifactorial roles from respiration to regulation of emotional state. 62 In addition, the diaphragm contributes to postural stability through controlling intra-abdominal pressure (IAP), working in conjunction with the transversus abdominis, pelvic floor muscles, and deep intrinsic muscles of the spine.22-24,26,62 Hodges et al22,26 demonstrated that diaphragm contraction creates trunk and postural stability before and during sudden voluntary movements of the extremities through modulating IAP. Recently published literature has demonstrated altered diaphragm function during postural activity in patients with other musculoskeletal conditions (eg, chronic low back pain) related to trunk instability and poor coordination of postural muscles.36,47 Therefore, the altered diaphragm contractility observed previously among patients with CAI could be associated with clinical deficiencies, such as postural control deficits. However, the association between altered diaphragm contractility and static postural control in patients with CAI is currently unknown. An examination of the association between diaphragm contractility and postural control measures may provide important insight into the source of aberrant postural control patterns in patients with CAI. Therefore, the purpose of this study was to examine the association of diaphragm contractility with static postural control in patients with CAI. We hypothesized that reduced diaphragm contractility would be associated with a less efficient postural control in patients with CAI.
Methods
Study Design
A descriptive laboratory, cross-sectional study design was employed to examine the association between diaphragm contractility and static postural control variables. Diaphragm contractility and static postural control were assessed in patients with CAI over 1 study visit. All study procedures were approved by the university institutional review board.
Participants
For the current study, we recruited a convenience sample of 15 physically active participants with CAI between the ages of 18 and 35 from the university community (Table 1). All participants read and signed an informed consent approved by the university institutional review board before enrollment. Physically active was defined as a score of 24 or higher on the Godin Leisure-Time Exercise Questionnaire. 16 All participants self-reported no history of (1) diagnosed balance or vestibular disorders; (2) low back pain and injury; (3) surgery in the lower extremity and trunk; (4) a concussion in the past 6 months; (5) diagnosed cardiopulmonary disorder, scoliosis, ankylosing spondylitis, or any other disorders that can affect/alter the function of the respiratory system; or (6) any musculoskeletal and neurovascular injuries and disorders in the chest and the lower extremity in the past 2 years other than lateral ankle sprains.
Anthropometric and ankle injury characteristics for participants with chronic ankle instability
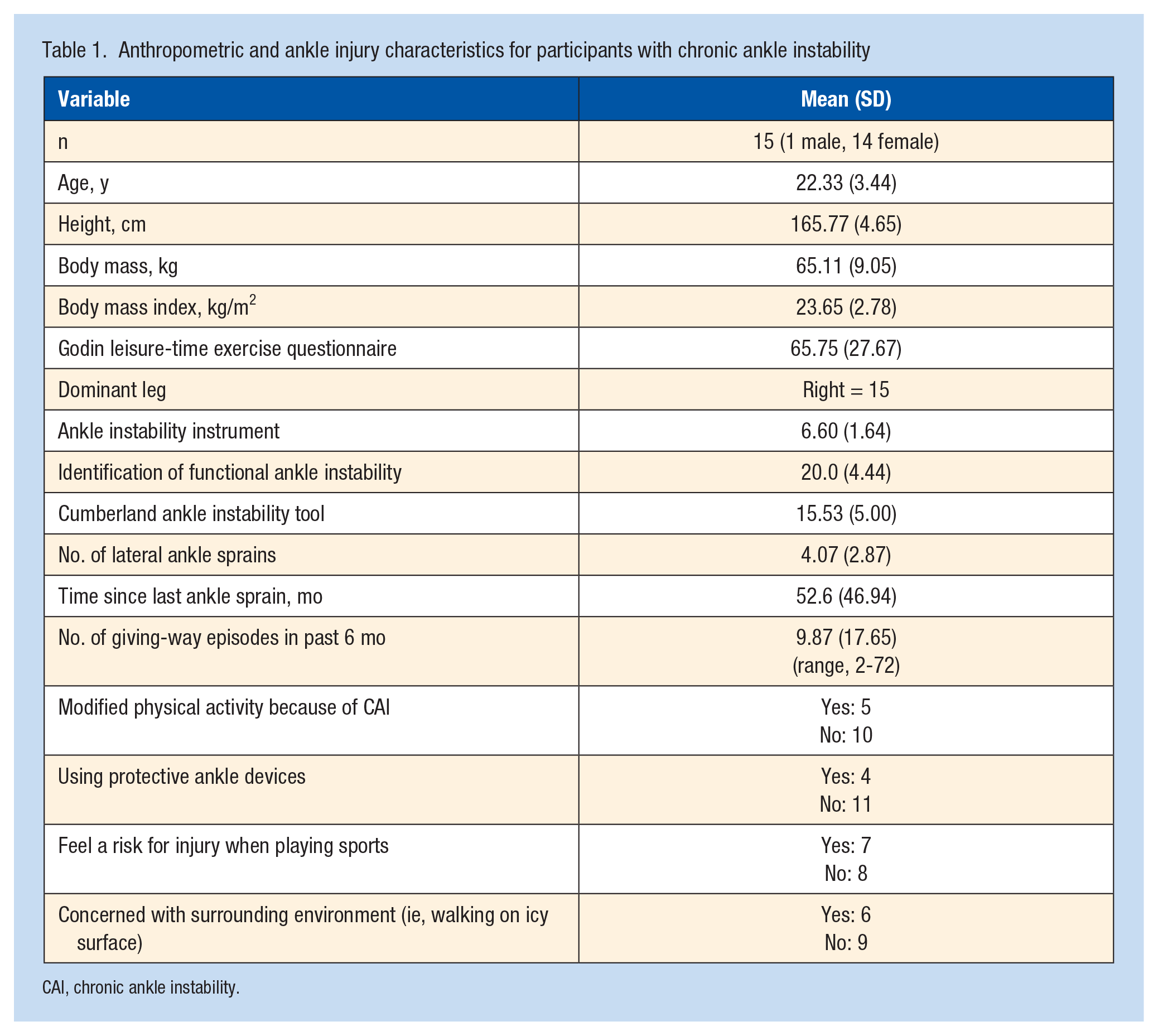
CAI, chronic ankle instability.
Based on the guidelines endorsed by the International Ankle Consortium, 17 the following specific inclusion criteria for participants with CAI were used: (1) a previous history of at least 1 significant lateral ankle sprain resulting in swelling, pain, and temporary loss of function; (2) a history of feelings of giving way at least twice in the past 6 months; (3) ongoing perceived ankle instability during daily activities; and (4) a score ≥5 on the Ankle Instability Instrument, ≥11 on the Identification of Functional Ankle Instability, and ≤24 on the Cumberland Ankle Instability Tool. No participant with CAI had acutely sprained his/her ankle in the previous 3 months of testing. A previous study reported a potential association between limb-dominance and risk of ankle sprain, 3 and therefore, we only included participants who had CAI on the dominant leg in this current study. The dominant leg that was defined as the limb used to kick a ball. 60
Ultrasonographic Assessment of Diaphragm Contractility
The validity and reliability for ultrasonographic assessment of diaphragm thickness and contractility has been established previously.8,18 Our methods of ultrasonographic image acquisition and processing were described in greater detail in earlier studies.18,54 Briefly, participants were instructed to lie in the supine position and maintain normal and quiet breathing during ultrasonographic image acquisition. To image the right- and left-hemidiaphragm, the 12L-RS linear ultrasound probe (GE Healthcare) was positioned over the zone of apposition of the diaphragm at the 8th intercostal space (between the 8th and the 9th ribs) in the midaxillary lines.18,54 We captured bilaterally 3 ultrasound images of the diaphragm at the end of resting inspiration and expiration over 3 breathing cycles using a LOGIQ e ultrasound machine (GE Healthcare). We measured bilaterally diaphragm thickness (cm) as the distance between the central point of the superior border (the pleural membrane) and the inferior border (the peritoneum membrane) of the diaphragam.18,54 The central point of the diaphragm was identified manually by the examiner as the middle of space between 8th and 9th ribs. We calculated bilaterally the degree of diaphragm contractility from the diaphragm thickness values (diaphragm contractility = [(diaphragm thickness at the end of inspiration - diaphragm thickness at the end of expiration) ÷ diaphragm thickness at the end of expiration ] × 100). 50 Higher values of diaphragm contractility reflect a greater change in diaphragm thickness from the end of inspiration to expiration as well as indicate a more effective diaphragmatic contraction and better diaphragm function.
Static Postural Control Assessment
Static postural control was assessed during a 20-second single-leg stance balance task on the involved leg with barefoot under an eyes-open condition. Participants were instructed to stand barefoot and maintain a single-leg stance with their testing foot flat on a force platform and their hands on their waist while maintain slight knee flexion. Participants were allowed 1 practice trial to become familiarized with the task and then asked to perform 3 testing trials. A trial was discarded and repeated if (1) the nontesting limb made contact on the force platform or the stance limb; (2) participants hopped or took a step with the stance limb; (3) participants lifted their forefoot or heel; or (4) they removed their hands from their waist.
Center of pressure (COP) trajectories in the anteroposterior (AP) and mediolateral (ML) directions were measured using a force platform (AccuSway Plus, AMTI) integrated with Balance Clinic software (AMTI) at a sampling rate of 100 Hz. The COP timeseries data were filtered with a low-pass, 4th-order Butterworth filter set at a cutoff frequency of 5 Hz.21,40 The COP trajectories were used to calculate COP velocity (COPV) and mean of time-to-boundary (TTB) minima in each direction with a custom MATLAB file (Mathworks, Inc) based on a previously described method.21,40 To calculate the TTB variables, the testing foot was placed in a rectangle marked on the force platform surface to allow for separation of the AP and ML components of COP trajectories. The boundaries of the foot were calculated using the actual foot length and width measures using previously described methodology.21,40 The average across all 3 trials was used for statistical analysis. A lower COPV and higher TTB mean minima scores represents better static postural control.
Statistical Analysis
We employed a separate Spearman’s Rho rank order correlation analysis to examine the strength of associations between diaphragm contractility and static postural control variables in participants with CAI. We interpreted correlation coefficients as negligible (0.0 ≤ ρ < 0.30), weak (0.30 ≤ ρ < 0.50), moderate (0.50 ≤ ρ < 0.70), strong (0.70 ≤ ρ < 0.90) or very strong (0.90 ≤ ρ ≤ 1.0). 44 A priori alpha level was set at P < 0.05 using SPSS 27.0 (SPSS, Inc) for all statistical tests.
Results
The dominant leg was the right side for all participants. Means and SDs for each variable are provided in Table 2. Moderate correlations of the right hemidiaphragm contractility were observed with COPV (ρ = -0.54; P = 0.02; observed power, 0.68) and TTB mean minima (ρ = 0.56; P = 0.02; observed power, 0.71) in the AP direction. Left hemidiaphragm contractility was correlated moderately with COPV (ρ = -0.56; P = 0.02; observed power, 0.71) and TTB mean minima (ρ = 0.60; P = 0.01; observed power, 0.78) in the AP direction. All other correlations were not statistically significant (P > 0.05, observed powers: a range from 0.09 to 0.31) (Table 3). The strength of these nonsignificant correlation coefficients was negligible or weak (Table 3).
Means and SDs for dependent variables
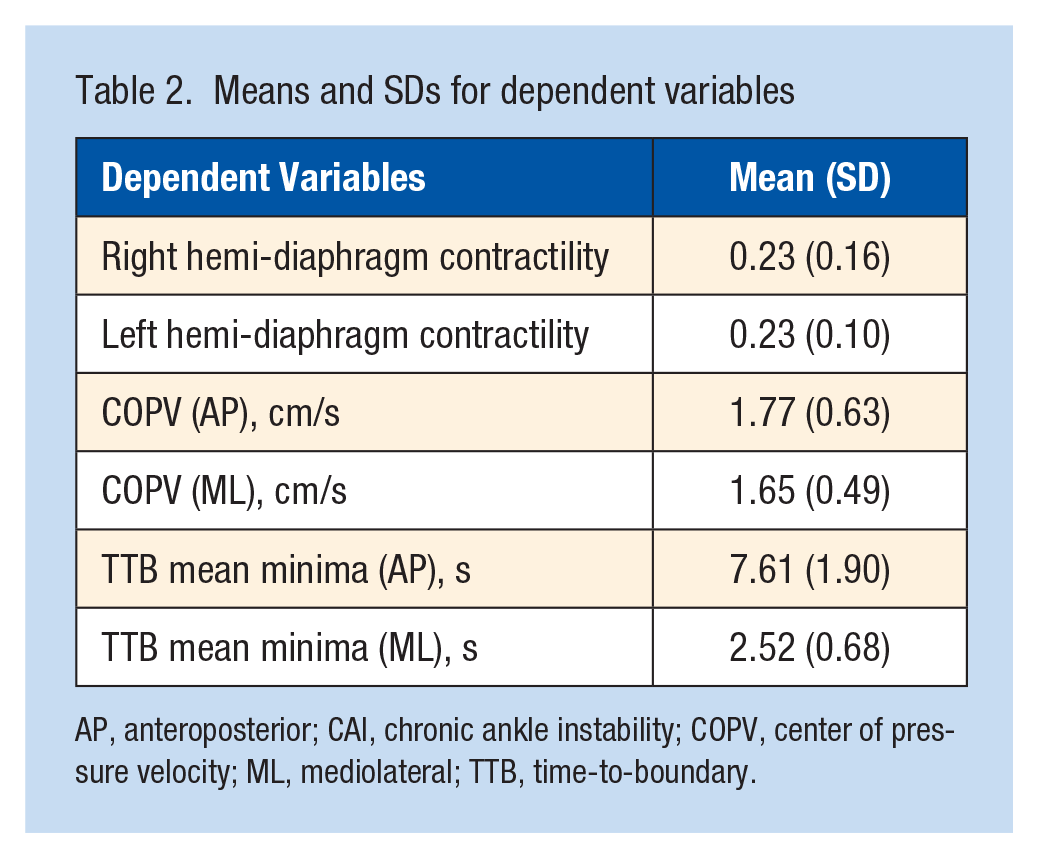
AP, anteroposterior; CAI, chronic ankle instability; COPV, center of pressure velocity; ML, mediolateral; TTB, time-to-boundary.
Results of Spearman’s Rho rank order correlations between diaphragm and static postural control variables
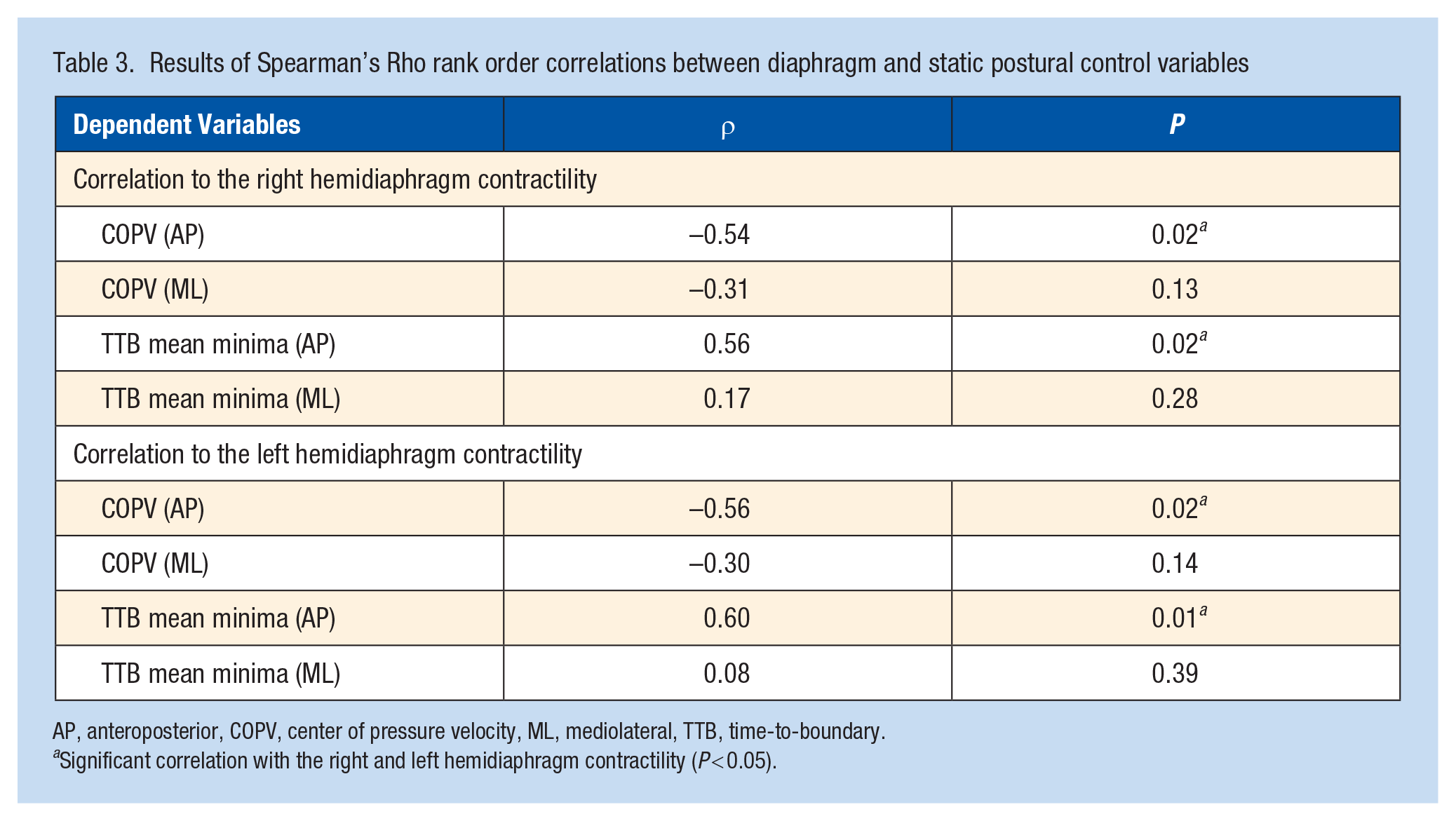
AP, anteroposterior, COPV, center of pressure velocity, ML, mediolateral, TTB, time-to-boundary.
Significant correlation with the right and left hemidiaphragm contractility (P < 0.05).
Discussion
Diminished postural control is typical after an initial lateral ankle sprain and persistent in the postacute and chronic phase of the injury.9,10,20 CAI is a neuromechanical injury that is linked with impairments in proximal muscles due to unique sensorimotor maladaptations within nervous system.20,45 The global alterations associated with CAI have been hypothesized to contribute to the alterations in static postural control. 53 Our current study identified positive and moderate correlations between the diaphragm contractility measures and the TTB mean minima in the AP direction in participants with CAI. The diaphragm contractility measures also correlated negatively and moderately with COPV in the AP direction in those with CAI. Positive correlation coefficients with TTB in the AP direction and negative coefficients with COPV in the AP direction indicate that participants with more effective diaphragmatic contraction may have better static postural control in the sagittal plane. Understanding of associations between diaphragm contractility and postural control in a CAI population may help to elucidate mechanisms of postural control deficiencies and could assist with the development of intervention protocols to restore the previous level of postural control before an injury and to mitigate further consequences of CAI. Lower diaphragm contractility may be related to diminished static postural control in the AP direction in patients with CAI, and, therefore, this unique exploration of diaphragm function may represent targets for intervention to restore static postural control for patients with CAI.
The diaphragm has been considered as a key element of postural stability by clinicians and researchers.4,46,62 The diaphragm can regulate IAP that helps to create postural stabilization by interacting with the transversus abdominis, the pelvic floor muscles, and the deep intrinsic muscles of the spine.22,24,26 As such, previous investigations have documented that poor diaphragm function presents in postural deficits and certain types of musculoskeletal injuries (eg, low back pain).35,36,48 Reduced diaphragm contractility increases reliance on accessory respiratory muscles (eg, pectoralis minor, scalene, sternocleidomastoid, serratus anterior, subclavius) and alters breathing mechanics manifesting as superior rib cage migration and reductions in abdominal excursion and lateral rib cage expansion.7,32 Maladaptive respiratory mechanics during respiration alter the mechanical relationship and arrangement of the diaphragm with the rib cage, placing the diaphragm in disadvantageous positions in the length-tension relationship.26,39,57 A loss of the optimal operating length of the diaphragm reduces its capacity to draw air into the lung during inspiration because of poor diaphragmatic decent upon contraction and insufficient tension of the diaphragm on the rib cage. 6 As result, compensatory breathing strategies can further develop, possibly degrading effects of IAP on postural control. 26
There is growing evidence of a significant contribution of diaphragmatic breathing to postural control.49,52 A previous study also observed patients with postural instability exhibited altered breathing patterns. 63 In addition, Bradley and Esformes 5 demonstrated breathing mechanics influenced functional movement patterns. In our current study, we observed that a lower change in diaphragm thickness from the end of inspiration to expiration related to worse static postural control in participants with CAI. The collective findings from previous and current studies suggest that the diaphragm has a crucial role in postural control; our study highlights a specific contribution that CAI may have in this relationship.
While we observed moderate correlations between diaphragm contractility and static postural control variables in the AP direction among participants with CAI, diaphragm contractility correlated negligibly or weakly with static postural control measures in the ML direction. Previous investigations have demonstrated that participants with CAI have less stable static postural control in the AP direction but not in the ML direction compared with uninjured controls.33,40 Researchers also identified potential adverse effects of altered neuromuscular function on static postural control among patients with CAI, particularly in the sagittal plane.55,56 Previous studies reported compensatory muscular activation patterns of proximal muscles and increases in sagittal-plane trunk and hip control in patients with CAI.55,56 Furthermore, thoracic dominant breathing with altered diaphragm function contributes to lower carbon dioxide levels in the bloodstream and an increase in respiratory rate, leading to a state of hyperventilation. 15 Previous research has demonstrated that an increase respiratory rate disturbs static postural control in the sagittal plane. 25 Perhaps our results suggest static postural control in the AP direction may be more linked to diaphragm contractility in patients with CAI than the ML direction.
The information gained from this study may provide insight into the current rehabilitation of CAI. There are diverse options to treat patients with CAI, and previous clinical trials have examined the effectiveness of a variety of intervention strategies on improving postural control in patients with CAI.2,12,13,41-43,51 However, much of the clinical research has concentrated efforts primarily on developing a peripheral impairment-based approach aimed to improve specific sensorimotor corrections in the ankle and foot.2,12,13,41-43,51 The peripheral impairment-based rehabilitation programs may be able to restore postural control by improving the ankle and foot function. Given that various factors (eg, altered proximal neuromuscular function, increased reliance on visual information) contribute to poor static postural control, there is room for further improvement in postural control and more innovative and adjunct approaches to the peripheral impairment-based interventions are required. Therefore, our results provided a potential alternate avenue to produce greater improvements in postural control outcomes. Our results suggest that altered diaphragm contractility could be a potential source for clinical deficiencies within patients with CAI. For example, previous clinical trials have reported that diaphragmatic breathing exercises significantly improve postural stability,49,52 and reduce pain and symptoms associated with other musculoskeletal injuries.1,59 Diaphragm breathing exercises may have the potential to help CAI patients to improve static postural control and break the cycle of recurrent injuries and impairments seen in CAI. Further research is required to examine how best to use the information from our study, but a possible area to explore could be the effectiveness of breathing exercises and techniques in restoring static postural control in patients with CAI to address the potential relationship we observed with diaphragmatic control.
Limitations
There are significant limitations to this current study. To minimize measurement errors, diaphragm contractility was assessed supine because we could maintain a firm transducer position on the examination site during ultrasonography. A previous study reported biomechanical breathing patterns changed from supine to standing positions, 27 and diaphragm function may differ by body positions as postural demands increase. Findings from our study may not adequately reflect diaphragm function during a single-leg balance task.
We did not measure pulmonary function, such as respiratory mouth pressure, and control respiratory measures during ultrasonography. Lung volume influences diaphragm contractility. 8 No participants self-reported pulmonary disease, and they were instructed to relax and quietly breathe normally, similar to activities of daily living. However, we cannot completely rule out that differences in inspiratory and expiratory mouth pressure during the quiet breathing among participants in this study influence our observations. Additional measures of pulmonary function with the quantification of diaphragm contractility are needed to confirm the associations between diaphragm contractility and static postural control in participants with CAI.
The small number of participants with CAI included in the present study is an important limitation to consider. The small sample size (15 participants with CAI) increases the risk for making a Type 2 error. Post hoc power analyses showed that we had moderate-to-strong power to detect significant and moderate correlations (observed powers, 0.70-0.80). However, nonsignificant findings were associated with low statistical power (observed powers: a range from 0.09 to 0.31), increasing the risk of a type 2 error. These nonsignificant correlations would need an expanded sample size to determine the true associations.
Conclusion
There were moderate correlations between diaphragm contractility and static postural control measures. Diaphragm contractility could be related to diminished static postural control, among the most common clinical deficiencies observed in patients with CAI.